
Abstract
The objective of this meta-analysis was to systematically review existing evidence and evaluate variations in levels of circulating endothelial progenitor cells (EPCs) among individuals with psoriatic arthritis (PsA), juvenile idiopathic arthritis (JIA), and rheumatoid arthritis (RA). Relevant studies were identified through database searches, and 20 records were enrolled. We used the fixed-effect model or random-effect model to estimate the pooled standardized mean difference (SMD) with 95% confidence intervals (CIs) in circulating EPC levels between inflammatory arthritis patients and controls. The results showed that circulating EPC levels differed among subtypes of inflammatory arthritis, with significantly lower levels in patients with RA (SMD = −0.848, 95% CI = −1.474 to −0.221, p = 0.008) and PsA (SMD = −0.791, 95% CI = −1.136 to −0.446, p < 0.001). However, no statistically significant difference was found in circulating EPC levels between patients with JIA and controls (SMD = −1.160, 95% CI = −2.578 to 0.259, p = 0.109). Subgroup analyses suggested that in patients with RA, circulating EPC levels were influenced by age, disease activity, and duration. Although many studies have investigated circulating EPC levels in patients with inflammatory arthritis, the results have been inconsistent. This meta-analysis offers a comprehensive overview of the existing evidence and emphasizes the association between levels of circulating EPCs and various types of arthritis. However, further research is needed to determine the specific mechanisms underlying the observed differences in EPC levels in different types of arthritis and to establish the clinical utility of this biomarker.
Keywords
Increased risk of cardiovascular disease (CVD) in patients with inflammatory arthritis.
Levels of circulating endothelial progenitor cells (EPCs) as a predictor of CVD in healthy populations.
The levels of EPCs in peripheral blood of patients with inflammatory arthritis in previous studies are contradictory.
Levels of circulating EPCs vary among subtypes of inflammatory arthritis.
Circulating EPC levels were significantly lower in patients with psoriatic arthritis (PsA) or rheumatoid arthritis (RA).
The level of EPCs provides valuable information to complement the diagnosis of RA or PsA.
Further research should focus on determining the specific mechanisms underlying the differences in EPC levels observed in inflammatory arthritis subtypes.
Introduction
Inflammatory arthritis is a chronic inflammatory disease characterized by persistent synovitis and structural joint damage.1,2 It includes several subtypes, such as psoriatic arthritis (PsA), ankylosing spondylitis (AS), spondyloarthritis (SpA), rheumatoid arthritis (RA), and juvenile idiopathic arthritis (JIA). Although the clinical manifestations of these diseases may vary, they all share a systemic inflammatory pathology that can affect multiple organs. Patients with inflammatory arthritis have a reduced life expectancy compared to the general population, primarily due to increased risk of cardiovascular disease (CVD). The global prevalence of inflammatory arthritis has approximately reached 3%, 3 and studies have suggested that it is associated with an elevated risk of cardiovascular (CV) mortality and morbidity.4,5 Well-established, traditional CV risk factors comprise diabetes, hypertension, dyslipidemia, and smoking. However, these risk factors did not fully explain the excessive CV mortality in patients with inflammatory arthritis. Other nontraditional risk factors, such as chronic inflammation and genetic factors, have emerged as potential amplifiers of CVD risk. 6 Additionally, patients with RA have been shown to have increased CV morbidity compared to healthy controls and patients with osteoarthritis. 7 Therefore, the identification of specific markers is particularly important for the diagnosis of inflammatory arthritis.
Endothelial progenitor cells (EPCs) are a population of circulating cells derived from hematopoietic stem cells that possess the ability to migrate and self-renew. These cells have the capacity to differentiate into vascular endothelial precursor cells, and are known to play a critical role in promoting angiogenesis and repairing damaged vessels.8,9 In clinical studies, EPCs are typically characterized by the co-expression of CD34, a hematopoietic stem cell marker, and VEGFR-2/KDR, a type 2 vascular endothelial growth factor receptor. 10 Furthermore, CD133 has been suggested as an additional marker for EPCs by experts in the field.11,12 Altered numbers or function of EPCs have been reported in patients with inflammatory arthritis and other autoimmune diseases, which may contribute to impaired endothelial repair mechanisms.13,14 The resulting endothelial dysfunction may be the primary cause of subclinical CV dysfunction observed in the early stages of inflammatory arthritis. 15
Although the level of circulating EPCs was considered to be a predictor of CVD in healthy populations, 16 studies on the level of EPCs in peripheral blood (PB) of patients with inflammatory arthritis were varied and even contradictory. Grisar et al. 17 first reported in 2005 that, compared with healthy controls, circulating EPCs proportions were significantly reduced in RA patients. However, other studies found that circulating EPCs proportions were slightly higher in RA patients.18,19 Similarly, studies on circulating EPC levels remain contradictory in patients with PsA or JIA.20–22 Nevertheless, systematic review and meta-analysis focusing on circulating EPC levels in patients with inflammatory arthritis, including PsA, JIA, and RA, is still lacking. Hence, the purpose of this meta-analysis was to evaluate the circulating levels of EPCs among patients with various subtypes of inflammatory arthritis. The findings aim to offer valuable insights for the complementary diagnosis of clinical inflammatory arthritis.
Materials and methods
Search strategy
This article follows the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (see Supplemental Table S1) 23 and the Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. 24 Two researchers (Hui Zhao and Lanlan Fang) independently searched Web of Science, PubMed, and MEDLINE about the relationship between EPCs and inflammatory arthritis until September 15th, 2022. The terms of keywords and search strategy, were as follows: ((Inflammatory arthritis) OR (Ankylosing spondylitis) OR (AS) OR (Spondyloarthritis) OR (SpA) OR (Rheumatoid arthritis) OR (RA) OR (Juvenile idiopathic arthritis) OR (JIA) OR (Psoriatic arthritis) OR (PsA)) AND ((Endothelial progenitor cells) OR (EPCs) OR (EPC)). In addition, we searched the related research manually from the references of the included studies to prevent omission. The following criteria were used to determine the eligibility for included studies: (1) cross-sectional, cohort studies, or case-control containing a control group consisting of individuals without PsA, JIA, RA, or the general population; (2) studies presented the circulating EPC levels in both inflammatory arthritis and control groups; and (3) language limited to English.
Data extraction
All relevant data for the included studies were extracted independently by two authors (Hui Zhao and Lanlan Fang). The following data were included: the author’s name, year, region, characteristics of participants (age, gender, and disease duration), circulating EPC levels (mean ± SD) in the patients and control group, design type, and other pertinent information. We attempted to email the corresponding author the necessary information when the above data are missing from the original article. Any disagreements over study inclusion or data extraction were resolved through discussion with a third reviewer (Faming Pan).
Quality assessment
The quality of the study is assessed using the Newcastle–Ottawa Quality Assessment Scale (NOS), 25 with the highest score being 9. Studies with a score between 7 and 9 are considered high quality, while those with scores between 4 and 6 and 0 and 3 are considered moderate quality and low quality, respectively.
Statistical analysis
The “Metafor” and “Meta” packages of the R 4.2.0(R Foundation for Statistical Computing, Vienna) software were used for all statistical analyses . We extracted the mean and standard deviation (mean ± SD) from the included studies, and for studies that reported median (range or interquartile range), we converted them to mean ± SD. 26 To evaluate circulating EPC levels in inflammatory arthritis patients and controls, we used standardized mean difference (SMD) and 95% confidence interval (CI).
To assess statistical heterogeneity across studies, Cochran’s Q statistic and I2 test were used, if there was significant heterogeneity (I2 > 50% or p < 0.05 for Q-test), a random-effect model was used, otherwise, a fixed-effect model was used for pooled analysis.27,28 To investigate possible sources of heterogeneity across studies, subgroup analyses and meta-regression were performed. Explanatory variables include the year of publication, age, female percentage of the sample, sample size, disease duration, C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), Disease Activity Score 28 (DAS28), and research quality score; grouping variables include region, markers used, age, ESR, DAS28, disease duration and quality score. Funnel plots, Egger’s test, and Begg’s regression test were used to detect potential publication bias. 29 Additionally, we conducted several sensitivity analyses. Firstly, we systematically excluded one study at a time to assess the impact of each individual study on the overall pooled results. Subsequently, a cumulative meta-analysis was performed to explore whether there was any variation in the results over time. Moreover, considering the limited number of included studies and the observed heterogeneity, we utilized the Hartung-Knapp-Sidik-Jonkman (HKSJ) meta-analysis method to summarize the main findings and compare them with the results obtained from the DerSimonian–Laird method. 30 Furthermore, in the RA group, we exclusively included studies that reported the proportion of peripheral blood mononuclear cells (PBMCs) as the measure of EPCs to examine its potential impact on the primary outcome. p < 0.05 indicates statistical differences.
Result
Publication search and characteristics of studies
A total of 747 articles were retrieved in Web of Science (n = 392), PubMed (n = 179), and MEDLINE (n = 176). A total of 315 records were excluded due to duplication, and 397 articles were excluded after browsing the titles and abstracts. Thirty-five articles were retrieved for full-text assessment. Ultimately, 20 studies were included in the meta-analysis (Figure 1). Table 1 summarizes the characteristics of all the included studies. Of these, 3 articles included 77 PsA patients and 67 controls,21,22,31 4 included 75 JIA patients and 75 controls,20,32–34 and 13 included 720 RA patients and 345 controls.17–19,35–44 In all included studies, case-control designs were used, and circulating EPC levels in PB were measured by flow cytometry (FCM). In the majority of studies, the level of EPCs was reported as a proportion of PBMCs, and a few studies described the EPC level either as the number of EPCs per milliliter of PB or relative to the count in 106 total cells. Despite the different units of EPC levels, our pooled effect values were reliable because pooled SMDs combined different methods or units from different studies. In addition, the results of the detailed methodological quality assessment are shown in Supplemental Table S2, with 20 studies having a quality score between 4 and 8 on the Newcastle–Ottawa scale.
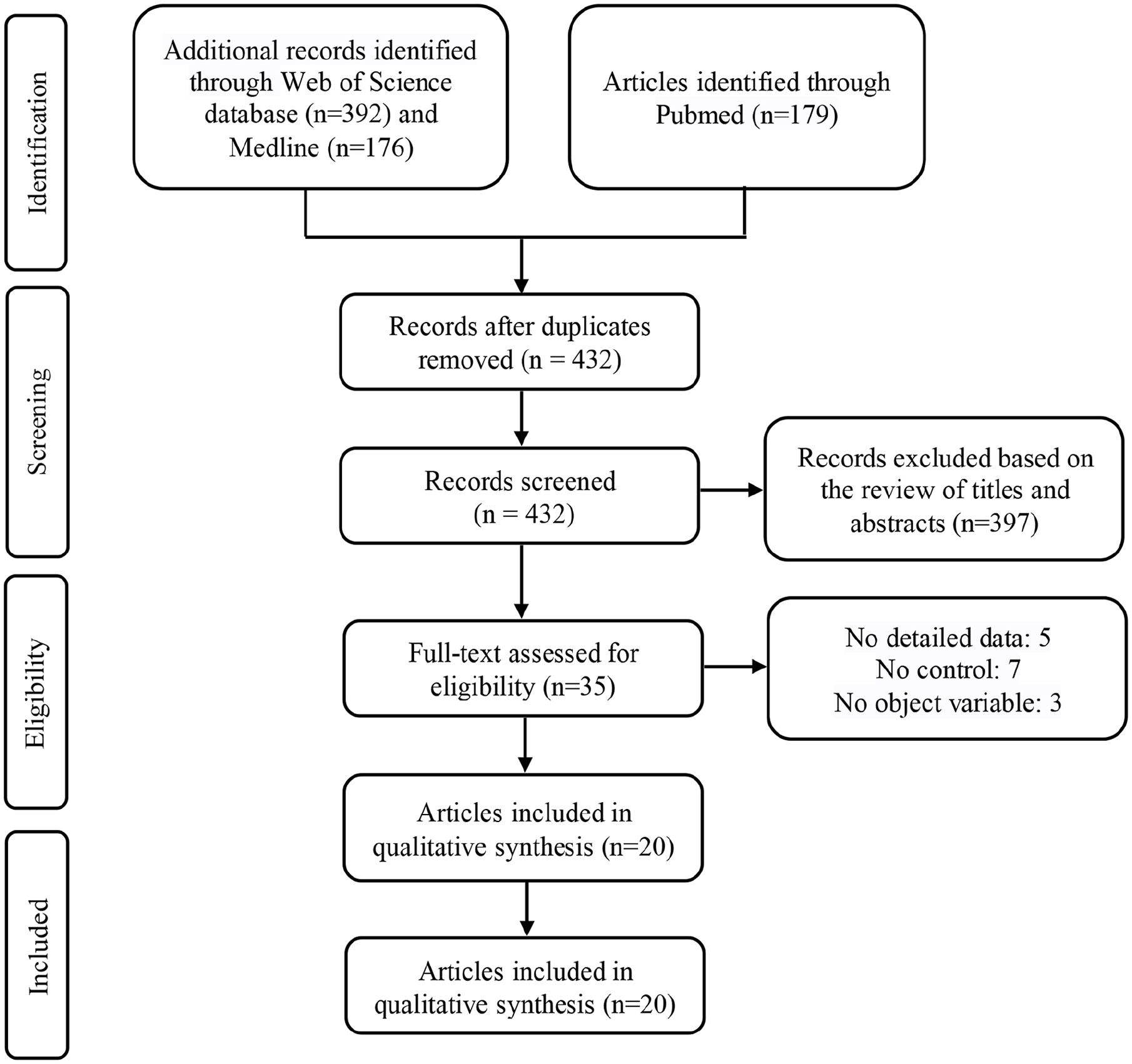
Flow chart of the literature search and study selection.
Basic characteristics of the included studies.
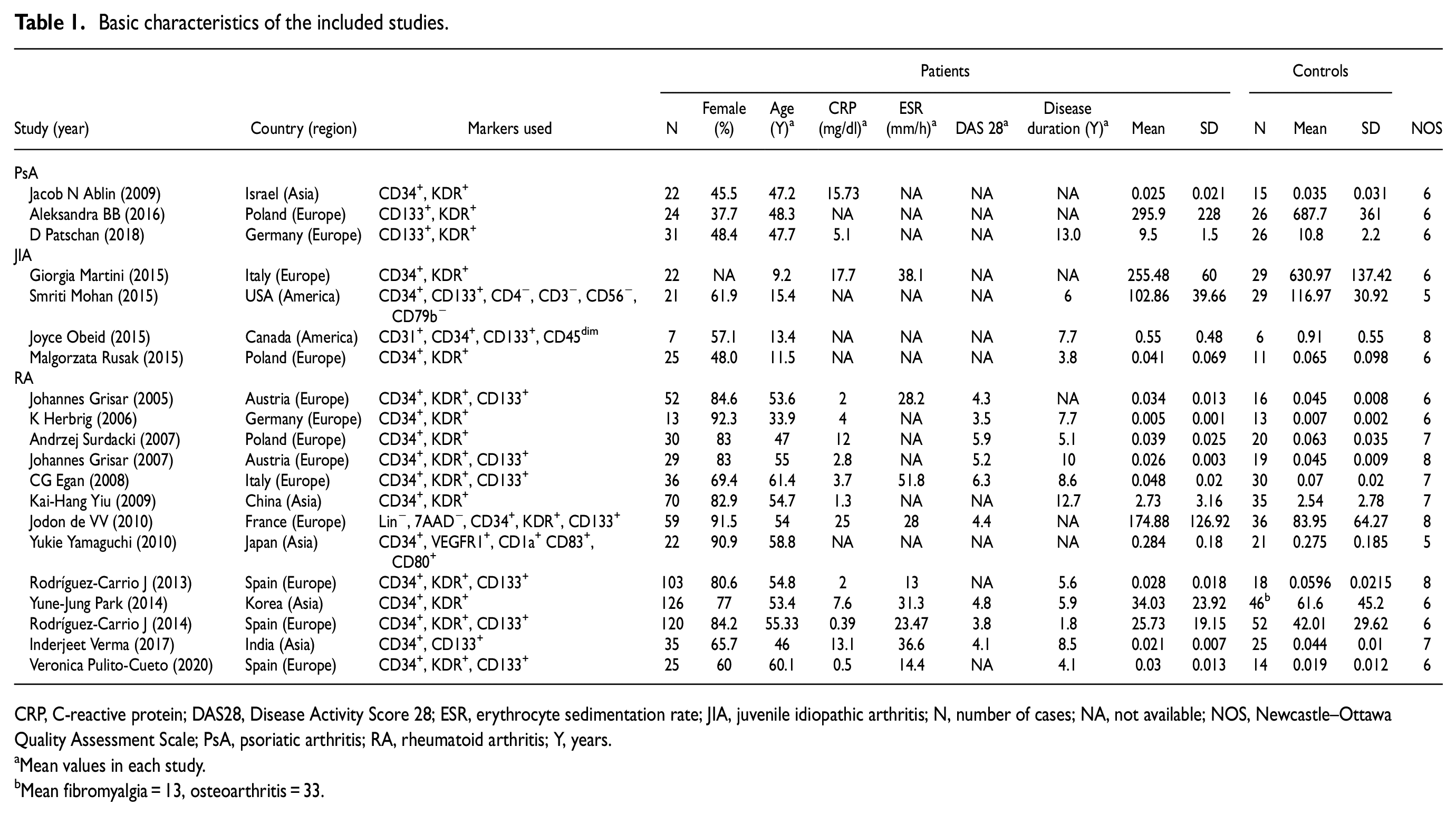
CRP, C-reactive protein; DAS28, Disease Activity Score 28; ESR, erythrocyte sedimentation rate; JIA, juvenile idiopathic arthritis; N, number of cases; NA, not available; NOS, Newcastle–Ottawa Quality Assessment Scale; PsA, psoriatic arthritis; RA, rheumatoid arthritis; Y, years.
Mean values in each study.
Mean fibromyalgia = 13, osteoarthritis = 33.
Pooled results
The levels of circulating EPCs were significantly lower in PsA patients than in controls using a fixed-effects model (SMD = −0.791, 95% CI = −1.136 to −0.446, p < 0.001), with no significant heterogeneity (I2 = 48.6%; Q = 3.89, p = 0.143). Meanwhile, a random-effects model showed no statistical difference in circulating EPC levels between JIA and control groups (SMD = −1.160, 95% CI = −2.578 to 0.259, p = 0.109), but significant heterogeneity was found (I2 = 91.6%; Q = 35.8, p < 0.001). Another random-effects model revealed significantly lower circulating EPC levels in RA patients compared to controls (SMD = −0.848, 95% CI = −1.474 to −0.221, p = 0.008), with significant heterogeneity (I2 = 92.7%; Q = 164.8, p < 0.001) (Table 2; Figure 2).
Pooled results of inflammatory arthritis.
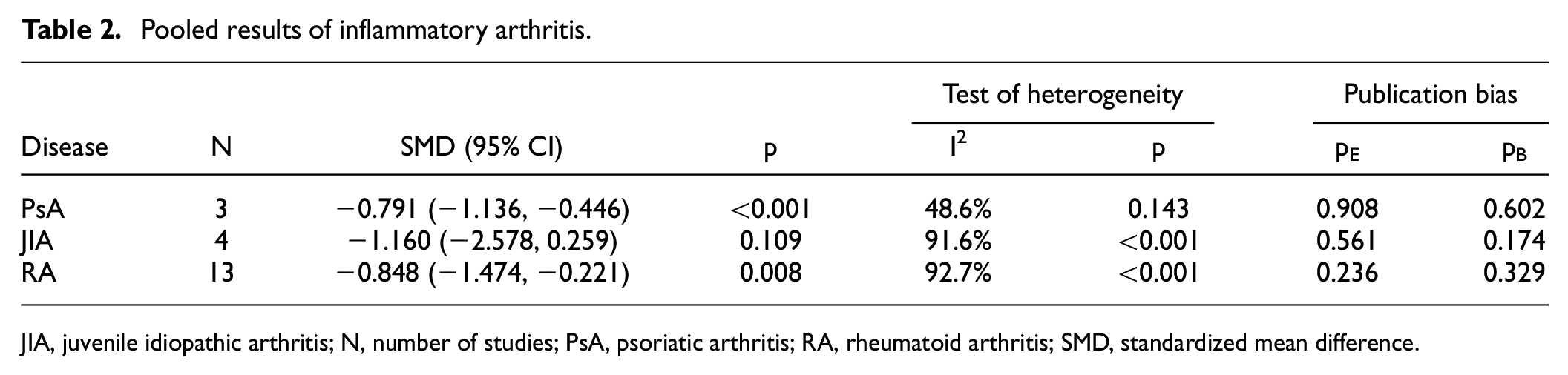
JIA, juvenile idiopathic arthritis; N, number of studies; PsA, psoriatic arthritis; RA, rheumatoid arthritis; SMD, standardized mean difference.
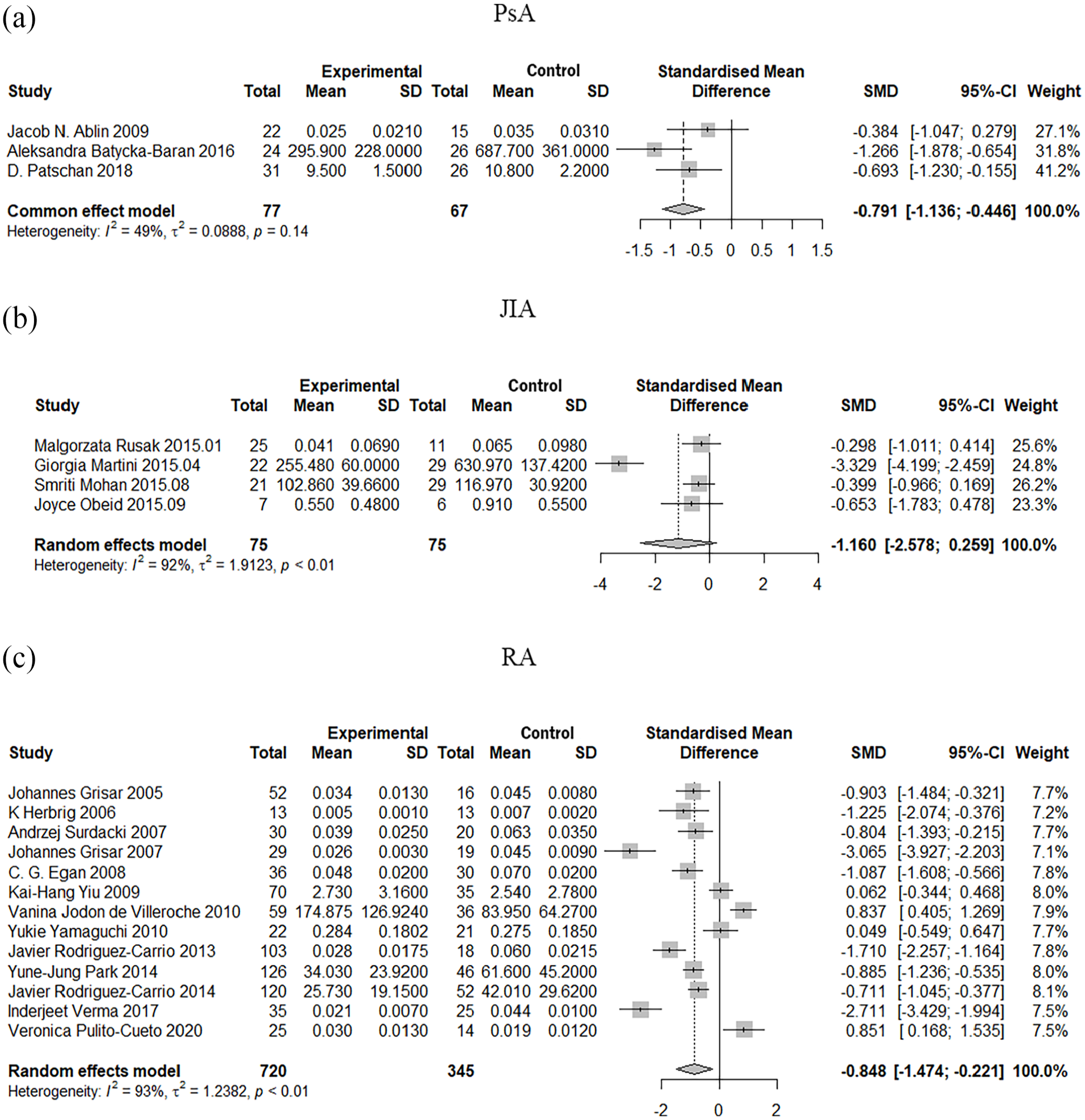
Forest plots on the difference in circulating EPC levels between patients and controls: (a) PsA vs controls group, (b) JIA patients vs controls group, and (c) RA patients vs controls group.
Subgroup analysis
The studies were stratified by region, markers used, age, ESR, DAS28, disease duration, and quality score, and the results are presented in Table 3. In PsA patients, lower levels of circulating EPCs were observed in studies conducted in the European population but not in the Asian population. Interestingly, we observed the same results in patients with RA. Furthermore, in young and middle-aged patients with RA (<60 years), there was a significant decrease in circulating EPC levels (pooled SMD = −0.976, 95% CI = −1.650 to −0.302, p = 0.005). However, no statistically significant difference was observed in older RA patients (≥60 years) (p = 0.892). In subgroups with ESR > 20 mm/h, DAS28 > 5.1, disease duration >6-year, and quality score ≥7, significantly lower levels of circulating EPCs were observed in RA patients (polled SMDESR = −0.889, 95% CI = −1.774 to −0.003, p = 0.049; polled SMDDAS28 = −1.617, 95% CI = −2.974 to −0.260, p = 0.020; polled SMDdisease duration = −1.575, 95% CI = −2.705 to −0.444, p = 0.006; polled SMDquality = −1.183, 95% CI = −2.221 to −0.145, p = 0.026).
Results of subgroup analyses.
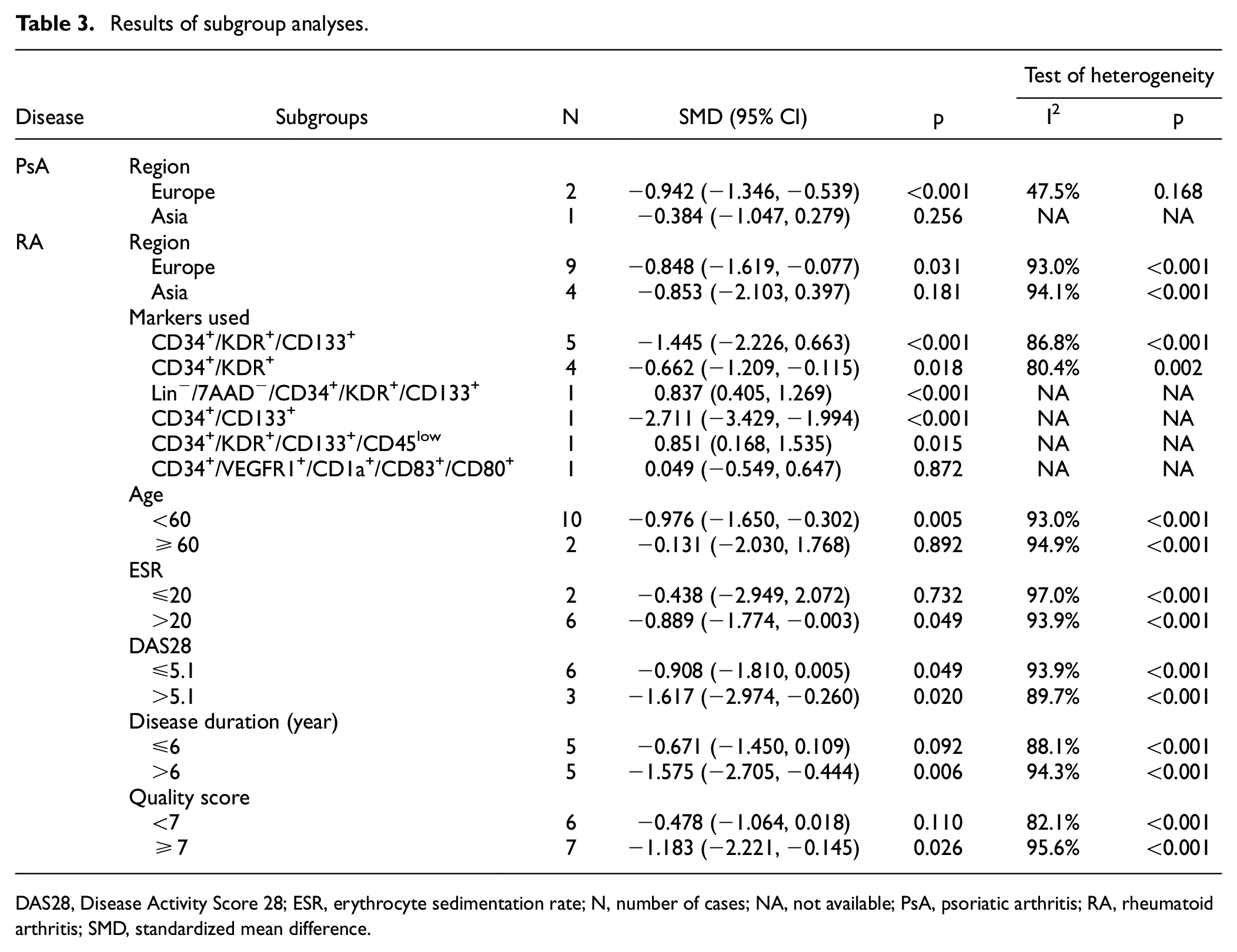
DAS28, Disease Activity Score 28; ESR, erythrocyte sedimentation rate; N, number of cases; NA, not available; PsA, psoriatic arthritis; RA, rheumatoid arthritis; SMD, standardized mean difference.
Meta-regression analysis and publication bias
To investigate potential sources of heterogeneity in EPC levels among patients with different types of arthritis, separate meta-regression analyses were conducted for the PsA, JIA, and RA groups. The results of these analyses are presented in Table 4. Our findings indicated that none of the following factors were identified as significant sources of heterogeneity: year of publication, patient sample size, proportion of female cases, age, disease duration, CRP, ESR, DAS28, and NOS score.
Results of meta-regression analyses.
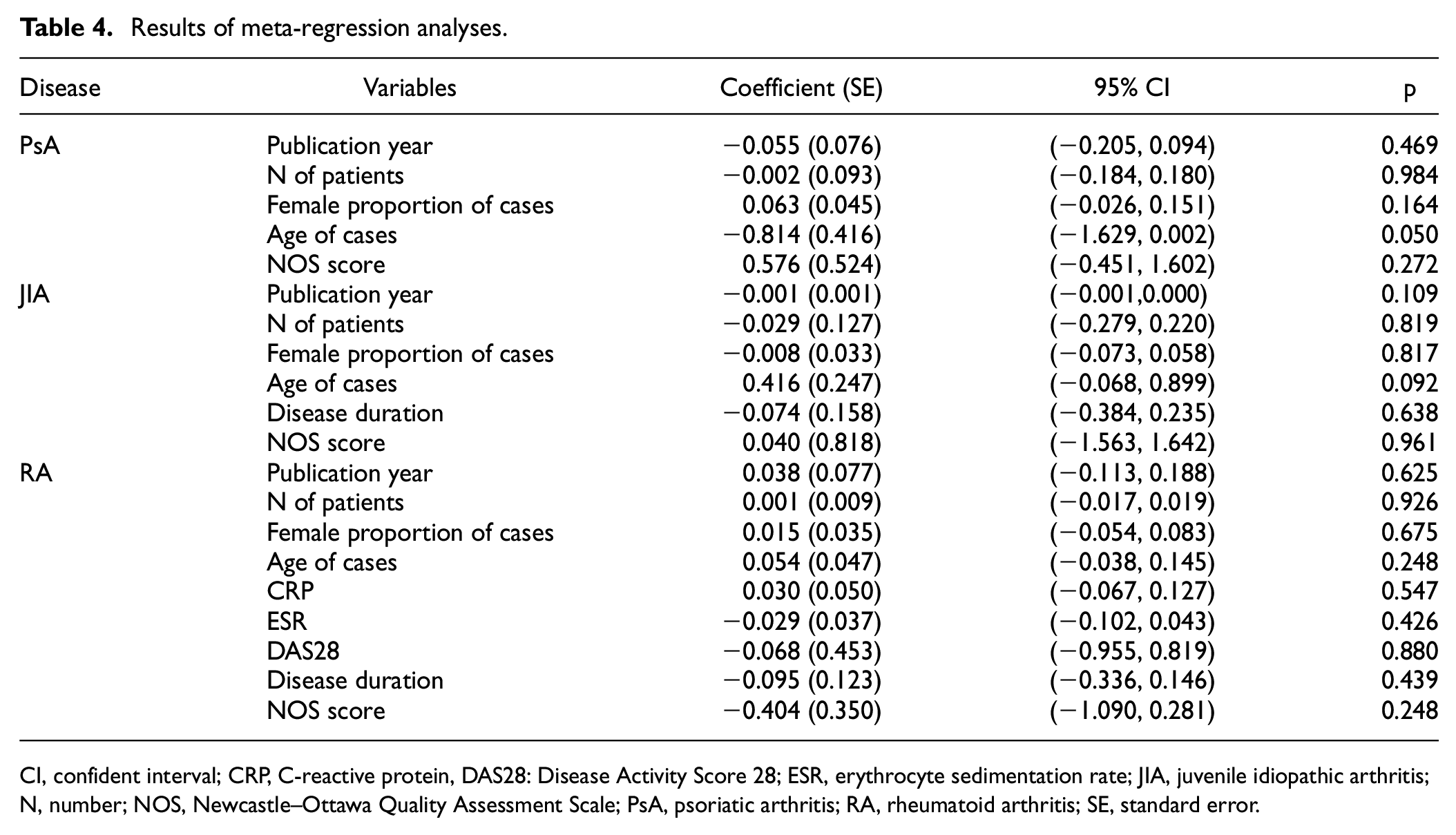
CI, confident interval; CRP, C-reactive protein, DAS28: Disease Activity Score 28; ESR, erythrocyte sedimentation rate; JIA, juvenile idiopathic arthritis; N, number; NOS, Newcastle–Ottawa Quality Assessment Scale; PsA, psoriatic arthritis; RA, rheumatoid arthritis; SE, standard error.
There is no statistically significant publication bias when comparing PsA patients or JIA patients or RA patients to controls, according to Egger’s test and Begg’s regression test (p > 0.05, Table 2). The funnel plot displayed visual symmetry, as shown in Supplemental Figure S1. However, we observed bias in the RA group. Removal of articles located outside the curve did not result in a significant change in the study results (SMD = −0.866, 95% CI = −1.055 to −0.677, p < 0.001). But this exclusion led to a significant reduction in heterogeneity (I2 = 0%, Q = 2.28, p = 0.810), as depicted in Supplemental Figure S2.
Sensitivity analysis
To assess the potential impact of individual studies on the overall results, we conducted a sensitivity analysis by systematically excluding one study at a time while analyzing the remaining studies. The findings revealed that no single study had a substantial effect on the pooled results, indicating the stability of our findings (refer to Supplemental Figure S3). The cumulative meta-analysis results (refer to Supplemental Figure S4) demonstrated that as more studies were included over time and the sample size increased, the CIs became narrower and reached a stabilized state. In the case of the RA group, the inclusion of two studies in 2010 initially influenced the results, but subsequent studies contributed to the stabilization of the findings.
Subsequently, we performed a meta-analysis of the main results using the HKSJ method, which yielded findings generally consistent with the DerSimonian–Laird method. The HKSJ analysis results (refer to Supplemental Figure S5) indicated that levels of EPCs were significantly lower in patients with PsA compared to controls (SMD = −0.791, 95% CI = −1.136 to −0.446, p < 0.001). However, no statistically significant difference in EPC levels was observed in patients with JIA compared to controls (SMD = −1.159, 95% CI = −3.462 to 1.143, p = 0.207). In the case of RA patients, EPC levels were significantly lower compared to controls (SMD = −0.848, 95% CI = −1.553 to −0.143, p = 0.022). The meta-analysis results for the RA group, depicted in Supplemental Figure S6, exclusively included studies that reported the proportion of EPCs in PBMCs. These results revealed a significantly lower number of EPCs in RA patients compared to controls (SMD = −1.164, 95% CI = −1.954 to −0.375, p = 0.004).
Discussion
EPCs were first described by Asahara in 1997. 45 They are precursor cells of endothelial cells (ECs) derived from hematopoietic stem cells of the bone marrow. After migration to the peripheral circulation, they release a variety of active molecules and growth factors and are involved in endothelial repair and neoangiogenesis through differentiation into mature ECs. 46 However, the mechanism of EPCs-mediated vascular repair remains unclear. Animal studies suggest that circulating EPCs may replace dysfunctional ECs under physiological conditions through endogenous repair mechanisms against endothelial injury. 47 The number of circulating EPCs depends on vessel wall integrity and their migration capability. 48 Moreover, there is growing evidence that EPCs play a crucial role in maintaining vascular homeostasis, increasing neovascularization after ischemic injury, and repairing existing vessels.49,50 Following this discovery, EPCs have been extensively investigated for their potential medical use in regenerative medicine and as markers of disease activity in autoimmune diseases in many cases. 51
Endothelial dysfunction is a key process that triggers vascular injury and accelerates the development of atherosclerotic plaques. Evidence suggests that the reserve and mobilization capacity of EPCs may progressively deplete in chronic inflammation. 52 Previous studies have indeed shown a reduced number of circulating EPCs and altered function in patients with systemic lupus erythematosus. 53 Since inflammatory arthritis is characterized by changes in the inflammatory response, it is reasonable to assume that circulating EPC levels may vary among patients with inflammatory arthritis. The relationship between circulating EPC levels and inflammatory arthritis has been examined in various studies, but the results are inconsistent. Some studies have reported lower circulating EPC levels in patients with RA, PsA, or JIA compared to controls.21,31,32,41,43 Moreover, studies have been conducted on circulating EPC levels with RA disease activity, and Spinelli et al. 54 revealed that short-term anti-Tumor Necrosis Factor (TNF) therapy was able to increase circulating EPC levels, and circulating EPC levels were negatively correlated with DAS28 in RA patients. However, Yiu et al. 39 and Yamaguchi et al. 40 reported no significant difference in circulating EPC levels between patients with RA and controls. Jodon de Villeroche et al. 18 and Pulito-Cueto et al., 19 who showed the opposite results, demonstrated that RA patients had higher EPC levels than controls. Some drugs may cause elevated levels of circulating EPCs, and baseline treatment of RA patients may explain part of the elevated levels of circulating EPCs seen in these studies. Notably, most studies showed no significant difference in circulating EPC levels in patients with JIA compared with controls,20,33,34 and circulating EPC levels were not enhanced by disease-specific anti-inflammatory treatment. Therefore, our aim was to explore the role of circulating EPCs in inflammatory arthritis (PsA, JIA, RA) through this meta-analysis, and the differences in circulating EPC levels in different inflammatory arthritic subtypes.
This meta-analysis included 20 studies with a total of 77 PsA patients, 75 JIA patients, and 720 RA patients. The results showed that circulating EPC levels were significantly decreased in three studies of PsA patients, while four studies found no significant difference in circulating EPC levels in JIA patients compared to controls. Moreover, 13 studies reported significantly decreased circulating EPC levels in RA patients compared to controls. However, interpreting these findings requires considering several factors. Firstly, the lack of standardized methods and criteria for identifying and describing circulating EPCs may account for the conflicting reports about their nature in disease states and their varying levels in inflammatory arthritis patients vs controls. Our subgroup analysis based on the different markers used showed reduced heterogeneity, but significant heterogeneity still remained. Meta-regression analyses suggested that factors such as the number of patients, publication year, the female proportion of cases, age, CRP, ESR, DAS28, disease duration, and NOS score were not the sources of heterogeneity among the studies. Secondly, heterogeneity can also be attributed to the influence of medications on circulating EPC levels. For instance, prednisolone and TNF-α blockers have been shown to increase circulating EPC levels,37,54 while methotrexate may cause a decrease. 35 However, the lack of detailed information on baseline treatment in the included studies precluded assessing their effects. Thirdly, variations in FCM platforms and reagents could have an impact on the measurement of circulating EPC levels. Nevertheless, in all the included studies, EPC levels were determined with reference to PBMCs, and our pooled effect values were reliable because they combined different methods or units from different studies. After taking all these factors into account, we found no significant difference in circulating EPC levels between JIA patients and controls. Although circulating EPC levels were significantly lower in PsA patients, the small number of included studies and low sample size limit its credibility as a diagnostic marker for the disease, and larger studies are needed to confirm this finding. While the exact mechanisms remain unclear, it is well established that RA patients have significantly lower levels of circulating EPCs. Therefore, we believe that EPC levels could serve as a valuable biomarker to supplement the diagnosis of RA, given the influence of the inflammatory microenvironment on EPCs reserve and mobilization capacity.
Subgroup analysis revealed that circulating EPC levels were significantly lower in PsA and RA patients than in controls in Europe but not in Asia. This could be attributed to genetic and environmental differences between the individuals from different regions. 55 Furthermore, different NOS scores affected circulating EPC levels in RA. In contrast to controls, circulating EPC levels in JIA patients were not significantly different. Previous studies have shown that the reduction in circulating EPC levels found in cohort studies of patients with coronary artery disease is associated with increasing age itself. 16 We suspect that the inconsistency between JIA and other arthritis types is due to the differences in age and the limited number of JIA studies. And in RA patients, we observed significantly lower levels of EPCs in the subgroup of young and middle-aged individuals (<60 years), while no significant difference was found in the older patient group (≥60 years). However, it is important to note that the limited number of included studies in the older subgroup restricts the generalizability of these findings. Thus, multicenter studies are needed to confirm these findings. Importantly, we observed a significant negative correlation between ESR, DAS28, disease duration, and circulating EPC levels in RA patients, indicating that higher disease activity and longer disease duration may result in a more pronounced decrease in circulating EPC levels. In fact, studies have demonstrated that long-term (>1 year) RA patients exhibited depletion of EPCs compared to earlier patients, and circulating EPC levels were inversely correlated with disease activity.17,56 Therefore, decreased levels of circulating EPCs may be involved in the development and progression of RA, partially explaining the associations between higher disease activity in RA and increased odds of risk of CV events. 57 We believe that circulating levels of EPCs are important in aiding the assessment of RA severity.
To the best of our knowledge, this is the first comprehensive meta-analysis of circulating EPC levels in patients with inflammatory arthritis (PsA, JIA, RA). Nonetheless, we acknowledge several limitations to our study. First, the significant heterogeneity across the studies may limit the generalizability of our pooled results. Owing to insufficient data in the included studies, the source of heterogeneity could not be fully understood. Other confounding factors, such as biochemical indicators, drug use, and body fat composition, may also affect circulating EPC levels in some individuals, which may account for the high degree of heterogeneity. Secondly, the lack of information on drug and biologic use in the included studies prevents further exploration of their effects on the relationship between circulating EPC levels and inflammatory arthritis. Third, JIA itself is a heterogeneous population with well-defined subgroups (e.g., RA-like, PsA-like, AS-like, and other forms), but the studies included here do not clearly distinguish between subtypes of disease, which somewhat limits our interpretation of the pooled data. Finally, the included studies were of hospital or single-center designs. Most of the studies were conducted in European countries, and there was a certain selection bias of patients and inconsistent results.
In conclusion, our study found that circulating levels of EPCs differed significantly among various subtypes of inflammatory arthritis, with patients diagnosed with RA or PsA showing markedly lower levels. These findings serve as a valuable reference for considering circulating EPCs as a potential complementary diagnostic tool for RA or PsA. Further research in this area could potentially lead to more accurate and effective diagnosis and treatment of RA or PsA, improving patient outcomes and quality of life.
Supplemental Material
sj-docx-1-imj-10.1177_10815589231182320 – Supplemental material for Could endothelial progenitor cells complement the diagnosis of inflammatory arthritis? A systematic review and meta-analysis
Supplemental material, sj-docx-1-imj-10.1177_10815589231182320 for Could endothelial progenitor cells complement the diagnosis of inflammatory arthritis? A systematic review and meta-analysis by Hui Zhao, Lanlan Fang, Yuting Chen, Yubo Ma, Qiang Zhou, Shengqian Xu, Zongwen Shuai, Guoqi Cai and Faming Pan in Journal of Investigative Medicine
Footnotes
Author contributions
HZ, LF, and FP conceived, designed, and performed the experiments. HZ wrote the article. YC, YM, and QZ analyzed the data. SX, ZS, and GC contributed reagents/materials/analysis tools. FP is the guarantor of the entire study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from the National Natural Science Foundation of China (81773514, 82073655) and the funds for Scientific Research of Anhui Medical University (2021lcxk004).
Statement of ethics
The ethical statement does not apply, as this study is based on published literature.
Data availability statement
All data generated or analyzed during this study are included in this article and its supplemental material files. Further enquiries can be directed to the corresponding author.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.