
Abstract
Carotid atherosclerosis and carotid plaque are key contributors to ischemic stroke pathology and cardiovascular disease. Composite lipid indices, including the Atherogenic Index of Plasma (AIP), Visceral Adiposity Index (VAI), and Lipid Accumulation Product (LAP), are biomarkers reflecting dyslipidemia, visceral adiposity, and metabolic dysfunction. However, evidence linking these indices to carotid atherosclerosis-related outcomes remains contradictory. This study aimed to evaluate the associations of AIP, VAI, and LAP with carotid atherosclerosis and carotid plaque. PubMed, Embase, Web of Science, and the Cochrane Library were searched from database inception to May 2025. Observational studies reporting associations between composite lipid indices and carotid atherosclerosis or carotid plaque were included. Adjusted odds ratios (ORs) and 95% confidence intervals (CIs) were extracted, and random-effects models were employed. For each lipid index, quantitative synthesis was conducted independently; AIP and VAI were examined as separate meta-analytic groups, while LAP was summarized descriptively because only one eligible study was available. Seven observational studies involving 97,573 participants were included (44,890 men and 52,683 women). AIP findings were reported in four studies, VAI in three, and LAP in one. The pooled analysis indicated a significant association between AIP and carotid plaque incidence (OR = 1.30, 95% CI: 1.18–1.44). VAI was also significantly associated with carotid atherosclerosis (OR = 1.48, 95% CI: 1.17–1.87). LAP was reported in only one study, with an OR of 1.43 (95% CI: 1.29–1.58), and was presented descriptively. In AIP subgroup analyses, significant associations were observed across carotid plaque type, study design, and sample-size strata. Sex-stratified analysis for VAI revealed a significant association in men but not in women; however, this finding should be interpreted cautiously. This systematic review and meta-analysis suggest that AIP and VAI are significantly associated with carotid atherosclerosis-related outcomes and may serve as useful supplementary metabolic markers for carotid atherosclerosis risk assessment. LAP showed a positive association in the single available study, but its clinical relevance requires further validation. Considering the small number of studies and the observational nature of the data, further large-scale prospective studies are required to corroborate these findings. The study protocol was registered with the International Platform of Registered Systematic Review and Meta-analysis Protocols (INPLASY) database (registration number: INPLASY202550082).
Introduction
Carotid atherosclerotic plaque is a primary driver of ischemic stroke pathophysiology and other cardiovascular diseases. It is closely related to lipid metabolism disorders, inflammatory responses, and visceral fat distribution.1–3 Based on global epidemiologic data, 3 in 2020, the estimated prevalence of carotid plaque among individuals aged 30 to 79 years was 21.1%, with a higher prevalence in men than in women. The formation of these plaques may be unstable, which increases the chance of rupture and could negatively impact patients’ clinical outcomes. Unstable plaques are characterized by a thin fibrous cap, a large lipid core, and intraplaque hemorrhage. 4 Furthermore, carotid plaques can be categorized based on their ultrasound characteristics into homogeneous or heterogeneous structures. Typically, heterogeneous plaques are unstable and associated with a higher incidence of ischemic stroke. 5 Traditional lipid indices such as low-density lipoprotein (LDL)-cholesterol (LDL-C) are fundamental for the assessment of cardiovascular disease risk; however, they are often unable to fully capture vascular damage, particularly the heterogeneity of the carotid plaques. 6 Composite lipid indices, which include the Atherogenic Index of Plasma (AIP), Visceral Adiposity Index (VAI), and Lipid Accumulation Product (LAP), are considered more comprehensive tools as they can better reflect metabolic disorders. This is primarily due to their integration of lipid profiles with body composition parameters, thus revealing vascular damage.7,8
AIP is a reliable marker for estimating the proportion of small and dense LDL particles, and higher levels are independently associated with the severity of coronary artery disease (CAD). 9 VAI captures metabolic dysfunction and visceral lipid function and provides a much more accurate discrimination in intracranial artery stenosis risk compared to body mass index (BMI). 10 LAP measures abdominal lipid accumulation, where a threshold exceeding 30 is associated with a 2.58-fold rise in the likelihood of carotid intra-plaque hemorrhage. Current research shows that these indices show variability in predicting cardiovascular diseases, 11 placing them all as lipid indicators. They are often studied together because they collectively represent a composite of dyslipidemia and visceral lipid dysfunction. AIP is independently associated with adverse cardiovascular events (such as MACE, stroke, and myocardial infarction) even after adjusting for LDL levels. 12 This suggests that it reflects mechanisms beyond traditional indices, such as oxidative stress. VAI and LAP are markers of visceral adiposity and lipotoxicity. When these indices are elevated, they indicate dysfunctional adipose tissue. Dysfunctional adipose tissue creates a pathophysiological cascade of increased circulation of pro-inflammatory adipokines, which can lead to reduced plaque stability.13–15 Consequently, the combined measurement of AIP, VAI, and LAP outperforms traditional markers and provides a more comprehensive assessment of cardiovascular risk by integrating metabolic, anthropometric, and plasma atherogenicity data. Traditional markers often focus on single indices, which lack an in-depth analysis of plaque stability and compositional characteristics.16,17 Moreover, they fail to carry out comprehensive integrated analyses of composite lipid indices, particularly for carotid plaque imaging phenotypes (e.g. calcification pattern, lipid core volume).18,19
While superior, these composite markers lack established diagnostic thresholds, and the predictive effectiveness of indices varies across different populations (e.g. diabetes mellitus, chronic kidney disease). For example, the optimal cutoff value for LAP is 40% lower in patients with chronic kidney disease than in the general population. 8 Furthermore, current studies only measure the relationship between distinct composite indices and pathological processes associated with CAD.20–22 Based on these limitations, this study aimed to clarify the associations between AIP, VAI, and LAP with carotid atherosclerosis (CAS) and carotid plaque, and to investigate their potential as non-invasive biomarkers through a systematic evaluation and meta-analysis. This approach could offer valuable insights for personalized risk assessment and targeted lipid-lowering therapies.
Materials and methods
Protocol and registration
This meta-analysis was conducted in accordance with the Observational Studies in Epidemiology (MOOSE) guidelines and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 statement to ensure thorough and transparent reporting.23,24 These guidelines provide a standardized framework for conducting and reporting systematic reviews and meta-analyses. In addition, the study protocol was registered with the International Platform of Registered Systematic Review and Meta-analysis Protocols (INPLASY) database (registration number: INPLASY202550082). All review procedures, including literature search, study selection, data extraction, and statistical analysis, were conducted following the established protocol to improve reproducibility and minimize reporting bias.
Literature search strategy
Four international databases, including PubMed, Cochrane, Embase, and Web of Science, were searched comprehensively for relevant studies examining the relationship between composite lipid indices (AIP, VAI, and LAP) and carotid atherosclerosis from the inception of each database until May 2025 (Figure 1). Related Medical Subject Headings (MeSH) in PubMed, Emtree terms in Embase, and free-text keywords using Boolean operators (“AND,”“OR”) were also used to broaden the search results. The core search strategy was structured as follows: (“atherogenic index of plasma” OR “AIP” OR “visceral adiposity index” OR “VAI” OR “lipid accumulation product” OR “LAP”) AND (“carotid atherosclerosis” OR “carotid plaque” OR “carotid artery plaque” OR “carotid stenosis”). No language limitations were enforced during the preliminary search to reduce selection bias. Studies published in languages other than English were translated as needed. Through our search, relevant literature was identified and retrieved to minimize publication bias and maximize the reliability of our findings. The detailed search strategies are listed in Supplemental Tables 1–4.
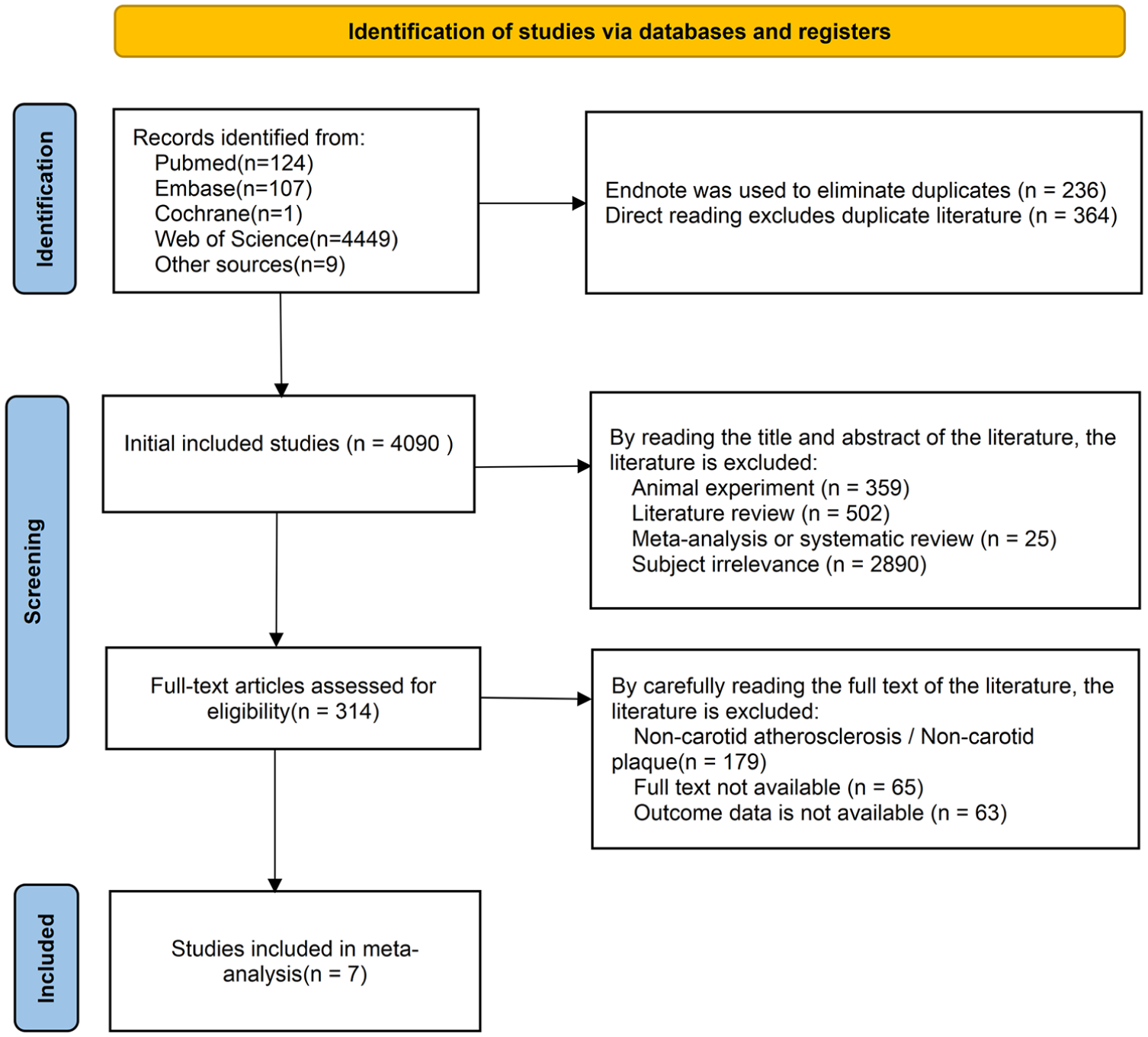
Flow diagram of the literature search and study selection process.
Inclusion criteria
The inclusion criteria consisted of studies that met the PECO framework: (1) study population aged 18 years or older, regardless of sex or ethnicity; (2) studies that examined at least one composite lipid index, including the AIP, VAI, or LAP; (3) these indices are compared to disease outcomes of interest, including carotid atherosclerosis, carotid artery plaque, or carotid atherosclerotic plaque; (4) the disease outcomes of interest diagnosed by imaging methods, including carotid ultrasonography, computed tomography angiography (CTA), or magnetic resonance angiography (MRA), according to recognized clinical or imaging criteria, such as increased carotid intima-media thickness or focal plaque formation; 25,26 and (5) observational studies, including cross-sectional, case–control, and cohort studies. 27 Studies had to report adjusted effect estimates, which consist of odds ratios (ORs), hazard ratios (HRs), or relative risks (RRs) with the associated 95% confidence intervals (CIs), or to provide enough data for their extraction. When multiple adjusted models were reported, the estimate from the model with the most complete adjustment for potential confounders was extracted.
Exclusion criteria
Studies were excluded if they met any of the following criteria: (1) studies analyzing pediatric populations exclusively; (2) studies that did not evaluate AIP, VAI, LAP, or other relevant composite lipid indices; (3) studies that did not report carotid atherosclerosis, carotid artery plaque, or carotid atherosclerotic plaque as outcomes; (4) studies reporting only unadjusted estimates or univariate analyses without sufficient adjusted data; and (5) duplicate publications or studies that involve overlapping populations. When populations overlap, the study with the largest sample size, the most complete data, or the most significant outcome information was kept; and (6) reviews, meta-analyses, conference abstracts, case reports, editorials, letters, animal experiments, or studies without sufficient original data for quantitative or descriptive synthesis. No limitations were placed on the year of publication.
Literature screening and data extraction
Based on predefined criteria, two reviewers (Song and Ouyang) independently screened the titles, abstracts, and full texts of the included articles to appraise their inclusion eligibility. In the event of a disagreement, the original articles were examined again, and consensus was reached through a discussion. Relevant data were extracted, including author names, publication year, grouping basis, lipid index, study type, carotid plaque outcome type, sample population, sample size, age, gender, OR, lower CI, upper CI, diagnostic criteria, corrected model, and covariate adjustments. 28 These data are then organized into Table 1.
Basic information on included studies.
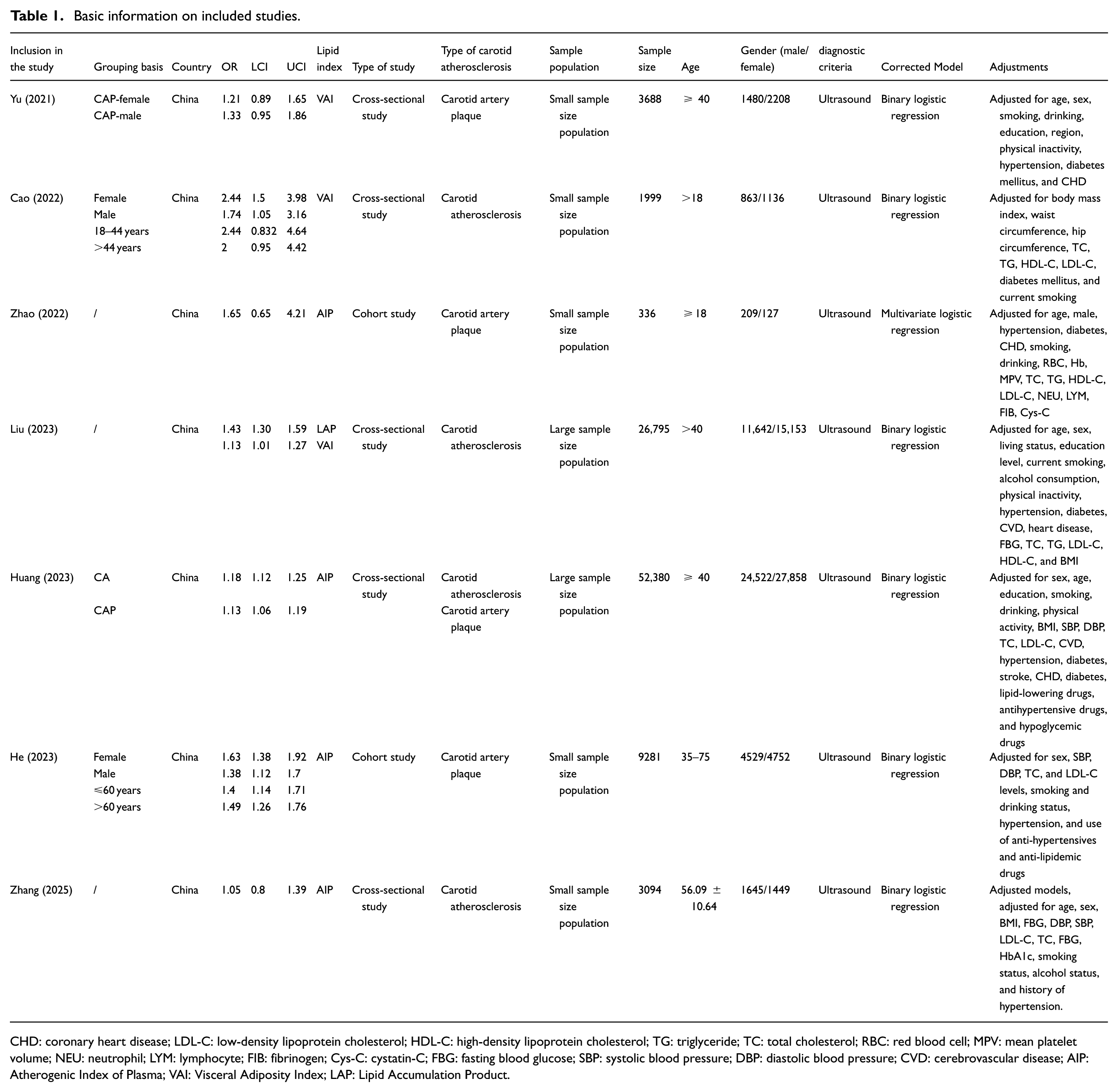
CHD: coronary heart disease; LDL-C: low-density lipoprotein cholesterol; HDL-C: high-density lipoprotein cholesterol; TG: triglyceride; TC: total cholesterol; RBC: red blood cell; MPV: mean platelet volume; NEU: neutrophil; LYM: lymphocyte; FIB: fibrinogen; Cys-C: cystatin-C; FBG: fasting blood glucose; SBP: systolic blood pressure; DBP: diastolic blood pressure; CVD: cerebrovascular disease; AIP: Atherogenic Index of Plasma; VAI: Visceral Adiposity Index; LAP: Lipid Accumulation Product.
Study quality assessment
Two assessors appraised study quality using criteria recommended by the Agency for Healthcare Research and Quality (AHRQ). 29 The following aspects were evaluated: (1) A clearly defined data source; (2) the criteria for inclusion and exclusion for both the exposed and non-exposed groups, either established or cited from earlier research; (3) a specified time frame for identifying patients; (4) whether the subjects were selected consecutively, and whether the selection of study subjects was not population-based; (5) the extent to which the subjective biases of the assessors influence other elements of the study subjects; (6) whether quality assurance measures were performed and reported; (7) whether the reasons for patient exclusion were explained; (8) whether measures to evaluate or control for confounders were reported; (9) whether the handling method of missing data was mentioned, if applicable; (10) whether the response rate and data collection completeness were mentioned; and (11) whether the percentage of incomplete patient data or follow-up results were described, if follow-up was conducted. Each item was assessed as “yes,”“no,” or “unclear.”
Statistical analysis
All statistical analyses were performed and reported according to standard methodological guidelines, 30 using STATA 18.0. Adjusted odds ratios (ORs) and corresponding 95% confidence intervals (CIs) were extracted as the primary effect measures. When an included study reported multiple adjusted models, the estimate from the model with the most comprehensive adjustment for possible confounders was selected. ORs and 95% CIs were transformed into log ORs and standard errors for meta-analysis and then back-transformed to ORs for presentation. Given the clinical and methodological differences observed in the included observational studies, such as variations in study populations, definitions of carotid plaque outcomes, and covariate adjustments, random-effects models based on the DerSimonian–Laird method were used for the pooled analyses. 31 Heterogeneity was assessed using Cochran’s Q test and the I2 statistic. I2 values of approximately 25%, 50%, and 75% were considered to indicate low, moderate, and high heterogeneity, respectively.
To ensure consistency between the analysis and the study’s objective and meta-analytic principle, 32 a quantitative synthesis was conducted separately for each composite lipid index rather than pooling different indices together. The AIP and VAI were analyzed as independent meta-analytic groups. The LAP was descriptively summarized and was not included in the formal pooled meta-analysis since just one eligible study reported the LAP.
Predefined subgroup analyses were conducted only within the same lipid index when sufficient data were available. For AIP, subgroup analyses were performed according to carotid plaque outcome type, study design, and sample size group. For VAI, subgroup analysis was performed by sex. For LAP, subgroup analysis was not performed because only one eligible study was available. Certain subgroup combinations could not be analyzed due to insufficient data; Table 2 lists the reasoning.
Subgroup analysis summary.
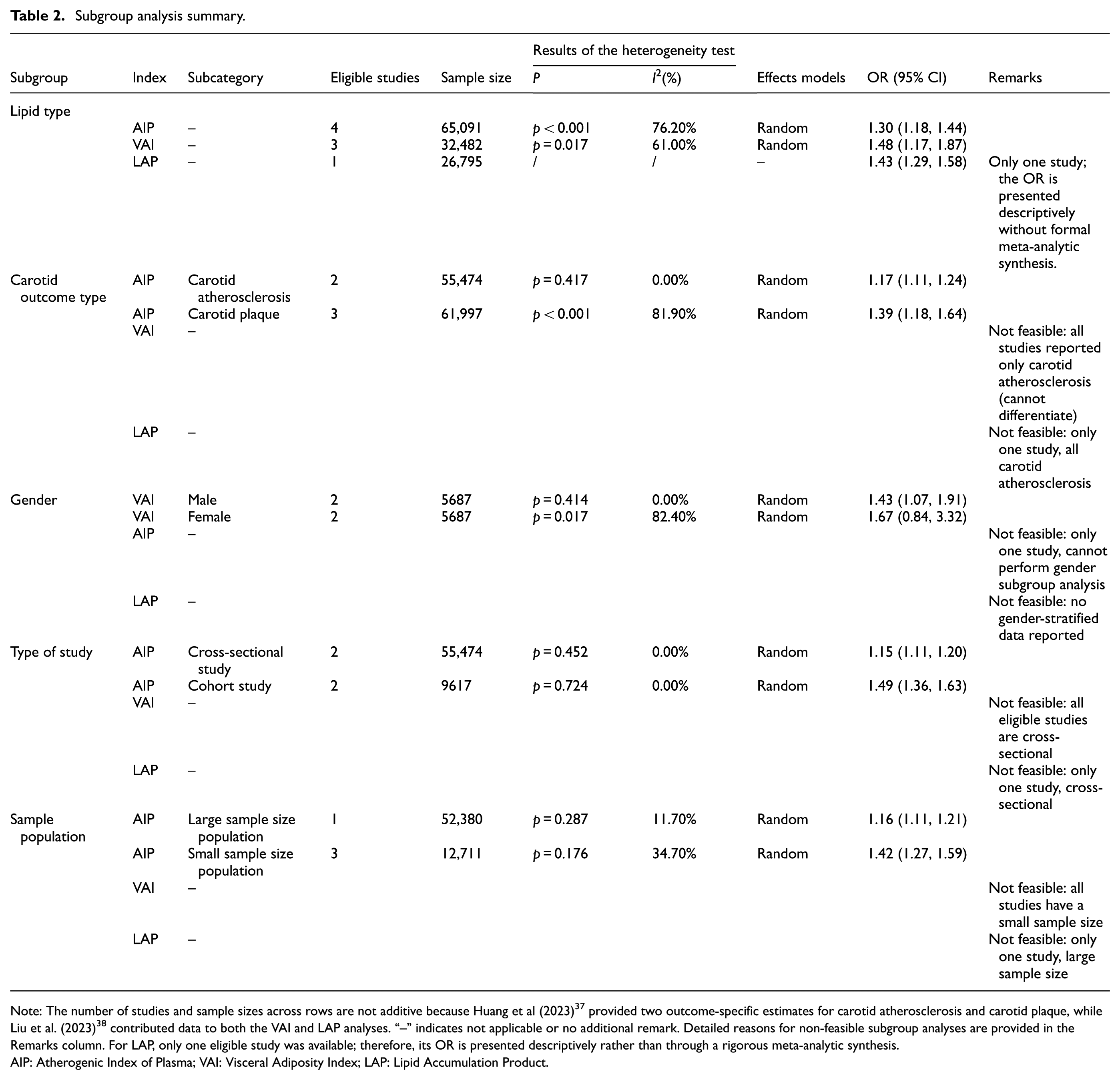
Note: The number of studies and sample sizes across rows are not additive because Huang et al (2023) 37 provided two outcome-specific estimates for carotid atherosclerosis and carotid plaque, while Liu et al. (2023) 38 contributed data to both the VAI and LAP analyses. “–” indicates not applicable or no additional remark. Detailed reasons for non-feasible subgroup analyses are provided in the Remarks column. For LAP, only one eligible study was available; therefore, its OR is presented descriptively rather than through a rigorous meta-analytic synthesis.
AIP: Atherogenic Index of Plasma; VAI: Visceral Adiposity Index; LAP: Lipid Accumulation Product.
Publication bias was assessed using funnel plots and Egger’s regression test 33 when the number of available studies was sufficient. The results of the publication bias evaluation were interpreted cautiously since each index-specific analysis included a limited number of studies. Sensitivity analysis was performed by sequentially omitting one study at a time to evaluate the robustness of the pooled estimates. 34 A two-sided P value <0.05 was considered statistically significant.
Results
Characteristics of the included studies
This study incorporated a total of 7 eligible observational studies, encompassing a cumulative sample size of 97,573 participants (44,890 males and 52,683 females).35–41 These included one study on LAP (involving 26,795 participants), three on VAI (involving 32,482 participants), and four on AIP (involving 65,091 participants). While only one study has analyzed LAP, it has been considered due to its relevance as a composite lipid indicator that is of current research interest. Its effect size contributes to a preliminary assessment of the association trend; however, it is crucial to note that subgroup analysis and robustness checks were not conducted, necessitating a cautious interpretation of its findings.
The baseline characteristics and quality assessment of the included studies are detailed in Table 1 and Supplemental Table 5. Publication bias tests and sensitivity analyses were performed separately for AIP and VAI. The results demonstrated that the funnel plots exhibited a generally symmetrical distribution, and Egger’s test indicated no significant publication bias. Following the sequential exclusion of individual studies, the sensitivity analysis results remained robust and showed no obvious directional changes in the effect size, reflecting the reliability of the pooled results. Due to the inclusion of only one study for LAP, the corresponding publication bias and sensitivity analyses could not be performed (Figures 2–4).
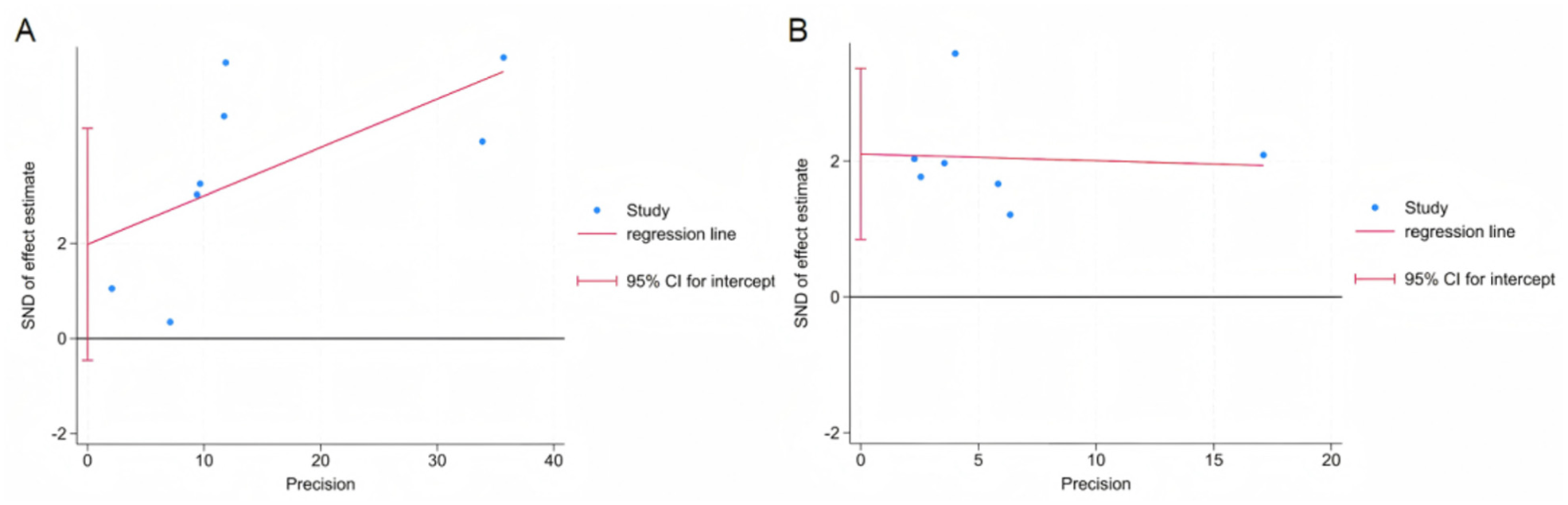
Egger’s regression test for publication bias. (a) Egger’s test plot for studies reporting the association between the AIP and carotid plaque and (b) Egger’s test plot for studies reporting the association between the VAI and carotid plaque.
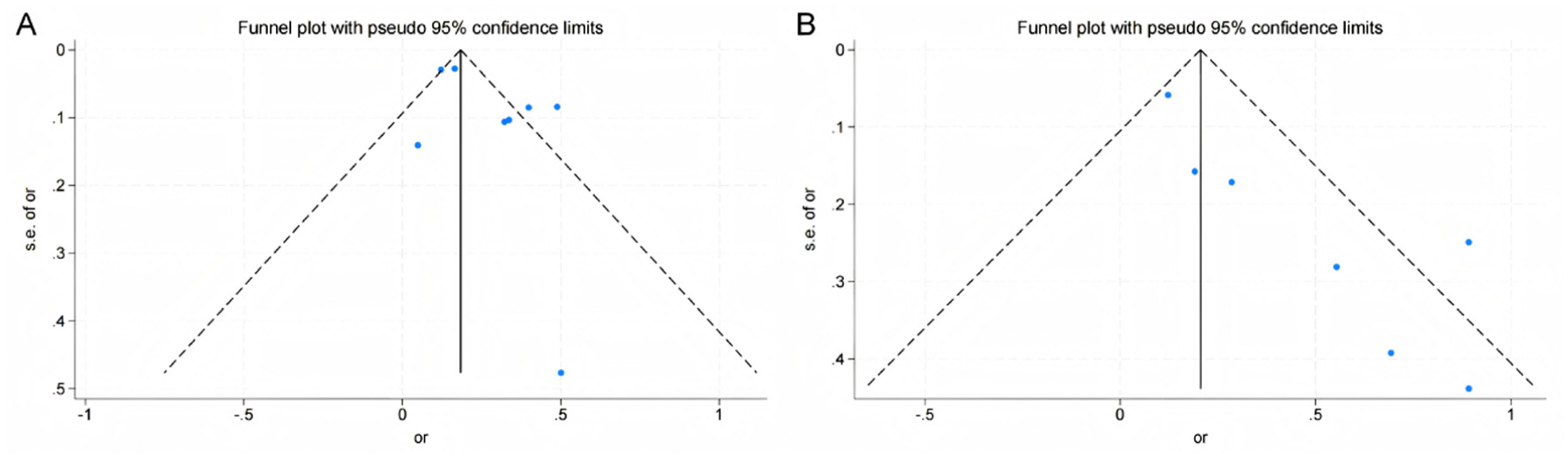
Funnel plots for assessing publication bias. (a) Funnel plot of studies reporting the association between the AIP and carotid plaque and (b) funnel plot of studies reporting the association between the VAI and carotid plaque.
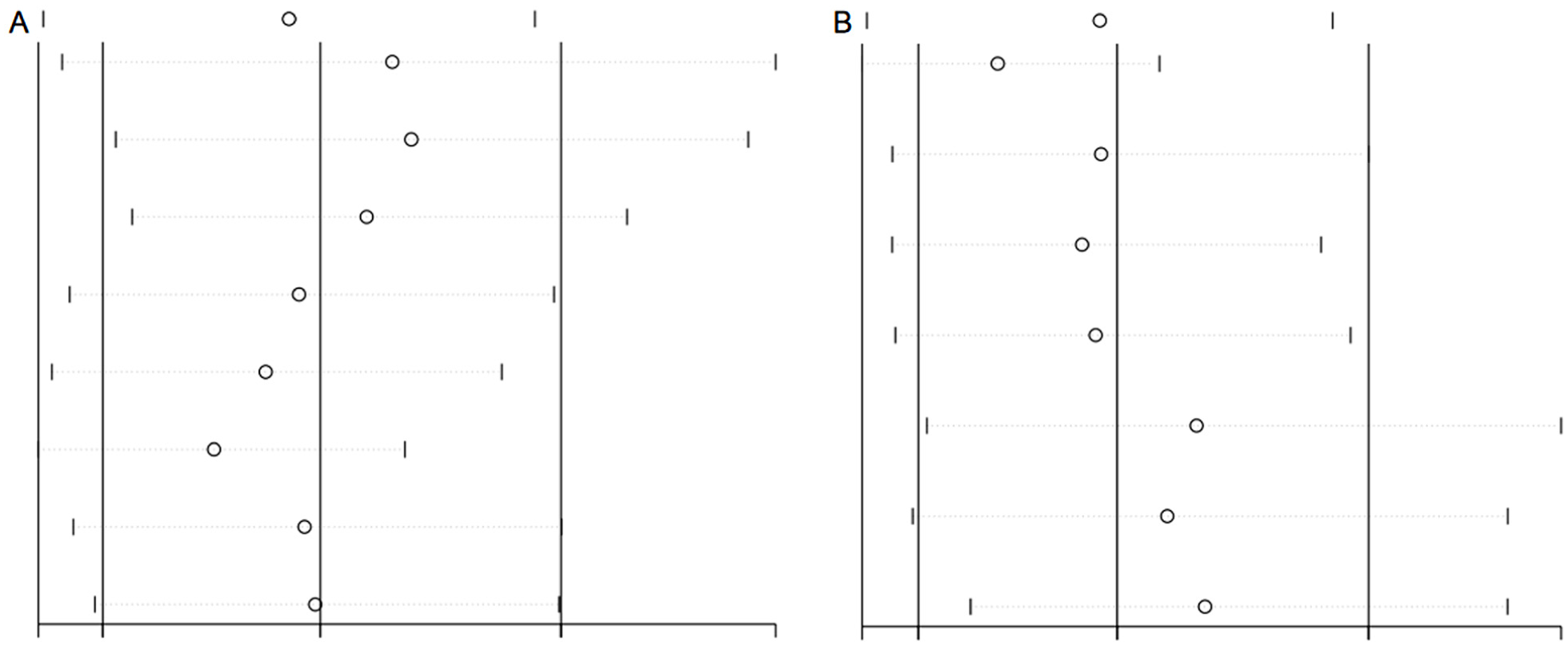
Leave-one-out sensitivity analysis of the overall results. (a) Sensitivity analysis plot for studies reporting the association between the AIP and carotid plaque and (b) sensitivity analysis plot for studies reporting the association between the VAI and carotid plaque.
Primary analysis of the association between different composite lipid indices and carotid atherosclerotic plaque
Given the unique biological significance of each lipid index, index-specific analyses were performed to evaluate the relationships between atherosclerosis-related outcomes and AIP, VAI, and LAP (Table 2 and Figure 5). In the four studies that reported AIP, the pooled OR was 1.30 (95% CI: 1.18–1.44), exhibiting moderate heterogeneity (I2 = 76.2%, p < 0.001), with the application of a random-effects model. For the three studies reporting VAI, the pooled OR was 1.48 (95% CI: 1.17–1.87), showing moderate heterogeneity (I2 = 61.0%, p = 0.017), with the application of a random-effects model.
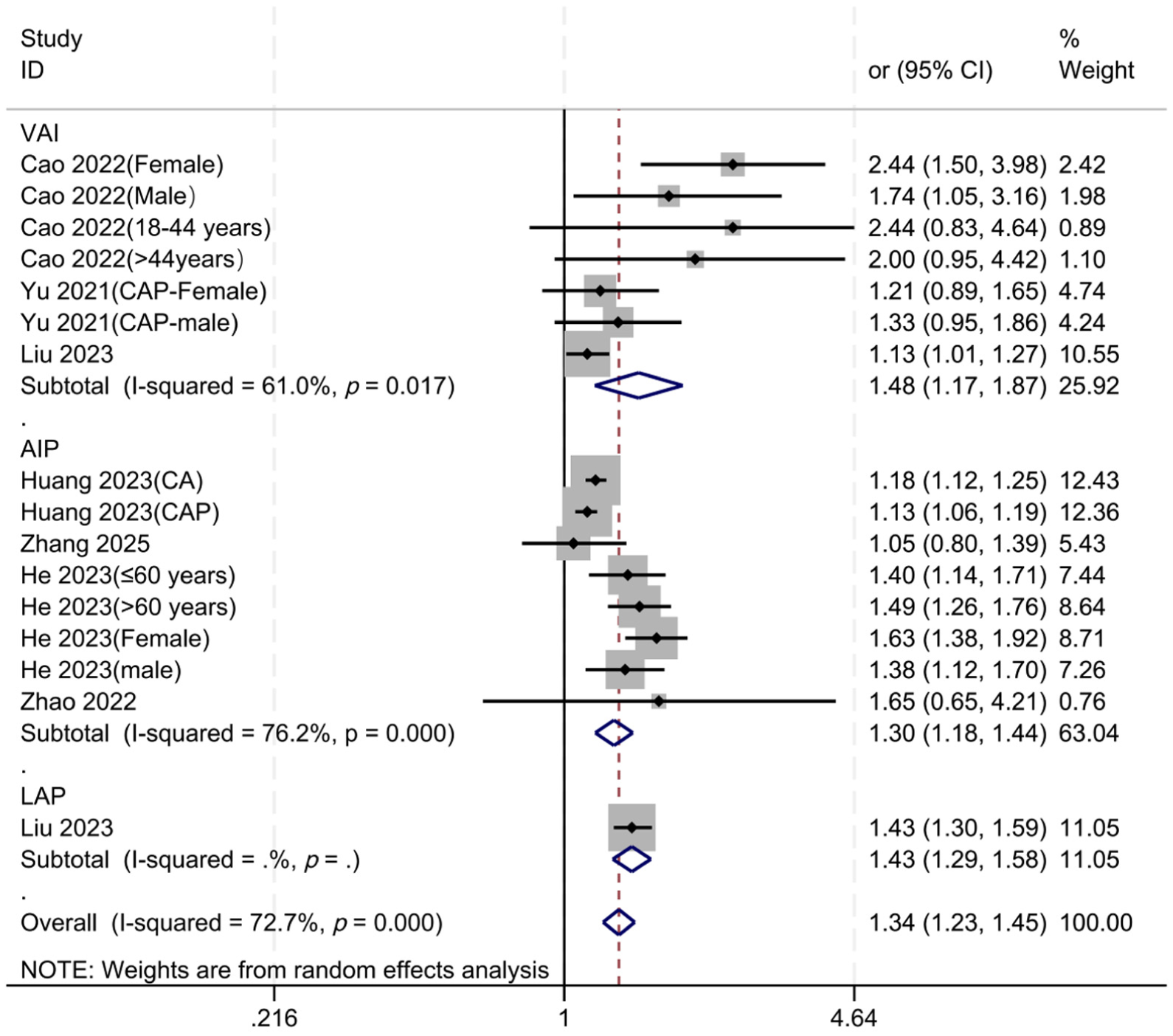
Forest plot indicating the association between composite lipid indices and the outcome, stratified by index type: VAI, AIP, and LAP.
Only one eligible study reported LAP, with an OR of 1.43 (95% CI: 1.29–1.58). Therefore, LAP was not included in a formal pooled meta-analysis and was presented descriptively only. Overall, the quantitative results mainly support positive associations of AIP and VAI with carotid atherosclerosis-related outcomes. While LAP demonstrated a positive correlation in the single available study, this finding should be interpreted cautiously and requires further validation in future studies.
Subgroup analysis
To explore potential sources of heterogeneity, subgroup analyses were conducted according to carotid pathology outcomes, outcome type, sex, study design, and sample size, where data were available. The Remarks column of Table 2 lists the explanations for index–subgroup combinations that could not be examined as a result of insufficient data. Subgroup analyses for LAP were not carried out as only one study reported LAP; this study was cross-sectional, focused on carotid atherosclerosis, and lacked sex-stratified data.
For AIP, subgroup analyses were performed according to carotid pathology outcome type, study design, and sample size. When stratified by carotid pathology outcome type, the pooled OR was 1.17 (95% CI: 1.11–1.24; I2 = 0%) for carotid atherosclerosis and 1.39 (95% CI: 1.18–1.64; I2 = 81.9%) for carotid plaque (Figure 6), suggesting a stronger association between AIP and carotid plaque. In the analysis of subgroups based on study design, the pooled odds ratio (OR) was found to be 1.15 (95% CI: 1.11–1.20; I2 = 0%) for cross-sectional studies, while for cohort studies, it was 1.49 (95% CI: 1.36–1.63; I2 = 0%), as illustrated in Figure 7. In the analysis of subgroups based on sample size, the large-sample subgroup included only one study, Huang et al (2023), 37 which reported two outcome definitions: carotid atherosclerosis and carotid plaque. The summary OR, based on these two estimates, was 1.16 (95% CI: 1.11–1.21; I2 = 11.7%). In the subgroup with a small sample size, comprising three studies, the pooled OR was 1.42 (95% CI: 1.27–1.59; I2 = 34.7%) (Figure 8). The findings from these subgroups must be interpreted with caution, as the large-sample subgroup was derived from a single study, and its two estimates were obtained from different outcome definitions within the same study population. Sex-stratified subgroup analysis for AIP was not conducted, as only one study provided sex-specific data.
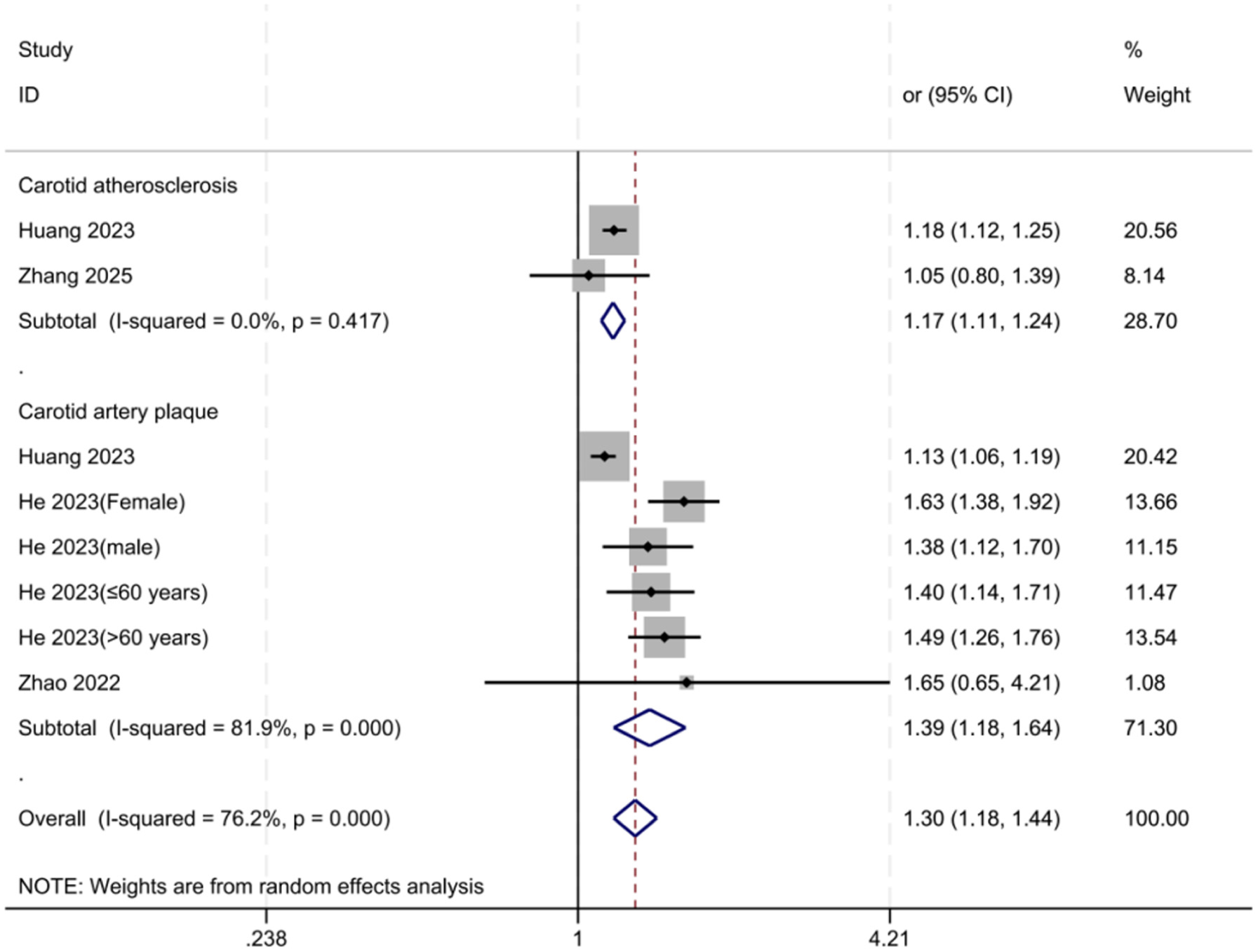
Forest plot of the subgroup analysis of the association between AIP and carotid pathology outcomes, stratified by carotid pathology outcome type.
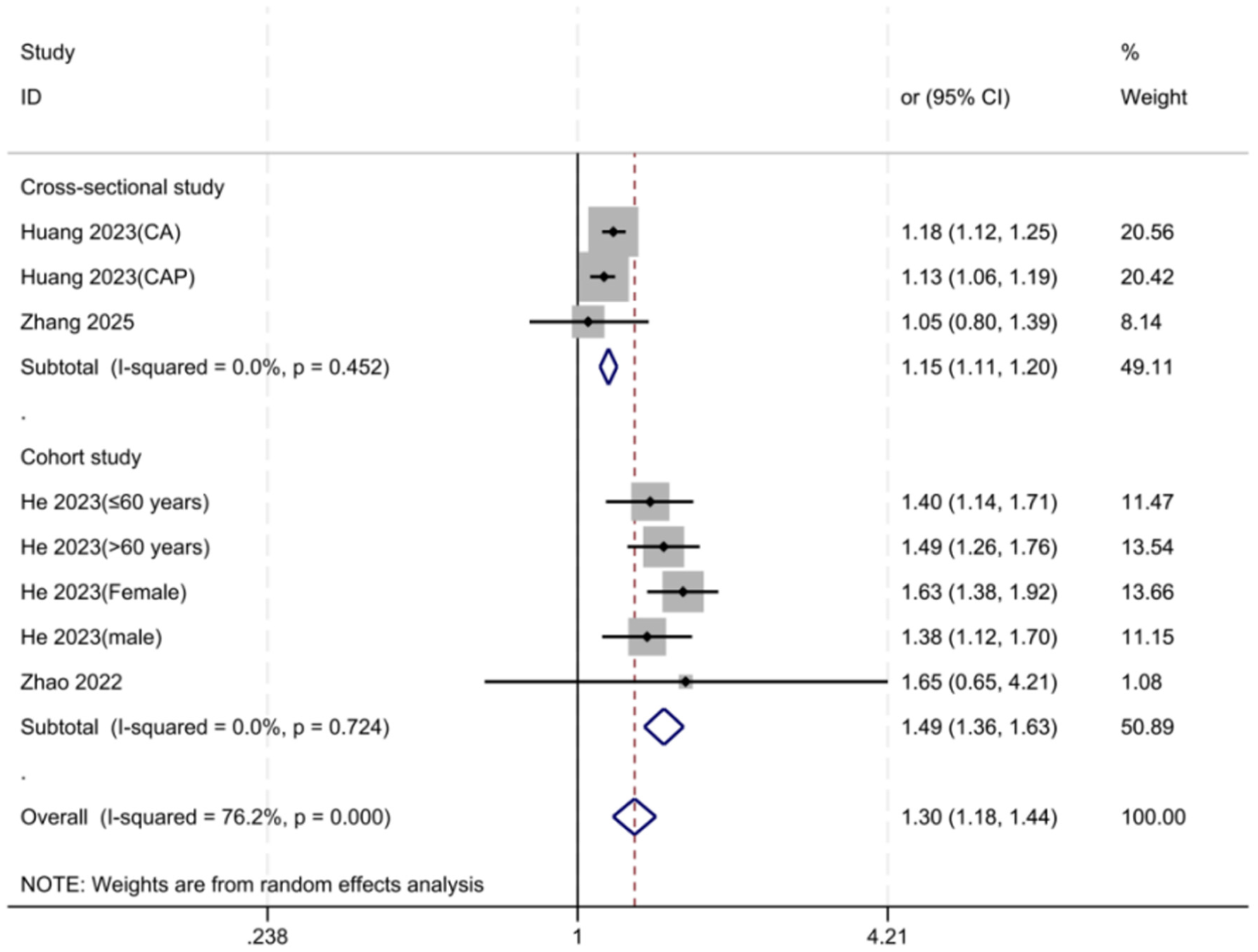
Forest plot of the subgroup analysis of the association between AIP and carotid pathology outcomes, stratified by study design.
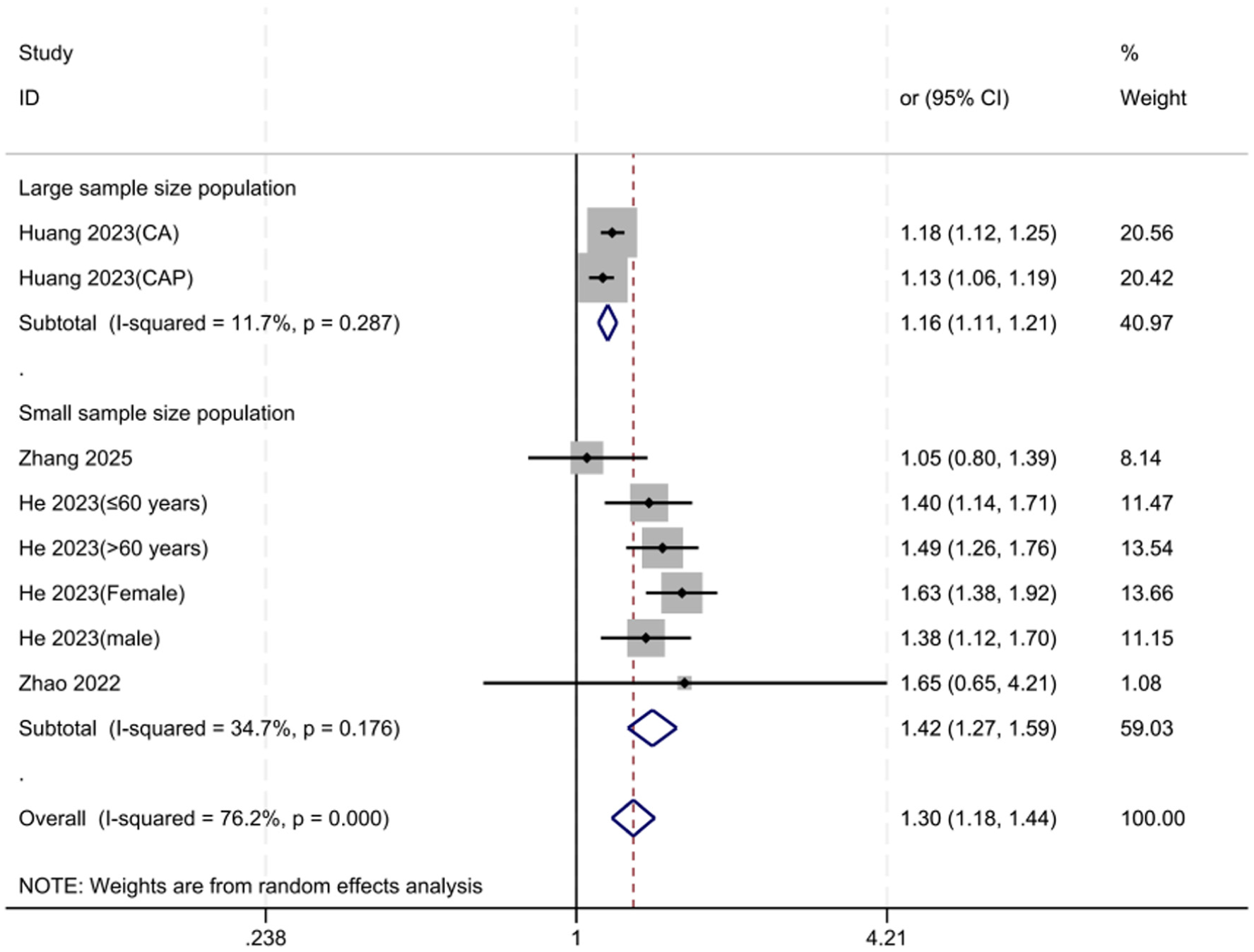
Forest plot of the subgroup analysis of the association between AIP and carotid pathology outcomes, stratified by sample size.
For VAI, subgroup analysis was only stratified based on sex. The pooled OR was 1.43 (95% CI: 1.07–1.91; I 2 = 0%) in men and 1.67 (95% CI: 0.84–3.32; I2 = 82.4%) in women (Figure 9). While the association was statistically significant in men but not in women, this finding should be interpreted as exploratory, as only two studies provided sex-stratified data, and notable heterogeneity was observed in the female subgroup. In addition, all VAI studies included were cross-sectional in nature, categorized as small-sample studies, and reported on carotid atherosclerosis without differentiating between plaque types. Therefore, subgroup analyses of VAI by study design, sample size, or carotid pathology outcome type could not be performed.
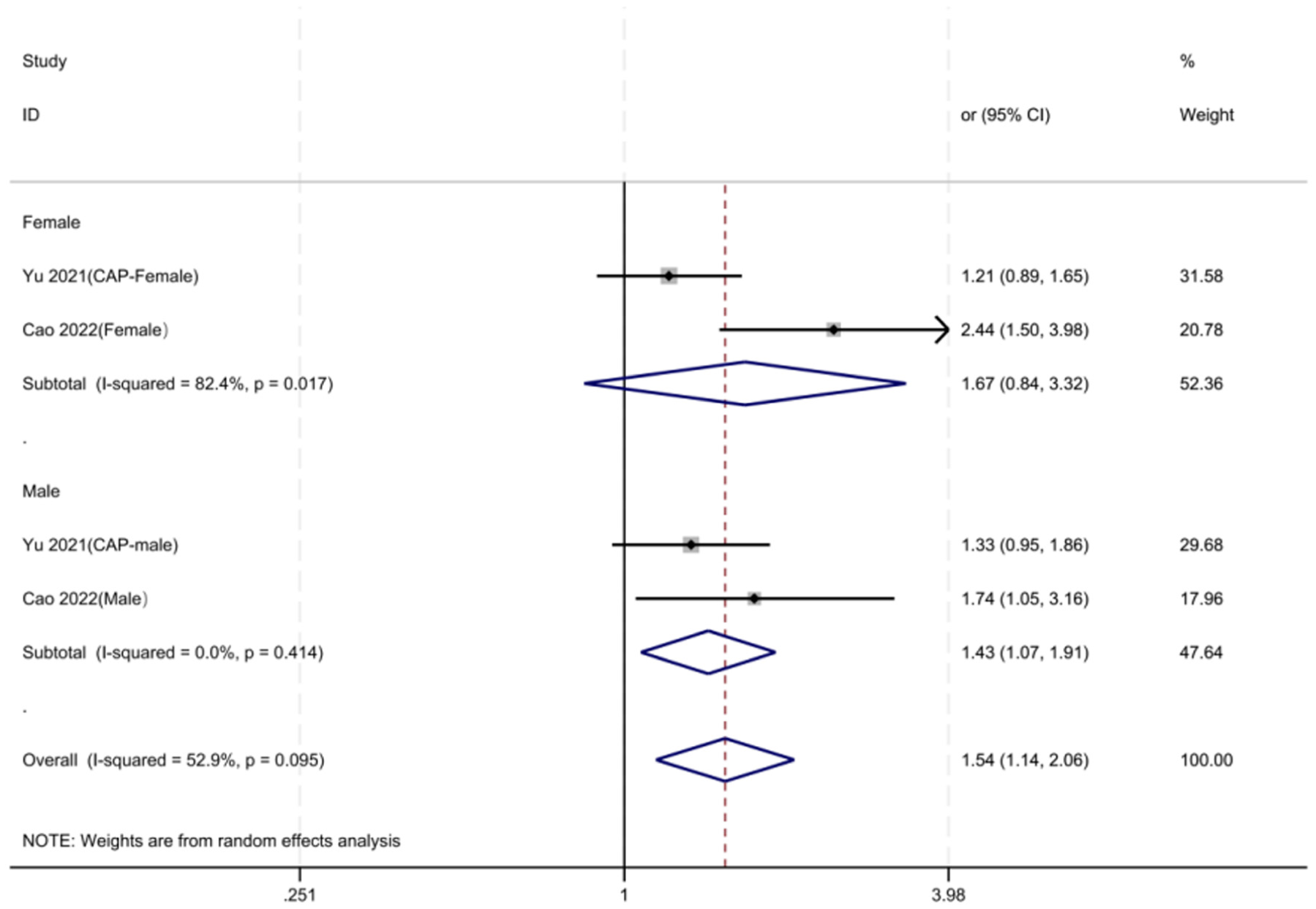
Forest plot of the subgroup analysis of the association between VAI and carotid atherosclerosis, stratified by sex.
Discussion
This systematic review and meta-analysis evaluated the association between composite lipid indices and carotid atherosclerosis-related outcomes. The primary results demonstrated a strong correlation between increased odds of carotid atherosclerosis or carotid plaque and both the AIP and the VAI. In particular, carotid pathology outcomes were positively correlated with AIP, and VAI was also significantly associated with carotid atherosclerosis. Since only a single eligible study provided data on the LAP, it was excluded from the formal pooled meta-analysis and instead summarized descriptively. Therefore, the findings mainly support the potential value of AIP and VAI as complementary metabolic indicators for carotid atherosclerosis risk assessment, whereas the clinical relevance of LAP still requires further validation. Lipid metabolism disorders play a central role in the development of atherosclerosis and plaque progression. 42 The combined effects of dyslipidemia, insulin resistance, visceral adiposity, and systemic inflammation may not be adequately reflected by single lipid markers, despite the widespread use of traditional lipid parameters, including LDL-C, triglycerides, HDL-C, and total cholesterol in cardiovascular risk assessment. 43 Composite lipid indices integrate lipid abnormalities with metabolic or anthropometric characteristics, and this may provide additional information for assessement. 44 Previous studies have also suggested that composite metabolic indices, such as the triglyceride-glucose index, are associated with carotid atherosclerosis and plaque formation, supporting the concept that combined metabolic indicators may better capture the multifactorial nature of atherosclerosis than isolated lipid parameters. 45 However, unlike TyG, this study specifically targeted AIP, VAI, and LAP, which are more directly related to atherogenic lipid balance, visceral adipose dysfunction, and abdominal lipid accumulation.10,46 The biological plausibility of the association between AIP and carotid atherosclerosis is supported by several mechanisms. It has been demonstrated that AIP reflects the balance between triglycerides and HDL-C and is considered an indirect marker of atherogenic dyslipidemia, particularly small dense LDL particles. 47 These particles are more readily oxidized, have a greater tendency to infiltrate the arterial wall, and exhibit a stronger correlation with endothelial dysfunction, inflammation, and plaque instability. 48 Increased carotid intima-media thickness and carotid plaque formation have been linked to elevated AIP, and new cohort data indicate that cumulative AIP could be a predictor of new carotid plaque formation, surpassing the predictive value of triglycerides or HDL-C alone.37,49 These vascular changes may be mediated by oxidative stress, lipid deposition, endothelial injury, and inflammatory activation. 48 Furthermore, a recent study found a nonlinear correlation between AIP and unstable carotid plaque, which was defined by plaque echogenicity and morphological features like incomplete fibrous cap or ulceration. This suggests that AIP may be associated with both the presence of carotid plaque and plaque vulnerability. 50 These mechanisms may partly explain why AIP showed a consistent positive association with carotid pathology outcomes in the present meta-analysis.
VAI may reflect another important pathway linking visceral adiposity and carotid atherosclerosis. VAI is calculated using waist circumference, BMI, triglycerides, and HDL-C, and it indirectly reflects visceral adipose dysfunction, insulin resistance, and abnormal lipid storage.51,52 Visceral adipose tissue is considered both a passive energy store and an active endocrine inflammatory organ. 53 Dysfunctional visceral fat can promote chronic low-grade inflammation through the release of pro-inflammatory adipokines and cytokines, aggravate insulin resistance, increase oxidative stress, and impair endothelial function.53–55 These processes may accelerate vascular smooth muscle cell activation, extracellular matrix remodeling, arterial wall thickening, and plaque formation. 55 The results of this analysis are in line with earlier research that found positive correlations between VAI and carotid intima-media thickness, intracranial or extracranial atherosclerotic burden, and cardiovascular outcomes.10,46,51,56 Consequently, VAI could be a beneficial marker for identifying individuals whose carotid atherosclerosis risk is driven by visceral adiposity and metabolic dysfunction.
Due to the availability of only one eligible trial, LAP was excluded from the formal pooled analysis; however, its potential significance should not be disregarded. LAP is a measure of lipid accumulation in the abdomen and is strongly associated with visceral fat deposition and cardiometabolic risk.10,57 Excess lipid accumulation may contribute to endothelial dysfunction, oxidative stress, insulin resistance, and inflammatory activation, all of which are involved in the development of atherosclerosis.58,59 Previous studies have reported associations between LAP and broader atherosclerotic burden, including coronary, intracranial, and extracranial atherosclerosis; however, direct evidence linking LAP to specific carotid plaque vulnerability features remains limited. 56 Future research should clarify whether LAP is linked to these imaging-defined plaque characteristics due to plaque composition, such as intraplaque hemorrhage, lipid-rich necrotic core, calcification pattern, and stenosis, which more closely determine plaque vulnerability. 60 Nevertheless, the evidence for LAP in the present review was limited to a single study, so its association with carotid atherosclerosis should be interpreted cautiously. Future studies are needed to clarify whether LAP has independent predictive value beyond AIP, VAI, and conventional lipid parameters.
The present findings are generally consistent with previous studies showing that composite lipid indices are associated with subclinical atherosclerosis and vascular injury. 61 These indicators may more accurately represent the combined effects of dyslipidemia, insulin resistance, visceral obesity, and systemic inflammation than conventional lipid measures. 62 However, the level of correlation was not uniform across the various indices and subgroups. This variation may be partially attributed to the unique biological significance associated with each index. AIP mainly reflects atherogenic lipid imbalance, whereas VAI and LAP are more closely related to visceral adipose dysfunction and lipid accumulation.63,64 Therefore, these indices should not be regarded as interchangeable markers, but rather as complementary indicators reflecting different metabolic pathways involved in carotid atherosclerosis. 65
The subgroup analyses provided additional information, although only explanatory. 66 For AIP, positive associations were observed across different carotid outcome types, study designs, and sample-size groups. The association appeared stronger in the carotid artery plaque subgroup than in the carotid atherosclerosis subgroup, which may suggest that AIP is more closely related to plaque formation or plaque-related vascular injury. 67 In addition, the pooled effect estimate appeared higher in cohort studies than in cross-sectional studies. This result might suggest that AIP could be useful in long-term risk assessment, but it should be interpreted cautiously due to the small number of available studies and the possibility that variations in study population, diagnostic criteria, follow-up design, and covariate adjustment affected the findings.66,67 For VAI, sex-stratified analysis suggested a significant association in men, whereas the association in women was not statistically significant. This difference may be related to sex-specific fat distribution, hormonal status, and differences in metabolic risk profiles, but the number of sex-stratified studies was small. 68 Therefore, the sex-specific finding should be considered exploratory rather than definitive.
The findings of this study may have clinical implications. Carotid ultrasonography remains an important imaging method for detecting carotid intima-media thickening and plaque formation.25,26 However, it may not always be feasible for large-scale early screening. Composite lipid indices are simple, inexpensive, and derived from routinely available anthropometric and laboratory parameters.46,67 As a result, AIP and VAI may be useful additional markers for identifying patients more likely to develop carotid atherosclerosis, particularly in groups that have metabolic syndrome, obesity, dyslipidemia, or insulin resistance.37,46,67 Nevertheless, these indices should not replace imaging diagnosis or established cardiovascular risk assessment tools. Instead, they may help improve preliminary risk stratification and provide additional information for early lifestyle intervention and metabolic management.
This study has several strengths. First, it systematically summarized the available evidence on the association between composite lipid indices and carotid atherosclerosis-related outcomes. Second, the updated analysis avoids inappropriately pooling several cholesterol indices in response to methodological issues. Since there was only one relevant study, LAP was summarized descriptively, but AIP and VAI were examined independently. This approach is more consistent with the study objective and improves the interpretability of the results. Third, subgroup analyses were performed only within the same lipid index when sufficient data were available, which reduced methodological inconsistency. In addition, sensitivity analyses and publication-bias assessments were performed for AIP and VAI when data permitted.
The study also had several limitations. First, all included studies were conducted in Chinese populations, which may limit the generalizability of the findings to other ethnic or geographic populations. Second, the number of eligible studies was limited, especially for LAP, which was reported in only one study and could not be formally pooled. Third, the majority of the studies included were observational, with some being cross-sectional; as a result, establishing causal relationships between composite lipid indices and carotid atherosclerosis was not possible. Fourth, certain analyses still showed heterogeneity, which could be caused by variations in diagnostic criteria, outcome definitions, study designs, population characteristics, and covariate adjustment. Fifth, most studies reported the presence of carotid atherosclerosis or plaque but did not provide detailed imaging information on plaque composition, lipid core size, calcification pattern, fibrous cap status, or intraplaque hemorrhage. Finally, residual confounding could not be completely ruled out because the included studies used various correction models. To confirm the clinical applicability of AIP and VAI and to determine whether LAP offers more prognostic information for carotid atherosclerosis and plaque susceptibility, future large-scale prospective studies in diverse populations are required.
Conclusions
Through subgroup analyses of different composite lipid indices, different carotid atherosclerosis types, different genders, different study types, and different sample populations, the present study further demonstrated that the composite lipid indices were strongly associated with the formation and development of carotid atherosclerotic plaque. These findings were similar across genders, study designs, sample sizes, carotid atherosclerosis symptoms, and composite lipid indices, indicating that these indices have excellent predictive potential in a variety of settings. These findings support the potential application of composite lipid indices in assessing carotid atherosclerotic plaque, providing a new biological basis for individualized risk assessment and intervention.
Supplemental Material
sj-docx-1-imj-10.1177_10815589261462549 – Supplemental material for Associations of composite lipid indices with carotid atherosclerosis-related outcomes: A systematic review and meta-analysis focused on AIP and VAI
Supplemental material, sj-docx-1-imj-10.1177_10815589261462549 for Associations of composite lipid indices with carotid atherosclerosis-related outcomes: A systematic review and meta-analysis focused on AIP and VAI by Ji Ouyang, Jiayuan Song, Xingxing Zhang, Yuehang Xu, Peiyao Li and Zhixi Hu in Journal of Investigative Medicine
Footnotes
Acknowledgements
We express our sincere gratitude to Professor Zhixi Hu for his invaluable contributions to the research ideas and funding support for this paper.
Ethical considerations
This study utilized publicly available summary data, and according to relevant guidelines, ethics approval was not required. The use of open-access data ensured the protection of individual privacy, thereby removing the need for additional ethical review.
Author contributions
Conceptualization, Jiayuan Song; Methodology, Ji Ouyang; Software, Ji Ouyang; Validation, Xingxing Zhang; Formal Analysis, Xingxing Zhang; Investigation, Ji Ouyang; Resources, Jiayuan Song; Data Curation, Jiayuan Song; Writing – Original Draft Preparation, Ji Ouyang; Writing – Review & Editing, Jiayuan Song; Visualization, Peiyao Li; Supervision, Peiyao Li; Project Administration, Yuehang Xu; Funding Acquisition, Zhixi Hu. All authors have read and agreed to the published version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (Grant No. 82274412).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The original contributions presented in the study are included in the article; further inquiries can be directed to the corresponding author.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.