
Abstract
Background
Parathyroid hormone (PTH) revealed a positive action on progenitor cells released from bone marrow, and many mechanisms supported PTH as a tool to improve stem cell-based therapy in experimental models of ischemia. Elevated PTH resulted in increased mobilization of progenitors into the peripheral blood of patients affected by untreated primary hyperparathyroidism. A frequent finding in uremic patients is a higher PTH level, and different therapeutic strategies are adopted and implemented to achieve an intermediary PTH level. On the contrary, the amount of progenitors commonly results to be extremely reduced.
Objective
In the present study, we investigated, in a cohort of uremic patients, the effect of different levels of PTH on mobilization of progenitor cell populations.
Methods
Eighty patients (26 women, 54 men) were enrolled. Following the Kidney Disease Outcomes Quality Initiative (KDOQI) guidelines, patients were divided in 3 groups for PTH levels: low-PTH group with a PTH level lower than 150 pg/mL (n = 25), KDOQI-PTH group with a PTH level between 150 and 300 pg/mL (n = 37), and high-PTH group with a PTH level higher than 300 pg/mL (n = 18). Patients with high levels of PTH were treated differently to achieve KDOQI targets: 5 received intravenous calcitriol and P binders, 3 received intravenous paracalcitriol, and 10 received cinacalcet. We quantified, by the combination of surface markers (CD45+, CD34+, CD31+, and c-kit+), the number of hematopoietic and endothelial progenitor cells.
Results
High-PTH group demonstrated a significantly higher level of CD45+/CD34+/c-kit+ with respect to low-PTH and KDOQI-PTH groups (1.02 [SD, 0.12] vs. 0.56 [SD, 0.14] cells/uL, P < 0.01; and 1.02 [SD, 0.12] vs. 0.46 [SD, 0.20] cells/uL, P < 0.05). CD45+/CD34+/CD31+ levels resulted significantly increased in the KDOQI-PTH group compared with those observed in the low- (1.83 [SD, 0.72] vs 1.26 [SD, 0.83] cells/μL, P = 0.04) and high-PTH groups (1.83 [SD, 0.72] vs 1.20 [SD, 1.15] cells/μL, P = 0.04). Receiver operating characteristic analyses were performed to define the ability of CD45+/34+/31+ to identify the presence of an optimal PTH status (>150 but <300 pg/mL) among all hemodialysis patients. The area under the curve of CD45+/34+/31+ was 0.674 (95% confidence interval [CI], 0.501-0.819) with a best cutoff level of 1.36 cells/μL (sensitivity, 80.0; specificity, 59.1; P < 0.05). After 4 months, we demonstrated an increase in endothelial progenitor cell number in 13 patients with secondary hyperparathyroidism that achieved KDOQI targets in PTH levels after pharmacological treatment.
Conclusions
Our data confirm, with acknowledged limitations due to the low number of patients, the effect of PTH on bone marrow-derived progenitor cells emphasizing that, in our cohort, an intermediary PTH level, achieved following specific guidelines, results in an equilibrate balance between different subsets of progenitor cells.
Different stimuli were recently investigated while operating on bone marrow and inducing direct mobilization of bone marrow-derived stem cells. 1 Physiologically, these cells develop through an organized developmental hierarchy initiated by hematopoietic stem cells (HSCs) that give rise to progressively more committed progenitor cells such as the so-called endothelial progenitor cells (EPCs) moving to the sites of the vascular injury to repair endothelial damage or terminally differentiating in the full spectrum of circulating blood cells.2,3 Parathyroid hormone (PTH) revealed a positive action on progenitor cells released from bone marrow, and many mechanisms supported PTH as a tool to improve stem cell-based therapy in experimental models of endothelial dysfunction and ischemia. 4 Brunner et al. 5 showed that elevated PTH serum levels result in increased mobilization of progenitors into the peripheral blood of patients affected by untreated primary hyperparathyroidism. A frequent finding in patients with renal failure is a higher PTH level, associated with a significantly increased relative risk of death from cardiovascular disease and a worsened endothelial function, compared with groups with a lower PTH level. 6 Different medical or surgical therapeutic strategies are adopted and implemented to achieve an intermediary PTH level following specific guidelines against secondary hyperparathyroidism.7,8 With these concepts as starting points, the amount of progenitor cells in patients with renal failure should be expected rising together with the PTH levels, but this hypothesis is in contrast with common results of a reduced mobilization of progenitors in these patients. 9 The aim of the present study was to investigate, in a cohort of hemodialysis (HD) patients, the effect of different levels of PTH on mobilization of progenitor cell populations.
Materials and Methods
Patients
Between May 2008 and February 2009, we enrolled 80 patients (26 women, 54 men; mean age, 54 [SD, 14] years; mean dialysis age, 43 months; residual glomerular filtration rate, 2.3 [SD, 0.6] mL/min), receiving regular renal replacement treatment with standard bicarbonate dialysis (138 mmol/L Na, 35 mmol/L HCO3, 1.5 mmol/L K, 1.25 mmol/L Ca, and 0.75 mmol/L Mg) by cuprophane or semisynthetic membranes (dialysis filter surface area, 1.1-1.7 m2) with a dialytic rhythm of 4-hour sessions 3 times a week. Patients’ clinical condition was stable. No racial differences were present. All patients had their dry weight stable for at least 3 months, had achieved a normotensive edema-free state, and had an adequate dialysis delivery (Kt/V ≥ 1.3). Throughout the study period, each patient complied with fluid and food restrictions, with a constant ultrafiltration volume being maintained. The subjects were excluded if they had a condition leading to a catabolic state, such as malignancy, infection requiring antibiotics within 2 months before enrollment, or corticosteroid treatment. Other criteria for exclusion were smoking, secondary hypertension, and statin therapy. All HD patients were usually given subcutaneous erythropoietin (EPO) to achieve target hemoglobin (Hb) level between 11 and 12 g/dL for at least 6 weeks, and none had received packed red cell transfusion in the 4 months preceding the start of the study. Patients underwent treatment with angiotensin-converting enzyme inhibitors, calcium antagonists, angiotensin receptor antagonists, nitrate agents, diuretics, vitamin D analog, and calcium-containing phosphate binders. None of the subjects enrolled had undergone surgery in the 6 months before the study. Following the Kidney Disease Outcomes Quality Initiative (KDOQI) guidelines, patients were divided in 3 groups for PTH levels: low-PTH group with a PTH level lower than 150 pg/mL (n = 25), KDOQI-PTH group with a PTH level between 150 and 300 pg/mL (n = 37), and high-PTH group with a PTH level higher than 300 pg/mL (n = 18). Patients with high levels of PTH were treated differently to achieve KDOQI targets: 5 received intravenous calcitriol and P binders, 3 received intravenous paracalcitriol, and 10 were treated with cinacalcet. After a follow up of 4 months, only 13 patients attained a PTH level between 150 and 300 pg/mL and were again examined to establish shifting in progenitors’ quantification.
Control Group
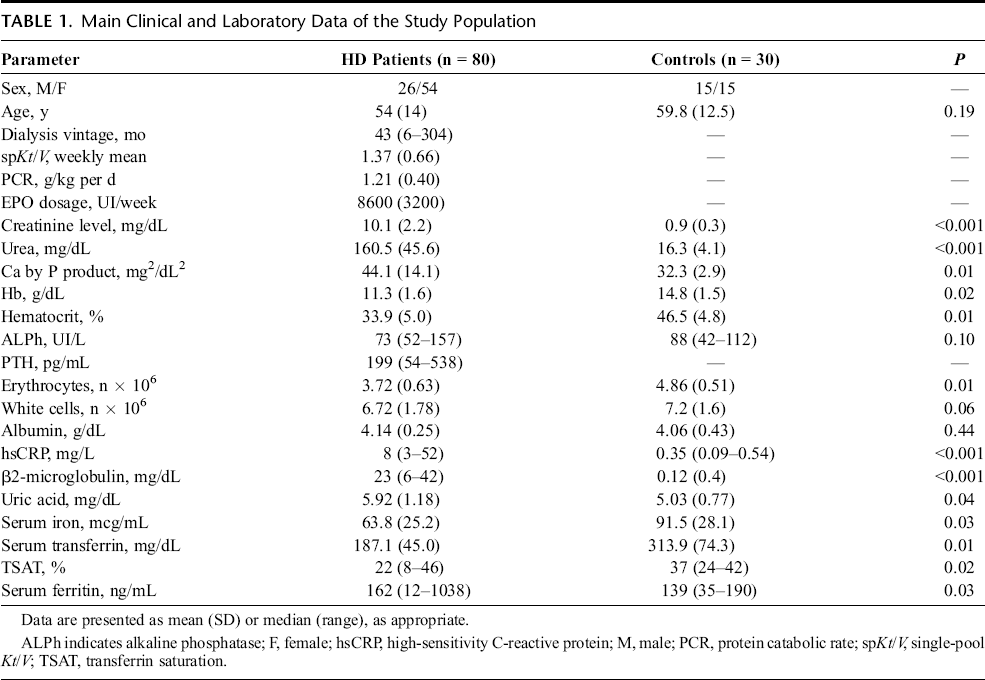
The control group consisted of 30 subjects (15 women, 15 men; mean age, 59.8 [SD, 12.5] years) without evidence in their clinical history and clinical examination of atherosclerotic disease, hypertension, diabetes, or hypercholesterolemia. Moreover, none of the control subjects was on drugs. Data from patients and control group are summarized in Table 1.
Main Clinical and Laboratory Data of the Study Population
Laboratory Measurements
Peripheral venous blood samples were taken in the midweek interdialytic day via a 20-gauge butterfly inserted into a forearm vein. Biochemical parameters were measured in all patients, according to the standard methods used in the routine clinical laboratory. All samples were processed within 2 hours after collection. Laboratory parameters were assessed: serum concentration of intact PTH, total calcium, inorganic phosphate, sodium, potassium, creatinine level, urea nitrogen, aminotransferases, gamma-glutamyl transpeptidase, alkaline phosphatase, glucose, complete blood count (including Hb), hematocrit, leukocytes, and platelets. In addition, thyroid parameters thyroid-stimulating hormone, free thyroxine, and free triiodothyronine were measured.
Quantification of Circulating Progenitor Cells
We performed a protocol similar to Brunner et al. 31 Briefly, cytometric analyses were performed using a flow cytometer (EPICS-XL; Beckman-Coulter, Brea, CA) according to the International Society of Hematotherapy and Graft Engineering guidelines and to a standard protocol. 10 Each analysis included 100,000 events. For immunophenotyping, the following monoclonal antibodies were used: CD45 fluorescein isothiocyanate- or CD45 phycoerythrin (PE)-conjugated antibody, combined with CD34 PE-cyanine 5 conjugated antibody and with CD31 fluorescein isothiocyanate-conjugated antibody to identify EPC cells or with c-kit+ (CD117) PE-conjugated antibody to identify HSCs cells (Beckman Coulter). Samples were excluded from the evaluation in case of high amounts of cell detritus or smudge cells (>20%), no exact delimitable population in any dot plot, or high numbers of positive cells in the isotype control (>2%; Fig. 1B). We quantified, by the combination of surface markers (CD45+, CD34+, CD31+, and c-kit+), the number of CD45+/CD34+, measured while including other populations and because its reduction was recently confirmed as independent and significant predictor for vascular risks and all-cause mortality in patients on chronic HD 11 ; subsequently, we enumerated CD45+/CD34+/c-kit+ named as HSCs and CD45+/CD34+/CD31+, indicated as a subtype that is able to develop to endothelial cells, named as EPCs.
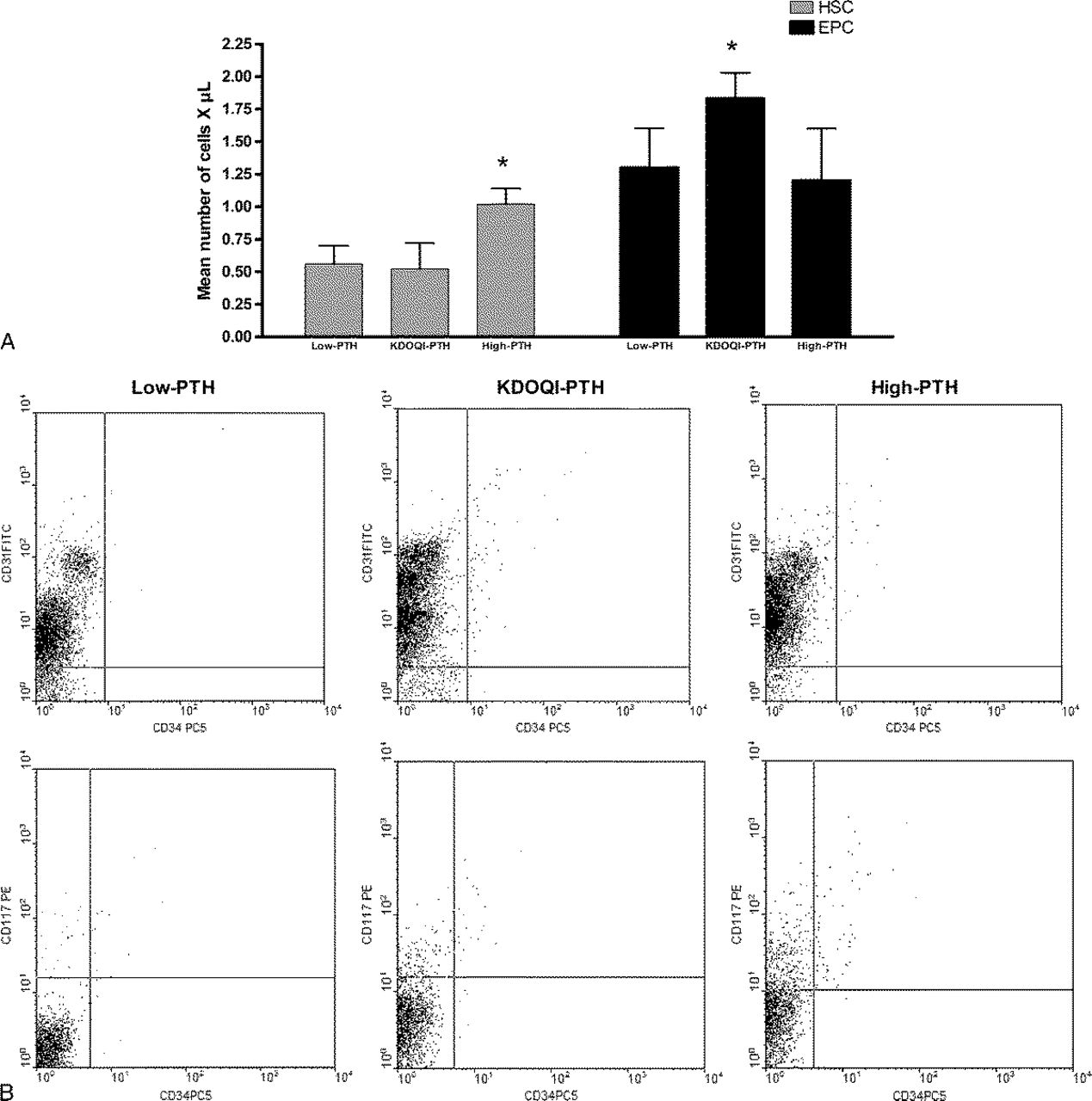
Hematopoietic stem cell and EPC populations in the peripheral blood of HD patients divided for PTH levels. A, Histogram shows that HSC was significantly increased in the high-PTH group with respect to other groups (*P < 0.05), whereas EPC increased significantly in patients with PTH at target following KDOQI guidelines with respect to other groups (*P < 0.05). B, Representative fluorescence-activated cell sorter scan of data of patients belonging to single groups.
Statistical Analysis
Statistical analysis was performed with the MedCalc (ver. 8.0; MedCalc Software, Mariakerke, Belgium) software and the Graphpad Prism (ver. 4.0; GraphPad Software, La Jolla, CA) package. Data are presented as mean (SD) or median (range), as appropriate. Differences between groups were established by unpaired t test for normally distributed values and by Kruskal-Wallis analysis followed by Dunn test for nonparametric values. Receiver operating characteristic analysis was used to calculate the area under the curve (AUC) for EPC populations and to find the best cutoff values able to identify the presence of an optimal PTH status (>150 but <300 pg/mL). Sensibility and specificity were also computed. All results were considered significant if P < 0.05.
Results
Clinical Characteristics and Basal Concentration of Progenitor Cells in the Peripheral Blood
The main characteristics of the study cohort patients and healthy controls and the basal concentration of progenitor cells in the peripheral blood are summarized in Table 1. Hemodialysis patients had significantly lower basal levels of CD45+/CD34+ (1.69 [SD, 0.87] vs 3.55 [SD, 1.37], P < 0.01) and CD45+/CD34+/CD31+ (1.80 [SD, 1.00] vs 2.26 [SD, 0.54], P < 0.05) than healthy controls. Hemodialysis patients and healthy controls had no statistically significant difference in CD45+/CD34+/c-kit+ (0.71 [SD, 0.66] vs 0.64 [SD, 0.12], not significant).
Differences in Progenitors Level between PTH Groups
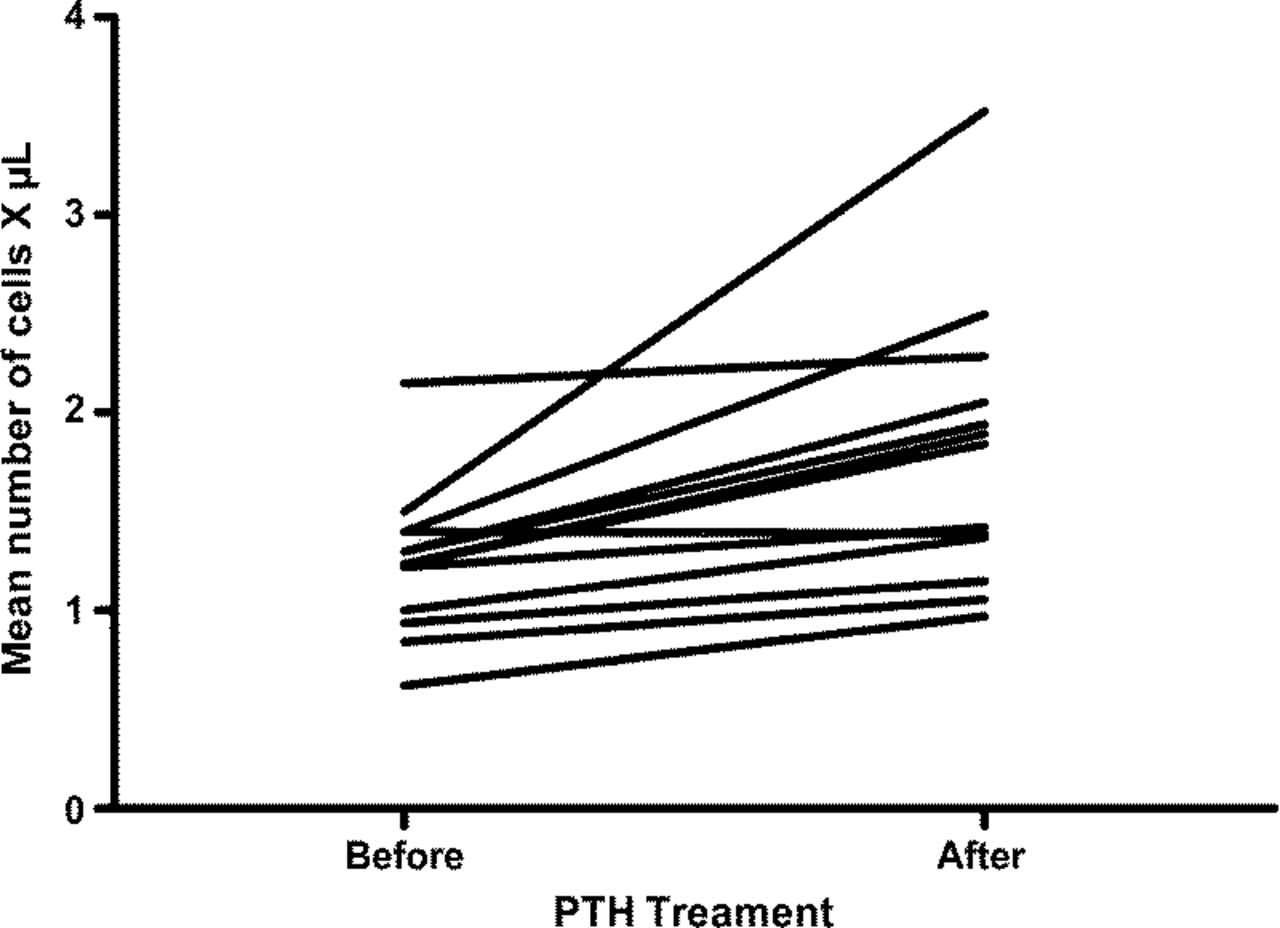
Hemodialysis patients achieving a KDOQI-PTH status (>150 but <300 pg/mL) showed reduced circulating levels of CD45+/34+ cells compared with those belonging to the low-PTH group (1.32 [SD, 0.50] vs 1.88 [SD, 0.96] cells/μL, P = 0.03) and to the high-PTH group (1.32 [SD, 0.50] vs 2.01 [SD, 1.02] cells/μL, P = 0.03). High-PTH group demonstrated a significantly higher level of CD45+/CD34+/c-kit+ with respect to low- and KDOQI-PTH group (1.02 [SD, 0.12] vs. 0.56 [SD, 0.14] cells/uL, P < 0.01; and 1.02 [SD, 0.12] vs. 0.46 [SD, 0.20] cells/uL, P < 0.05). CD45+/CD34+/CD31+ levels resulted significantly increased in the KDOQI-PTH group compared with those observed in the low- (1.83 [SD, 0.72] vs 1.26 [SD, 0.83] cells/μL, P = 0.04) and high-PTH group (1.83 [SD, 0.72] vs 1.20 [SD, 1.15] cells/μL, P = 0.04). Any statistical difference in both CD45+/CD34+ and CD45+/CD34+/CD31+ EPC populations was noticed between the low- and the high-PTH groups, and in CD45+/CD34+/c-kit+, between KDOQI and low-PTH groups (Fig. 1A). After 4 months, we demonstrated an increase in EPC cell numbers in 13 patients with secondary hyperparathyroidism that achieved KDOQI targets in PTH levels after pharmacological treatment (Fig. 2).
Endothelial progenitor cell populations quantification in the peripheral blood of 13 patients with hyperparathyroidism reaching KDOQI-PTH level target after pharmacological treatment (P < 0.05).
Receiver Operating Characteristic Analysis
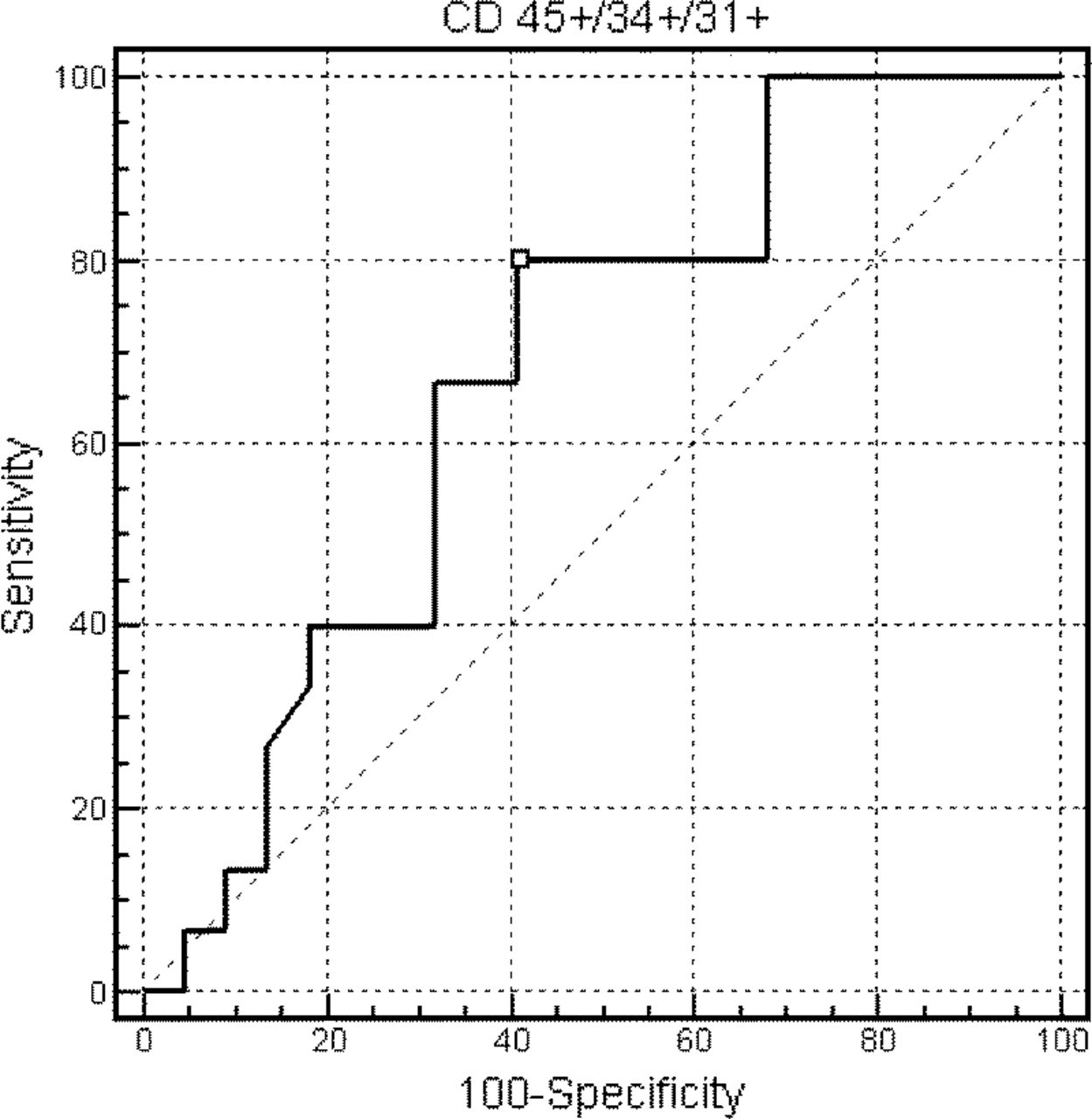
Receiver operating characteristic analyses were performed to define the ability of CD45+/34+/31+ to identify the presence of an optimal PTH status (>150 but <300 pg/mL) among all HD patients. The AUC of CD45+/34+/31+ was 0.674 (95% CI, 0.501-0.819) with a best cutoff level of 1.36 cells/μL (sensitivity, 80.0; specificity, 59.1; P < 0.05; Fig. 3).
Receiver operating characteristic analyses was performed to define the ability of EPC to identify the presence of an optimal PTH status following KDOQI guidelines (>150 but <300 pg/mL) among all HD patients. The AUC of EPC was 0.674 (95% CI, 0.501-0.819) with a best cutoff level of 1.36 cells/μL (sensitivity, 80.0; specificity, 59.1).
Discussion
Our analysis permitted us to explore the mobilization of different subsets of progenitor cells in relationship to PTH levels in HD patients. An important finding was to confirm that PTH levels similar to Brunner et al.31 resulted in an enhanced progression of progenitors to endothelial committed cells, but simultaneously, higher PTH levels caused an opposite effect causing a reduced EPC release. In progenitors’ biology, mobilization of adult stem cells is a succession of specific progenitors and precursors, characterized by the progressive and rapid loss of stem cell potential. The most primitive progenitors are found near the thin layer of cells lining the bone marrow cavity, known as the endosteum, and with their differentiation, they migrate into the medullary marrow cavity. 12 While maturing in the circulation, HSCs and EPCs are characterized by the gradual expression and/or disappearance of surface markers. 13 Many stimuli are able to rouse the mobilization of HSCs into the bloodstream and transformation in EPCs. 14 The examples are by ischemia through stromal cell-derived factor 1 and vascular endothelial growth factor increase 15 ; EPO 16 ; granulocyte colony-stimulating factor (CSF) and granulocyte monocyte CSF, usually used to harvest HSCs from blood in hematology; statins 17 ; and physical exercise. 18 In recent times, we showed that revascularization performed on HD patients affected by critical peripheral artery disease stimulated release of progenitor cells from the bone marrow, and prostanoids improved this mechanism. 19 In addition, a physiologic hemodynamic stress, such as dipping hands in icy water (named cold pressor test), was able to rapidly increase progenitor cells. 20 Furthermore, we found elevated numbers of EPCs in patients undergoing HD, reflecting the direct response of bone marrow to hemodynamic stress on vessels. 21 Latest studies have highlighted the potential benefit of PTH on the mobilization of progenitors. 22 In human, patients who had previously failed to produce a sufficient number of HSC in their peripheral blood for therapeutic aims, the pretreatment with PTH followed by the filgrastim, a granulocyte-CSF analog for up to 14 days permitted to meet the therapeutic mobilization criteria. 4 Parathyroid hormone signaling to osteoblasts resulted in an increase in the number of c-kit+ cells. 23 After PTH treatment, the number of all cells and in particular of HSCs in S, G2, and M phases, respectively, was significantly increased compared with the control group, reflecting an enhanced proliferation activity through PTH. 24 The same group demonstrated in animal models that PTH application after myocardial infarction increased migration of angiogenic CD45+/CD34+ progenitor cells to the ischemic heart attenuating ischemic cardiomyopathy. 5 In these studies, PTH treatment was administered for a short period, whereas in our model, patients are continuously stimulated by PTH for parathyroid adenomas. In fact, a prolonged decrease in serum calcium and vitamin D (1,25[OH]2D3), and increase in serum phosphorus, such as in patients with chronic renal failure, lead to the appropriate secondary increase in serum PTH. This secondary hyperparathyroidism involves increases in PTH gene expression, synthesis, and secretion, and if chronic, to proliferation of the parathyroid cells. 25 Recent clinical practice guidelines are designed to focus on the problem early in the course of kidney disease, when it is recommended to evaluate the levels of PTH and to intervene early if the levels are elevated. While kidney disease progresses, efforts to control hyperparathyroidism will need to be intensified, and several therapeutic options are available, such as phosphate binders, repletion of vitamin D, the use of active vitamin D sterols, whereas in patients on dialysis, therapeutic options involve the full spectrum of agents including the use of calcimimetic agents or vitamin D analogs, surgical parathyroidectomy, and evaluation of appropriate levels of dialysate calcium. 26 The studied group was divided into 3 subgroups for PTH levels following the National Kidney Foundation-Dialysis Outcomes Quality Initiative Clinical Practice Guidelines, an established and widely accepted set of recommendations for bone metabolism and disease in chronic kidney disease. 27 In accordance with literature, CD45+/CD34+ showed a lower level in HD patients than in control population. Usually, it was attributed to cell apoptosis due to an increase in oxidative stress and correlated to defective neovascularization and endothelial dysfunction.28,29 In patients on long-term HD, Herbrig et al. 30 found that the migratory activity of EPCs was markedly altered, as well as their adhesion to the protein matrix and to endothelial cells with respect to a healthy population. Hematopoietic stem cells effectively increased in high-PTH group, but we considered, as high PTH, levels higher than 300 mg/dL, whereas Brunner et al. 31 assumed an elevated amount of approximately 160 mg/dL usually believed as PTH optimal target, following KDOQI, in renal failure patients on HD. Endothelial progenitor cells instead showed higher levels in the group achieving KDOQI-PTH levels. Receiver operating characteristic analysis permitted us to define that PTH levels at target, following KDOQI guidelines, resulted in the levels of EPCs (1.36 cells/μL) better than the analysis conducted with high- and low-PTH groups. Patients with high PTH levels received pharmacological treatment to achieve KDOQI-PTH targets. Only 13 patients reached this target in 4 months, and EPC was quantified another time, confirming an enhanced mobilization. In conclusion, our data confirm, with acknowledged limitations due to the low number of patients, the effect of PTH on bone marrow-derived progenitor cells emphasizing that, in our cohort of patients, an intermediary PTH level, achieved the following specific guidelines, result in an equilibrate balance between different subsets of progenitor cells.