
Abstract
Liver biopsy remains the diagnostic gold standard for assessing liver fibrosis severity; however, its cost and invasiveness highlight the need for accurate, noninvasive alternatives. This study evaluates the performance of FibroPredict, a novel algorithm, for detecting advanced liver fibrosis in high-risk populations. It compares its accuracy to transient elastography (TE), the current noninvasive reference standard. A retrospective cohort study of 316 high-risk individuals used electronic health record (EHR) data and routine laboratory results to calculate FibroPredict, APRI (Aspartate Aminotransferase-to-Platelet Ratio Index), and FIB-4 scores, which were then compared to liver stiffness measurements (LSM) obtained through TE. FibroPredict demonstrated a sensitivity of 96.8% and a negative predictive value (NPV) of 90.9% at a cutoff score of ≥135 for detecting advanced fibrosis (LSM ≥ 8 kPa), outperforming FIB-4 in sensitivity and the ability to rule out advanced fibrosis. APRI, at a cutoff of 1.5, showed high specificity (98.41%) but low sensitivity (6.32%), making it more suitable for confirming rather than excluding advanced fibrosis. However, FibroPredict’s specificity was low (21.0%), resulting in higher false-positive rates. FIB-4, with a cutoff of ≥2.67, showed lower sensitivity but better specificity (46.8%). FibroPredict’s excellent sensitivity and high NPV make it a promising tool for ruling out advanced fibrosis, particularly in resource-limited settings. However, its low specificity underscores the need for confirmatory tests, such as TE, or combining it with APRI to enhance diagnostic accuracy.
Introduction
Liver cirrhosis is a chronic, progressive condition characterized by irreversible scarring of liver tissue, commonly resulting from prolonged damage due to diseases such as chronic hepatitis, alcohol-related liver disease, or metabolic-associated steatotic liver disease (MASLD). 1 Globally, cirrhosis ranks as the 11th most common cause of death, associated with significant morbidity and long-term health complications.2,3 Unfortunately, many patients are not diagnosed in the early stages, with about 75% presenting with decompensated cirrhosis at diagnosis, a severe stage marked by significantly increased morbidity and mortality risks. The annual rate of decompensation among patients with compensated cirrhosis can reach as high as 11%.4,5
Traditionally, liver biopsy has been the gold standard for assessing the degree of fibrosis, providing direct tissue evaluation. 6 However, its invasive nature and potential complications have led to the rise of noninvasive methods such as Magnetic Resonance Elastography (MRE) and transient elastography (TE). While MRE offers superior accuracy, its high cost and limited availability constrain its use. Conversely, transient elastography, implemented through devices like FibroScan, has emerged as the noninvasive gold standard for assessing liver fibrosis due to its accessibility and ease of use. 7
FibroScan measures liver stiffness and fat content via transient elastography, wherein mechanical vibrations generate shear waves, and their velocity, expressed in kilopascals (kPa), is used to calculate liver stiffness measurement (LSM).8,9 Higher LSM values correlate with more advanced fibrosis, with values <8.0 kPa demonstrating excellent negative predictive value (NPV) for ruling out advanced fibrosis.10,11 Conversely, LSM values ≥8 kPa indicate a heightened risk of advanced fibrosis. The Controlled Attenuation Parameter (CAP), derived simultaneously, quantifies liver fat content by measuring ultrasound wave attenuation, providing an additional noninvasive measure of hepatic steatosis. 12 LSM and CAP have revolutionized the noninvasive evaluation of liver fibrosis and steatosis, offering clinicians rapid and reliable tools for patient management. 13
In recent years, the development of algorithmic screening methods has opened new avenues for early detection of liver cirrhosis. These methods utilize advanced computational models, often integrating machine learning, to analyze clinical and biochemical parameters from EHR and routine lab results.
FibroPredict is an innovative algorithmic screening method to identify individuals at risk of advanced liver fibrosis. Prior research indicates that a FibroPredict score ≥135 highly suggests advanced fibrosis, warranting further diagnostic evaluation. 14
This study aims to critically evaluate the diagnostic performance of FibroPredict, with particular emphasis on its correlation with TE, a widely recognized noninvasive gold standard for fibrosis assessment. Furthermore, a comparative analysis is conducted with FIB-4, an extensively validated fibrosis scoring system, 15 to elucidate FibroPredict’s relative diagnostic efficacy. Through this comprehensive evaluation, the study aims to advance the clinical integration of noninvasive screening methodologies, thereby enhancing the early detection and management of liver fibrosis in high-risk populations.
Advanced liver fibrosis is a significant cause of morbidity and mortality, often detected late in high-risk populations. Liver biopsy is the gold standard for diagnosis, but is invasive and costly. Noninvasive tools such as transient elastography (TE) and scoring systems such as FIB-4 are commonly used, though they each have limitations, particularly in balancing sensitivity and specificity.
The FibroPredict algorithm demonstrated superior sensitivity (96.8%) and high negative predictive value (90.9%) compared to FIB-4 for detecting advanced liver fibrosis in high-risk populations. While FibroPredict excels in ruling out advanced fibrosis, its low specificity (21%) highlights the need for confirmatory diagnostics such as TE or complementary use with APRI. These findings support FibroPredict’s role in enhancing the early detection of advanced fibrosis and improving resource utilization, offering a valuable addition to existing noninvasive screening tools and potentially refining the current stepwise diagnostic framework while aligning with recent AASLD recommendations.
FibroPredict offers a cost-effective and accessible screening method leveraging routine lab tests, making it particularly useful in resource-limited settings. Its integration into clinical workflows could reduce reliance on invasive diagnostics while ensuring early detection of advanced fibrosis. By complementing tools such as FIB-4 and APRI, FibroPredict strengthens targeted screening strategies for high-risk populations. Further research should explore enhancing its specificity through biomarker integration and validating its utility in broader, diverse populations.
Methods
Study design
This retrospective cohort study utilized EHR data from Clalit Health Services (CHS) to evaluate the effectiveness of algorithmic screening for liver fibrosis and cirrhosis in a high-risk population. Specifically, it examines the correlation between algorithm-generated predictions, such as FibroPredict scores, and liver stiffness measurements obtained through TE. By assessing this correlation, the study aims to validate the diagnostic accuracy of computational tools when integrated with noninvasive imaging techniques, paving the way for earlier and more precise detection of advanced liver disease.
Ethical considerations
This study received ethical approval from the Clalit EMC Helsinki Committee (Approval No. 0092-23-EMC). Due to its retrospective design, the requirement for patient consent was waived. Strict confidentiality measures were implemented, ensuring the removal of all personal identifiers from the data to ensure participant privacy.
Study population
The study included 316 high-risk individuals aged 18 and older with chronic liver diseases who were evaluated at a hospital-affiliated liver clinic. High-risk status in this context refers to patients with chronic liver disease who were referred specifically for specialized evaluation by hepatologists, reflecting a more advanced or complex disease profile compared to individuals with chronic liver disease managed in general practice or non-hospital-affiliated clinics. Participants were stratified into two cohorts based on their TE (FibroScan) results: individuals with moderate-to-advanced fibrosis and individuals with no or mild fibrosis.
Data collection
Transient elastography: We analyzed data from 316 FibroScan (Echosens) tests conducted between 2020 and 2024. The patients were stratified into two groups based on their LSM values, expressed in kilopascals (kPa). The first group consisted of 190 patients with moderate-to-severe fibrosis, characterized by LSM values greater than 8 kPa, indicative of significant liver scarring. The second group included 126 patients with no or mild fibrosis, with LSM values less than 8 kPa, suggesting minimal liver damage.
FibroPredict development
Data collection and feature selection
The original study incorporated data from 2,255,580 observations spanning 16 years (2004–2020). FibroPredict was trained on key laboratory parameters, including hemoglobin, platelet count, white blood cell count, liver function tests (AST, ALT, bilirubin, and albumin), glucose metabolism markers (HbA1c and fasting glucose), and lipid profile components (cholesterol, HDL, LDL, and triglycerides). Age and sex were also included as predictive variables. The model employed a gradient-boosting survival analysis framework to predict cirrhosis onset within a five-year follow-up window.
Model development and validation
A rolling-origin-update approach was used to partition the dataset into training and validation subsets, ensuring temporal independence. The model’s performance was assessed using time-dependent receiver operating characteristic (ROC) curves and area under the curve (AUC) metrics. The prospective validation phase involved external clinical testing, comparing FibroPredict’s predictions against TE-confirmed fibrosis severity. As validated in a prior study, a predefined threshold of ≥135 was used to identify patients with a high probability of advanced fibrosis.
Ethical considerations
The Clalit Helsinki Committee (0195-17-COM2) and the Emek Medical Center Helsinki Committee (0208-20-EMC) approved the study protocol. The study’s ClinicalTrials.gov registration number is NCT05218538. All procedures adhered to ethical guidelines for human research, with de-identified data used for retrospective analyses and informed consent obtained for prospective evaluations.
FIB-4 calculation and cutoffs
FIB-4 is calculated based on a patient’s age, aspartate aminotransferase (AST), alanine aminotransferase (ALT), and platelet count. We calculated the FIB-4 score for all participants using these parameters to compare its performance with FibroPredict and TE (FibroScan). The FIB-4 cutoff values were interpreted as follows: below 1.3 indicates normal or mild fibrosis, between 1.3 and 2.67 suggests intermediate fibrosis, and 2.67 or above indicates the potential for advanced liver fibrosis. Since our study population is at high risk for liver fibrosis, we chose to adopt a FIB-4 cutoff of 2.67 or above to identify individuals with a higher likelihood of advanced liver fibrosis. This decision ensures that we capture cases requiring further evaluation with greater specificity, aligning with the needs of our at-risk population.
APRI score calculation
The APRI score was calculated using the following formula: [(AST/ULN) × 100] / Platelet count (109/L), where ULN represents the upper limit of normal AST. APRI values ≥1.5 were considered indicative of advanced fibrosis.
Comparative analysis
We conducted a comparative analysis to evaluate the diagnostic performance of Fibro Predict and FIB-4 in identifying advanced liver fibrosis, using FibroScan as the reference standard. FibroScan LSM of ≥8 kPa indicated advanced fibrosis. First, Fibro Predict scores were compared to FibroScan results, with a threshold of ≥ 135 for advanced fibrosis. Similarly, FIB-4 scores were compared to FibroScan results, applying a cutoff of ≥2.67, consistent with the high-risk status of our population. Given its established role in fibrosis evaluation, APRI was analyzed at a threshold of ≥1.5. Finally, we directly compared the performance of FibroPredict and FIB-4 to assess their relative accuracy and clinical utility in detecting advanced fibrosis. The analysis aimed to determine the sensitivity, specificity, positive predictive value, negative predictive value, and overall effectiveness of each method in this high-risk cohort.
Results
The study included 316 patients with an average age of 61.8 years (range: 16–90) and 166 males (52.5%). Laboratory values, including mean levels of WBC (7.07, range: 1.26–108.30), hemoglobin (13.36, range: 7.10–18.10), platelets (200.22, range: 30.00–758.00), albumin (4.02, range: 2.23–5.12), and AST (42.75, range: 7.00–260.00), are presented with their respective ranges (Table 1).
Baseline Demographic and Clinical Characteristics of the Study Population.
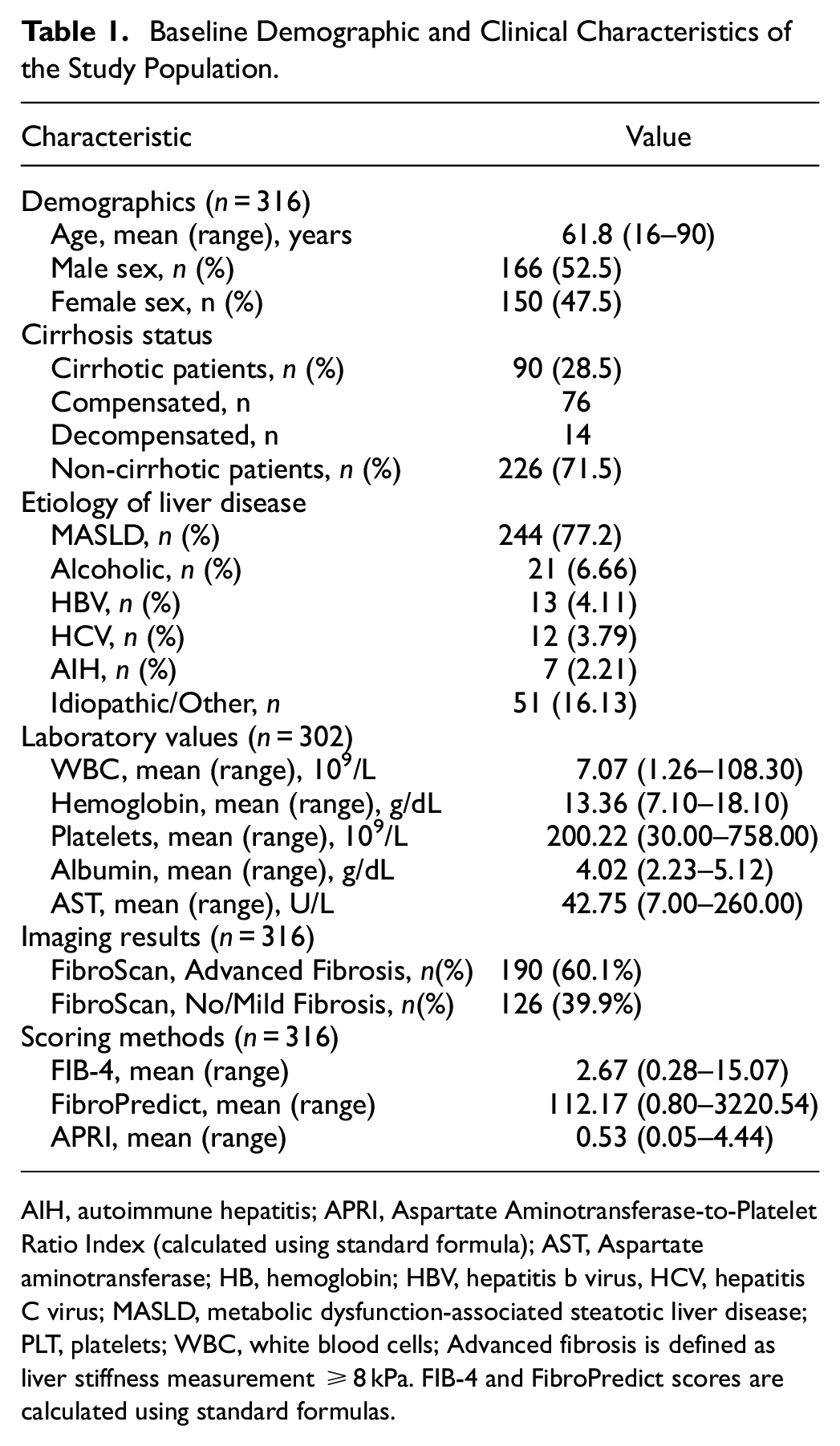
AIH, autoimmune hepatitis; APRI, Aspartate Aminotransferase-to-Platelet Ratio Index (calculated using standard formula); AST, Aspartate aminotransferase; HB, hemoglobin; HBV, hepatitis b virus, HCV, hepatitis C virus; MASLD, metabolic dysfunction-associated steatotic liver disease; PLT, platelets; WBC, white blood cells; Advanced fibrosis is defined as liver stiffness measurement ≥8 kPa. FIB-4 and FibroPredict scores are calculated using standard formulas.
Regarding cirrhosis status, 90 (28.5%) patients were cirrhotic, 14 (15.5%) of them were decompensated, and 226 (71.5%) were non-cirrhotic. The etiology of liver disease was primarily MASLD, affecting 244 patients (77.2%). Other etiologies included alcohol-related liver disease (21 patients, 6.66%), hepatitis B virus (HBV) infection (13 patients, 4.11%), hepatitis C virus (HCV) infection (12 patients, 3.79%), autoimmune hepatitis (AIH; 7 patients, 2.21%), and idiopathic or other causes (51 patients, 16.13%). Thirty-eight (12.0%) patients had more than one underlying etiology, with MASLD frequently coexisting with either alcohol-related liver disease or viral hepatitis.
Imaging results from FibroScan indicate that 60.1% of the participants had advanced fibrosis (LSM ≥8 kPa), while 39.9% had no or mild fibrosis (LSM <8 kPa).
The diagnostic performance of FibroPredict and FIB-4 for identifying advanced fibrosis was assessed and compared using sensitivity, specificity, PPV, and NPV as primary metrics (Table 2). FibroPredict, at a threshold of ≥135, demonstrated excellent sensitivity (96.8%) and a high NPV (90.9%), indicating its effectiveness in minimizing missed cases of advanced fibrosis. However, its specificity was limited to 21.0%, resulting in a significant proportion of false-positive cases, underscoring the need for confirmatory testing in patients flagged as high-risk by FibroPredict.
Performance metrics for FibroPredict, FIB-4, and APRI in all scenarios.
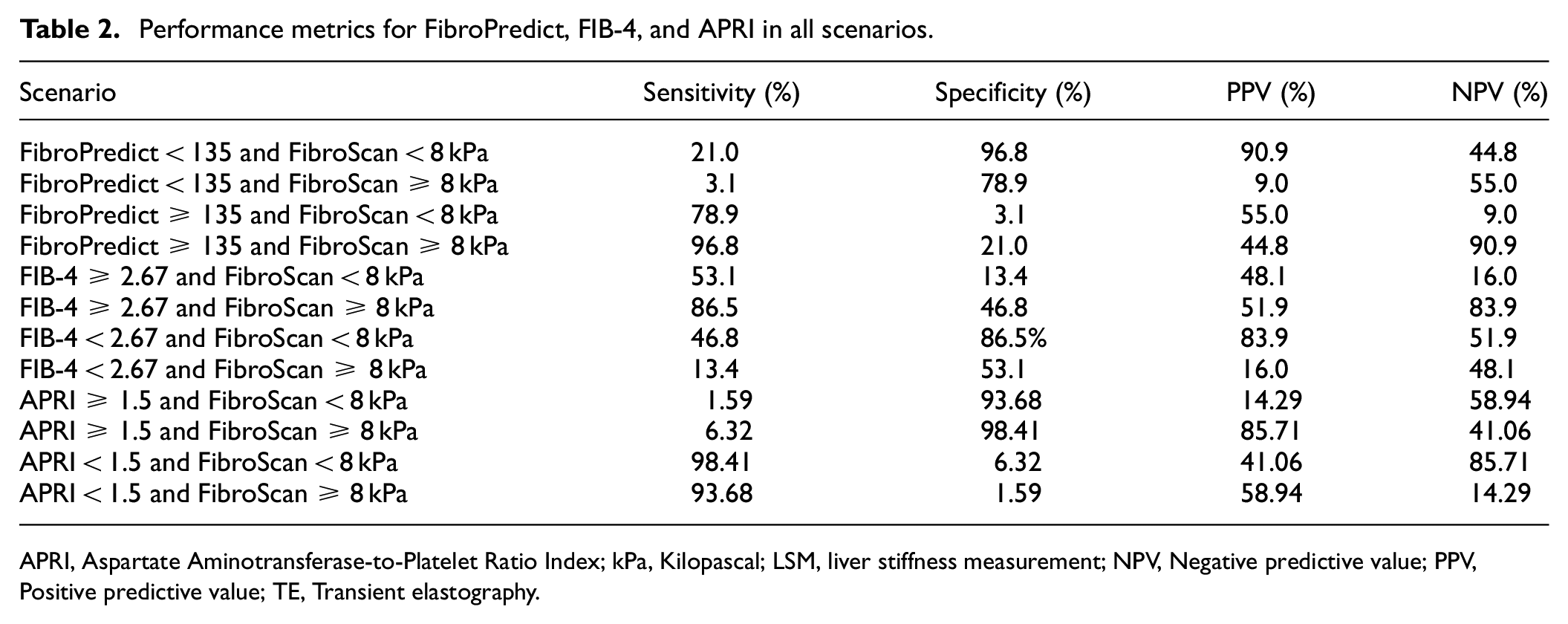
APRI, Aspartate Aminotransferase-to-Platelet Ratio Index; kPa, Kilopascal; LSM, liver stiffness measurement; NPV, Negative predictive value; PPV, Positive predictive value; TE, Transient elastography.
Conversely, FIB-4, at a threshold of ≥2.67, exhibited a more balanced diagnostic profile, achieving a sensitivity of 86.5% and a specificity of 46.8%. The PPV and NPV for FIB-4 were 51.9% and 83.9%, respectively. These findings suggest that while FIB-4 is less sensitive than FibroPredict, its higher specificity makes it a valuable secondary tool for refining diagnoses, particularly in cases flagged as high-risk by FibroPredict.
Regarding the overall diagnostic utility, Fibro Predict demonstrated a stronger ability to exclude advanced fibrosis due to its superior sensitivity and NPV. In contrast, FIB-4’s higher specificity supports its use as a confirmatory tool to reduce false positives identified by FibroPredict.
The diagnostic performance of FibroPredict and FIB-4 for identifying advanced fibrosis was assessed and compared using sensitivity, specificity, PPV, and NPV as primary metrics (Table 2). FibroPredict, at a threshold of ≥135, demonstrated excellent sensitivity (96.8%) and a high NPV (90.9%), indicating its effectiveness in minimizing missed cases of advanced fibrosis. However, its specificity was limited to 21.0%, resulting in a significant proportion of false-positive cases, underscoring the need for confirmatory testing in patients flagged as high-risk by FibroPredict.
Conversely, FIB-4, at a threshold of ≥2.67, exhibited a more balanced diagnostic profile, achieving a sensitivity of 86.5% and a specificity of 46.8%. The PPV and NPV for FIB-4 were 51.9% and 83.9%, respectively. These findings suggest that while FIB-4 is less sensitive than FibroPredict, its higher specificity makes it a valuable secondary tool for refining diagnoses, particularly in cases flagged as high-risk by FibroPredict.
Regarding the overall diagnostic utility, FibroPredict demonstrated a stronger ability to exclude advanced fibrosis due to its superior sensitivity and NPV. In contrast, FIB-4’s higher specificity supports its use as a confirmatory tool to reduce false positives identified by FibroPredict.
The ROC curves illustrate the diagnostic performance of FibroPredict and FIB-4 in detecting advanced liver fibrosis, with FibroScan as the reference standard (Figure 1). FibroPredict, with an AUC of 0.78, demonstrated moderate diagnostic accuracy and high sensitivity, making it particularly useful as a screening tool for identifying advanced fibrosis cases. Its emphasis on sensitivity ensures minimal missed cases, which is especially critical in high-risk populations. FIB-4, with an AUC of 0.75, also exhibited moderate diagnostic accuracy but a slightly lower AUC than FibroPredict. Its balanced sensitivity and specificity make it a valuable complementary tool, particularly when minimizing false positives is essential.
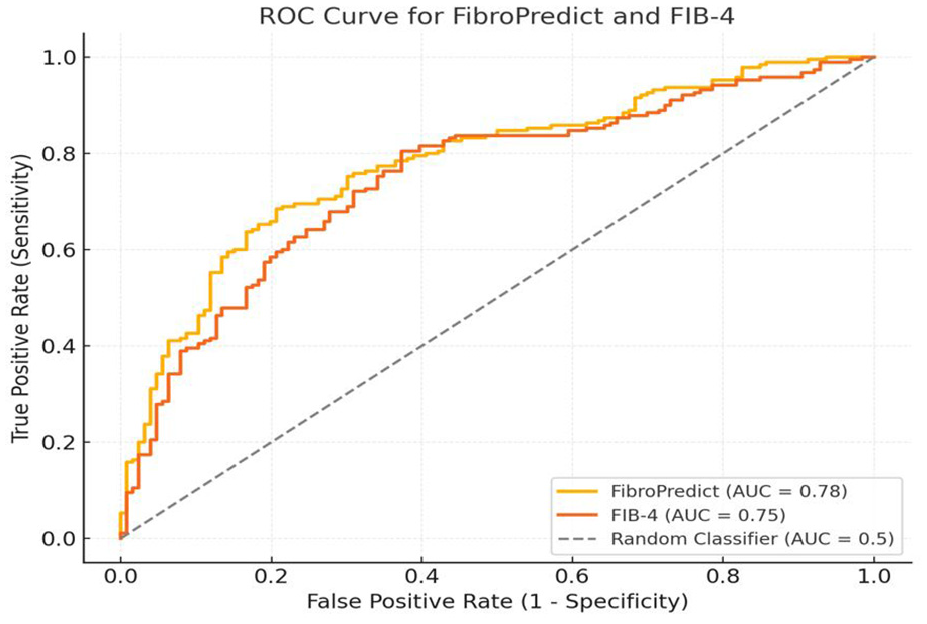
Receiver operating characteristic curve analysis comparing FibroPredict and FIB-4 for advanced liver fibrosis detection.
Discussion
The global rise in cirrhosis prevalence, along with its associated morbidity, mortality, and healthcare costs, has underscored the need for effective screening strategies to enable early detection and intervention. While identifying advanced fibrosis or compensated cirrhosis may improve outcomes, the impact of routine screening on clinically significant endpoints remains uncertain.
Recent models, such as the Chronic Liver Disease (CLivD) risk score and LiverRisk score, have been developed to predict liver fibrosis and future liver-related outcomes using demographic and routine clinical variables.16,17 Despite these advancements, FIB-4 and APRI remain the most widely used noninvasive screening tools, though recent studies have questioned FIB-4’s sensitivity and risk of overdiagnosis in specific populations.18,19
This study evaluated FibroPredict’s diagnostic performance in detecting advanced liver fibrosis. It used TE as the reference standard and compared its accuracy to the widely used noninvasive scoring systems FIB-4 and APRI. These comparisons align with recent AASLD recommendations on noninvasive liver disease assessment (NILDA), which advocate for integrating multiple noninvasive tools to enhance diagnostic accuracy. 20
FibroPredict demonstrated excellent sensitivity (96.8%) at a cutoff of ≥135 for detecting advanced fibrosis (FibroScan ≥ 8 kPa), highlighting its potential as a screening tool. This high sensitivity is crucial for identifying most cases of advanced fibrosis in high-risk populations, where early detection is paramount for timely intervention. In addition, FibroPredict exhibited an NPV of 90.9%, indicating its reliability in ruling out advanced fibrosis among individuals with scores below the threshold. However, the specificity at this cutoff was low (21%), resulting in a high rate of false positives and the potential for unnecessary referrals for confirmatory diagnostics.
Conversely, APRI at a cutoff of 1.5 showed low sensitivity (6.32%) but very high specificity (98.41%), making it a more reliable confirmatory test rather than a screening tool. The combination of high sensitivity from FibroPredict and high specificity from APRI suggests that a dual-step approach may optimize diagnostic accuracy.
Compared to FIB-4, FibroPredict showed superior sensitivity (96.8% vs 86.5%) for detecting advanced fibrosis, though at the cost of lower specificity. While FIB-4 demonstrated better specificity (46.8%) at scores ≥ 2.67, this advantage came with reduced sensitivity, potentially leading to missed diagnoses. Furthermore, FibroPredict’s higher NPV (90.9% vs. 83.9%) underscores its value in ruling out advanced fibrosis with greater confidence. Both tools exhibited high specificity for excluding advanced fibrosis when scores were below their respective thresholds (FibroPredict < 135 and FIB-4 < 2.67), though FibroPredict had a slight edge in this context.
The combination of high sensitivity and NPV makes FibroPredict particularly valuable for screening in high-risk populations, such as individuals with metabolic syndrome, chronic hepatitis, or other conditions associated with an increased risk of liver fibrosis. This is important as AASLD now recommends targeted screening for populations at increased risk, including individuals with type 2 diabetes mellitus, obesity with metabolic complications, significant alcohol use, and a family history of cirrhosis, highlighting the importance of prioritizing high-risk groups for fibrosis screening.20,21 Another significant advantage of FibroPredict is its cost-effectiveness, as it utilizes routine liver blood test results for screening.
This study has several limitations that should be considered. First, it was conducted in a hospital liver clinic setting with a predominantly high-risk population, which may limit the generalizability of the findings to low-risk populations. Second, the study was single-centered with a moderate sample size, restricting broader applicability. Multicenter studies involving diverse ethnic and demographic groups are needed to validate the performance of FibroPredict in broader populations.
In conclusion, Fibro Predict is a highly sensitive, noninvasive screening tool for advanced liver fibrosis, particularly effective in high-risk populations. Its reliance on routine laboratory tests enhances accessibility and cost-effectiveness. Integrating APRI into the FibroPredict framework enhances diagnostic accuracy, and a stepwise approach integrating FibroPredict, FIB-4, and APRI could optimize noninvasive screening strategies, reducing unnecessary referrals while maintaining diagnostic accuracy.
Footnotes
Acknowledgements
None.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee (Approval No. 0092-23-EMC) in February 2024 with the need for written informed consent waived.
Data availability
The datasets generated and/or analyzed during the current study are not publicly available because of Clalit health service policy but are available from the corresponding author on reasonable request.