
Abstract
Background:
Preceptors are vital in shaping the clinical education of psychiatric and mental health nurse practitioners (PMHNPs). A shortage of behavioral health providers has led to calls for increased capacity in PMHNP programs. Growing competition for sites and concerns for the recruitment and retention of qualified preceptors mean fewer placements.
Aims:
The purpose of this study was to identify motivations and barriers that current PMHNPs encounter when deciding to precept students. In addition, we aimed to analyze the relationship between demographic variables and the likelihood of precepting.
Methods:
The investigators developed and administered an online survey to collect demographic and other qualitative and quantitative data from 93 currently practicing PMHNPs, recruited via professional networks, nursing associations, and social media platforms. Data were analyzed in Qualtrics, and results were reported using descriptive statistics.
Results:
Common motivational themes include contributing to the future of the profession, mentorship, teaching, and maintaining a connection to academic faculty and institutions. Frequently cited challenges associated with precepting responsibilities included time constraints, competing clinical demands, paperwork and administrative burden, student professionalism, and lack of compensation for precepting work.
Conclusion:
Findings revealed a framework for creating incentives for precepting, including university perks, title, recognition, access, appreciation, organizational discounts, and a built-in compensation structure, with time reported as being most valuable. We developed an enhanced understanding and identified ways to improve the recruitment and retention of qualified preceptors in this field.
Keywords
Introduction
The United States is currently grappling with dual mental health crises, including an increase in reported mental health concerns and a historic shortage of mental health and substance use treatment providers (Sanders et al., 2023). As of December 2025, the Health Resources and Services Administration (HRSA) reported that 40% (137 million) of Americans live in a mental health professional shortage area (HRSA, 2025).
This shortage isn’t evenly distributed across the nation. A staggering 31% of urban centers have no psychiatric nurse practitioners (HRSA, 2025). This disparity means that many individuals seeking help are left without access to the care they desperately need.
As a result, fewer than half of those who reach out for behavioral health services receive any treatment. In some regions, that figure sinks to less than a quarter, leaving countless individuals without the support necessary for their mental well-being (Sanders et al., 2023).
The repercussions of this shortage are dire. Increased rates of suicidality among both youth and adults have been directly linked to the lack of available mental health services (Garnett & Curtin, 2023). As the country faces a growing behavioral health crisis, particularly among young people, the demand for services is consistently outpacing the supply. This makes the shortage of mental health professionals a pressing public health concern that requires immediate attention and a call to train more mental health professionals to meet demand. Schools of Nursing are attempting to fill gaps in care by training more psychiatric and mental health nurse practitioners (PMHNPs) and other advanced practice registered nurses (APRNs) to meet this need (American Association of Colleges of Nursing [AACN], 2025).
Preceptors, highly skilled and trained nursing professionals who provide practical, real-world, hands-on clinical training to future APRNs, are a vital part of the mandatory hands-on training in all PMHNP programs. By bringing students into their practices and acting as teachers, coaches, role models, facilitators, and supervisors, preceptors help to develop safe, competent, skilled clinicians (Chan, Baker, et al., 2025).
Since the COVID-19 pandemic, methods of delivering mental health care have changed. According to the American Hospital Association (AHA), the use of telehealth services for mental health spiked to roughly 40% to 50% of visits in 2020 and has remained high, with data indicating that 67% of mental health visits still occurred via telehealth through 2024 (AHA Center for Health Innovation, 2026). As a result, teleprecepting, another effective training method for educating nurse practitioner (NP) students across a variety of specialties, is frequently sought by schools of nursing in mental health tracks. Teleprecepting PMHNP students follows similar principles as in-person teaching, with prescribed modifications for transition to the virtual environment (Johnson et al., 2022). Because teleprecepting is an innovative, convenient, and highly desirable method of clinical education for PMHNP students, the availability of preceptors is further hindered by programs competing for placements.
The role of preceptors in advanced practice psychiatric and mental nursing education is crucial to maintaining robust APRN programs. The shortage of PMHNP providers and of qualified clinical preceptors has led to increased competition for clinical sites available for student placement in PMHNP programs (Hawkins, 2019; McInnis et al., 2021). As a result, thousands of students are turned away from quality programs in a profession where an ongoing shortage of clinical sites has translated into severely limited access to mental health care services (Watanabe, 2025).
The shortage of clinicians, particularly psychiatrists and PMHNPs, significantly affects health care access and the quality of mental health services. Projections by the National Alliance on Mental Illness (NAMI) indicate that the supply of adult psychiatrists may decrease by 20% by 2030, while demand is expected to rise by 3%, resulting in a shortage of over 12,000 psychiatrists (NAMI, 2025). This situation is further exacerbated by escalating mental health needs, worsened by the COVID-19 pandemic (NAMI, 2025). According to the Centers for Disease Control and Prevention (CDC, 2025), a mental health crisis is evident, with increasing unmet behavioral health needs across all age groups.
HRSA (2025) reports that only 39% of U.S. counties have an adequate number of mental health professionals, particularly in rural and underserved areas. Notably, 60% of rural communities are designated as mental health professional shortage areas (HPSAs), often lacking any mental health providers. These shortages lead to increased waiting times for mental health evaluations, sometimes extending for weeks or months (McNeely et al., 2022). This delay can escalate mental health crises and result in diminished quality of care, characterized by inadequate treatment options and increased reliance on emergency services. In addition, the overburdened workforce experiences high rates of burnout, with nearly 75% of clinicians reporting job dissatisfaction (Shanafelt et al., 2025). According to the most current data in HRSA’s State of the Behavioral Healthcare Workforce, there were 39,354 psychiatric advanced practice registered nurses, 3,224 psychiatric physician assistants, and 52,164 psychiatrists in practice in 2025, highlighting the pressing need for solutions to address these supply and distribution challenges (HRSA, 2025).
Schools of nursing have been incentivized to increase enrollment in PMHNP programs, partnering with government agencies to offer scholarships, grants, and loan-repayment opportunities (Last et al., 2024). However, while programs continue to expand enrollment, the shortage of clinical sites and preceptors remains a barrier to admission (Gonzalez & Eckhardt, 2024). According to the American Association of Colleges of Nursing (AACN), more than 80,000 qualified applications were rejected from schools of nursing in 2024, in part due to an insufficient supply of clinical placements (AACN, 2025). This lack of sites is a cyclical problem: With the provider shortage, there is growing concern about the recruitment and retention of qualified preceptors, which, in turn, limits the profession’s ability to expand access during a critical shortage.
Large online APRN programs have further complicated the preceptor’s capacity for clinical education. In remote learning environments, students may not have direct access to a nursing professor to address issues that arise when a student is confused, underperforming, or facing a personal challenge that affects the quality of the required work. Preceptors can also experience inadequate support and feel disconnected from an online institution (Bradshaw et al., 2021). Many preceptors lack academic experience in clinical education methods and may not fully understand their significance or their role as clinical instructors (National Advisory Council on Nurse Education and Practice, 2021).
The impact on schools of nursing’s ability to compensate by increasing enrollment in PMHNP programs is ongoing. In 2023, in the United States, nursing schools rejected nearly 66,000 qualified applications for bachelor’s and graduate nursing programs (AACN, 2024). In California that same year, only about 1,900 were accepted into graduate nursing programs (California Board of Registered Nursing [CA BRN], 2024). As evidenced by a pattern of rejection of qualified applicants and a limited number of graduates entering the field of behavioral health, perpetuating a lack of clinical sites (McInnis et al., 2021), the authors find it imperative to determine the etiology of the shortage of qualified preceptors and provide a comprehensive plan to recruit and maintain them.
Finding qualified preceptors for nurse practitioner students is one of the greatest challenges for NP programs (Doherty et al., 2020). A report by the National Organization of Nurse Practitioner Faculties highlights that the increasing number of NP programs does not align with the availability of qualified preceptors (Lofgren et al., 2021; McInnis et al., 2021). Many studies indicate a significant shortage of qualified preceptors for APRN students (Hawkins, 2019; Lofgren et al., 2021). There is limited research on why this shortage persists and how to mitigate it (Boyce et al., 2022), and a dearth of research on the shortage of PMHNP preceptors, despite a growing population of clinicians in this area. This study investigates ways to improve recruitment and retention of qualified PMHNP preceptors for APRN students by surveying practicing PMHNPs directly about their motivations for precepting or not precepting students.
Aim of This Study
This study aimed to explore the role of preceptorship among psychiatric APRNs by focusing on quantifying the motivations that encourage them to take on this responsibility, identifying the barriers that prevent behavioral health APRNs from precepting, and analyzing the relationship between demographic variables and the likelihood of engaging in preceptorship. By understanding these factors, we can gain insights into the incentives and challenges APRNs face in this critical educational role.
Methods
Design
This study used a cross-sectional design and collected data via an online survey.
Participants
The study targeted currently practicing PMHNPs, who were recruited through professional nursing organization email listservs and message boards, including the American Psychiatric Nurses Association (APNA) and the International Society of Psychiatric-Mental Health Nurses (ISPN). Additional recruiting was sent to administrative leaders of schools of nursing with PMHNP programs in the United States. The recruitment period spanned 6 weeks from July 1, 2025, through August 12, 2025.
Although the survey was distributed on U.S. and international online message boards, eligibility was limited to PMHNPs, and recruitment was open to all individuals meeting specific criteria. To be eligible to participate, respondents had to meet specific inclusion criteria: they must be actively practicing as PMHNPs in the United States and provide informed consent to participate in the study. Conversely, individuals were excluded from the study if they were retired PMHNPs. Retired nurses were excluded to maintain a focus on actively practicing professionals, thereby ensuring that the data reflect present-day workforce demands and factors contributing to the current shortage of preceptors.
This study was reviewed by the University of California, Los Angeles (UCLA) Institutional Review Board and was determined to be exempt from full review due to its minimal risk and use of anonymous survey methodology. Participation was voluntary, and informed consent was obtained electronically prior to survey completion.
Data Collection
Data were collected via an online Qualtrics survey distributed through the aforementioned channels. Prior to distribution, the survey underwent pilot testing to identify any issues with question clarity and technical functionality. This structured approach facilitated the collection of valuable data while ensuring a positive participant experience. Measures were implemented to protect participant anonymity and confidentiality. The survey began with a clear informed consent statement outlining the purpose of the study, participants’ rights, and contact information for the investigators.
The Qualtrics survey was organized into distinct sections. The survey instrument consisted of an initial set of nine items that collected demographic and employment-related characteristics. Respondents who indicated involvement in precepting were routed to an additional 10-item section specific to precepting. This section included both closed-ended and open-ended items, with free-text fields, to elicit qualitative insights into the perceived challenges and rewards of the precepting role.
Analysis
Text iQ was used to analyze the qualitative data collected on APRNs’ perceptions of precepting. Text iQ categorized responses as “very negative,” “negative,” “mixed,” “positive,” “very positive,” or “neutral.” Recurring key terms were identified and coded. Related concepts were grouped, leading to the emergence of themes.
Stats iQ was used to analyze quantitative data and summarize the frequencies and percentages of descriptive categorical variables. These categorical variables include gender, age, race/ethnicity, years of experience in practice and precepting, practice setting, and status of independent practice authorization.
Crosstabs iQ was used for descriptive analysis to explore patterns and distributions among categorical variables. Cross-tabulation of age groups with sentiments and scores of perceptions related to motivation and barriers to precepting was examined.
Results
Demographic Data
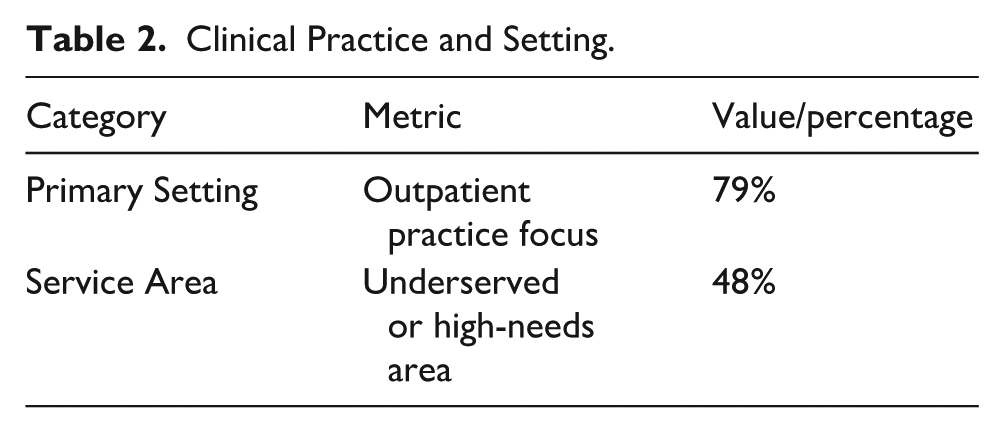
A total of 93 APRNs working in behavioral health participated in the survey during the 6-week data collection period from July to August 2025. Demographic data indicated that most respondents were seasoned clinicians with substantial professional experience. At least 72% of those surveyed reported having 6 or more years of APRN practice. Eighty-five percent of participants maintained PMHNP board certification, with 58% of those in California practicing independently under California AB 890 (Sections 103 and 104) practice authority (CA BRN, 2024). More than half of the sample was aged 51 years or older, with 88% identifying as female. Seventy-nine percent identified as White or European Americans. Regarding clinical practice settings, 79% of respondents reported working in an outpatient practice focus, and just under half, 48%, indicated that they provide services in an underserved or high-needs area. Participant demographic characteristics are summarized in Tables 1 and 2.
Participant Demographics and Professional Profile.
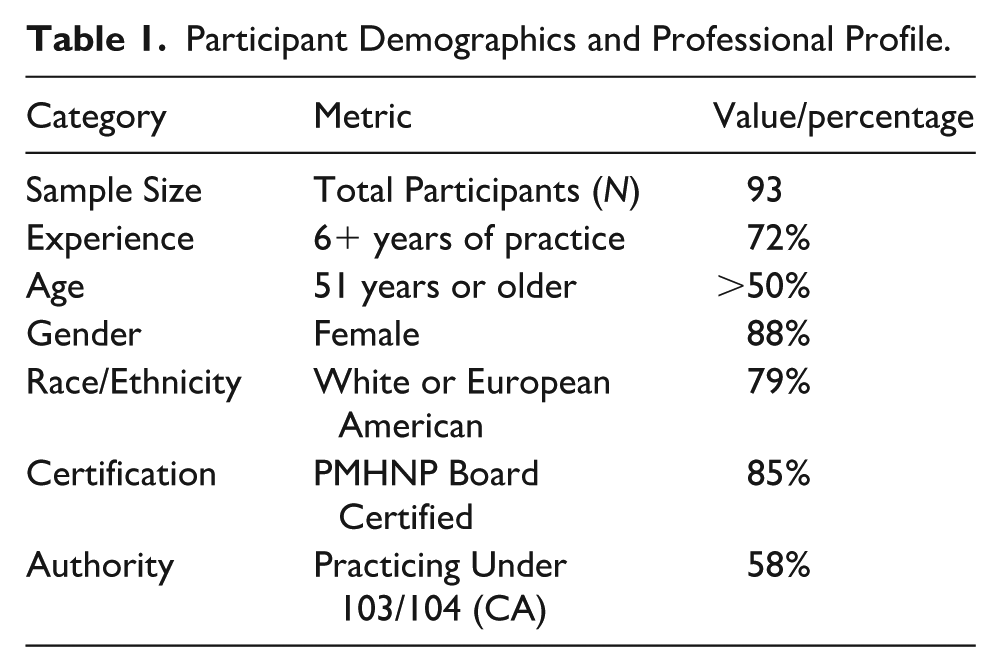
Clinical Practice and Setting.
Precepting Practices
Of those completing the survey, precepting was common: 72% reported precepting PMHNP students at some point in their careers. Of note, at the time the survey was conducted, 42% reported that they were currently precepting students. Among those who serve as preceptors, 86% typically support three to four PMHNP students per year, indicating a substantial teaching load for many participants. Precepting activities and workload are summarized in Table 3.
Precepting Activities and Workload.
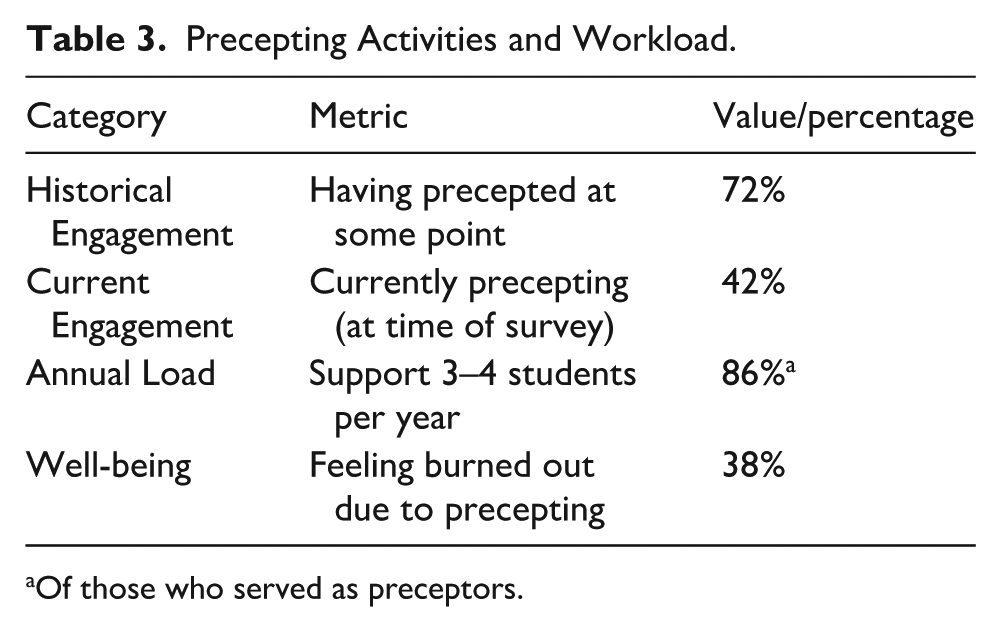
Of those who served as preceptors.
Motivations and Barriers
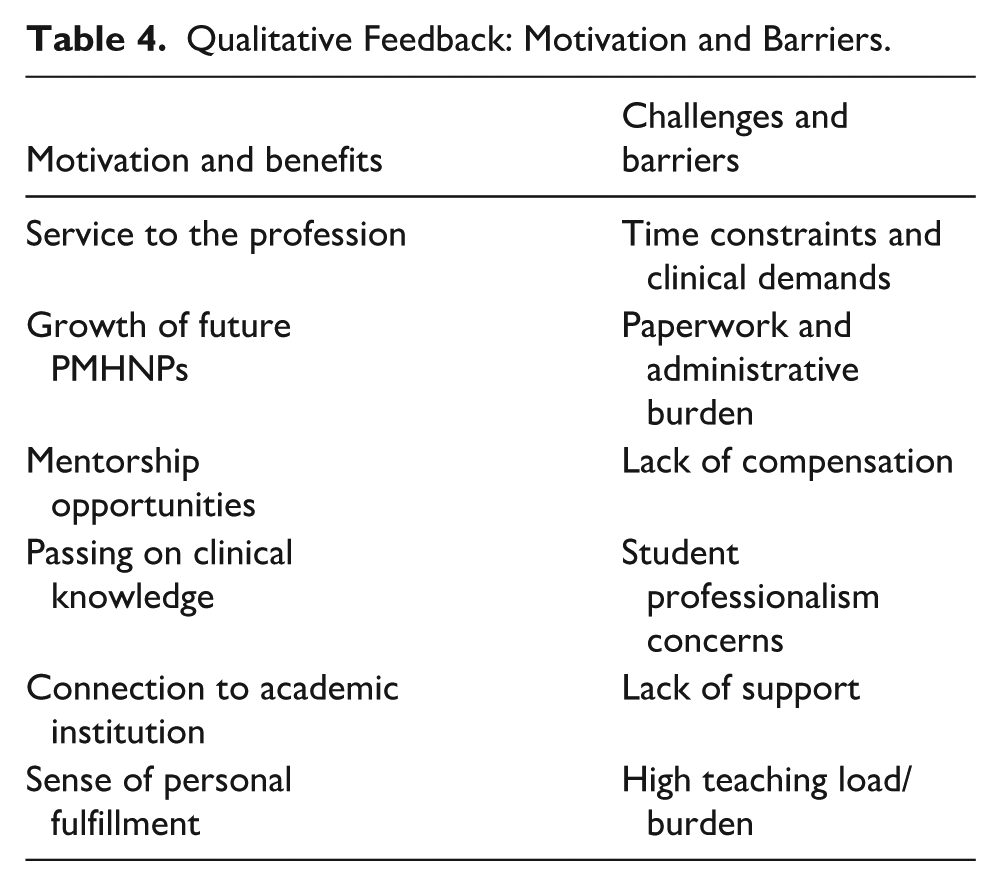
Respondents described several recurring benefits associated with precepting. Those who precepted reported a sense of fulfillment. Common themes included service to the profession, contributing to the growth and professional development of future PMHNPs, opportunities to provide mentorship, and passing on practical clinical knowledge. Maintaining a meaningful connection to academic faculty and institutions was also a common and recurring theme.
Participants also identified several challenges associated with precepting responsibilities. Frequently cited concerns included frustration with time constraints and competing clinical demands, considerable paperwork and administrative burden, concerns about student professionalism, lack of support, and lack of compensation for the time and effort involved in precepting. Notably, 38% of respondents reported feeling burned out due to the demands of precepting, underscoring the strain of balancing teaching and clinical responsibilities. Themes identified in motivations and barriers to precepting are summarized in Table 4.
Qualitative Feedback: Motivation and Barriers.
Preceptor Requests by Age Group
Demographics
Clear generational differences emerged in the types of support requested by survey participants, particularly regarding compensation, time allocation, and workplace accommodations. Among respondents, those aged 29 to 44 consistently expressed a greater need for both financial and time-related support than those aged 60 to 74. Participants aged 45 to 59 fell between the two groups in terms of financial incentives, a conducive work environment, and time compensation.
Baby Boomers: Ages 60 to 74
In contrast, Baby Boomers showed substantially lower levels of concern in these areas. Less than 9% of respondents requested monetary assistance or indicated a need for more time. This lower frequency may reflect differing career stages, greater financial stability, or established routines that require fewer accommodations. It may also indicate that Baby Boomers perceive work expectations as more manageable or are more accustomed to existing workplace structures.
Generation X (Gen X): Ages 45 to 59
In contrast to the other demographic groups, Gen X respondents demonstrated a moderate level of need. Twenty-six percent of participants in this cohort requested financial compensation, and 29% requested more time. This suggests that while Gen X experiences some pressures like Millennials (see below), the intensity of these needs is not as pronounced, with time reported as slightly more desirable than money.
Millennials: Ages 29 to 44
Millennials showed the strongest emphasis on compensation, with 33% requesting monetary support. A similar proportion indicated the need for additional time or flexible time allocation. These findings suggest that Millennials may be experiencing greater financial pressure or feel less adequately compensated relative to their workload. In addition, their requests for time may reflect challenges related to work–life balance, caregiving responsibilities, or burnout.
Discussion
Overall, the findings indicate that Millennials exhibit the highest demand for both financial and time-related accommodations, followed by Gen X, while Baby Boomers report the lowest levels of need. These results suggest that willingness and capacity to precept may vary across career stages and are influenced by more complex financial pressures and work–life priorities. These generational patterns may reflect broader socioeconomic trends, including prohibitive homeownership costs, rising living costs, shifting work expectations, student debt, behavioral health services, and differences in career stability. According to Friese et al. (2026), new nurses entering the profession are burdened by greater student loan debt than previous generations. The average debt upon graduation for a newly practicing APRN in 2025 is $66,420, a considerable increase from previous years. With a focus on meeting basic needs and on time being valued, as found in the survey, younger, debt-burdened PMHNPs are more likely to seek compensation. Taken together, these findings imply that a one-size-fits-all approach to recruitment and retention may be insufficient. Recognizing these generational differences can help universities better tailor support strategies to meet the distinct needs of preceptors. Prioritizing preceptor support in underserved and high-needs settings may be particularly important for advancing health equity and improving access to behavioral health services.
Time limits are embedded in treatment delivery models and structurally built into how care is designed and measured. This finding highlights that the most reported barrier to precepting is not simply workload, but a systematic misalignment between educational responsibilities and productivity-based care delivery. These constraints emerged as one of the most prominent barriers to precepting, referencing not only individual workload challenges but also larger misalignment between productivity models and educational responsibilities. The misalignment between productivity-based care delivery models and educational roles is exacerbated by demanding schedules that lack workload adjustments, creating tension between patient care and teaching responsibilities. These results suggest that improving the preceptor’s capacity will require structural redesign rather than individual willingness. Embedding precepting within patient care rather than treating it as additional work may improve the quality of the clinical learning environment.
Strengths and Limitations
This study has several methodological strengths. First, a mixed-methods survey design allowed for qualitative data that provided a clearer understanding of precepting PMHNP experiences and precepting behaviors. Second, the samples of practicing PMHNPs were recruited from diverse sources, including national nursing organizations and academic networks, over a geographically diverse area. Third, candid reporting of experiences and reduced response bias likely resulted from anonymous data collection. Finally, the survey was pilot-tested to improve clarity and usability.
Despite these strengths, several limitations should be considered in interpreting the findings. The sample size (N = 93) was small and represented a convenience sample, which may limit representation. The sample demographics were weighted to California practicing providers with experience who were white, female clinicians, which may reduce the generalizability to more diverse populations and geographic areas. Reliance on self-reported data introduces possible bias in social desirability and recall. Finally, the use of a non-validated survey instrument may limit how this study compares with others.
Recommendations
Considering the survey findings and demonstrated generational differences in compensation requests and time allocation, several recommendations are proposed to enhance preceptor engagement, satisfaction, and sustainability. These recommendations aim to strengthen institutional support structures, promote consistency across academic programs, and acknowledge the increasing value clinicians place on protected time.
Establish Uniform Flat-Rate Compensation Structure
A standardized compensation structure is supported by the finding that a lack of financial support was a frequently reported barrier, particularly among younger clinicians. Academic institutions should develop and implement standardized compensation frameworks that acknowledge the instructional labor of preceptors. To reduce inter-institutional variability and promote equity, universities are encouraged to collaborate in creating uniform flat-rate compensation structures. Such standardization would provide clarity for both preceptors and academic partners and reinforce the perceived value of clinical teaching.
State and Federal Financial Solutions
The finding that both time constraints and lack of compensation were among the most cited barriers supports the need for system-level incentives to offset the demands of workload, another approach that would address the frustration shared by both Millennials and Gen X. While it is technically legal for schools of nursing to provide financial compensation to preceptors, there are strict ethical, regulatory, and policy considerations to navigate, particularly in California, where “cash-in-hand” payments from students are often discouraged or prohibited by universities due to conflict of interest concerns. As a result, schools may pay preceptors as adjunct faculty through stipends or third-party contracts. So, while direct compensation from schools for precepting services is generally not practiced in public institutions, state financial incentives to hospitals and medical facilities to increase clinical placement opportunities would allow those entities to compensate their precepting clinicians or buy out time for their services (Gardenier et al., 2019).
States with serious shortages, such as Georgia, Maryland, Colorado, South Carolina, Alabama, and Virginia, currently offer tax credits, financial incentives, or tax-exempt grants to health care professionals, including nurses, who mentor nursing students. Currently, the PRECEPT Nurses Act is legislation under consideration in the U.S. House of Representatives. This federal program, introduced in January 2025, if passed, would grant a $2,000 tax credit per year to nurses who precept for at least 200 hours (H.R. 392, 2025–2026).
Enhance Institutional Recognition and Access to University Resources
Respondents identified mentorship, professional fulfillment, and academic connections as motivating factors for precepting; non-financial incentives remain an important retention strategy. Universities should formalize systems of recognition that may include academic titles, including adjunct or affiliate faculty appointments, structured acknowledgment of contributions, such as annual awards or recognition events, and increased access to institutional resources, such as libraries, educational platforms, and professional development opportunities. These measures affirm preceptors’ professional identity and foster deeper institutional affiliation.
Align Institutional With Accrediting Bodies
The Magnet Recognition Program, established by the American Nurses Credentialing Center (ANCC), acknowledges health care organizations that demonstrate excellence in quality patient care, nursing practice, and innovations in professional nursing. Mentorship is explicitly recognized as a vital component of nursing excellence within this framework. Consequently, many Magnet-designated hospitals may implement specific policies that encourage APRNs to engage in precepting, thereby fostering a culture of continuous learning and professional development.
Despite the Magnet designation, it is important to note that not all institutions require APRNs to serve as preceptors. Aside from the incentive of credit given for time spent precepting toward certification, the ANCC does not impose any requirements or incentives for APRNs to precept, nor does it necessitate the inclusion of precepting responsibilities in the job descriptions for advanced practice roles in Magnet facilities. Addressing this gap is crucial for mitigating the ongoing shortage of qualified preceptors in the field.
Expand Continuing Education Units (CEUs) Support Through Partnerships
Access to CEU-based opportunities serves as a meaningful incentive for participants who identified professional growth and connection to academic institutions as motivating factors. Institutions should explore coordinated strategies to provide CEU opportunities for preceptors. This may involve streamlined mechanisms for CEU documentation or the development of partnership agreements with national professional organizations to secure discounted certification or CEU rates. Enhanced access to CEUs serves as both an incentive and a means of supporting ongoing clinical competency.
Prioritize Protected Time as a Core Component of Preceptor Support
Because most respondents reported time as a barrier and the known variable that many clinicians identify time as being as valuable as monetary compensation, institutions should prioritize models that incorporate protected or reduced clinical workload for precepting activities. Such approaches may include allocating dedicated teaching time, modifying clinical schedules, or formally integrating precepting responsibilities into workload calculations. Institutions should move beyond informal accommodations and implement policies that include precepting in workload expectations. This may include reducing panel size, updating revenue value unit formulas, or including precepting in full-time equivalent job calculations. As state-specific full practice designation expands, there is an opportunity to redesign these models using NP-led clinics. In 2026, California’s newly defined full practice NP licenses commenced issuance monthly. The impact of starting nurse-led practices is yet unknown. In addition, larger health care organizations and academic partners should collaborate to redefine productivity frameworks to explicitly account for teaching. Prioritizing time protection may mitigate burnout and enhance the quality of the learning experience.
Examine Cross-Disciplinary Models of Preceptorship
Findings indicating that time and workload pressures are central barriers suggest that sustainable solutions may require redesigning education models. Several disciplines have successfully embedded precepting within standard workload expectations, often paired with schedule reductions or institutionally recognized teaching time. Universities and clinical partners should undertake a cross-disciplinary review to identify best practices and determine which strategies may be feasibly adapted for health care providers. Adopting such models may promote greater alignment between teaching demands and clinical responsibilities.
Establish a Comprehensive Preceptor Development Program
Findings that potential preceptors seek out the work for a sense of connection to universities and faculty are another area to capitalize on in recruitment and retention efforts. To mitigate feelings of disengagement from nursing faculty and schools of nursing, a structured system of onboarding, mentorship, and consistent feedback should be developed (Chan, Benner, et al., 2025). Thorough training for new preceptors, covering educational methodologies and clinical expectations, creates an understanding between the institution and the preceptor, promoting engagement. Providing mentorship opportunities by pairing experienced preceptors with new ones is another way to promote a culture of support and shared learning, ultimately increasing preceptor engagement. Finally, respondents who noted a lack of support from the schools of nursing they serve cited communication as a major obstacle. Regularly gathering feedback from preceptors to identify challenges and areas for improvement should be non-negotiable to remove this barrier. By adopting these recommendations, nursing programs can create a more supportive environment for preceptors, leading to better-prepared nursing graduates and ultimately, improved patient care outcomes.
Conclusion
The role of preceptors in the clinical education of PMHNPs is critical. As the landscape of clinical education faces increasing challenges, understanding the motivations and barriers that current PMHNPs encounter when deciding to precept is essential for addressing the preceptor shortage. While many practicing PMHNPs are altruistically motivated and enjoy serving the nursing profession, they also face significant barriers, including time constraints, administrative burdens, and burnout related to precepting.
Our research underscores the need for structured incentives at the governmental, accreditation, systemic, and institutional levels to promote change, not only by identifying preceptor concerns but also by addressing the reasons for recruitment and retention challenges and providing a framework for potential improvements. The findings should serve as a call for ongoing dialogue and action to foster a more supportive environment for these skilled clinicians. Incentives such as recognition, institutional perks, and compensation are tangible, reasonable, and aligned with preceptors’ needs and the demands of precepting. By implementing these strategies, we can enhance the precepting experience and ensure a robust pipeline of skilled PMHNPs for the future. Addressing these factors and conducting future research on the efficacy of the interventions mentioned above to improve the recruitment and retention of PMHNP preceptors will be vital for sustaining the quality of clinical education and ensuring the continued growth and development of the mental health nursing profession.
Footnotes
Author Contributions
All authors contributed to the conception and design of the study or to the acquisition, of data. Vanndy Loth conducted the analysis, and interpretation of the data. Stacey Green and Lynda Creighton-Wong drafted and critically revised the manuscript. Janet Meda and Chris Cleary collected data and reviewed and assisted with the revision. All authors gave final approval of the version that was submitted for publication. All authors agree to be accountable for all aspects of the work, ensuring integrity and accuracy. No funding was received for this study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.