
Abstract
Introduction
The preferred first-line regimen in advanced renal cell carcinoma (aRCC) remains uncertain, because rapid evolution of immunotherapy-based combination regimens quickly outdates the existing evidence. Current strategies for synthesizing these data lack clarity and applicability. Thus, we performed a meta-analysis comparing the effectiveness and safety of dual immunotherapy and immunotherapy plus tyrosine kinase inhibitors in aRCC.
Methods
A systematic search was conducted across two databases, PubMed and the Cochrane Library, for literature published between January 2000 and March 2025. Cohort studies providing direct comparisons of these therapies were included. A random-effect model was utilized to pool hazard ratios (HRs) with 95% confidence intervals (CIs) for progression-free survival (PFS) and overall survival (OS).
Results
Six studies, including 5486 patients, were analyzed. There was no statistically significant difference in progression-free survival between the two interventions (HR 0.92, 95% CI 0.84–1.00, p = 0.06, I2 = 7%). The OS benefit was similar for both regimens (HR 1.00, 95% CI 0.89–1.12, p = 1.00, I2 = 0%). Limited availability of safety data precluded a comprehensive assessment of their toxicity profiles.
Conclusion
The findings of this meta-analysis do not support a definitive preference for either of the immunotherapy combinations. Nevertheless, given the low certainty of retrospective data, randomized controlled trials and prospective cohort studies are needed to inform evidence-based clinical decisions.
Keywords
Introduction
Renal cell carcinoma (RCC), the ninth most prevalent urological malignancy, is associated with a poor prognosis. The major subtype is clear cell carcinoma, whereas papillary, chromophobe, and Bellini duct carcinomas are less common. 1 Pathogenetically, mutations in the tumor suppressor von Hippel–Lindau (VHL) gene are primary drivers of disease development and progression. 2 Over the past three decades, the therapeutic landscape has evolved from immune cytokines to targeted therapies. 3 Sunitinib was the first agent to demonstrate a definitive survival benefit for this disease (hazard ratio [HR] 0.42, 95% confidence interval [CI] 0.32–0.54).4,5 However, the effectiveness of tyrosine kinase inhibitors diminishes over time due to acquired resistance. 2
Renal cell carcinoma has been traditionally considered chemo resistant but highly immunogenic. Despite of robust T lymphocyte infiltration in tumor microenvironment, the cells escape immune detection by activating suppressor checkpoints. 6 Immunotherapy targeting these checkpoints has become a cornerstone of the treatment. 6 Following the Checkmate-025 phase-III trial, nivolumab became the preferred option for patients progressing after one or more vascular endothelial growth factor receptor (VEGFR) therapies. 7 Nevertheless, only 31% patients demonstrated a durable response exceeding one year, highlighting the complex and dynamic nature of tumor response. 7 Subsequently, including immunotherapy-based combination regimens has augmented antitumor response, thus overcoming the limitations of monotherapies. 6 The CheckMate-214 trial evaluated the efficacy and safety of nivolumab plus ipilimumab and sunitinib. 8 The results demonstrated superiority in survival outcomes favoring dual immunotherapy for patients with International Metastatic Renal Cell Carcinoma Database Consortium (IMDC) intermediate-and poor-risk disease. 8 Similarly, the CheckMate-9ER trial reported improved progression-free survival and overall survival for nivolumab plus cabozantinib regimen over sunitinib. 9 In the KEYNOTE-426 trial, axitinib plus pembrolizumab combination showed a survival advantage over single agent tyrosine kinase inhibitor. 10 These findings from randomized controlled trials established these treatment regimens as the standard of care for advanced renal cell carcinoma.8,9,10,11,12 However, the lack of direct comparative trials leaves the choice of the optimal therapy contentious. 13 Therefore, to guide evidence-based clinical decisions, we conducted a systematic review and meta-analysis comparing these two first-line combinations, dual immunotherapy and immunotherapy plus tyrosine kinase inhibitors in patients with aRCC.
Materials and methods
Data sources and search strategy
This systematic review and meta-analysis conform to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines (Supplementary Table 1). The protocol was registered in PROSPERO (CRD420251072815). A detailed search strategy was developed using a combination of keywords and medical subject headings (MeSH) terms. It included “renal cell carcinoma”, “immunotherapy plus targeted therapy”, “dual immunotherapy”, “nivolumab plus ipilimumab”, “pembrolizumab plus axitinib”. The systematic search was conducted across two databases: MEDLINE (PubMed) and the Cochrane Library. English language articles published between January 2000 and March 2025 were considered for analysis. Additionally, references were identified by hand-searching bibliographies and screening recent conference abstracts (Supplementary Table 2).
Study selection
Titles and abstracts were reviewed, and duplicates were removed using the Rayyan artificial intelligence tool.
24
Two authors (VP and BY) independently sought articles according to following inclusion criteria:
Patients with advanced or metastatic renal cell carcinoma. Prospective or retrospective cohort studies directly comparing dual immunotherapy with immunotherapy plus targeted therapy. Articles reporting hazard ratios for progression-free survival (PFS) and overall survival (OS).
Discrepancies at any stage were resolved through discussion among all authors. Ultimately, six publications were included for quantitative analysis.
Data extraction
Two authors independently extracted data into a Microsoft Excel spreadsheet. Details about study characteristics, patient demographics, objective response rate, median progression-free survival, median overall survival, hazard ratios for survival outcomes and treatment-related adverse events (TRAEs) were retrieved. If any essential information about study outcomes was missing or unclear, the corresponding authors were contacted for clarification.
Risk of bias assessment
The risk of bias assessment was done by using the Risk of Bias in Non-randomized Studies of Interventions (ROBINS-I) tool (Sterne et al.). It captures bias across seven domains. They include confounding, classification of intervention, selection of participants into the study, deviation from intended intervention, missing data, outcome measurement, and selection of reported results. Each domain was given a score of low, moderate, or high. This meta-analysis is inherently limited by its reliance on cohort studies. Therefore, progression-free survival and overall survival were further appraised using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) criteria.
Statistical analysis
Hazard ratios (HRs) with 95% confidence intervals (CIs) were extracted for PFS and OS. ReVMan software (Version 5.4) was used to perform the analysis. Heterogeneity across studies was assessed using the Q test and the I2 statistic, with a p-value ≥ 0.05 indicating non-significance. Given the different baseline characteristics of patient populations and treatment regimens across cohorts, the pooled effect estimate was calculated using a random effect model. Treatment-related adverse events (TRAEs) were summarized descriptively. A sensitivity analysis was conducted to assess the robustness of the pooled estimates.
Results
Study selection process
Database searching yielded 538 citations, of which 69 duplicates were removed. 24 After primary abstract screening, 14 records were considered for full text review. Eight articles were excluded due to incomplete data(n = 1) or because they evaluated the effectiveness of only one immunotherapy combination (n = 7). Ultimately, six cohort studies were included for analysis (Figure 1).13–17,22
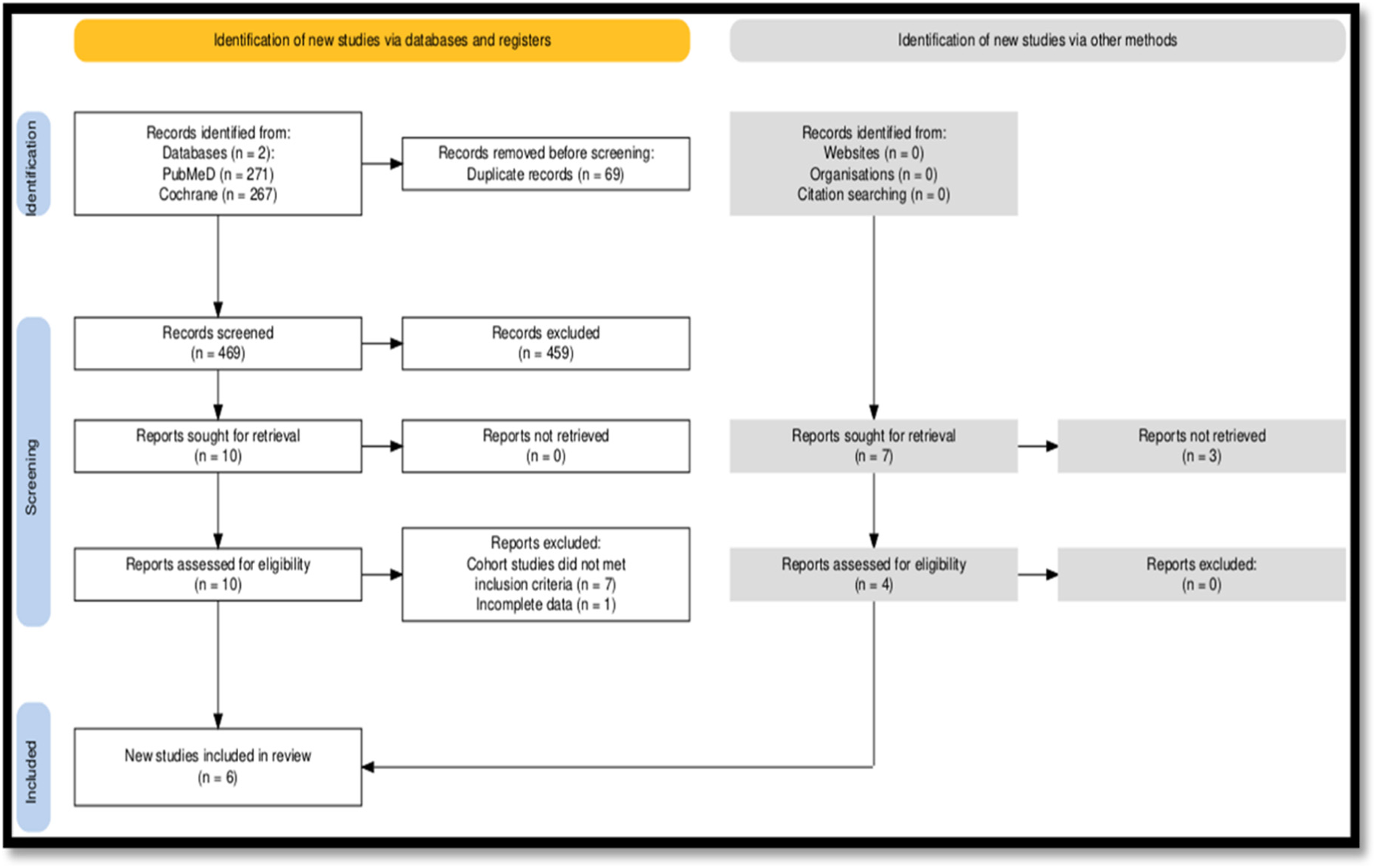
Preferred reporting items for systematic reviews and meta-analysis (PRISMA) flow diagram of the literature screening.
Study characteristics
The median age of participants ranged from 62.7 to 68 years. The proportion of males was higher than that of females. Median follow-up durations ranged from 7.2 to 60 months. The distribution of IMDC risk categories (favorable, intermediate, and poor-risk) varied across studies, with most patients classified as intermediate risk. Hazard ratios (HRs) for progression-free survival ranged from 0.53 to 1.17, and those for overall survival ranged from 0.72 to 1.16, reflecting variability in treatment effectiveness across cohorts (Table 1).
Baseline characteristics of the included studies.
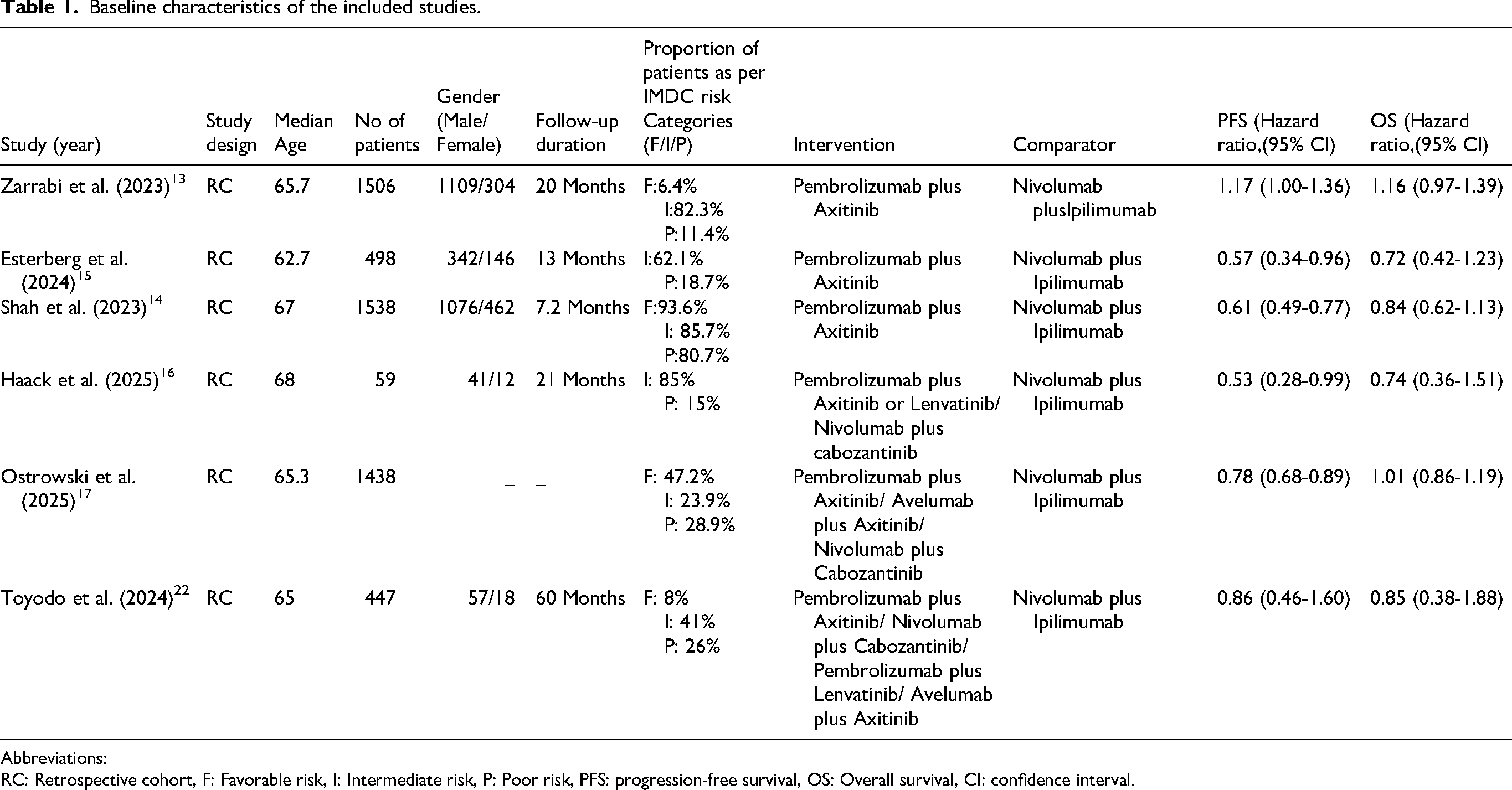
Abbreviations:
RC: Retrospective cohort, F: Favorable risk, I: Intermediate risk, P: Poor risk, PFS: progression-free survival, OS: Overall survival, CI: confidence interval.
Quality of study
The ROBINS-I tool indicated that four studies had a moderate risk of bias. It was primarily due to confounding, selection of participants, deviations from intended interventions, missing data, and outcome measurement. Two studies were judged to have a high risk of bias, mainly due to confounding and selection of reported results (Table 2).
Risk of bias assessment of studies as per ROBINS-I tool.

Effectiveness outcomes
Six studies, comprising 5486 patients, were included to derive summary estimates of survival outcomes. The pooled hazard ratio did not show a statistically significant PFS benefit for immunotherapy plus targeted therapy (HR = 0.92, 95% CI 0.84–1.00; p = 0.06; I2 = 7%) (Figure 2). Sensitivity analysis excluding two high-risk studies (Ostrowski et al., Toyoda et al.) confirmed this finding (Z = 0.86; p = 0.39) (Supplementary Figure. 1). Statistical heterogeneity among the studies was low (PFS, I2 = 7%, p = 0.37, OS, I2 = 0%, p = 0.98). The pooled hazard ratio for OS was 1.00 (95% CI, 0.89–1.12), indicating no statistically significant difference between the two treatment arms (Z = 0.03, p = 0.98) (Figure 3). Sensitivity analysis produced no meaningful change in the OS estimate. Funnel plots did not suggest publication bias (Supplementary Figure. 2 and Figure 3), though with only six included studies, this assessment is underpowered. Evidence quality for both progression-free survival and overall survival was rated low as per GRADE criteria (Supplementary Table. 3). 25
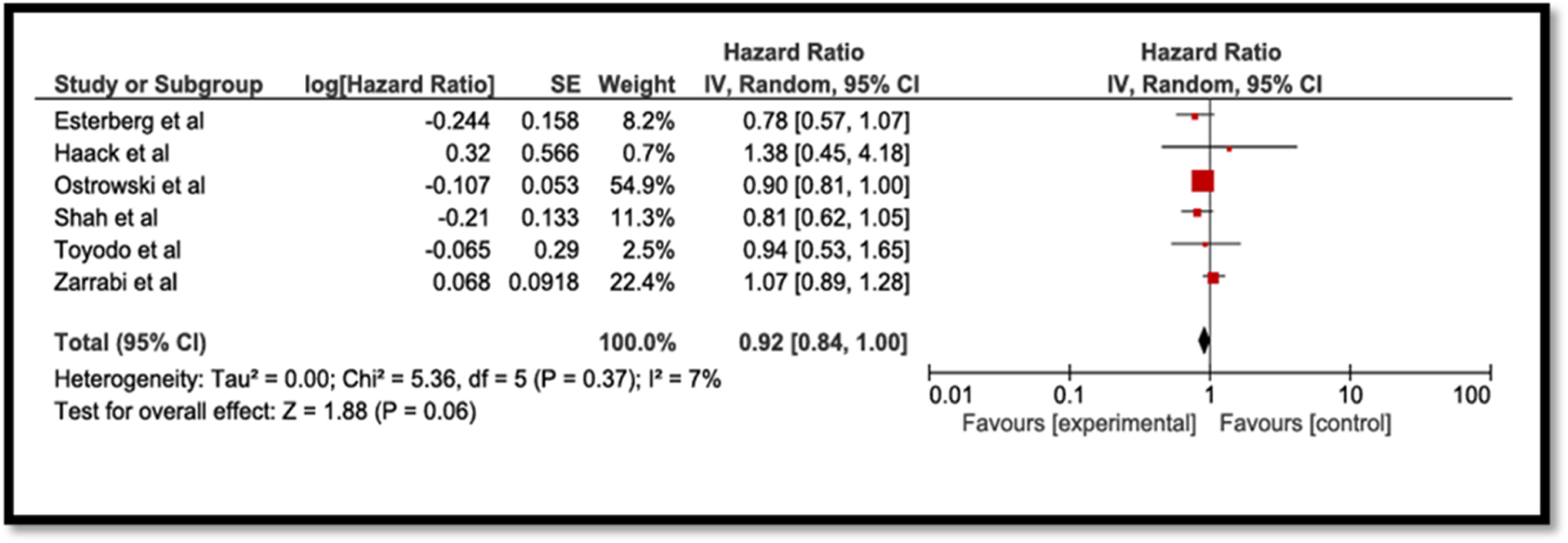
Forest-plot for progression-free survival (PFS).
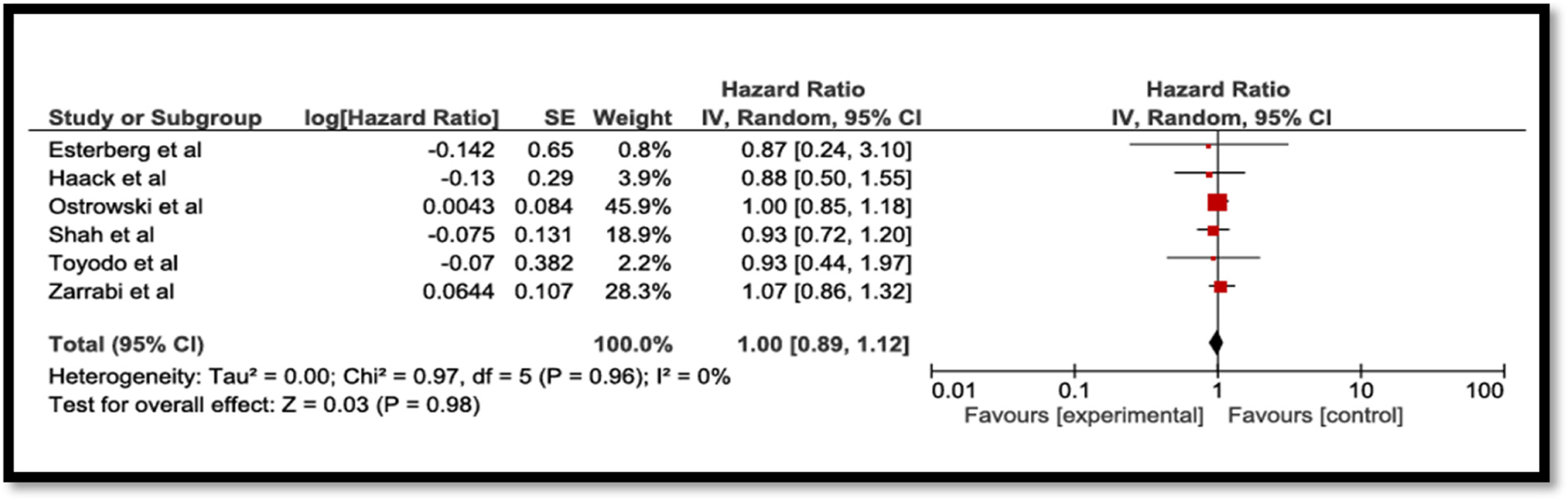
Forest plot for overall survival (OS).
Safety outcomes
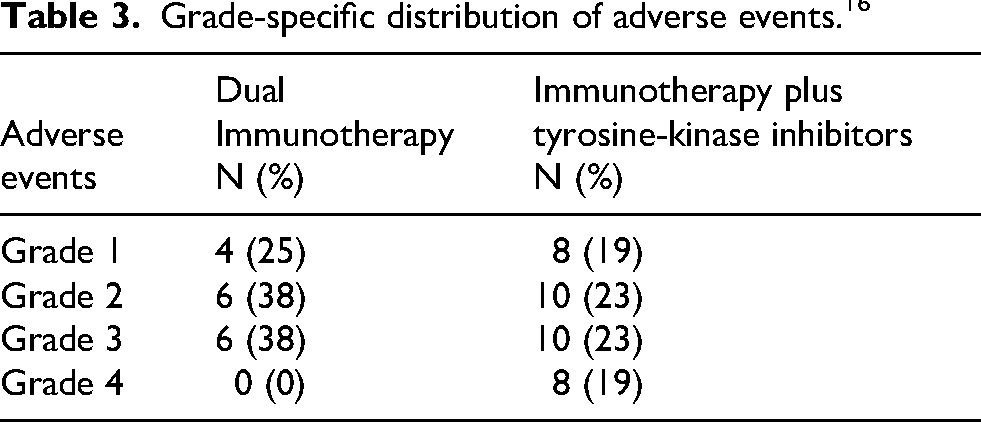
Safety data were insufficient for pooled analysis, as only one study reported adverse events. Treatment-related grade-3 adverse events included apoplexy, pulmonary embolism, subarachnoid hemorrhage, and atrioventricular block 16 (Table 3).
Grade-specific distribution of adverse events. 16
Discussion
Renal cell carcinoma is characterized by substantial immune filtration, and immunotherapy has long been established as a cornerstone of treatment. It enhances T-cell activity by blocking multiple inhibitory pathways, restoring vascular permeability, and improving immune cell entry and function. 6 According to National Comprehensive Network Guidelines (NCCN) and pivotal randomized controlled trials immunotherapy- based combination regimens are standard of care for patients with metastatic disease.11,18–20 Nonetheless, uncertainty remains about the optimal regimen. To our knowledge, this is the first pairwise meta-analysis evaluating effectiveness and safety of these first-line combination regimens for patients with advanced renal cell carcinoma. It primarily synthesizes evidence for PFS and OS from six cohort studies comprising a total of 5486 patients. The studies have minor variations in follow-up duration. Pooled analysis showed no difference in progression-free survival between these interventions. Shah et al. demonstrated superior PFS for pembrolizumab plus axitinib over dual immunotherapy (16.4 months (95% CI, 11.9-NR, p < 0.001). Similar results were observed in a study conducted by Esterberg et al. The Median PFS was 13 months for pembrolizumab plus axitinib and 8.3 months for dual immunotherapy (HR: 0.78, 95% CI, 0.68–0.90; p < 0.001).14,15 Subsequently, Haack et al. demonstrated a median PFS of 14 months for pembrolizumab plus axitinib and 6 months for nivolumab plus ipilimumab (HR: 0.53 (0.29–0.99), p = 0.039). 16 These findings favoring immunotherapy plus tyrosine kinase inhibitors in cohort studies are contradictory to our results. The discrepancy stems from low certainty of evidence as per GRADE criteria, because of serious risk of bias and imprecision. It precludes superiority conclusions for either of these regimens.
Overall survival (OS) outcomes were comparable between immunotherapy-based combination regimens. The similar results were reported by Shah et al. (HR: 0.84, 95% CI 0.62–1.13, p = 0.245), Esterberg et al. (HR:0.72, 95% CI [0.42–1.23], p = 0.226) and Haack et al. (HR: 0.74 (0.36–1.51); p = 0.403) [14–16]. In the network meta-analysis conducted by Chen et al., indirect cross-trial comparison between immunotherapy plus targeted therapies did not show statistically significant differences for survival outcomes. Although the rank probability analysis favored pembrolizumab plus lenvatinib for improved PFS in patients. 21 The findings of this analysis are similar to the NCCN guideline recommendations. 11 Zarrabi et al. demonstrates survival benefit for pembrolizumab plus axitinib in the favorable-risk subgroup. 13 However, the absence of regimen and IMDC-specific stratified data in some studies precluded quantitative subgroup analysis, this observation should be considered exploratory. The summary estimates for survival outcomes are derived from retrospective cohorts prone to selection bias due to confounding and have high methodological limitations, undermining their clinical applicability.
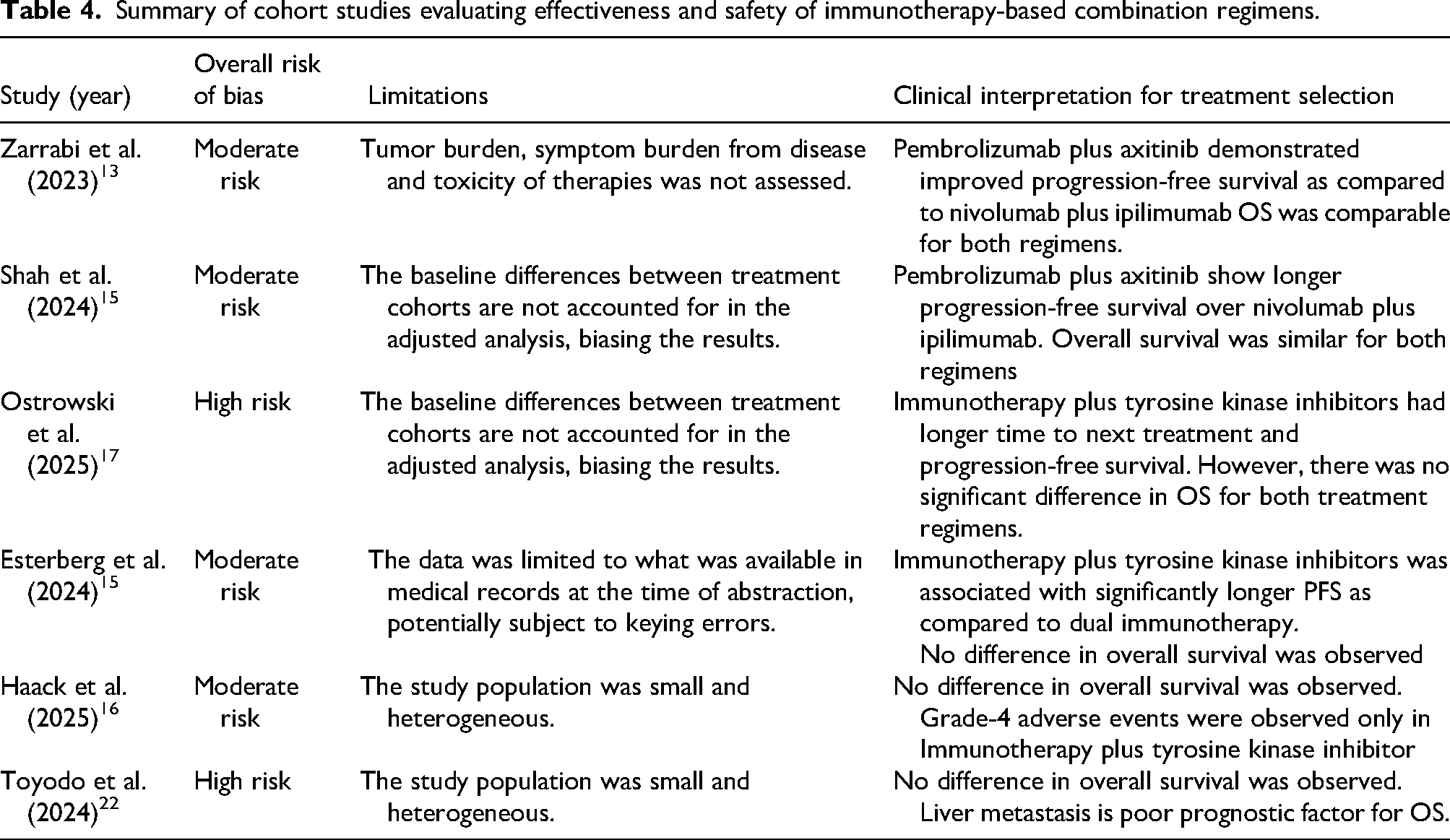
There is a lack of data available for safety, so no reliable conclusions can be drawn regarding the comparative safety profiles of these regimens. 16 Another drawback is that few studies had baseline differences within treatment cohorts, which may bias effect estimates for survival outcomes.14,16,17,22 Additionally, evidence for non–renal cell carcinoma comes from a single study, the findings cannot be generalized to those patients. These limitations substantially constrain the strength and generalizability of our findings. In practice, treatment selection should be based on patient factors such as age, gender, comorbidities, performance status, and toxicity profile rather than on survival difference alone (Table 4).
Summary of cohort studies evaluating effectiveness and safety of immunotherapy-based combination regimens.
Conclusion
The findings of this meta-analysis do not support a definitive preference for either immunotherapy combination. Treatment choices should be individualized based on clinical factors rather than survival benefit alone. Given the low certainty of evidence, randomized controlled trials and prospective cohort studies with longer follow-up are needed to guide evidence-based treatment selection and optimize patient outcomes.
Supplemental Material
sj-pdf-1-opp-10.1177_10781552261459599 - Supplemental material for Effectiveness and safety of first-line therapies, dual immunotherapy versus immunotherapy plus targeted therapy in advanced renal cell carcinoma: A systematic review and meta-analysis
Supplemental material, sj-pdf-1-opp-10.1177_10781552261459599 for Effectiveness and safety of first-line therapies, dual immunotherapy versus immunotherapy plus targeted therapy in advanced renal cell carcinoma: A systematic review and meta-analysis by Avinash Khadela, Vaishnavi Patel, Beema T Yoosuf and Rushabh Kothari in Journal of Oncology Pharmacy Practice
Footnotes
Acknowledgments
The authors have nothing to report.
Credit authorship contribution statement
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Data sharing does not apply to this article as no new data were created or analyzed in this study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.