
Abstract
Background:
Adolescents with attention-deficit/hyperactivity disorder (ADHD) often require long-acting or pro-drug stimulants, but telehealth prescribing is constrained by the Ryan Haight Act’s in-person requirements. While pandemic-era waivers temporarily lifted these mandates, their permanent status remains uncertain.
Aims:
Assess long-acting or pro-drug stimulant medication adherence using proportion of days covered (PDC) in adolescents with ADHD (12–17) receiving telehealth or hybrid care (2022–2024), comparing rates to post-pandemic (April 2020–June 2022) adherence rates in urban pediatric populations. Examine symptom scores on the Patient Health Questionnaire (PHQ-9), Generalized Anxiety Disorder Screening (GAD-2), and ADHD Symptom and Side Effect Tracking (ASSET). Compare visit attendance between telehealth and hybrid care.
Methods:
Program evaluation consisting of retrospective chart reviews, pre-visit surveys, and prescription data on 49 adolescents (21 telehealth and 28 hybrid) in a psychiatric clinic were evaluated.
Results:
The total sample mean PDC was .381. Hybrid group adherence was .448 and .313 for the telehealth group. PDC was the same as the post-pandemic adherence rate (.310–.440). Paired t-tests comparing GAD-2 scores were (p < .001), PHQ-9 (p < .001), and ASSET (p = .010). Telehealth attendance was lower than hybrid attendance.
Conclusions:
The hybrid care model showed better adherence and attendance than telehealth for adolescents with ADHD. PDC from this program evaluation was statistically similar to national trends in pediatric ADHD management. Future research must prioritize geographic and digital determinants, understand the impact of polypharmacy, and establish evidence-based strategies to enhance long-term adherence in telehealth care models.
The prescribing landscape for adolescents with attention-deficit/hyperactivity disorder (ADHD) in the United States underwent a paradigm shift toward fully virtual care during the COVID-19 pandemic (Danielson et al., 2024; Rao et al., 2025; Worthen et al., 2024). Prior to the public health emergency, the Ryan Haight Online Pharmacy Consumer Protection Act of 2008 (Ryan Haight Act) mandated at least one in-person evaluation annually to mitigate the risk of illegitimate distribution of controlled substances via telehealth (American Academy of Child & Adolescent Psychiatry Telepsychiatry and Quality Committee [AACAPTQ], 2017; Myers et al., 2017). While the lifting of these restrictions facilitated accessible and efficient prescribing of long-acting and pro-drug stimulants during the pandemic, the future of these flexibilities remains uncertain. It is currently unclear if the Drug Enforcement Administration (DEA) and Department of Health and Human Services (HHS) will permanently remove the annual in-person visit requirement (Worthen et al., 2024).
Recent literature indicates a concerning decline in medication adherence among adolescents since 2020 (Cunningham et al., 2021; McCabe et al., 2023). While some studies have compared pre-pandemic to post-pandemic adherence, there is a critical gap in research focusing on the longitudinal outcomes of 2022–2025 (Cunniff et al., 2024). Existing research in adult and broader pediatric populations has demonstrated that telehealth can yield equivalent symptom improvement and attendance to in-person care (Khan & Aslani, 2020). However, comparative data regarding the standard hybrid approach (incorporating an annual in-person medication visit) versus fully telehealth models remain sparse in adolescent populations. Therefore, the purpose of this program evaluation was to compare hybrid and fully telehealth models at a psychiatric clinic by measuring medication adherence, symptom management, and attendance. These findings aim to provide evidence-based insights for policymakers and stakeholders developing long-term telehealth regulations (AACAPTQ, 2017; Anghel et al., 2019; Khan & Aslani, 2020; Myers et al., 2017).
Aims
The evaluation aims were to (a) compare medication adherence for long-acting or pro-drug stimulants, measured by the proportion of days covered (PDC), between telehealth and hybrid care models among adolescents (ages 12–17 years) against established post-pandemic rates (April 2020–June 2022); (b) examine trends in symptom scores (utilizing a 50% improvement benchmark) from the initial to the final visit using the Patient Health Questionnaire (PHQ-9), Generalized Anxiety Disorder Screening (GAD-2), and ADHD Symptom and Side Effect Tracking (ASSET); and (c) compare follow-up visit attendance consistency (defined as four appointments per year, at least every 4 months) between telehealth and hybrid care (at least one annual in-person medication appointment).
Methods
Context
Setting and Subgroup Definition
The program evaluation was conducted at Rochester Center for Behavioral Medicine (RCBM), a psychiatric practice providing care across Michigan, focusing on ADHD. Leveraging telehealth, the clinic underwent significant expansion from 30 to approximately 100 clinicians from 2020 to 2023. Since 2023, the clinic has utilized a hybrid model requiring an annual in-person visit for all patients prescribed controlled substances.
The analytic sample for this evaluation was categorized into two subgroups to provide a meaningful comparison for the program: the hybrid subgroup (attending one annual in-person evaluation) and the fully telehealth subgroup (100% remote). This structure was designed to evaluate ADHD management and the prescribing patterns of long-acting or pro-drug stimulants across different service delivery models within the clinical setting.
Inclusion Criteria
Records were included if they met the following criteria: (a) confirmed diagnosis of inattentive, hyperactive/impulsive, or combined-type ADHD established during the diagnostic intake with a prescriber between June 1 and November 30, 2022; (b) ages 12–17 years at intake; (c) completion of digital pre-visit surveys at intake and follow-up appointments; and (d) initiated pharmacological treatment with long-acting or pro-drug stimulants during the 30-month observation period. Inclusion criteria were designed to preserve ecological validity by reflecting the clinical complexity of the adolescent population. To ensure a real-world sample of adolescents in a psychiatric setting, records were included regardless of psychiatric co-morbidity. This approach reflects the clinical reality that approximately 78% of this population presents with at least one co-occurring disorder, making long-acting or pro-drug stimulant monotherapy an infrequent finding for a real-world evaluation (Danielson et al., 2024).
Exclusion Criteria
Records were excluded due to the following: (a) seen at the clinic within 6 months prior to the specified intake window; (b) prescribed a long-acting or pro-drug stimulant within the 6 months preceding the intake; (c) under age 12 or over 17 at intake; or (d) did not initiate long-acting or pro-drug stimulant therapy.
Study of the Intervention
This program evaluation was grounded in the Pediatric Virtual Care Evaluation Framework, a specialized adaptation of the Supporting Pediatric Research on Outcomes and Utilization of Telehealth (SPROUT) Framework (Chuo et al., 2020; Dulude et al., 2023). While SPROUT provides a broad architecture for telehealth research, the Pediatric Virtual Care Evaluation Framework was specifically utilized to define clinical aims and metrics, ensuring they were developmentally appropriate for an adolescent ADHD population. The evaluation was structured around the framework’s four domains: Health Outcomes, Health Equity, Experience, and Value. This structure allowed for a direct comparison of medication adherence, symptom improvement, and attendance across telehealth and hybrid models (Dulude et al., 2023).
Ethical Considerations and Data Extraction
This project was exempted by the Duke University’s Institutional Review Board, as it involved retrospective de-identified chart reviews for quality improvement and the analysis of longitudinal outcomes. Data were extracted via comprehensive chart reviews and proprietary archived records from the electronic health record system at RCBM. The project utilized descriptive variables, such as concurrent psychiatric medications, to provide a comprehensive profile of the adolescent sample, while factors like parental marital status and digital accessibility were noted as being outside the primary scope of this evaluation.
Measures
The clinic utilized a standardized, multidimensional “pre-visit screening protocol” for all patients aged 12 years or older to facilitate longitudinal tracking of symptom improvement and medication tolerance. To provide a comprehensive clinical profile, the clinic employed the PHQ-9 (mood symptoms), GAD-2 (anxiety symptoms), and ASSET (ADHD symptoms) scales (MedaData, n.d.; Nasser et al., 2022; Shamoon et al., 2024; Young et al., 2023). This multifaceted approach allowed providers to monitor both the primary diagnosis and the high rates of co-occurring psychiatric disorders prevalent in this population. ADHD symptom severity was measured using the ASSET scale, a validated 10-item instrument designed for rapid clinical assessment (Young et al., 2023). The scale uses a six-point Likert-type system to evaluate two primary subscales: inattention and hyperactivity/impulsivity. In addition, data regarding the duration of medication supply were derived from provider-issued prescription records to calculate the PDC. Visit attendance was measured as the percentage of participants completing at least four annual appointments with a maximum gap of 4 months between visits.
Analysis
Data were analyzed in Microsoft Excel 2019 (Microsoft Corporation). The average PDC for each subgroup was calculated by dividing the sum of individual PDC scores each month by the total subgroup population size. A run chart was utilized to track trends in monthly average PDC over 30 months (June 2022 to December 2024). The primary PDC target was set at .700, a threshold adjusted from the traditional .800 “gold standard” to accommodate planned long-acting or pro-drug stimulant holidays. Additional low (.310) and high (.440) benchmarks were utilized, representing post-pandemic (April 2020–June 2022) adherence rates in urban pediatric populations (Barner et al., 2011; Cunniff et al., 2024). For clinical outcomes, paired t-tests were conducted for each scale, comparing the initial pre-visit score to the average of subsequent follow-up scores, with statistical significance set at p < .05. Clinical improvement was defined as 50% reduction in the baseline symptom score, a recognized benchmark for a good clinical response to treatment (Zimmerman et al., 2018). The threshold for “met criteria” was set at 80%.
Results
Sample Selection and Demographics
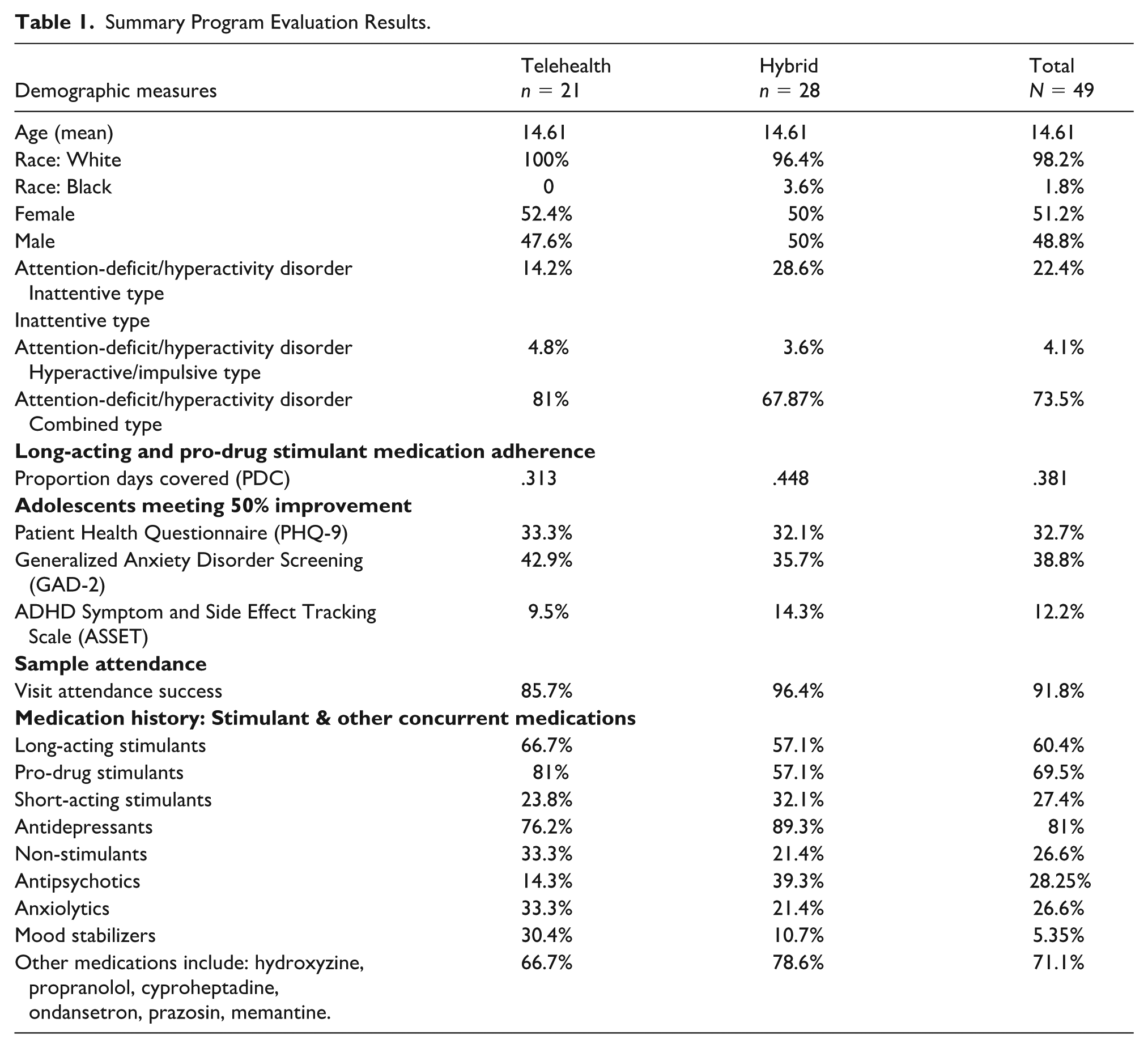
A total of 611 records were initially screened for eligibility. Of these, 83 records contained intakes during the 2022 calendar year. Following a detailed chart review, 34 records were excluded: Nine adolescents did not initiate long-acting or pro-drug stimulant therapy, 22 did not meet age or prior-use criteria, and three lacked the required longitudinal survey data for symptom evaluation. This resulted in the final total sample of N = 49. The total sample had a mean age of 14.61 years, which was consistent across the telehealth and hybrid subgroups (Table 1). Regarding racial distribution, 96.2% identified as White (100% telehealth; 96.4% hybrid), and 1.8% identified as Black (0% telehealth; 3.6% hybrid). The gender distribution across the total cohort was nearly equal, consisting of 51.23% female and 48.85% male. This balance remained consistent within the subgroups: The fully telehealth subgroup comprised 52.40% female and 47.60% male, while the hybrid subgroup achieved an exact 50% female and 50% male split. Descriptive data regarding other concurrent medications are detailed in Table 1.
Summary Program Evaluation Results.
PDC Comparison
The mean PDC for the total sample (N = 49) was .381 (Figure 1). Subgroup analysis revealed a distinct difference in adherence levels: The hybrid subgroup achieved a mean PDC of .448 (n = 28), while the fully telehealth subgroup demonstrated a mean PDC of .313 (n = 21). When compared to established post-pandemic parameters (ranging from .310 to .440), both subgroups, on average, met these clinical benchmarks.
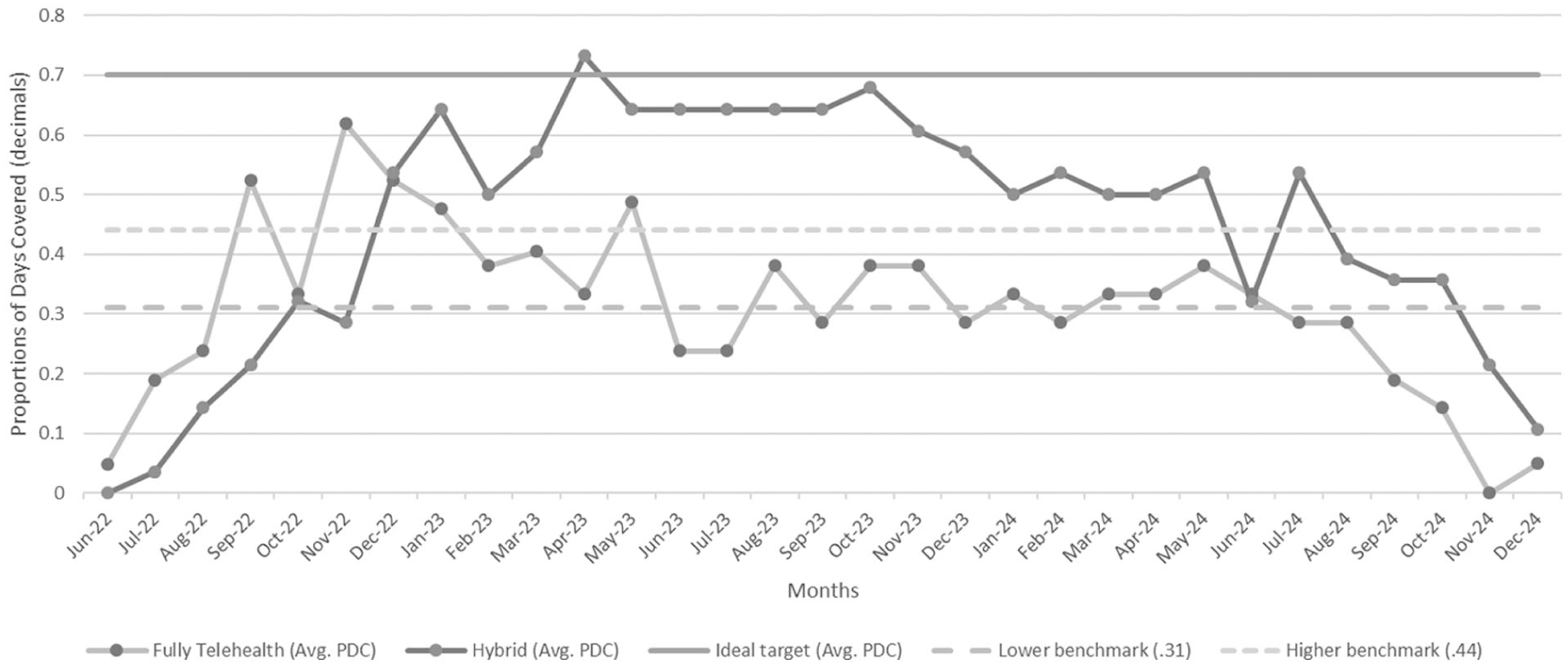
Monthly proportion of days covered (PDC) for hybrid and fully telehealth subgroups relative to evidence-based benchmarks (June 2022–December 2024).
The hybrid subgroup exhibited several periods of high engagement, notably reaching the ideal clinical benchmark of .700 in April 2023. This group experienced a significant upward trend early in the project, rising from .290 in November 2022 to .540 in December 2022. Adherence remained robust, averaging .640 from May through September 2023, before beginning a steady decline in October 2023 that culminated in a significant drop by July 2024. In contrast, the fully telehealth subgroup did not meet the ideal .700 benchmark at any point, although it reached a peak of .620 in November 2022. While the subgroup performed above the higher-range post-pandemic benchmarks from November 2022 through January 2023, it primarily met post-pandemic parameters from February 2023 to May 2024. However, the fully telehealth group fell below the lower post-pandemic benchmarks during the summer months of 2022 and 2023, as well as late 2024. A definitive downward trend in adherence was observed for this group from May 2024 (.380) until the end of the evaluation period in November 2024 (0).
Symptom Improvement
Symptom change from baseline to follow-up was assessed using paired sample t-tests (N = 49). Analysis revealed statistically significant improvements across all three clinical measures over the course of treatment. A significant decrease in mean scores was found for PHQ-9, which declined from 10.18 (SD = 6.03) to 7.05 (SD = 5.04), p < .001. Similarly, ASSET scores significantly decreased from baseline (M = 3.60, SD = 1.03) to follow-up (M = 3.22, SD = .91, p = .010). A significant reduction was also observed in GAD-2 mean scores, which decreased from 2.98 (SD = 1.66) to 1.89 (SD = 1.37, p < .001). The GAD-2 showed the highest rate of benchmark attainment, with 38.8% of the total cohort meeting the 50% threshold. For the PHQ-9, 32.7% of the sample achieved the threshold. Notably, the 50% improvement in ASSET scores occurred in only 12.2% of the total cohort. The analysis of clinical significance, defined as a 50% improvement in total score, revealed significant variation between telehealth and hybrid subgroups (Table 1).
Visit Attendance
Visit attendance success was defined as completing at least one prescriber visit every 4 months (minimum of four visits per year), with the success threshold set at 80% or greater over the evaluation period. While the total observation period spanned 24 months, visit attendance was adjusted proportionally based on the length of time each adolescent remained in the cohort to ensure a consistent measure. Overall, 91.8% of the total cohort met the 80% attendance criteria. When analyzed by modality, the hybrid subgroup demonstrated a higher success rate of 96.4% compared to the fully telehealth subgroup at 85.7% (Table 1). Furthermore, 79.2% of the total sample achieved perfect attendance (100% compliance) throughout the evaluation duration. The superior performance of the hybrid group was maintained despite the presence of a single outlier record that achieved only 50% of the required attendance. The hybrid subgroup exhibited higher engagement, outperforming the fully telehealth subgroup by a margin of 10.7% in meeting the established attendance criteria.
Discussion
Proportion of Days Covered
Adherence rates observed in this evaluation (.313 telehealth; .448 hybrid) were within the post-pandemic range established by Cunniff et al. (2024), suggesting the cohort’s performance was consistent with national trends in pediatric ADHD management. These findings suggest a hybrid care model may promote better outcomes and consistent medication use than fully telehealth at this clinical site. While the hybrid care group had a higher PDC, the drivers of this difference are unclear. The variance may be attributed to socioeconomic stability or parental support; however, these factors were not captured in this evaluation, and further research is needed to isolate the determinants of adherence in hybrid models.
Symptom Improvement
A 50% symptom-improvement threshold was utilized as a broad measure of program outcomes and was achieved in this sample; however, this metric may be influenced by variations in longitudinal symptom-measurement processes. Utilizing evidence-based benchmarks specific to each instrument (PHQ-9, GAD-2, and ASSET) in future evaluations could strengthen clinical relevance, particularly when assessing the reductions in ADHD symptoms and other psychiatric comorbidities, such as anxiety and depression (Danielson et al., 2024; Young et al., 2024).
Visit Attendance
Analysis of follow-up timeliness found a high rate of patient engagement, with 91.82% of the cohort meeting the criteria of four annual appointments and quarterly medication management. The hybrid subgroup had greater success than the fully telehealth subgroup. This difference suggests that the in-person component of hybrid care may be a critical factor in fostering consistent visit adherence and clinical engagement in adolescents. To enhance adherence within the fully telehealth model, cost-effective interventions should focus on strengthening the prescriber-patient relationship and fostering patient empowerment through technology (García-Pérez et al., 2020; Storetvedt et al., 2024). Recommended strategies include implementing gamification and short-form education to improve medication adherence and adopting secure direct text-message platforms to support rapport and follow-up consistency (García-Pérez et al., 2020; Storetvedt et al., 2024).
Future Implications
Policymakers and clinical stakeholders must evaluate the impact of the evolving regulatory landscape on medication continuity for fully remote adolescents. Specifically, the potential for new permanent DEA rulings following the expiration of Public Health Emergency waivers remains a critical concern. Updates to regulatory guidance concerning telehealth utilization remain complex and frequently contradictory for clinicians. While the DEA and HHS issued a fourth extension of telehealth prescribing flexibilities in the United States through December 31, 2026, the Centers for Medicare and Medicaid Services concurrently introduced service-level limitations. In September 2025, Medicare discontinued full coverage for non-psychiatric telehealth services (Center for Connected Health Policy/Public Health Institute, 2025; Fourth Temporary Extension, 89 Fed. Reg. 91557, 2024). Despite a decade of repeated introduction of bipartisan legislation proposing permanent telehealth flexibility, a lack of legislative support has stalled statutory change (VGM & Associates, 2025).
Digital and Geographic Determinants
Future research should prioritize the analysis of geographic location and digital determinants of health, such as high-speed internet access and device literacy. For the fully telehealth subgroup, these factors may have influenced the lower adherence rates (.313) more significantly than clinical variables alone. Establishing supportive structures to improve attendance and adherence within telehealth services is crucial for stakeholders developing the next decade of telehealth guidelines.
Clinical Complexity and Polypharmacy
While this evaluation focused on long-acting or pro-drug stimulants, the prevalence of polypharmacy in this population warrants deeper investigation. Future research should evaluate whether concurrent non-stimulant psychiatric medications act as a barrier or facilitator to daily ADHD routines. Mapping medication overlaps will provide a more nuanced understanding of real-world adherence in complex pediatric cases. Future investigations should utilize metrics that differentiate intentional stimulant holidays from medication non-adherence to obtain a more precise evaluation of patient behavior and account for planned treatment pauses without conflating them with unintentional adherence barriers.
Limitations
This evaluation was limited by a lack of demographic diversity (98.0% White sample), limiting generalizability to more diverse populations, where socioeconomics and pharmacy disparities often compound barriers to care (Danielson et al., 2024). Site-specific variables that could impact replicability of these findings include existing telehealth infrastructure at the site, provider-patient rapport, and regional medication availability. The administrative support at this practice likely contributed to the high attendance and adherence rates. Future research must investigate these intersections to ensure equitable access to long-acting or pro-drug stimulants across diverse geographic and clinical environments.
Conclusion
A comparative analysis of hybrid and fully remote telehealth models found that both are effective and comparable frameworks for managing adolescent ADHD. The total sample (N = 49) achieved medication adherence rates consistent with established national post-pandemic parameters, suggesting that both telehealth and hybrid modalities at the study site performed at a level comparable to national benchmarks. Clinical outcomes across all measures, PHQ-9, GAD-2, and ASSET, demonstrated statistically significant improvements (p < .05). Furthermore, 91.8% of the total sample met or exceeded the 80% attendance requirement. While these results are promising, larger-scale research is warranted to investigate multifactorial drivers of sustainable medication adherence in adolescents with ADHD. This program evaluation serves as a preliminary blueprint for establishing standard telehealth guidelines in psychiatric-mental health nursing.
Footnotes
Ethical Considerations
This project was a retrospective review of existing, de-identified patient data collected for clinical purposes and was submitted to the Institutional Review Board (IRB) at Duke University. The project was formally determined to meet the criteria for Exempt status under 45 CFR 46.102(e), 21 CFR 56.102(e), and 21 CFR 812.3(p), and satisfies the Privacy Rule as described in 45 CFR 164.514 (Protocol #Pro00117834).
Consent to Participate
Given that the study involved only the analysis of de-identified, pre-existing records, the Institutional Review Board (IRB) granted a waiver of informed consent.
Author Contribution
All authors contributed to the conception or design of the study or to the acquisition, analysis, or interpretation of the data. All authors drafted the manuscript, or critically revised the manuscript, and gave final approval of the version that was submitted for publication. All authors agree to be accountable for all aspects of the work, ensuring integrity and accuracy.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The primary author (Elizabeth Sweet) conducted this project at their place of employment, the Rochester Center for Behavior Medicine (RCBM), as part of a Doctor of Nursing Practice (DNP) degree at Duke University. R. N. Powell and Jill Fortain are also employees of the center. Please note that two members of the authorship team are original developers of the ASSET that is cited. Jessica Marsack and Nancy Crego declare that they have no conflicts of interest, financial or otherwise, that biased the conduct or reporting of this study.
Data Availability Statement
The data that support the findings of this study are not publicly available because of the inclusion of potentially identifying patient health information. However, de-identified data extracts are available upon reasonable request from co-author, RP, in coordination with corresponding author, pending approval by the Rochester Center for Behavioral Medicine.