
Abstract
Background:
This study examined how the presence of psychotic symptoms affects police decision-making during behavioral health crisis interventions, with a focus on outcomes of jail diversion, emergency department (ED) diversion, and involuntary hold.
Aims:
This study aimed to compare intervention patterns for individuals with and without psychotic presentations and to identify demographic, clinical, and operational factors associated with outcomes across groups.
Methods:
A retrospective analysis of 50,062 police-led crisis encounters recorded in the Massachusetts Department of Mental Health’s jail diversion program database between April 2023 and January 2025 was conducted, using stratified mixed-effects logistic regression with program location as a random effect.
Results:
Psychosis was present in 22.8% of all encounters and was associated with similar rates of jail diversion (87.9% vs. 84.7%) and ED diversion (43.1% vs. 54.3%), and higher rates of involuntary hold (26.1% vs. 11.5%). Assessment in home or community settings was associated with increased ED diversion across populations, while the presence of on-scene emergency or support personnel predicted involuntary hold. Among those with psychosis, charge severity, referral source, and prior police contact were associated with jail diversion, while mood disorder had a stronger association with involuntary hold in the non-psychosis group.
Conclusions:
Findings highlight the need for population-specific crisis response protocols that integrate clinical features, setting, and referral dynamics. Structured decision-making tools, co-response models, and expanded consultation roles for mental health professionals, including psychiatric nurses, may improve alignment between individual needs and intervention outcomes.
Keywords
Introduction
The deinstitutionalization movement of the 1960s led to a significant shift in where individuals with serious mental illness (SMI) are housed and how they receive care (Davis et al., 2012). SMI affects approximately 6% of adults and is characterized by severe functional impairment and limitations in major life activities (National Institute of Mental Health, 2024). While deinstitutionalization aimed to create more humane community-based care, chronic underfunding and fragmentation have created persistent barriers for individuals with SMI accessing consistent support.
Psychosis, characterized by some loss of contact with reality, including delusions, hallucinations, and disorganized thoughts and behaviors (National Institute of Mental Health, 2023), can be a presentation among individuals with SMI who experience homelessness, limited care access, or crisis situations. As a result, police officers may be called upon to respond to increasing behavioral health emergencies (Abramson, 2021). These calls are often in the absence of any criminal activity, with prior research indicating that only 15% of behavioral health crisis calls involve chargeable offenses (Petreca, Uveges, et al., 2025), representing a significant misalignment between traditional police scope and current utilization. Once deployed, police encounters with individuals experiencing psychosis have at times historically resulted in poor outcomes, including incarceration, frequent emergency department (ED) visits, and involuntary holds or hospitalization in a system not designed to provide treatment (Massachusetts Health Policy Commission, 2025).
Data also demonstrate that individuals with mental illness are overrepresented in carceral environments at rates at least three times higher than the general population (Substance Abuse and Mental Health Services Administration, 2024) and may face increased risk of death during police encounters (Fuller et al., 2015). Mental health jail diversion programs (JDP) aim to determine the most appropriate response to behavioral health crises, whether that involves linkage to community-based treatment, hospital-based care, de-escalation at the scene, or, when warranted, criminal justice processing. These programs shift the focus from default criminal justice processing toward more tailored intervention (Bonfine et al., 2024). Because police play a central role in deciding outcomes, including ED diversions and involuntary holds or hospitalizations (Petreca, Barros, et al., 2025), their decisions carry important implications for clinical practice broadly and psychiatric nursing specifically, where providers often engage at the intersection of law enforcement and post-crisis care systems (Petreca et al., 2024).
Background and Significance
Individuals with psychosis face significant barriers to initiating and maintaining mental health treatment (Corrigan et al., 2014), with gaps in care contributing to crises. Given their 24/7 availability, police are frequently the first point of contact for behavioral health crises (Abramson, 2021). Approximately 20% of police calls involve mental health needs (Abramson, 2021), with one in 10 individuals with mental illness encountering police in their care pathway (Livingston, 2016). Police interventions may be limited at times to ED transport or arrest, leaving gaps where individuals may be deemed safe but have significant unmet needs, leading to repeated police interactions (Bonfine et al., 2014; Watson et al., 2008). Treatment standards are often tied to dangerousness rather than need or disability (Dempsey et al., 2020), with ED-initiated care having limitations for long-term stability (Balfour et al., 2022).
Among those with SMI, psychosis is the symptom most likely to lead to criminal justice involvement (Cummings et al., 2020; Morgan et al., 2020), with individuals with psychotic disorders at higher risk of repeat arrests (Magee et al., 2021). Research on first-episode psychosis (FEP) shows individuals are more likely to have police contact and criminal charges, with studies reporting 17% to 37% incarcerated during untreated psychosis periods, causing treatment delays (Schumann et al., 2017). Among those incarcerated during the duration of untreated psychosis, approximately three-fourths (76%) were detained for a non-violent, often petty crime, which was defined as possession of illicit substances, driving violations, shoplifting, jaywalking, loitering, or child neglect (Wan et al., 2014).
Even when diverted from jail, individuals with psychosis are more likely to enter expensive inpatient pathways (Cheung et al., 2014; Substance Abuse and Mental Health Services Administration, 2023) and face challenges transitioning to outpatient care (Walker et al., 2019). Individuals with psychosis are twice as likely to be hospitalized involuntarily versus voluntarily (Walker et al., 2019). Police officers express a desire to refer individuals with psychosis to treatment earlier, before meeting acute dangerousness criteria (Dempsey et al., 2020). The protracted time between identifying psychosis and connecting to treatment causes harm and reinforces stereotypes about psychosis and violence risk (Fisher et al., 2006).
The Sequential Intercept Model identifies critical decision points for diverting individuals from criminal justice toward treatment (Munetz & Griffin, 2006). Intercept 0 involves community crisis services before law enforcement. Intercept 1 begins when police encounter individuals in crisis and decide between arrest or diversion, connection to community resources, or ED transport. This study focuses on Intercept 1 interventions, examining factors associated with police decision-making during behavioral health emergencies to optimize crisis response protocols.
Gaps in Knowledge
Behavioral health crises have become an increased driver of police encounters, and there has been increased implementation of diversion programs to try to meet these needs. However, analyzing the data to evaluate diversion practices and outcomes is a nascent area of study (Hailemariam et al., 2025; Petreca, Barros, et al., 2025). A lack of strong communication and coordination among components of the mental health and criminal justice systems further confounds the ability to appreciate patterns or enhance data-driven decision-making. Psychosis appears to be a risk factor for engagement with the criminal justice system, with individuals experiencing psychotic disorders demonstrating higher rates of arrest and repeat criminal justice contact compared with those with other mental health conditions (Cummings et al., 2020; Magee et al., 2021; Morgan et al., 2020). There is limited literature that specifically evaluates the impact of individuals experiencing a behavioral health crisis with or without psychosis, and how that impacts their trajectory. It is not known how presenting with psychosis versus other mental health symptoms affects police decision-making and ultimately may impact disposition. Furthermore, it is not yet clear what other factors contribute to police-led jail and ED diversions among those presenting with and without psychosis.
Study Objective and Significance
This study examined crisis intervention outcomes within police-led jail diversion programs, emphasizing differences between individuals with and without psychotic presentations. Our primary research question was: What demographic, clinical, and operational factors predict jail diversion, ED diversion, and involuntary hold outcomes among individuals presenting with psychotic symptoms during police-led crisis interventions? Our secondary question explored: How do these predictive factors and outcome patterns differ between individuals with psychotic presentations and those experiencing non-psychotic behavioral health crises?
Method
Study Design
This research employed a retrospective cohort design utilizing secondary data analysis to examine behavioral health crisis interventions conducted within jail diversion programs, with particular focus on comparing outcomes between individuals presenting with identifiable psychotic symptoms and those without such presentations.
Data Collection
Data were obtained from the Massachusetts Department of Mental Health’s (DMH) centralized jail diversion programs (JDP) reporting system, which maintains comprehensive records of all crisis interventions conducted by state-funded programs throughout Massachusetts.
The Massachusetts DMH requires systematic documentation of all JDP encounters through a standardized electronic reporting platform. This database captures detailed information regarding individual demographics, clinical presentations, incident characteristics, and intervention outcomes using structured drop-down fields that constrain data entry and ensure completeness across all participating programs, reducing the potential for missing or inconsistent documentation. Data collection occurs close to real-time following each crisis response, with entries completed by trained JDP personnel or designated program staff members. All participating programs operate primarily under pre-booking diversion frameworks, wherein individuals are redirected from the criminal justice system prior to formal charging procedures.
Sample and Study Period
The analysis covered JDP encounters recorded between April 2023 to January 2025, an observation period during which 155 state-supported JDPs were operational across Massachusetts. The initial dataset contained 50,062 individual crisis encounters captured within the DMH database. To ensure analytical rigor and data completeness, the inclusion criteria required complete documentation across all essential variables of interest. Following systematic review and data validation procedures, the final analytical sample comprised cases with comprehensive records suitable for examining the relationship between psychotic presentations and diversion outcomes.
Geographic representation within the sample included urban jurisdictions (33.7%), suburban communities (48.5%), and rural areas (13.1%), ensuring broad representation across diverse service environments. The majority of programs (n = 142) operated in partnership with municipal law enforcement agencies, while one program collaborated with the Massachusetts State Police. Crisis encounters became JDP-eligible through multiple pathways, including emergency dispatch calls, direct law enforcement contact, and referrals from program coordinators or community partners. The study protocol received approval from the institutional review board at Boston College.
Operational Framework and Decision-Making Authority
Within the Massachusetts JDP system, final determination regarding arrest versus diversion rests exclusively with responding law enforcement officers, regardless of program model or clinician involvement. In co-response configurations where mental health professionals accompany officers to crisis scenes, clinicians provide consultation regarding behavioral health needs and community resources, yet police officers maintain ultimate decisional authority regarding disposition outcomes. This operational structure reflects established protocols that preserve law enforcement’s statutory responsibilities while incorporating clinical expertise to inform intervention strategies.
Programs included in this analysis operate exclusively at Sequential Intercept Model Level 1, providing true pre-booking diversion without requiring criminal charges or court involvement. Individuals successfully diverted through these programs avoid formal entry into the criminal justice system and do not acquire criminal records associated with the presenting incident.
Variable Definitions and Measurement
Analytical Framework and Group Classification
To examine how behavioral health crisis outcomes differ across diagnostic presentations, we employed a stratified analytical approach. We divided the dataset into two distinct subsamples based on presenting concern: one for individuals with psychotic symptoms and one for those without. This stratification allowed us to investigate whether the predictors of diversion and hospitalization outcomes differ meaningfully between these groups.
Psychosis Classification
The dataset permitted multiple presenting concerns to be selected per case. Individuals were classified into the psychosis group if psychotic symptoms such as hallucinations, delusions, or disorganized thought were documented, regardless of co-occurring diagnoses such as mood disorders, substance use, or developmental conditions. All remaining individuals—those for whom psychosis was not selected in any form—were assigned to the non-psychosis group. This binary classification ensured that the psychosis group represented any case where psychotic features were present, while the comparison group was entirely free of psychotic indicators. Presenting concerns were documented by the lead responder on scene, either the mental health professional in co-response encounters or the Crisis Intervention Team (CIT)-trained officer in law enforcement-only responses.
Outcome Variables
Three primary outcome measures were examined to provide a comprehensive understanding of diversion patterns. Jail diversion was defined as incidents involving potential criminal charges where the individual was redirected to community-based services rather than arrested and processed through the criminal justice system. ED diversion represented cases where individuals were connected to alternative behavioral health resources instead of being transported to hospital EDs for psychiatric evaluation. Involuntary hold included instances where individuals were transported to inpatient psychiatric facilities under civil commitment laws, based on determinations of imminent risk or inability to engage in voluntary care.
Control Variables
Control variables encompassed multiple domains relevant to crisis intervention outcomes. Responder configuration captured whether the call involved a co-response team pairing mental health clinicians with law enforcement officers, or CIT-trained officers responding independently. Referral sources documented the pathway through which the crisis came to program attention, including emergency dispatch calls, agency referrals, self-referrals, or alternative sources. Assessment location specified where the individual was evaluated, such as their residence, public settings, police stations, or other locations.
Demographic characteristics included age, sex, race, and ethnicity. Clinical factors encompassed documented substance use history, including past or present substance use patterns. The nature of call variable captured behavioral indicators that prompted the crisis response, such as disorganized behavior, suicidal ideation, or aggressive presentations. Prior police history indicated whether the individual had a documented history of criminal charges or arrests. Temporal factors included time of day, categorized by shift periods such as day, evening, and overnight hours. For encounters involving potential criminal charges, offense severity was categorized using Massachusetts legal classifications ranging from minor infractions to serious felonies.
Data Processing and Preparation
The standardized data entry platform requires complete documentation across all fields before an encounter record can be saved, ensuring a dataset free of missing values. One-hot encoding transformations, a method of converting categorical variables into binary indicator variables suitable for regression modeling, were applied to categorical predictors. This process utilized pandas and numpy libraries within the Python programming environment to ensure efficient data manipulation and numerical computation.
Statistical Analysis
All statistical analyses were conducted using Python 3.8 with scikit-learn version 1.6.1, statsmodels version 0.14.4, scipy version 1.16.0, pandas version 2.1.1, and numpy version 1.26.0. Given the binary nature of the outcome variables, logistic regression was selected as the primary analytical approach. To account for the clustered structure of observations within JDP locations, we implemented a mixed-effects logistic regression model with location specified as a random effect. We supplemented our model with additional machine learning techniques to capture complex interaction effects that traditional regression methods might not adequately address. The unit of analysis was the crisis encounter rather than the individual. Three separate models were developed corresponding to each outcome variable: jail diversion, emergency department diversion, and involuntary hold. This approach allowed for examination of how psychotic presentations are associated with different aspects of crisis response decision-making. Fixed effects included the variables most relevant to our research question, which were entered into the model as predictors of the outcome.
Following separate model development for each population, comparative analysis examined differences in predictor significance, effect sizes, and model performance between the psychosis and non-psychosis groups to identify distinct patterns in crisis intervention decision-making. This comparative framework allowed us to assess whether demographic, clinical, and operational factors were associated with outcomes differently across the two populations.
Multicollinearity assessment was conducted through correlation matrix analysis and variance inflation factor (VIF) calculations to ensure model stability and interpretability. Variables exhibiting VIF values exceeding 5.0 were carefully evaluated for adjustment or exclusion to maintain analytical rigor. Model performance evaluation incorporated multiple metrics, including accuracy, precision, recall, F1 scores, and receiver operating characteristic curve analysis to comprehensively assess predictive capability and clinical utility.
The analytical framework accommodated the full spectrum of crisis encounters, recognizing that diversion considerations apply differently based on incident characteristics and legal factors. For cases involving potential criminal charges, offense severity was modeled as a categorical predictor to test its interaction with psychotic presentations on diversion outcomes. This comprehensive approach ensured robust examination of the research questions while maintaining analytical precision and clinical relevance.
Results
Sample Characteristics
The dataset comprised 50,062 crisis intervention encounters captured within the Massachusetts DMH jail diversion program database from April 2023 to January 2025. Of these, 11,401 encounters (22.8%) involved individuals presenting with identifiable psychotic symptoms, while 38,661 encounters (77.2%) involved individuals experiencing non-psychotic behavioral health crises (Table 1).
Sample Characteristics of Police-Led Crisis Encounters by Psychosis Status.
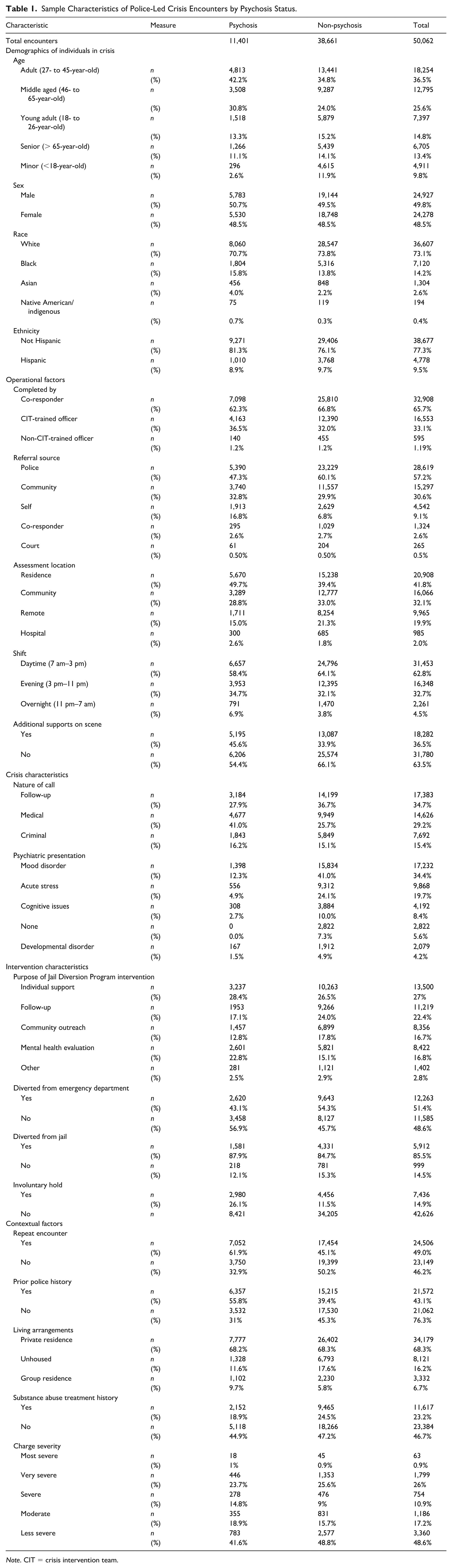
Note. CIT = crisis intervention team.
Descriptive comparisons between groups revealed several key differences in demographic and operational characteristics. Individuals in the psychosis group were more likely to be aged 27 to 65 and more frequently had prior police contact (55.8% vs. 39.4%) and repeat encounters (61.9% vs. 45.1%) than those without psychotic symptoms. The psychosis group also had higher rates of medical-related call types and was more often assessed at their residence (49.7%) compared with the non-psychosis group (39.4%), who were more likely to be assessed in community settings (33.0%).
Notable differences also emerged in intervention outcomes. Among encounters involving chargeable offenses, individuals with psychotic presentations were slightly more likely to be diverted from jail (87.9%) compared with those in the non-psychosis group (84.7%). Emergency department diversion was also less frequent in the psychosis group (43.1%) than in the non-psychosis group (54.3%). Conversely, involuntary hold was more than twice as common among those with psychotic symptoms (26.1%) relative to those without (11.5%).
These descriptive patterns highlight important baseline differences that inform the multivariate regression models that follow, which examine the distinct factors associated with each crisis intervention outcome across the two groups.
Crisis Intervention Outcomes: Psychotic Presentation Group
Logistic regression analysis identified key predictors of crisis intervention outcomes among individuals presenting with psychotic symptoms. The results demonstrate distinct patterns of association across the three outcome measures, with assessment location, purpose of intervention, and clinical factors emerging as primary factors linked to decision-making (Table 2).
Predictors of Jail Diversion, Emergency Department Diversion, and Involuntary Hold for Encounters Involving Individuals Presenting With Psychosis.
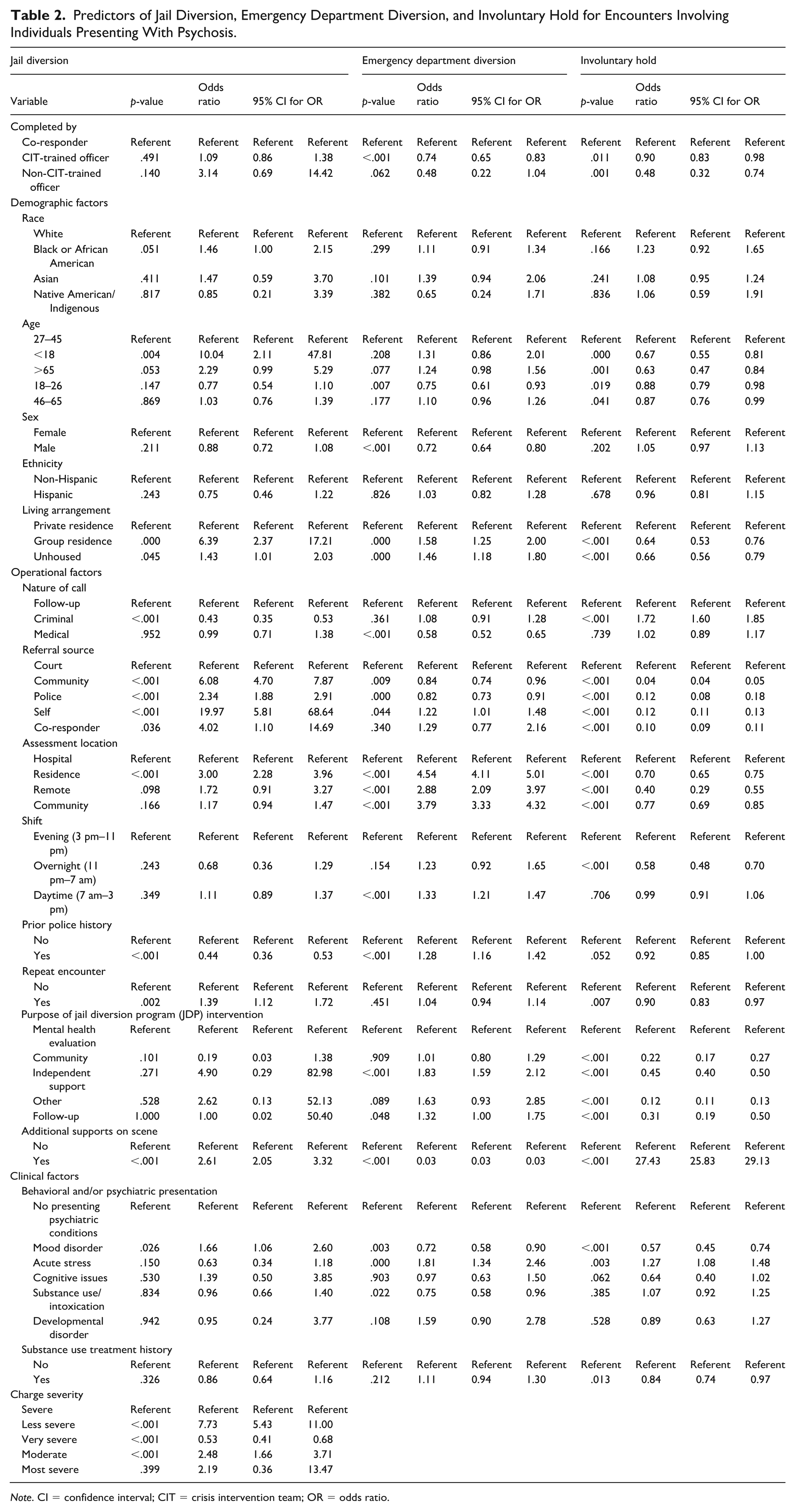
Note. CI = confidence interval; CIT = crisis intervention team; OR = odds ratio.
Emergency Department Diversion
Assessment location emerged as the strongest predictor of ED diversion among individuals with psychotic presentations. Residence-based assessments (OR = 4.54, 95% CI [4.11, 5.01], p < .001) and community-based assessments (OR = 3.79, 95% CI [3.33, 4.32], p < .001) were strongly associated with increased diversion likelihood. Independent support purpose (OR = 1.83, 95% CI [1.59, 2.12], p < .001) and follow-up purpose (OR = 1.32, 95% CI [1.00, 1.75], p = .048) also showed positive associations.
Factors that decreased the likelihood of ED diversion included additional supports on scene, such as fire department or emergency medical services (EMS; OR = 0.03, 95% CI [0.03, 0.03], p < .001), CIT-trained officer involvement (OR = 0.74, 95% CI [0.65, 0.83], p < .001), and male sex (OR = 0.72, 95% CI [0.64, 0.80], p < .001).
Jail Diversion
Among individuals with psychotic presentations and chargeable offenses, charge severity was the dominant predictor. Less severe charges (OR = 7.73, 95% CI [5.43, 11.00], p < .001) and moderate charges (OR = 2.48, 95% CI [1.66, 3.71], p < .001) showed strong positive associations with diversion. Self-referral (OR = 19.97, 95% CI [5.81, 68.64], p < .001) and minor status (OR = 10.04, 95% CI [2.11, 47.81], p = .004) were also associated with higher diversion likelihood. Conversely, criminal-related calls (OR = 0.43, 95% CI [0.35, 0.53], p < .001) and prior police history (OR = 0.44, 95% CI [0.36, 0.53], p < .001) reduced diversion odds.
Involuntary Hold
The presence of additional supports on scene was the most robust predictor of involuntary hold (OR = 27.43, 95% CI [25.83, 29.13], p < .001). Protective factors included encounters focused on individual support (OR = 0.45, 95% CI [0.40, 0.50], p < .001), follow-up encounters (OR = 0.31, 95% CI [0.19, 0.50], p < .001), self-referrals (OR = 0.12, 95% CI [0.11, 0.13], p < .001), and minor status (OR = 0.67, 95% CI [0.55, 0.81], p < .001).
Crisis Intervention Outcomes: Non-psychotic Presentation Group
Predictive patterns among individuals experiencing non-psychotic behavioral health crises demonstrated both similarities and notable differences compared with the psychotic presentation group. Assessment location again emerged as a critical predictor, while charge severity showed even stronger associations with diversion outcomes in this population (Table 3).
Predictors of Jail Diversion, Emergency Department Diversion, and Involuntary Hold for Encounters Involving Individuals Presenting Without Psychosis.
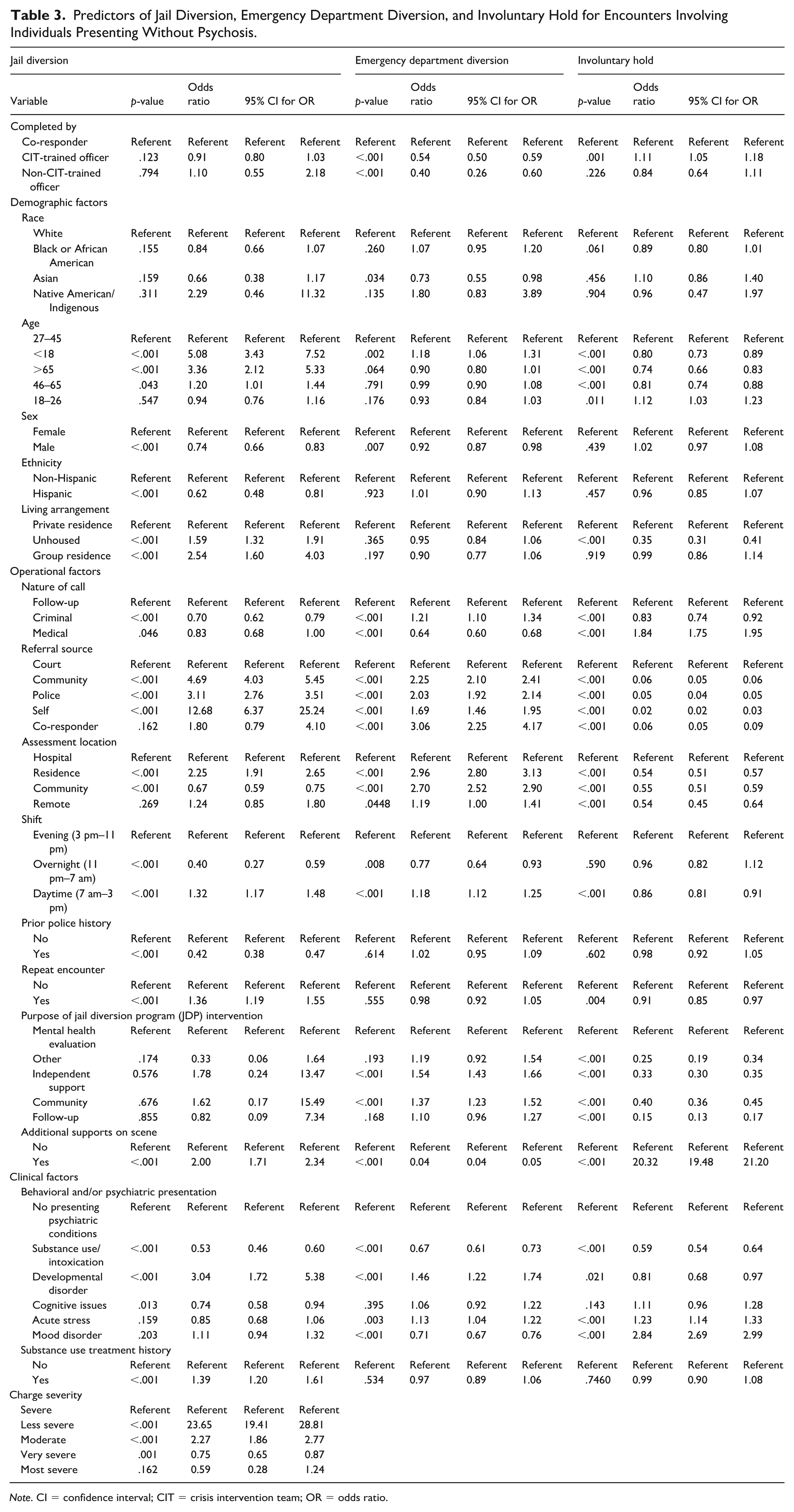
Note. CI = confidence interval; CIT = crisis intervention team; OR = odds ratio.
Emergency Department Diversion
As in the psychosis group, assessment at residence (OR = 2.96, 95% CI [2.80, 3.13], p < .001) and in community settings (OR = 2.70, 95% CI [2.52, 2.90], p < .001) were highly associated with diversion. Other positive predictors included independent support purpose (OR = 1.54, 95% CI [1.43, 1.66], p < .001) and co-responder referral (OR = 3.06, 95% CI [2.25, 4.17], p < .001). Negative predictors included additional supports on scene (OR = 0.04, 95% CI [0.04, 0.05], p < .001), CIT-trained officer involvement (OR = 0.54, 95% CI [0.50, 0.59], p < .001), and mood disorder (OR = 0.71, 95% CI [0.67, 0.76], p < .001).
Jail Diversion
Charge severity had even stronger predictive power in the non-psychosis group. Less severe charges (OR = 23.65, 95% CI [19.41, 28.81], p < .001) and moderate charges (OR = 2.27, 95% CI [1.86, 2.77], p < .001) were associated with higher odds of diversion. Additional positive predictors of jail diversion included self-referral (OR = 12.68, 95% CI [6.37, 25.24], p < .001), senior age (>65; OR = 3.36, 95% CI [2.12, 5.33], p < .001), and developmental disorder (OR = 3.04, 95% CI [1.72, 5.38], p < .001). Prior police history (OR = 0.42, 95% CI [0.38, 0.47], p < .001) and overnight timing for the encounter (OR = 0.40, 95% CI [0.27, 0.59], p < .001) reduced the likelihood of diversion.
Figure 1 summarizes predictors of jail diversion for both psychosis and non-psychosis groups, highlighting the stronger role of charge severity in the non-psychosis group.
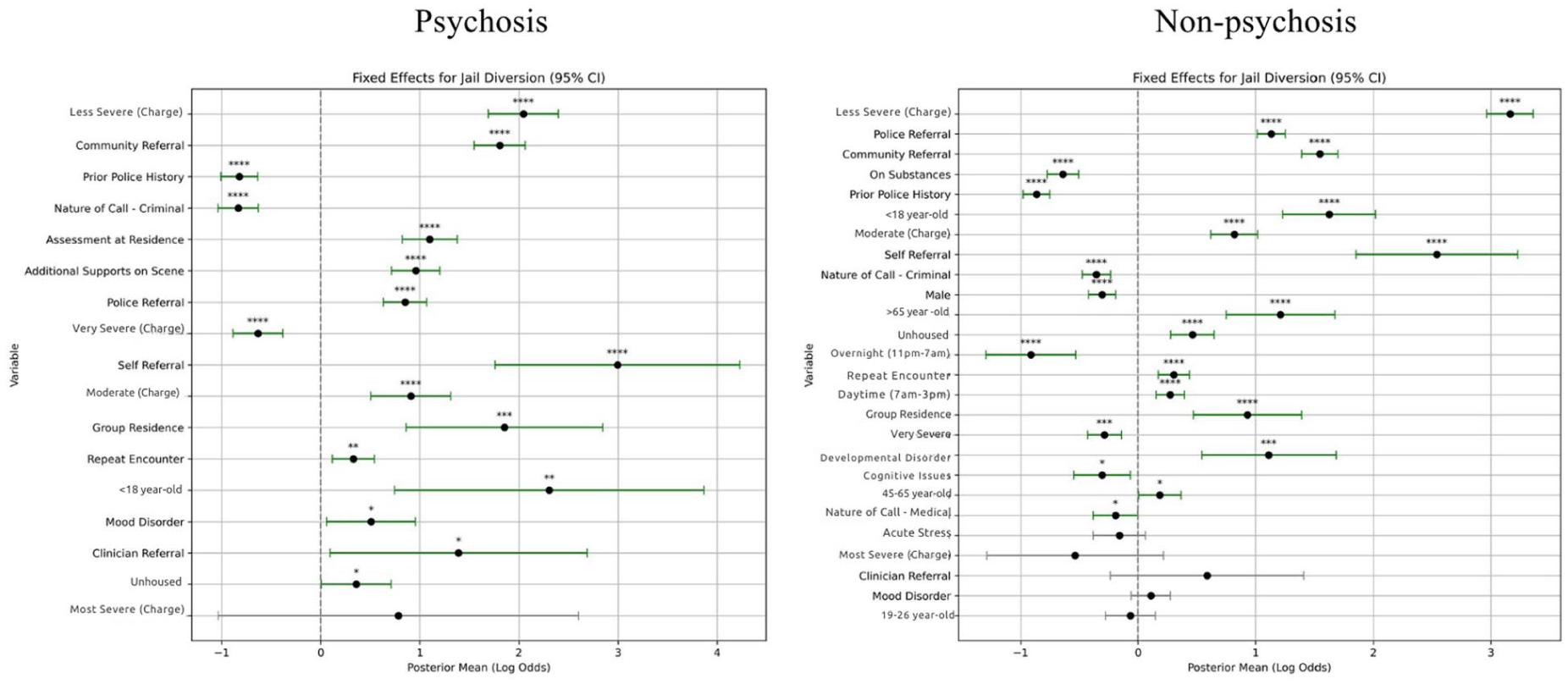
Predictors of jail diversion in police-led crisis encounters by psychosis status.
Involuntary Hold
Additional supports on scene again showed the strongest positive association (OR = 20.32, 95% CI [19.48, 21.20], p < .001), mirroring the psychosis group. Mood disorder was a stronger predictor of hospitalization in this group (OR = 2.84, 95% CI [2.69, 2.99], p < .001). Protective factors included follow-up purpose (OR = 0.15, 95% CI [0.13, 0.17], p < .001), independent support purpose (OR = 0.33, 95% CI [0.30, 0.35], p < .001), and homelessness (OR = 0.35, 95% CI [0.31, 0.41], p < .001). Age-related protective effects were consistent with those observed in the psychosis group.
Figure 2 presents predictors of involuntary hospitalization across groups. This shows the consistent influence of on-scene supports and the differential role of mood disorders.
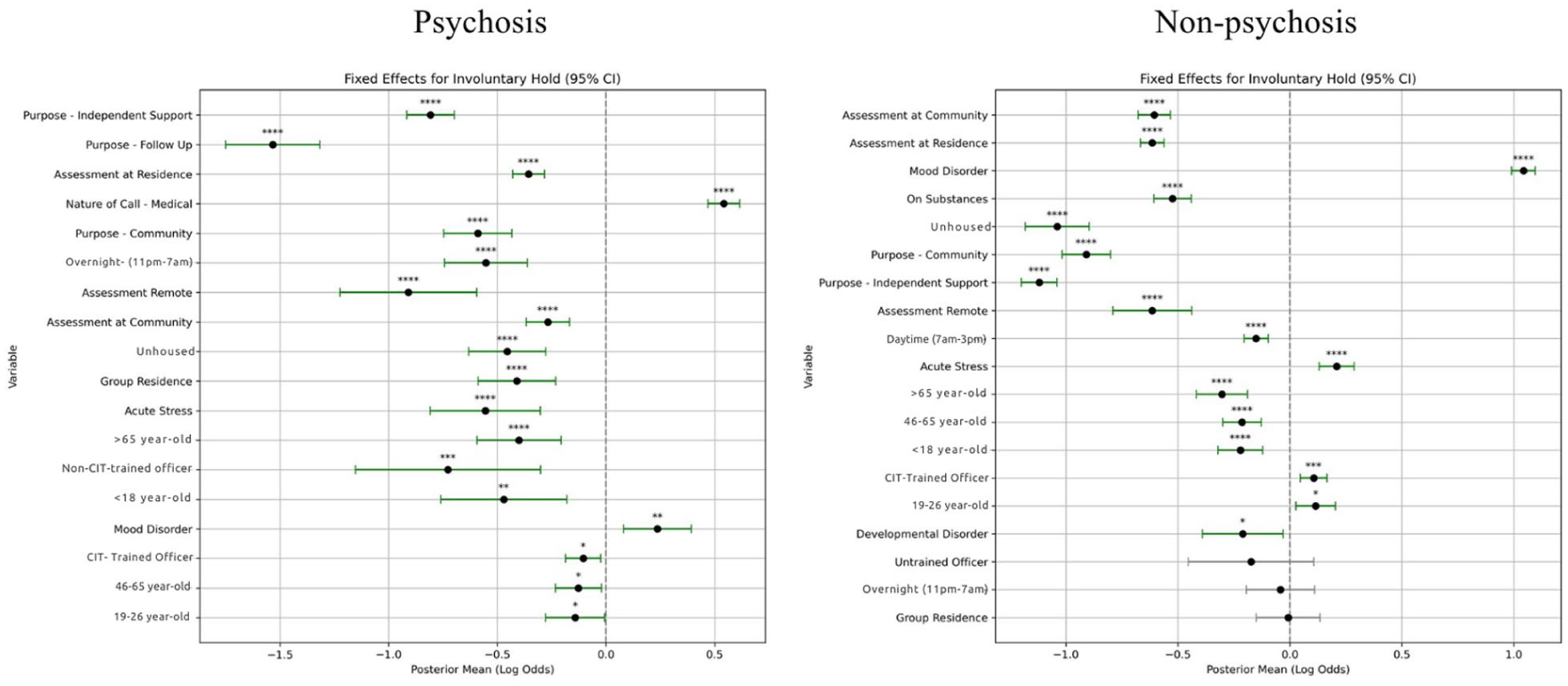
Predictors of involuntary hospitalization in police-led crisis encounters by psychosis status.
Discussion
The patterns revealed in our analysis demonstrate that crisis intervention outcomes in behavioral health emergencies involve complex interactions between psychiatric presentations, operational factors, and individual characteristics. Rather than any single variable determining intervention pathways, our findings show how different elements of the crisis response system are associated with variation in care decisions across distinct populations (Bonfine et al., 2014). These interactions help explain why certain approaches to crisis response are more likely to connect individuals with appropriate levels of care depending on their presenting symptoms.
This study examined key predictors of crisis intervention outcomes across three distinct pathways, highlighting the importance of population-specific approaches to behavioral health crises. These findings underscore the potential for enhanced collaboration among law enforcement, mental health professionals, and community services in ensuring individuals in crisis receive care appropriate to their clinical presentation (Watson & Fulambarker, 2012). By better understanding the factors linked to different intervention outcomes, these insights can inform practices that optimize crisis response effectiveness while reducing unnecessary reliance on restrictive interventions.
Key Predictors of Crisis Intervention Outcomes
A salient finding relates to the differential predictive strength of charge severity across psychiatric presentations. Less severe charges demonstrated stronger associations with jail diversion in the non-psychosis group compared with the psychosis group, suggesting that legal factors may operate as more definitive decision-making criteria for individuals without psychotic presentations, while clinical considerations assume greater prominence when psychotic symptoms are present. This pattern aligns with research demonstrating that crisis responders may perceive individuals with psychotic presentations as inherently higher risk regardless of offense severity (Corrigan et al., 2014; Watson et al., 2008). Given that nearly a quarter of all behavioral health calls in our sample involved psychotic presentations, this finding carries substantial impact.
Assessment location emerged as the most consistent predictor across both populations and all three outcomes. Residence-based and community-based assessments were strongly associated with ED diversion in both groups, while hospital-based assessments reduced diversion likelihood. This finding supports previous research emphasizing the importance of conducting assessments in familiar environments and reflects broader principles of recovery-oriented care that prioritize maintaining individuals in their natural environments when clinically appropriate (Compton et al., 2014; Price et al., 2015; Steadman et al., 2000).
The complex relationship between mood disorders and crisis intervention outcomes revealed important differences across populations. While mood disorders showed negative associations with ED diversion in both groups, they demonstrated a stronger association with involuntary hold in the non-psychosis group, where mood disorder more likely serves as the primary clinical indicator of acute risk. In the psychosis group, mood disorder operated as a comorbidity within an already-defined presentation, which may attenuate its independent association with the outcome. These differences likely reflect varying clinical decision-making thresholds across diagnostic contexts rather than inconsistent practice (Fisher et al., 2006; Morabito et al., 2012).
According to our data, the presence of additional supports on scene consistently predicted involuntary hold across both populations. While this finding may reflect appropriate escalation of care in genuinely higher acuity situations, it could also indicate patterns where the presence of EMS is linked with more restrictive intervention decisions. This relationship suggests that current protocols may inadequately distinguish between EMS presence as an indicator of severity versus situations where alternative community-based interventions might be appropriate. The retrospective design of this study cannot determine whether EMS presence reflects encounter acuity, influences decision-making toward more restrictive interventions, or both, and this warrants examination in future prospective work (Scott, 2000; Trivedi et al., 2019).
Implications for Crisis Response Programs
Our analysis revealed that encounters involving CIT-trained officers were associated with lower rates of ED diversion across both populations. These findings warrant further investigation to understand the contextual factors that may shape diversion outcomes when CIT-trained officers respond to behavioral health crises. This pattern may reflect heightened caution in assessment decisions, concerns about liability, or defensive decision-making practices that emerge from increased awareness of potential complications (Bailey et al., 2018; Canada et al., 2012). This may also reflect a combination of increased awareness of mental health treatment needs alongside inadequate alternative care options in the community (Dempsey et al., 2020). These factors could lead officers to err on the side of caution when making diversion decisions, despite their specialized training.
The difference in diversion patterns likely reflects both the varying clinical complexity across psychiatric presentations and the need for ongoing refinement of crisis intervention protocols to optimize assessment and diversion decisions. Enhanced training in clinical decision-making frameworks that balance risk assessment with therapeutic intervention principles may improve outcomes while maintaining appropriate safety considerations (Ellis, 2014; Shapiro et al., 2015). While CIT training provides officers with valuable skills for communication and management of behavioral health crises, comprehensive clinical assessment remains within the specialized expertise of health care professionals (Dempsey et al., 2020). This recognition supports the development of collaborative response models that leverage the distinct strengths of both law enforcement and clinical professionals while maintaining clear role boundaries that optimize outcomes for individuals in crisis (Barros & Petreca, 2025).
Our examination of referral sources revealed that self-referral consistently predicted favorable diversion outcomes across both populations. This finding suggests that individuals who initiate contact themselves may be more amenable to community-based interventions and may present with different risk profiles compared with those who come to attention through law enforcement or involuntary mechanisms. Programs that facilitate direct access to crisis services may achieve better outcomes than those relying primarily on law enforcement-initiated contact (McKenna et al., 2015; Substance Abuse and Mental Health Services Administration, 2014). On the other hand, prior police contact or encounters were negatively associated with diversion, and this further highlights the need for individuals to have access to 24/7 non-police-based behavioral health crisis resources for self-referral. This is also consistent with emerging work on how to best intervene at the point of the 911 call to reroute lower-risk behavioral health crises rather than deploying police officers (Massachusetts Association for Mental Health–Technical Assistance Collaborative, 2023). Analyzing data to support specialized dispatch tracking, particularly among high utilizers of emergency services or to identify locations with clusters of behavioral health crisis calls, are other ways to proactively address individual and community needs (Tentner et al., 2019; US Department of Justice, 2023). Collaboration with co-responders and outpatient care clinicians, with individuals’ consent, can further help identify best practices to meet individual needs in terms of communication and crisis response planning. Specialized dispatch tracking may be especially valuable for those with psychosis, who often have unique communication needs and, in our dataset, were more likely to be assessed at their residence.
The demographic patterns in our findings were notable, with age-related factors consistently showing protective effects against involuntary hold or hospitalization across both populations. Individuals aged 27 to 45 were more likely to be involuntarily hospitalized than any other age group, regardless of psychotic versus non-psychotic presentation, suggesting that age considerations shape intervention decisions in ways that may reflect both clinical judgment and systematic biases (Walker et al., 2019). For crisis response programs, this underscores the need to support police officers in conducting comprehensive assessments to include individualized risk, behavioral, and medical health status, current needs, and means or supports to meet those needs in the least restrictive setting.
Practice Recommendations
Several factors related to crisis intervention outcomes underscore the need for more flexible community mental health resources. The substantial differences in predictive patterns between psychotic and non-psychotic presentations support the development of population-specific crisis intervention protocols rather than uniform approaches across all behavioral health emergencies (Draine et al., 2002; Munetz & Griffin, 2006). Such protocols would need to address the differential importance of legal and clinical factors across presentations while maintaining coordination throughout intervention pathways.
Appropriate management of behavioral health crises requires recognition that assessment location is significantly associated with outcomes across all populations. Once law enforcement is engaged, programs should prioritize developing capabilities for comprehensive assessments in residence and community settings rather than defaulting to hospital-based evaluations, particularly given the strong associations between residence and community assessments with favorable diversion outcomes. While CIT training already includes on-scene assessment components, our findings suggest that enhanced clinical consultation resources and structured decision-making tools could improve complex situations in community settings (Bailey et al., 2018; Wood et al., 2017).
The strong association between additional supports on scene and involuntary hospitalization warrants examination of how the presence of emergency medical services is associated with variation in crisis intervention decisions. The consistent pattern across both populations suggests that EMS involvement may signal higher acuity situations requiring immediate medical attention, but it may also reflect systematic patterns where medical presence drives decisions toward hospital-based interventions regardless of whether less restrictive alternatives might be appropriate. Training protocols should address how to effectively coordinate between law enforcement and EMS while maintaining focus on least restrictive intervention principles (Bratina et al., 2020; Zun, 2012). This could include enhancing existing CIT training with interdisciplinary case scenarios with EMS and police, including individuals with and without psychosis. Psychiatric nurses are well-positioned to improve outcomes in these areas given their expertise in both medical and mental health assessment (Allen et al., 2014; Kracher et al., 2022), through several potential mechanisms, such as inclusion in co-response teams, expanded consultation roles within 24/7 crisis and emergency response systems, and contributions to training police and EMS.
Given that our findings indicate differential effects of charge severity across populations, training programs should emphasize decision-making frameworks that account for the varying importance of legal, clinical, and operational factors across different symptom presentations. Our finding that prior police history reduced jail diversion likelihood among individuals with psychosis is consistent with research suggesting that a known criminal record increases the likelihood of arrest over diversion (Magee et al., 2021; Petreca, Uveges, et al., 2025). This underscores the value of enhanced collaboration between crisis intervention programs and community mental health services to support continuity of care. Enhanced clinical assessment and risk evaluation training for crisis responders could improve intervention determinations for individuals with psychotic symptoms, particularly when legal factors provide limited guidance for optimal outcomes (Compton et al., 2014; Rogers et al., 2019).
The patterns observed with CIT-trained officers suggest opportunities for enhanced clinical support within police-led crisis response teams. Co-response models that include clinical professionals alongside law enforcement may provide additional resources and expertise to support complex decision-making while building upon the valuable communication skills that CIT training provides (Yang et al., 2024). As mentioned above, psychiatric nurse practitioners serve a dual purpose, with the Nurse-Police Assistance Crisis Team model showing promise, as forensic nurses can evaluate both medical and psychiatric needs while navigating legal intersections, potentially providing the clinical expertise needed to support more confident diversion decisions (Balfour et al., 2022; Petreca et al., 2024). The differential outcomes observed between co-responder and CIT-only encounters in this dataset provide empirical support for models that integrate clinical expertise directly into police-led crisis response. For individuals presenting with psychosis specifically, where clinical and legal factors interact in complex ways, the presence of a clinician with expertise in both psychiatric and medical assessment may be particularly consequential for diversion outcomes (Petreca et al., 2024).
The differential impact of mood disorders on intervention outcomes across populations has particular relevance for crisis response training. The stronger association between mood disorders and involuntary hold in the non-psychosis group likely reflects its role as the primary clinical indicator of acute risk in that context, which is expected. Nonetheless, crisis responders may benefit from enhanced education regarding intervention options for mood-related crises, particularly in identifying when community-based alternatives can safely address acute distress without requiring involuntary commitment (Charette et al., 2014). Availability and awareness of alternatives, including behavioral health urgent centers, crisis stabilization units, and respites, are essential.
Resource availability is strongly linked to intervention choices, with EDs often serving as the default option when alternatives are unknown or lacking (Balfour & Zeller, 2023). This is particularly evident during overnight shifts when fewer specialized teams are available. Police need real-time access to clinical expertise and alternative resources across all shifts to optimize intervention outcomes. One option includes the integration of nursing expertise through co-response models or consultation mechanisms that could provide essential clinical support for complex decision-making, especially when traditional legal frameworks may be insufficient for determining appropriate intervention pathways (Petreca et al., 2024).
Strengths and Limitations
This study has several strengths, including a large dataset with standardized data entry from across Massachusetts, enhancing the reliability of the findings. Data were from diverse geographical areas comprising urban, suburban, and rural settings, increasing the generalizability of results within the state context. The stratified analytical approach represents a methodological advancement over previous studies that have treated psychiatric presentations as simple categorical variables (Clifasefi et al., 2013).
This study’s data offer valuable insights into crisis intervention dynamics within Massachusetts’ context of mental health resources, state policies, and crisis intervention programs. However, further research across other states with different mental health infrastructures and program designs would be beneficial to determine the generalizability of these findings (Newton et al., 2022). In addition, while this study provides statewide insights, local adaptations of crisis response protocols, jurisdictional resource availability, and variation in practice norms across settings were not captured by the data and may influence outcomes in ways that this analysis could not account for.
The classification of psychotic versus non-psychotic presentations relied on documentation by crisis response personnel, which may introduce variability in categorization that does not align with standardized diagnostic criteria. However, this approach may actually strengthen the ecological validity of the findings since these are the real-world conditions under which crisis intervention decisions are made (Staines et al., 2022). The cross-sectional nature of the data limits our ability to assess causal relationships between predictor variables and outcomes or examine long-term outcomes of individuals receiving different interventions.
Future Research Directions
Future research should explore the effectiveness of identified predictor variables in supporting successful crisis interventions and long-term outcomes by examining variables such as demographics, crisis types, resource availability, and responder characteristics through longitudinal studies (Nick et al., 2022). Investigating differences within states, including urban, suburban, and rural classification alongside contextual variables like officer discretion, community attitudes toward mental health, and resource availability, could deepen understanding of how these elements shape intervention outcomes.
Systematic evaluation of police-led crisis intervention models, especially the expansion of co-response teams that include clinical expertise and alternative assessment approaches, is essential. Research examining models such as the Nurse-Police Assistance Crisis Team could provide additional valuable insights into how clinical expertise can be effectively integrated into police-led crisis response while maintaining public safety priorities (Petreca et al., 2024). Recent research has begun to identify specific predictors of ED diversion in police-led behavioral health responses, providing an empirical foundation for understanding when clinical consultation may be most beneficial (Petreca, Barros, et al., 2025). Knowledge of these predictors can be leveraged to develop additional training materials, including simulation and case scenarios mirroring particular municipalities’ needs (Watson et al., 2024). Strengthening collaboration between community mental health centers, clinical professionals, and law enforcement through targeted training may improve intervention outcomes, while research could identify population-specific factors affecting intervention success.
Qualitative research exploring the decision-making processes of crisis response teams could illuminate the mechanisms underlying the observed predictive patterns, particularly the relationship between emergency medical services presence and involuntary hold, given the consistent strength of this association across populations. Further research on communication and interdisciplinary teamwork between EMS, police officers, and co-responders may also enhance our understanding of factors associated with the functioning of police-led teams. Understanding how responders integrate clinical, legal, and operational considerations in real-time decision-making would inform more effective training protocols and decision-support tools that incorporate clinical expertise (Gillard et al., 2015).
Conclusion
This study demonstrates how specific characteristics of crisis incidents, psychiatric presentations, and available resources relate to intervention outcomes in police-led behavioral health crisis response. The findings highlight the significant differences in predictive patterns across populations and reveal areas for improvement in current crisis intervention strategies. The study underscores the need for a population-specific approach to crisis intervention that considers clinical presentations, timing of incidents, types of behavioral health concerns, and available community resources.
The results emphasize the importance of enhancing assessment capabilities within police-led crisis response, particularly in residential and community settings where favorable outcomes are more likely. Future interventions should focus on improving existing models associated with favorable outcomes and developing innovative approaches that incorporate clinical expertise to bridge gaps in current service provision. In addition, addressing disparities in intervention outcomes across different populations and improving coordination between law enforcement, clinical professionals, and community services are essential steps toward optimizing crisis response systems. As communities continue to address the intersection of law enforcement and behavioral health crises, these findings offer a foundation for evidence-based policy decisions and program improvements aimed at better serving individuals in crisis while ensuring appropriate intervention pathways based on clinical presentation and individual needs.
Footnotes
Acknowledgements
We thank Alison Perry and Emily Pudvah for their support in coordinating the research efforts. We also thank the Massachusetts Department of Mental Health, Jail Diversion Programs, for funding this study.
Author Contributions
All authors contributed to the conception or design of the study or to the acquisition, analysis, or interpretation of the data. All authors drafted the manuscript, or critically revised the manuscript, and gave final approval of the version that was submitted for publication. All authors agree to be accountable for all aspects of the work, ensuring integrity and accuracy.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Massachusetts Department of Mental Health, Jail Diversion Programs (PI: Victor G. Petreca).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.