
Abstract
Introduction
Cyclin Dependent Kinase (CDK) 4/6 inhibitors are changing the landscape of breast cancer treatment. These medications are generally well-tolerated, but incidences of hepatotoxicity have been reported in the literature.
Case Report
In this case, we present a 36-year-old Caucasian female who was diagnosed with hormone-receptor (HR) positive, human epidermal growth factor receptor 2 (HER2) negative metastatic breast cancer who initiated first line treatment with an aromatase inhibitor and a cyclin-dependent kinase (CDK) 4/6 inhibitor, ribociclib. Following treatment initiation, she experienced grade 4 hepatoxicity.
Management and Outcome
Ribociclib was discontinued due to probable cause of hepatotoxicity based on a Naranjo score of 7. Once her liver enzymes resolved to grade 1 toxicity, she was transitioned to another CDK 4/6 inhibitor, palbociclib. The patient has remained on palbociclib for 1 year of treatment with normalization of her liver function enzymes and stable disease.
Discussion
This case presents a successful rechallenge of an alternative CDK 4/6 inhibitor after grade 4 ribociclib-induced hepatotoxicity and reviews similar cases of ribociclib-induced hepatoxicity and management strategies.
Introduction
Cyclin Dependent Kinase (CDK) 4/6 inhibitors in combination with endocrine therapy are the recommended first line treatment for metastatic HR positive, HER2 negative breast cancer without visceral crisis. 1 There are currently three CDK 4/6 inhibitors approved in this setting by the Food and Drug Administration – palbociclib, ribociclib, and abemaciclib. The side effect profiles of these medications vary and selection of the appropriate CDK 4/6 inhibitor should be based on patient specific factors.
Recently, there has been a marked increase in the usage of ribociclib among all three CDK 4/6 inhibitors. The recent increase in prescribing could be attributed to the category 1 designation for ribociclib in the NCCN guidelines due to the overall survival benefit seen in the Monaleesa-7 trial.1,2 It can be anticipated that ribociclib's usage will continue to increase given the newest indication for adjuvant treatment of early-stage breast cancer approved by the FDA in September 2024 based on results from the NATALEE trial. 3 The increased ribociclib usage, has brought attention to the rare, but serious adverse effect of hepatotoxicity in which grade 3 or higher hepatotoxicity incidence has been reported in up to 11% of patients. 2 Close monitoring of liver function tests are recommended by the manufacturer. 4
This case presents a 36-year-old female patient with metastatic breast cancer who tolerated palbociclib after failure to tolerate ribociclib due to grade 4 hepatotoxicity. Written informed consent and permission to publish this case report was obtained from the patient. This report will discuss our patient case, available data on hepatotoxicity associated with CDK 4/6 inhibitors, and similar cases to assist with management of ribociclib-induced hepatotoxicity without the need to abandon the CDK 4/6 inhibitor class.
Case report
We present a 36-year-old Caucasian female with no significant past medical history who presented to the emergency department with a chief complaint of fatigue, nausea, and recent diagnosis of pneumonia. Routine lab work revealed transaminitis and computed tomography (CT) scans demonstrated a spiculated right breast lesion, innumerable liver lesions, widespread lytic bony lesions including a right femoral head/neck lesion concerning for impending pathologic fracture, and periportal/retroperitoneal lymphadenopathy consistent with a diffuse metastatic malignancy. Patient underwent a liver biopsy which revealed metastatic adenocarcinoma, consistent with breast primary. The biomarkers revealed estrogen receptor 96%, progesterone receptor 49%, HER2 negative (IHC 0).
Given pre-menopausal status, ovarian function suppression was initiated on 8/31/2023. On 9/7/2023, patient started ribociclib 600 mg daily on days 1–21 then off for 7 days and letrozole 2.5 mg daily. Denosumab was added on 9/29/24 after dental clearance. At baseline, patient had grade 1 elevation of AST and alkaline phosphate attributed to innumerable liver lesions observed on imaging. Her ALT and bilirubin were within normal limits. Lab work was completed according to package insert recommendations. At two weeks and four weeks, labs demonstrated improving liver function tests (LFTs). At week 6 of treatment, LFTs’ began to trend up with a grade 2 elevation of AST and grade 1 elevation of both ALT and alkaline phosphate. At that time, treatment continued, and imaging was ordered due to concern of disease progression. On the contrary, CT scans and nuclear medicine bone scans conveyed disease response to the ribociclib and aromatase inhibitor after 9 weeks of treatment.
The patient returned to clinic for cycle 3 where she was found to have grade 4 AST elevation, grade 3 ALT elevation, grade 2 alkaline phosphate elevation, and rise in bilirubin (AST 970 U/L, ALT 804 U/L, alkaline phosphate 403 U/L and bilirubin 1.2 mg/dL). At this time ribociclib was held and letrozole continued. Since the adverse reaction due to ribociclib was considered, the Naranjo algorithm was applied and the score was found to be 7, indicating a probable cause (see supplemental material).
Management and outcome
Two weeks after holding ribociclib, there was a continued increase in AST, ALT, alkaline phosphate, and bilirubin values. Patient was admitted for further workup and found to have hepatocellular injury concerning for drug induced liver injury (DILI) from ribociclib. 5 On discharge, the ribociclib was discontinued. On discussion with hepatology, a course of prednisone 40 mg by mouth daily was trialed for the ribociclib-induced DILI. Prednisone was started on 11/28/23 and completed on 12/20/23 resulting in resolution of elevated LFTs. Given good disease response to the CDK 4/6 inhibitor, we discussed trying an alternative CDK 4/6 inhibitor with close monitoring. She started palbociclib at a reduced dose of 100 mg on days 1–21 every 28 days on 1/19/24. The patient has remained on palbociclib for ∼1 year with complete normalization of her liver function tests and stable disease. Figure 1 shows the AST/ALT trends while on ribociclib and after initiating palbociclib.
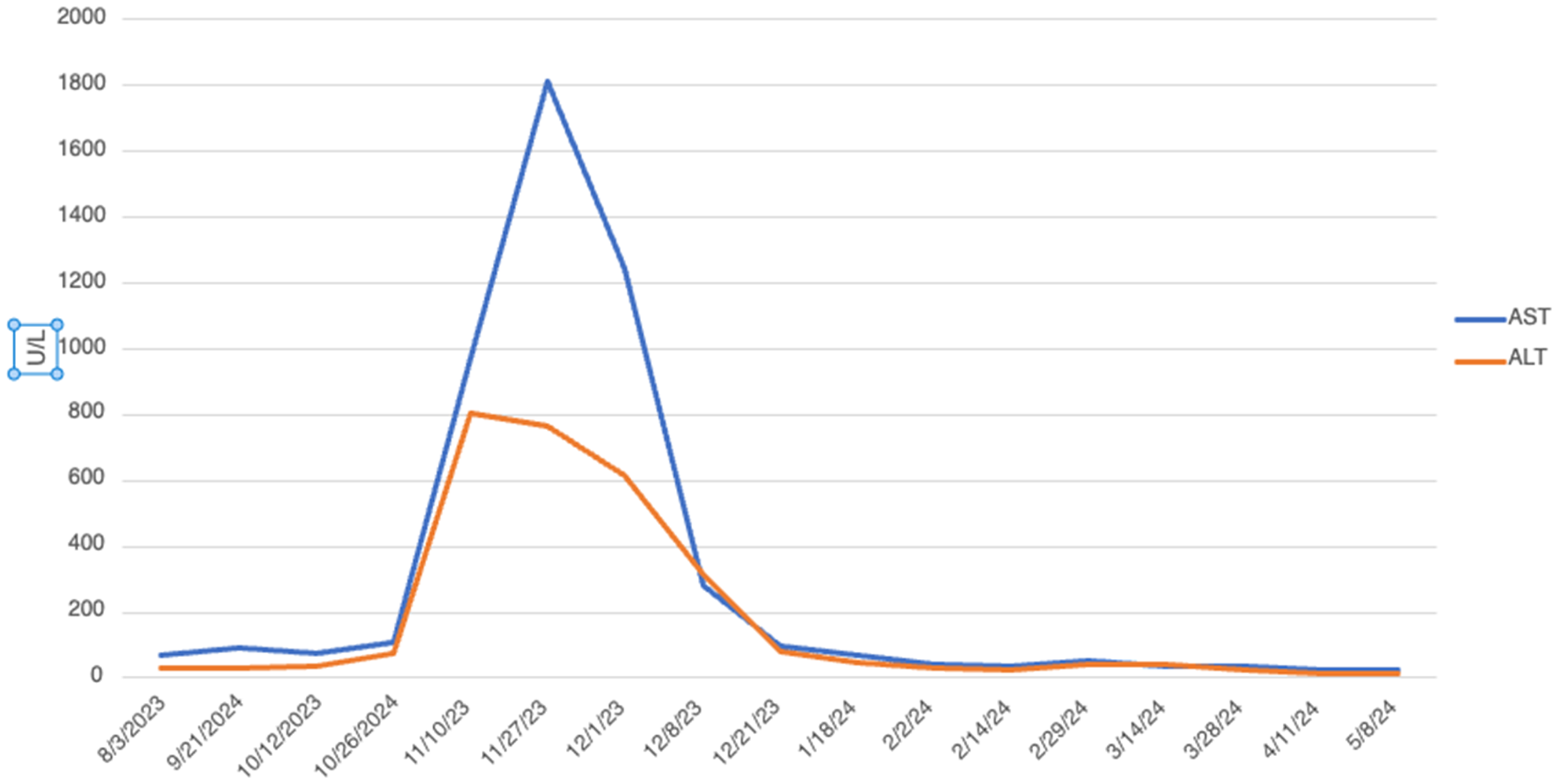
AST and ALT trends before and after intiation of ribociclib and palbociclib.
Discussion
CDK 4/6 inhibitors have changed the landscape of HR + HER2- metastatic breast cancer treatment due to their significant increases in progression free survival. Moreover, the National Comprehensive Cancer Network (NCCN) guideline for breast cancer recently updated their guidelines to recommend ribociclib in combination with an aromatase inhibitor as a category 1 recommendation for first line treatment due to the results of the MONALESSA-7 trial.1,2 This trial reported an overall survival benefit with ribociclib in combination with an aromatase inhibitor. 2 At this time, palbociclib and abemaciclib in combination with an aromatase inhibitor have not demonstrated an overall survival benefit in this setting. 1 Due to the overall survival benefit data, ribociclib is often favored by providers over palbociclib and abemaciclib. However, selection of the most appropriate CDK 4/6 inhibitor should also be based on patient specific factors due to the varying side effect profile, drug-drug interactions, and dosing schedule of these medications.
The incidence of hepatotoxicity reported in pivotal trials among CDK 4/6 inhibitors is summarized in Table 1. PALOMA-3 reported the lowest incidence of grade 3 ALT elevation of only 3% in patients receiving palbociclib. 6 MONALEESA-2 reported higher incidences of grade 3 or 4 ALT elevations with ribociclib at 9.6% and grade 3 or 4 AST elevation of 5.4%. 7 The MONALESSA-7 trial reported similar incidence of grade 3 hepatobiliary toxicity with ribociclib at 10.4%. 2 The MONARCH-3 trial reported incidence of grade 3 or 4 ALT elevation with abemaciclib at 5.8% and grade 3 or 4 AST elevation of 3.8%. 8 In an article by Onesti et al., ribociclib showed a higher risk of hepatic toxicity, than palbociclib and abemaciclib. 9 The absolute risk for grade 3–4 ALT increase was 0.097 (ribociclib), 0.046 (abemaciclib) and 0.034 (palbociclib). The absolute risk for AST increase was 0.054 (ribociclib), 0.029 (abemaciclib), and 0.029 (palbociclib). 9 Based on the reported incidences of hepatotoxicity in pivotal trials and the data presented above, we decided to rechallenge with palbociclib over abemaciclib due to lower incidence and lower absolute risk of ALT and AST elevations.
Rates of ALT/AST elevations with CDK 4/6 inhibitors from phase 3 clinical trials.
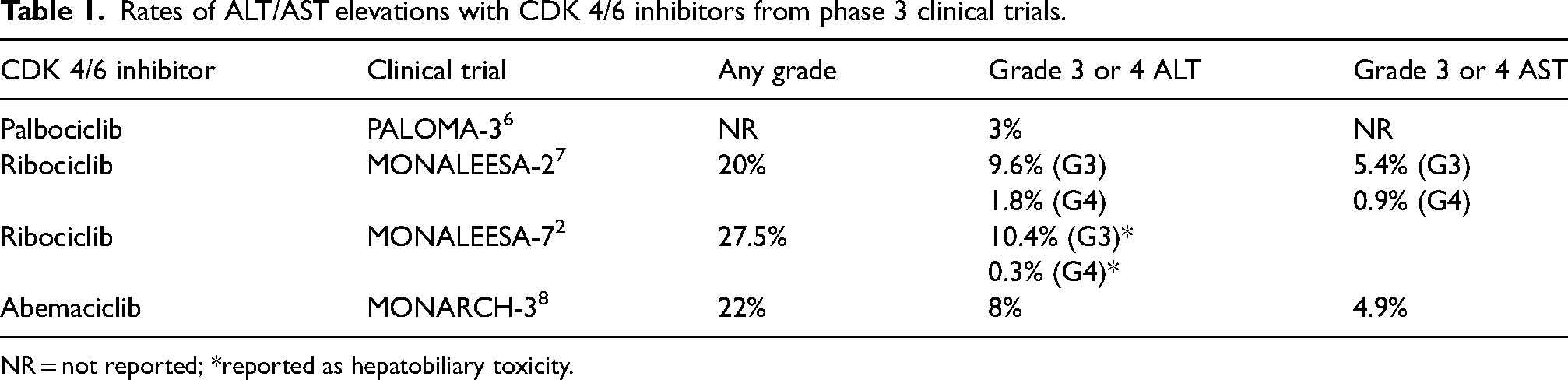
NR = not reported; *reported as hepatobiliary toxicity.
Recently, abemaciclib and ribociclib have received indications in the adjuvant setting for patients with early-stage breast cancer. The MonarchE trial evaluated abemaciclib 150 mg twice daily in combination with endocrine therapy for patients with high-risk stage III early HR + breast cancer. 10 This trial demonstrated an invasive disease-free survival benefit with abemaciclib in combination with endocrine therapy compared to endocrine therapy alone. 10 Grade 1–2 elevations of AST and ALT were reported roughly at 10%. Grade 3 elevations of AST and ALT were 1.8% and 2.6%, respectively. Grade 4 elevations of AST and ALT were seen in <0.2%. 10 The NATALEE trial evaluated ribociclib at a reduced dose of 400 mg in combination with endocrine therapy as adjuvant treatment for patients with stage II or III early stage HR + breast cancer. 10 This trial demonstrated an increase in invasive-free survival with ribociclib in combination with endocrine therapy compared to endocrine therapy alone. 11 All grade transaminitis were reported in roughly 15–20% of patients, whereas roughly 5% of patients experienced grade 3 elevations and roughly 1% experienced grade 4 elevations. 11 Despite the use of a reduced ribociclib dose in the adjuvant setting, hepatotoxicity was still reported indicating that his may not be a dose dependent toxicity. 11 Since abemaciclib and ribociclib will now be prescribed for patients with early stage and metastatic disease, it is important to be aware of risk of hepatotoxicity when selecting a CDK 4/6 inhibitor and monitor patients appropriately.
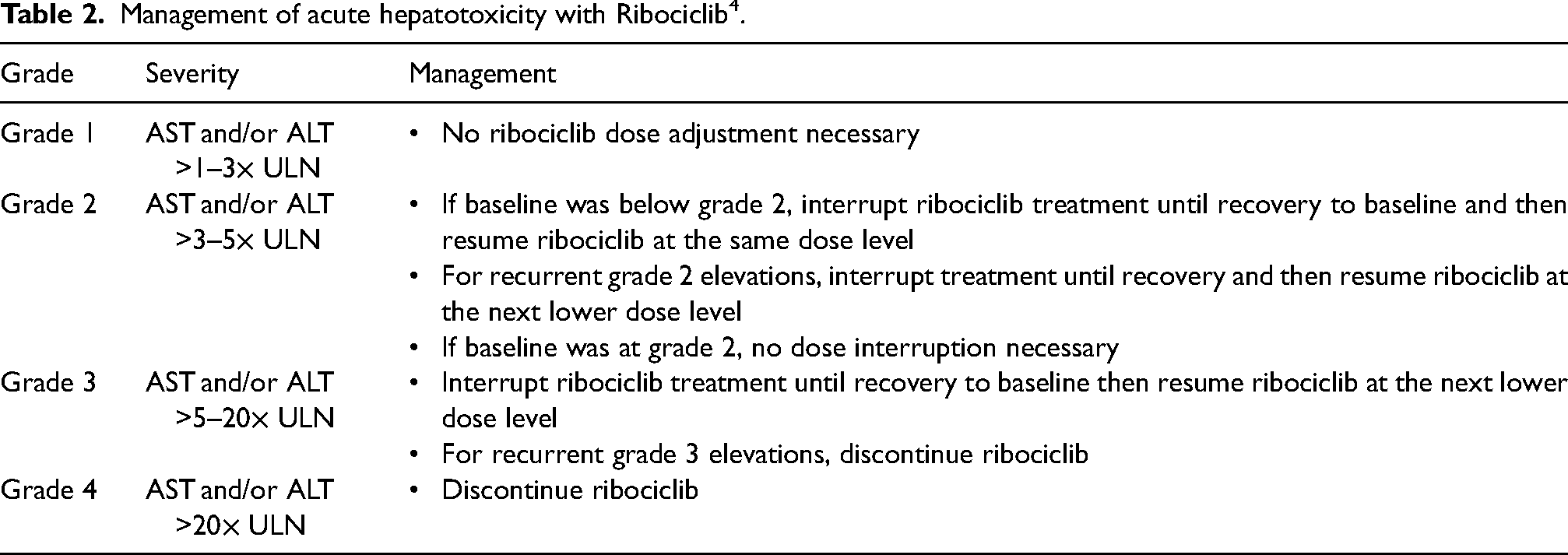
Patients should be monitored for hepatotoxicity with routine lab work every 2 weeks for the first 2 months then monthly or as clinically necessary. 4 Package insert recommendations for management of hepatotoxicity are summarized in Table 2. Dose interruption of ribociclib is recommended for grade 2 LFT elevations (unless elevated at baseline as seen in our patient). Grade 4 LFT elevations warrant discontinuation of ribociclib. 4
Management of acute hepatotoxicity with Ribociclib 4 .
The onset of hepatotoxicity has been reported in the literature at a median 16 weeks of therapy. 12 In our patient case, onset of grade 4 AST elevation and grade 3 ALT elevation occurred at 9 weeks (64 days). This is earlier than the reported median; however, a range of 2–135 weeks has been reported. 12 Ciaccio et al. also reported liver enzyme normalization occurs after a median of 43 days following discontinuation of the CDK4/6 inhibitor. 12 In our patient case, we saw very similar results with liver enzymes recovery to grade 1 after 41 days.
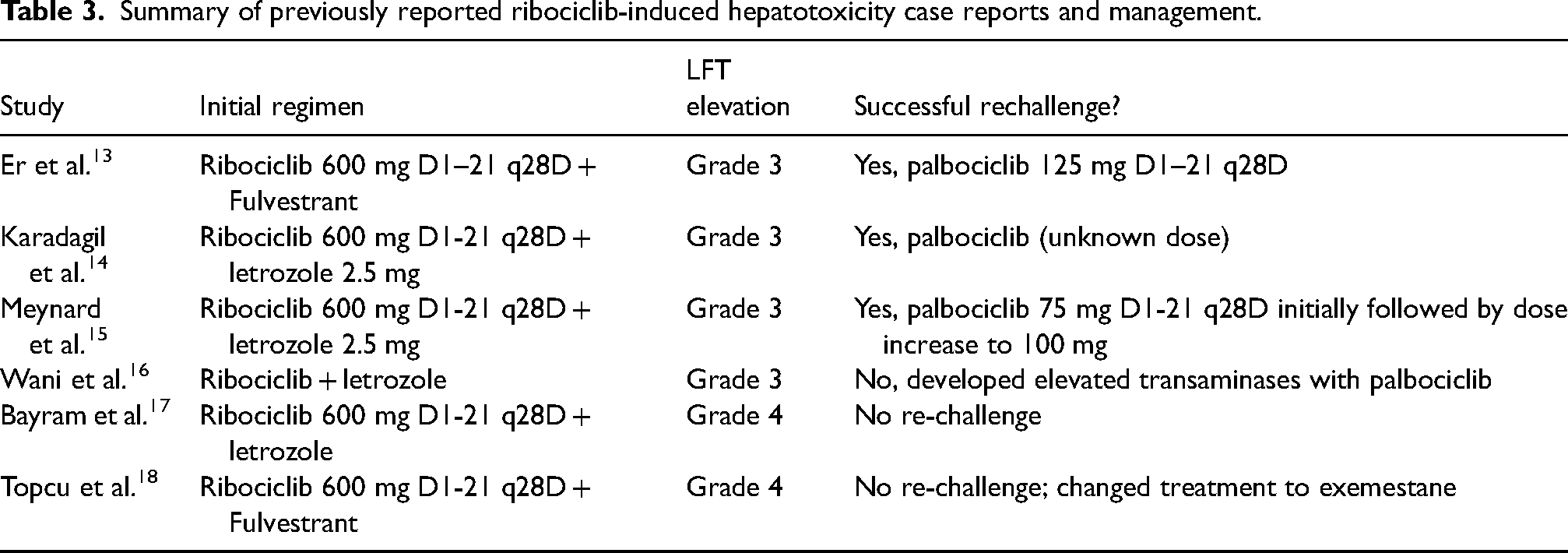
There have been other cases of reported hepatotoxicity with ribociclib. Table 3 summarizes previously reported ribociclib-induced hepatotoxicity case reports and management strategies. Er et al. described a patient who initiated treatment with ribociclib 600 mg in combination with fulvestrant and experienced grade 3 hepatotoxicity during her third cycle of treatment, which was a similar onset to our case. 13 The patient was dose reduced to 400 mg and also experienced grade 3 hepatotoxicity. The hepatotoxicity lasted roughly 14 days each time. The observed recovery was shorter than in our case. They discontinued the ribociclib and started the patient on palbociclib 125 mg + fulvestrant. The authors commented that they chose to start her at full palbociclib dose to increase treatment success. This patient tolerated palbociclib without any hepatotoxicity (∼4 months of therapy at time of publication). 13 Karadagil et al. described a patient who started ribociclib 600 mg and experienced neutropenia requiring a dose reduction to 400 mg during the first month of therapy. 14 The patient then experienced grade 3 elevations in AST and ALT within the first month of the dose reduction. The patient was further dose reduced to the ribociclib 200 mg with persistent hepatotoxicity and ultimately switched to palbociclib which was tolerated at an unknown dose. 14 Meynard et al. also described a case of hepatotoxicity related to ribociclib 600 mg with an onset of 16 weeks on ribociclib 600 mg. 15 This onset is on par with the onset reported in the literature but was significantly shorter than our patient case. The hepatotoxicity lasted 14 weeks in this case which was longer than what is reported in the literature and our case. In this case, the authors decided on a dose escalation and started the patient on Palbociclib 75 mg then increased to 100 mg. At time of publication, the patient has successfully completed 1 year of treatment without toxicity or progression on palbociclib. 15
Summary of previously reported ribociclib-induced hepatotoxicity case reports and management.
Conclusion
With increasing use of ribociclib in both metastatic and recently early-stage breast cancer settings, physicians may encounter ribociclib induced hepatotoxicity. This case report demonstrates the successful re-challenge of an alternative CDK 4/6 inhibitor on development of ribociclib induced hepatotoxicity allowing physicians to continue patients with CDK 4/6 responsive disease in a safe manner.
Supplemental Material
sj-docx-1-opp-10.1177_10781552251340613 - Supplemental material for Rechallenge of an alternative CDK 4/6 inhibitor after hepatotoxicity in the treatment of hormone-positive metastatic breast cancer
Supplemental material, sj-docx-1-opp-10.1177_10781552251340613 for Rechallenge of an alternative CDK 4/6 inhibitor after hepatotoxicity in the treatment of hormone-positive metastatic breast cancer by Kasey Jackson, Kiera Roubal, Christopher Rangel and Frank Brescia in Journal of Oncology Pharmacy Practice
Footnotes
Author contribution
KJ: Data Curation, Writing - Original Draft; KR: Writing - Review & Editing; CR: Writing - Review & Editing, Supervision; FB: Writing - Review & Editing, Supervision.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval and informed consent statements: Our institution does not require ethical approval for reporting individual cases or case series. Written informed consent was provided by the patient.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.