
Abstract
Cirrhosis, an advanced stage of liver disease, induces cirrhosis-associated immune dysfunction syndrome (CAIDS), characterized by both innate and adaptive immune dysfunction. Inflammation triggered by factors such as alcohol, viruses, toxins, and cholesterol induces metabolic reprogramming of both innate and adaptive immune cells. Our study specifically sought to investigate the compromised adaptive immune response in cirrhosis by focusing on assessing T-cell exhaustion and activation markers on helper and cytotoxic T cells. A prospective observational study involving 19 liver cirrhosis patients and 36 healthy controls was conducted. The hepatic decompensation degree was assessed using various parameters, including serum bilirubin, albumin, international normalized ratio, ascites, and hepatic encephalopathy. T cell activation (CD38, CD44, CD69, HLADR) and exhaustion markers (CTLA-4, PD-1, TIM-3, LAG-3) were assessed on helper and cytotoxic T cells by flow cytometry. Cirrhosis patients showed reduced T cells with no alteration in the CD4:CD8 T cell ratio. Among activation markers, HLADR showed increased expression on CD8+ T cells (p = 0.031). Regarding exhaustion markers, LAG-3 and TIM-3 exhibited increased expression in cirrhotic patients compared to controls in both CD4 and CD8 T cells (p = 0.004, p = 0.016, p = 0.001, p = 0.004, respectively). Neither cirrhotic nor healthy controls showed CTLA expression. PD-1 did not differ significantly between the two groups. Co-expression of PD-1/TIM-3 on CD8+ T cells was notably higher in cirrhotic patients (p < 0.002). The observation of impaired adaptive immunity with notable T-cell exhaustion and activation in cirrhosis underscores the potential relevance of immunotherapy.
Keywords
Introduction
Cirrhosis, the advanced stage of chronic liver diseases, manifests as a complex syndrome known as cirrhosis-associated immune dysfunction syndrome (CAIDS), characterized by various levels of immune dysfunction. This condition exerts a profound impact on both innate and adaptive immune functions, altering the body’s ability to combat infections and maintain homeostasis. 1 The innate immune system acts as the initial defense against pathogens, encompassing both cellular and humoral elements. This includes pattern recognition receptors (PRRs), antimicrobial peptides, and various immune cells such as phagocytes (neutrophils, monocyte/macrophages, mast cells, and macrophages), antigen-presenting cells (dendritic cells, natural killer cells, and NK–T cells). Additionally, components like the complement system and diverse cytokines contribute to its functionality. However, in cirrhosis, there’s a compromise in the synthesis and function of PRRs and other crucial proteins vital for innate immunity, leading to a reduction in the body’s ability to combat bacterial threats. The liver, a predominantly innate immune organ, is affected by cirrhosis, leading to functional abnormalities in key components of innate immunity.2,3
The liver also plays a crucial role in adaptive immunity by housing lymphocytes in its parenchyma and portal tracts. In cirrhosis, there is a disruption in the long-lasting B and T lymphocyte-mediated immune response against specific microbial agents. CD8+ T cells outnumber CD4+ T cells in the liver, and memory cells exceed their counterparts in the bloodstream. This imbalance contributes to adaptive immune dysfunction in cirrhosis. 4 Inflammation triggered by factors such as alcohol, viruses, toxins, and cholesterol induces metabolic reprogramming of both innate and adaptive immune cells. This reprogramming contributes to functional abnormalities in neutrophils, macrophages, natural killer cells, and the complement system, collectively impairing innate immune responses. 5
B and T cell defects in alcoholic liver disease are well-researched. 6 Similarly, dysfunctions in T-cells, linked to co-inhibitory signaling and persistent hyperactivation seen in hepatocellular cancer and chronic viral infections, are known.7–9 The knowledge has been utilized for anticancer therapy in the form of the reversal of T-cell exhaustion. However, the full extent of T cell dysfunction in cirrhosis has not been studied yet and necessitates further exploration. Our study specifically sought to investigate the compromised adaptive immune response in cirrhosis by focusing on assessing T-cell exhaustion and activation markers on helper and cytotoxic T cells.
Cirrhosis impairs both innate and adaptive immune responses. However, the extent and mechanism of T-cell dysfunction in cirrhosis is less understood and requires research.
The study identified significant exhaustion of T-cells characterized by expression of LAG-3 and TIM-3, which may contribute to the impaired immune responses in cirrhosis patients.
Co-expression of multiple inhibitory checkpoints (e.g., PD-1/LAG-3 and PD-1/TIM-3) on T-cells in cirrhotic patients, suggesting a more advanced state of T-cell exhaustion and highlighting potential biomarkers of immune dysfunction in cirrhosis.
The identification of specific immune checkpoint markers such as PD-1, LAG-3, and TIM-3 as contributors to T-cell exhaustion in cirrhosis suggests that targeted immunotherapy could be developed to restore T-cell function.
The study highlights the potential for using immune activation and exhaustion markers as biomarkers to assess disease severity and predict clinical outcomes in cirrhosis patients.
Material and methods
Setting and participants
A prospective observational study involving 19 patients diagnosed with liver cirrhosis attending the Out-patient Department of Hepatology, Sanjay Gandhi Post-Graduate Institute of Medical Sciences, Lucknow, India, from July 2021 to December 2021 and 36 individuals constituting a control group of healthy participants was carried out. The underlying causes of cirrhosis were identified as Hepatitis C Virus (HCV) in 10 out of 19 cases, HBV in 2 cases, alcohol-related liver disease in 3 cases, metabolic dysfunction-associated fatty liver diseases (MDFLD) in 2 cases, and other causes in the remaining 2 cases. All the HCV patients achieved a sustained virological response after treatment with the sofosbuvir plus velpatasvir combination. None of them were viremic at the time of the study. All the HBV-infected patients were on entecavir and had undetectable HBV DNA at the time of the study. None of those with alcohol-related cirrhosis were actively consuming alcohol. All of them were abstinent for 12 months or more.
Cirrhosis was diagnosed with a combination of findings of relevant history and clinical examination, biochemical investigations, radiological evaluations, endoscopic examination for esophageal or gastric varices as evidence of portal hypertension, and AST-Platelet ratio index. Hepatic decompensation was defined by the presence of any of the following: (i) serum bilirubin levels exceeding 2.5 times the upper limit of normal along with a prolonged prothrombin time (prolonged by >3 s or an international normalized ratio >1.5), (ii) the development of ascites, or (iii) the occurrence of hepatic encephalopathy. 10 The study was ratified by the Institutional Ethics Committee, and all participants provided informed written consent.
Blood sampling and immunophenotyping
Three milliliters of venous blood were collected in Ethylene diamine tetraacetic acid (EDTA) vials from all participants for flow cytometry, which was performed within 4 h after sample collection. The stain-lyse-wash protocol was followed for sample preparation. 100 µL EDTA blood was stained with fluorochrome-labeled monoclonal antibodies. These antibodies targeted markers such as anti-CD44, anti-CD69, anti-HLADR, and anti-CD38 for T cell activation, and anti-CTLA (Cytotoxic T lymphocyte-associated protein-4), anti-PD-1 (Programmed cell death protein-1), anti-LAG-3 (Lymphocyte-activation gene-3), and anti-TIM-3 (T-cell immunoglobulin and mucin-domain containing-3) for T cell exhaustion, in addition to CD3, CD4, and CD8 gating of T cells, respectively. Cells were acquired on FACS Canto II flow cytometer from Becton Dickinson Biosciences, ensuring the acquisition of at least 10,000 CD3+T cells to ensure an adequate number of T cells for analysis. T cells were distinguished based on the presence of anti-CD3 expression. Among these, helper and cytotoxic T cells were recognized by their expression of CD4 and CD8, respectively. Expressions of activation and exhaustion markers were further analyzed on helper and cytotoxic T cells. Data were analyzed by the FACS Diva software package. All antibodies were supplied by Becton Dickinson Biosciences, San Jose, CA, USA. Figure 1 illustrates the gating strategy utilized in the study (Figure 1).
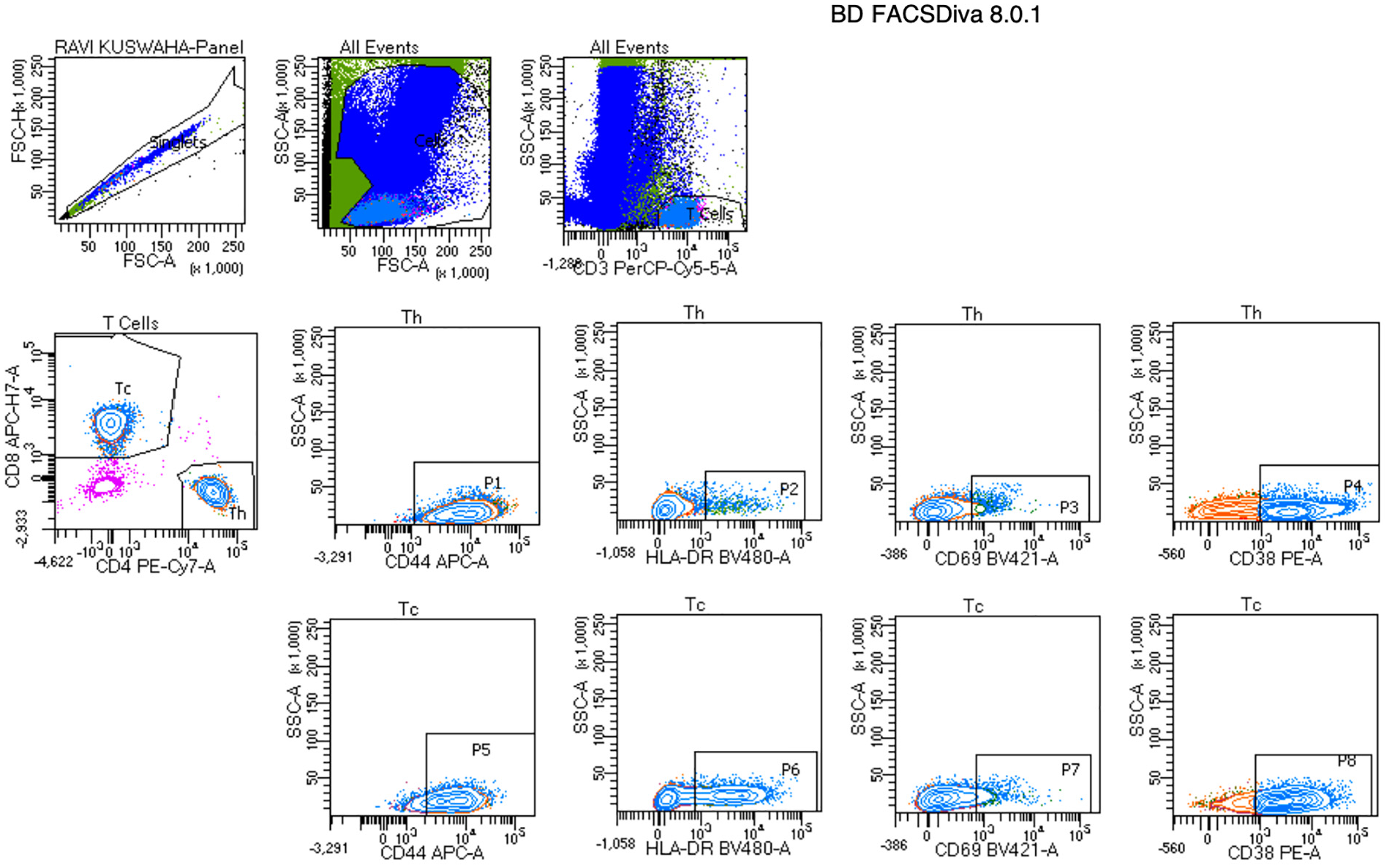
shows a flow plot of the gating pattern; single cells are selected based on FSC area vs height, followed by CD3+T cells (SSC vs CD3), of which CD4+T cells and CD8+T cells are selected. Expression of various markers is shown on both CD4+ (Th) and CD8+T (Tc) cells. FSC, Forward Scatter; SSC, Side Scatter.
Statistical analysis
All the data were analyzed with IBM SPSS Statistics for Windows, Version 24.0 (Armonk, NY, USA). Data were represented as mean ± standard deviation. An independent sample t-test was performed to compare two continuous variable data. P < 0.05 was considered as statistically significant. Intergroup comparisons among three groups were performed using one-way ANOVA, followed by post hoc analysis with the Tukey test.
Results
Demographic and clinical characteristics of the study population
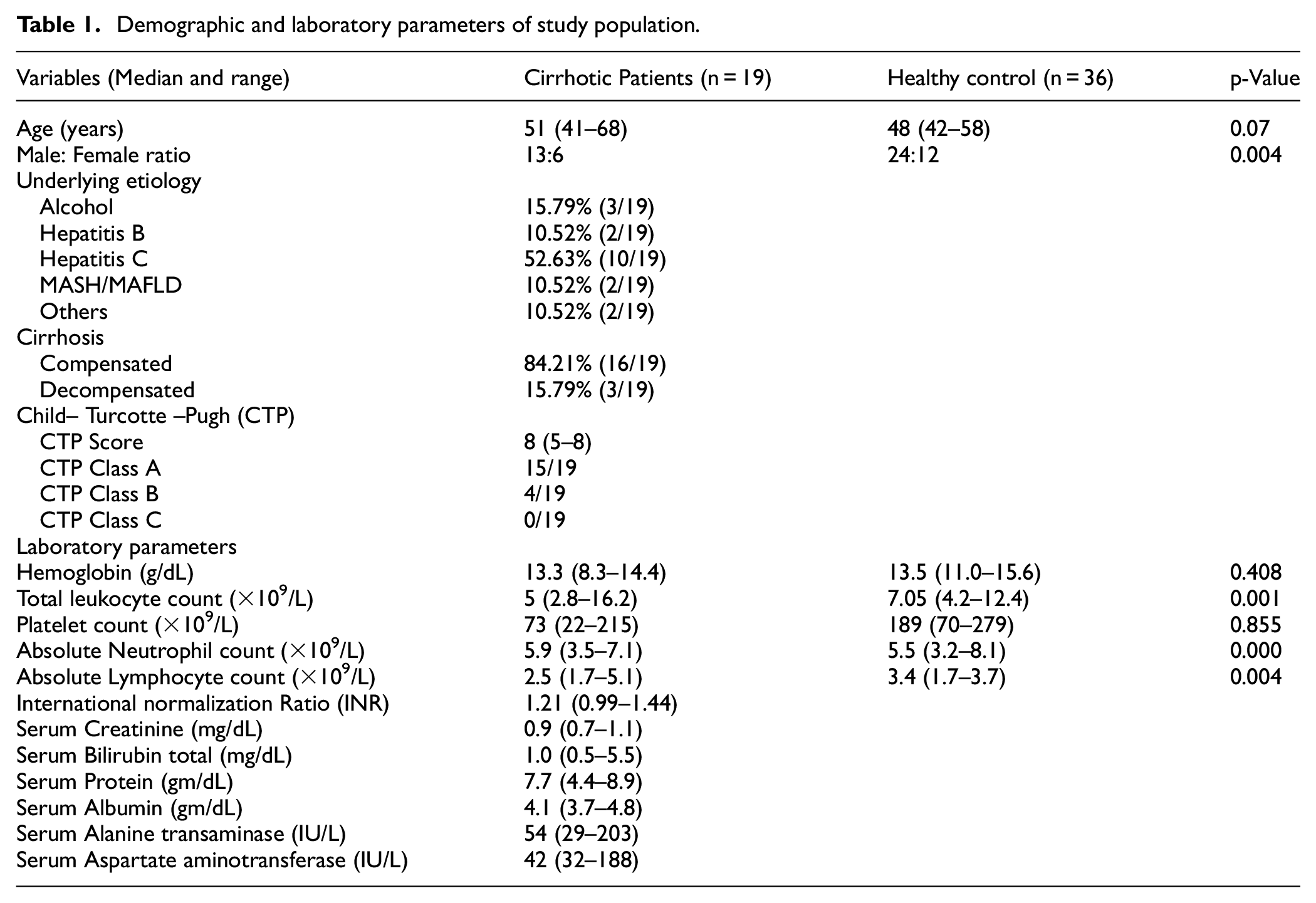
The study included 19 patients with cirrhosis, diagnosed based on clinical, laboratory, and radiological findings. The underlying causes of cirrhosis were identified as HCV in 10 out of 19 cases, HBV in 2 cases, alcohol-related liver disease in 3 cases, MDFLD in 2 cases, and other causes in the remaining 2 cases. The severity of liver cirrhosis was assessed based on a scoring system (Child Turcotte Pugh) using five clinical and laboratory criteria: serum bilirubin, serum albumin, ascites, encephalopathy, prothrombin time or international normalized ratio >1.5. 11 The majority of patients were in Child–Turcotte–Pugh (CTP) class A (15/19) with good hepatic function, followed by CTP class B (4/19) with moderate hepatic function. None of them were in CTP class C or advanced hepatic dysfunction. Table 1 displays the demographic and clinical characteristics of both patients and healthy controls (Table 1).
Demographic and laboratory parameters of study population.
Characterization of T cell in cirrhosis
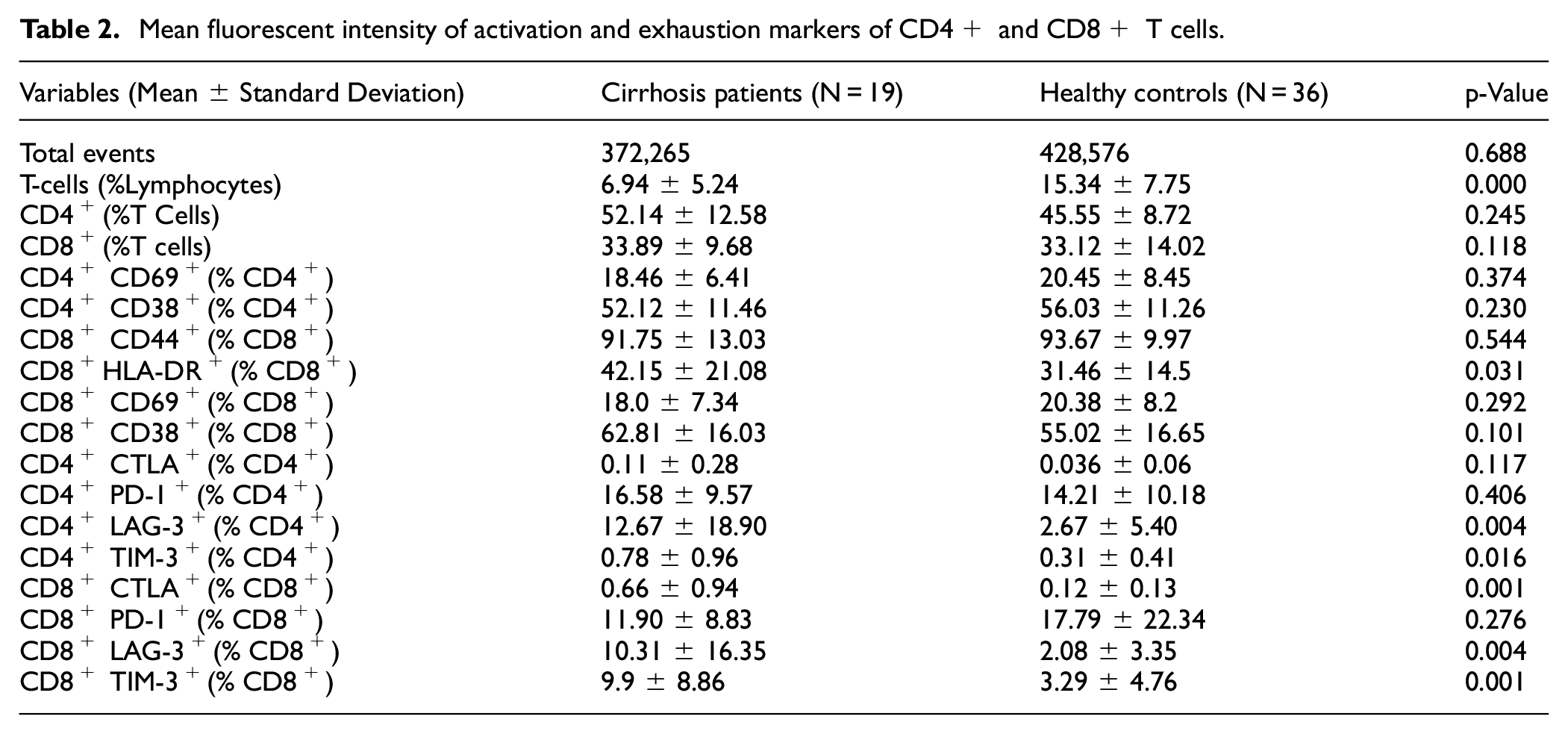
Pan T cell depletion was noted in cirrhosis patients. However, both helper and cytotoxic T cell numbers were comparable, and there was no difference in the CD4:CD8 T cell ratio. Among the activation markers (CD69, CD38, CD44, and HLADR), only HLADR showed increased expression on CD8+ T cells (p = 0.031) in cirrhotic patients. Among the exhaustion markers, LAG-3 showed increased expression in cirrhotic patients when compared with healthy controls both in CD4 (Mean MFI = 12.67 ± 18.90, 0.12 ± 0.13) and CD8 T cells (Mean MFI = 10.31 ± 16.35, 2.08 ± 3.35), respectively (p = 0.004, p = 0.004). Similarly, TIM-3 showed increased expression in cirrhotic patients when compared with healthy controls both in CD4 (Mean MFI = 0.78 ± 0.96, 0.31 ± 0.41) and CD8 T cells (Mean MFI = 9.9 ± 8.86, 3.29 ± 4.76) respectively (p = 0.016, p = 0.001; Figure 2).
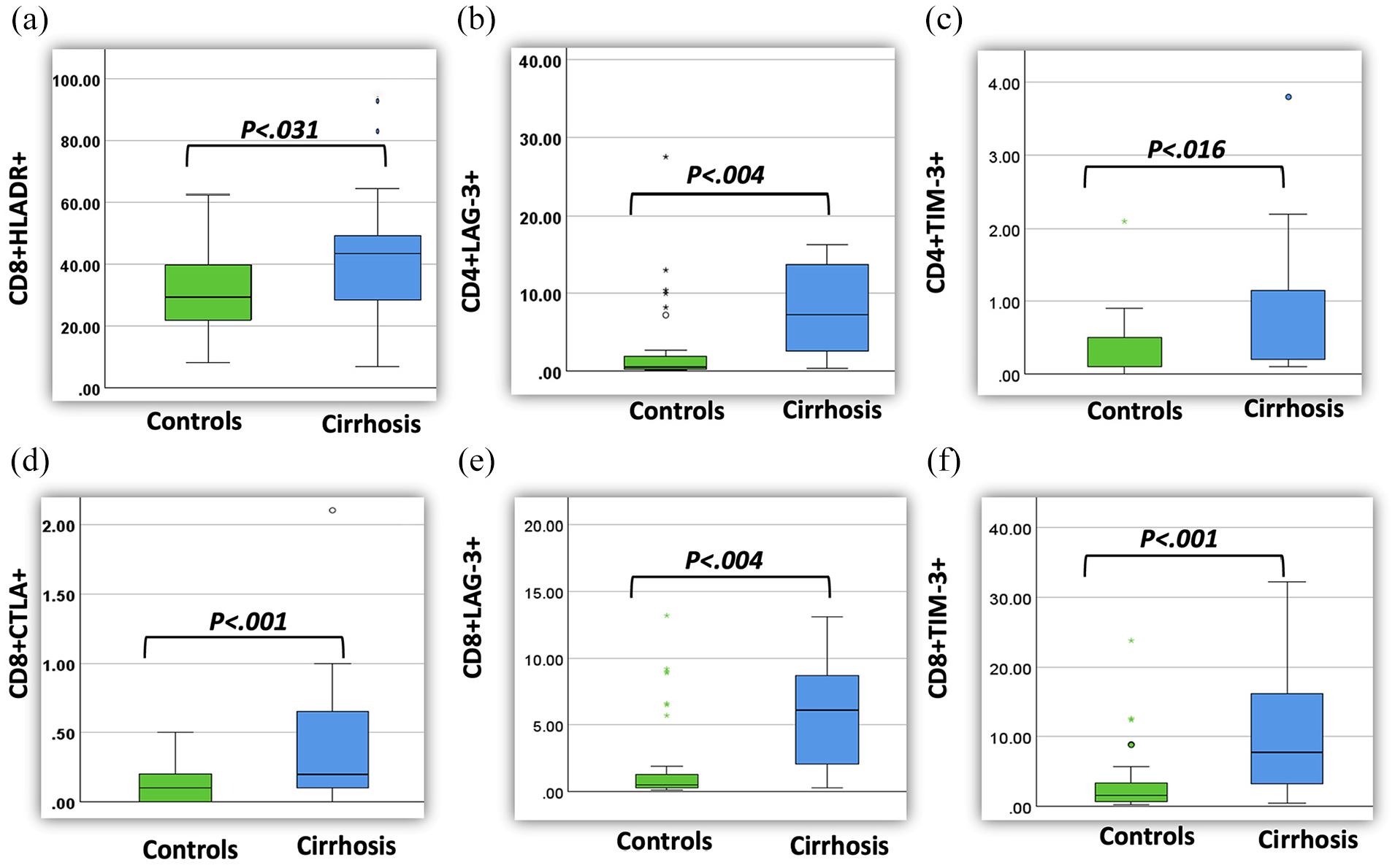
Box plot showing a significant increase in the expression of HLA-DR, CTLA, LAG-3, and TIM-3 on CD8+ T cells ((a), (d), (e), (f)) and elevated LAG-3 and TIM-3 expression on CD4+ T cells ((b), (c)) in cirrhotic patients compared to healthy controls.
CTLA expression was not seen in CD4 T cells in both cirrhotic patients (Mean MFI = 0.11 ± 0.28) and healthy controls (0.03 ± 0.06), respectively. However, CD8 T cells show dim expression of CTLA in cirrhotic patients (Mean MFI = 0.66 ± 0.94, 0.12 ± 0.13), respectively (p = 0.001). PD-1 was expressed in both cirrhotic patients and healthy controls in CD4+ T cells (mean MFI = 16.58 ± 9.57 and 14.21 ± 10.18) and CD8+T cells (11.90 ± 8.83 and 17.79 ± 22.34), respectively, and didn’t show any statistical difference in both diseased and healthy group. The expression profile of different T-cell markers is shown in Table 2.
Mean fluorescent intensity of activation and exhaustion markers of CD4+ and CD8+ T cells.
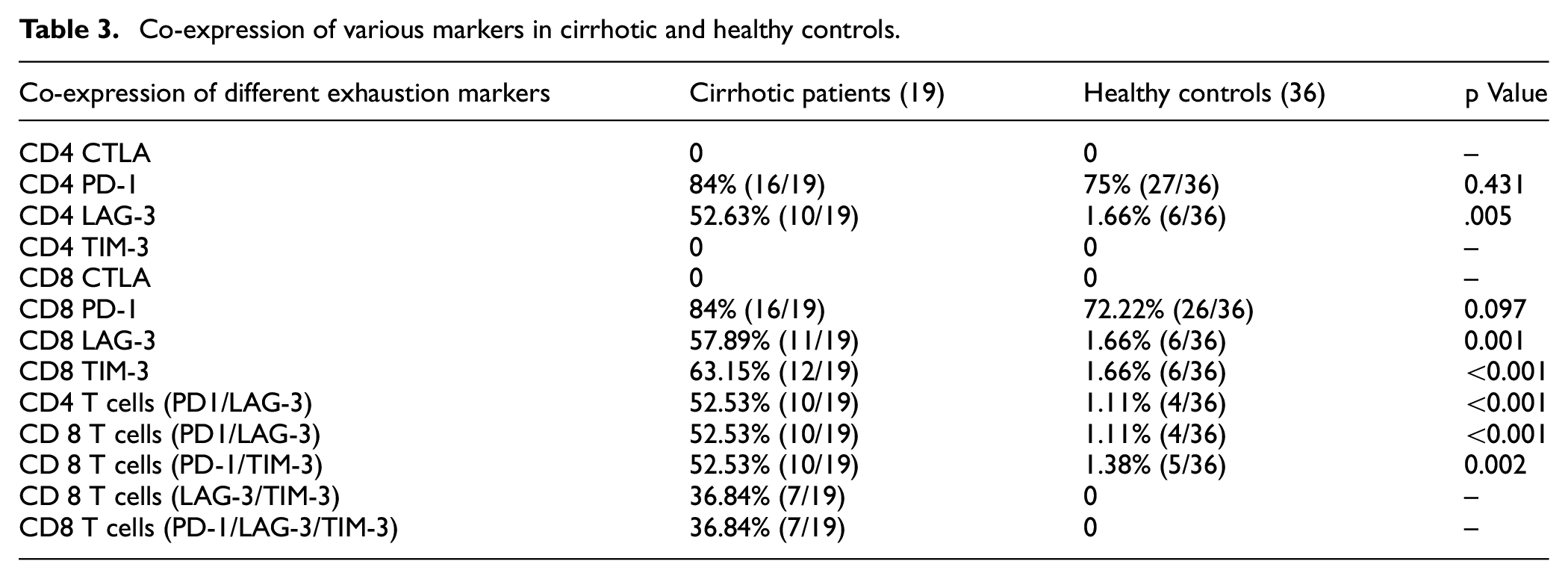
None of the cirrhotic or healthy controls shows expression of CTLA on T lymphocytes. Likewise, TIM-3 expression was absent in CD4 T cells in both groups. Both PD-1 and LAG-3 exhibited simultaneous expression on helper and cytotoxic T cells in the majority of cirrhotic patients compared to controls (p < 0.001, p < 0.001).
Additionally, co-expression of PD-1/TIM-3 on CD8+T cells was seen in a significant number of cirrhotic patients (p < 0.002). A minority of cirrhotic patients (36.84%) showed both LAG-3+/TIM-3+ expression and LAG-3/TIM-3/PD-1 on cytotoxic cells, respectively; however, none of the healthy controls showed co-expression of these markers. Table 3 represents the co-expression of various markers in cirrhotic and healthy controls (Table 3).
Co-expression of various markers in cirrhotic and healthy controls.
The data were analyzed based on underlying etiology to explore differences in T-cell biology. A statistically significant difference was observed in CD4+ T-cells, with increased expression of HLA-DR and CD38 (activation markers) and PD-1 and LAG-3 (exhaustion markers) in the hepatitis group compared to others (MAFLD and alcohol). However, no significant intergroup differences were noted in CD8+ T-cells.
Discussion
CAIDS is characterized by impairment in both innate and adaptive immune systems. While innate immune dysfunction in cirrhosis is well documented in the literature, we have limited knowledge of adaptive immune dysfunction. 12
This study comprehensively investigates the compromised adaptive immune response in cirrhosis by assessing immune activation and exhaustion in helper and cytotoxic T cells in patients of cirrhosis. The pan T cell depletion in our cirrhosis patients with normal CD4:CD8 T cells ratio suggests a specific impairment of T cell subsets rather than a generalized T cell deficiency. We observed overexpression of HLADR on CD8 T cells, reflecting ongoing immune activation and increased expression of LAG-3 and TIM-3 in both helper and cytotoxic cells, denoting exhaustion and immune tolerance, suggesting impaired T cell function and immunosuppression in cirrhosis.
Rueschenbaum et al. showcased heightened expression of activation markers (CD38, CD69, HLA-DR), exhaustion markers (CTLA4, PD-1, TIM-3, LAG-3, and TIGIT), and apoptotic marker CD95 on cytotoxic T cells in cirrhosis patients, mirroring our findings. These alterations were evident early in the course of the disease among compensated, decompensated, acutely decompensated, and acute chronic liver failure in their study. 13
Recent observations have indicated increased levels of immune checkpoint markers (PD-1, CTLA-4, TIM-3) on CD8 T cells, implying T cell exhaustion causes dysfunction in cirrhotic patients. They have also suggested the role of CTLA-4, PD-1, and TIM-3 blockade in reversing the T cell exhaustion.14,15 They also indicated an altered phenotype of cytotoxic T cells, with increased expression of the activation marker (HLADR) in cirrhotic patients. While no significant correlation was found between HLA-DR expression on CD8+ T cells and MELD score, elevated levels of circulating HLA-DR on CD8+ T cells were observed in acute decompensation patients with concurrent infection. This indicates a potential role of this cell population in susceptibility to and/or compromised immune responses during episodes of infection and suggests that monitoring of such abnormal phenotype of CD8 T cells can serve as an immunomodulatory marker in cirrhosis patients. The co-expression of HLA-DR and PD1 serves as a predictive factor for poor outcomes, emphasizing the significance of utilizing a panel of biomarkers rather than relying solely on the expression of a single molecule to identify patients at high risk. 14
The actual mechanism of T cell activation is not known, though it has been suggested in various studies that it may be part of systemic immune activation in response to underlying inflammation.16,17 T-cell activation in cirrhosis manifests a dual effect. Initially, it compromises the immune response against viral pathogens, fostering persistent infections and disease advancement. Subsequently, excessive activation results in the release of cytokines, exacerbating liver inflammation, damage, and progression of fibrosis. Patients with cirrhosis are susceptible to bacterial infection because of compromised immune response. The low-grade inflammatory reaction in response to a bacterial challenge or extensive hepatocyte damage arises from heightened intestinal barrier permeability, characterized by loosening tight junctions, increased bacterial transcytosis, and a decrease in mediators that restrict bacterial contact with intestinal microvilli. Incomplete resolution of inflammation leads to disruption of both innate and adaptive immune functions, significantly impacting the body’s ability to combat infections and maintain homeostasis in the advanced stage of chronic liver diseases. 18
In chronic infections and malignancies, continual exposure to antigens in suboptimal conditions can trigger the onset of T-cell exhaustion marked by upregulation of exhaustion deciphering immune checkpoint.7,8 The exhausted T cells overexpress inhibitory receptors or checkpoints, such as PD-1, CTLA4, TIM3, and LAG3, on the surface. 19 The common characteristics of T-cell exhaustion result in dysfunction of antigen-specific T-cell recognition, progressively declining effector activity, incompetent proliferative capacity, altered expression of transcription factors, compromised antigen-independent homeostatic proliferation, extensive epigenetic status, and altered metabolic requirements. 20
Fewer studies have described intrahepatic expression of activated CD8 T cells in cirrhosis and autoimmune hepatitis and have correlated it with the necro-inflammatory score in patients.21,22 The precise mechanisms driving immune cell paralysis remain incompletely understood, although several factors contribute to its development: excessive inhibitory immunoregulatory responses triggered to counteract severe systemic inflammation, exhaustion of effector immune cells due to persistent chronic stimulation of enteric origin, and dysfunction of immune effectors associated with metabolic and neuroendocrine abnormalities linked to hepatic insufficiency. 18
Our study also examined the co-expression of various inhibitory checkpoints in cirrhotic patients. Co-expression of PD-1/LAG-3 and PD-1/TIM-3 was significantly elevated in cirrhotic patients, particularly on CD8 T cells, suggesting a condition of T cell exhaustion characterized by multiple inhibitory pathways. A minority of patients showed co-expression of LAG-3/TIM-3 or PD-1/LAG-3/TIM-3 on CD8 T cells, indicating extreme T cell exhaustion. While PD-1 levels were elevated in most of our patients, its expression was also observed in the control group, with no significant difference compared to healthy controls. This implies that anti-PD-1 therapy might offer benefits on a case-by-case basis, especially in instances of PD-1 overexpression. Therapeutic targeting of PD-1 or its ligand PD-L1 shows promise in restoring T cell function and controlling liver inflammation in preclinical and clinical studies. However, further research is needed to elucidate the complex interplay between PD-1 signaling and liver disease pathogenesis for the development of effective therapies. There are conflicting reports about its use in chronic liver diseases, as the downregulation of T cells may favor carcinogenesis due to reduced immune surveillance.23,24
Our study has a few limitations, such as a smaller sample size restricting the generalizability of our findings. Therefore, further investigations involving larger cohorts are necessary to validate our results and elucidate the mechanisms of underlying T-cell dysfunction in cirrhosis. Additionally, longitudinal studies are warranted to investigate the dynamic changes in T cell activation and exhaustion markers throughout cirrhosis progression and in response to therapeutic interventions.
To conclude, our study provides valuable insights into the compromised adaptive immune response in cirrhosis. The observed T cell dysfunction and exhaustion in cirrhosis underscore the importance of immune monitoring and therapeutic interventions targeting immune checkpoint pathways to restore T cell function and improve patient outcomes. The specific alterations in T cell subsets and exhaustion markers provide potential biomarkers for assessing disease severity and predicting treatment responses in cirrhotic patients. Lastly, the identification of novel therapeutic targets aimed at reversing T-cell dysfunction may offer promising avenues for the management of cirrhosis and its associated complications. Further research is warranted to validate our findings and explore potential therapeutic interventions aimed at restoring T-cell function in cirrhosis.
Footnotes
Acknowledgements
We would like to thank the laboratory technician, Mr. Hirendra Kumar, who was instrumental in processing the samples.
Author contributions
Study design: HD, GY, AG. Data collection: HK, MK Data analysis: MK, HSM, GY. Data interpretation: HD, AG, HSM. Preparation of manuscript: GY, HD. Literature search/analysis: GY, HD. All authors have read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Institutional Ethics Committee of Sanjay Gandhi Postgraduate Institute of Medical Sciences. (Ref Code: PGI/BE/1304) dated 1 June 2021.
Consent for publication
Written informed consent to publish was obtained from study participants.
Availability of data and materials
The datasets used and/or analyzed in the current study are available from the corresponding author upon reasonable request.