
Abstract
Background:
Pneumonia in immunocompromised patients with cancer is associated with high morbidity, diagnostic uncertainty, and poor short-term outcomes. Precision radiopharmaceutical approaches may improve lesion localization, biodistribution assessment, and patient-specific treatment planning in this vulnerable population group.
Methods:
The authors conducted a prospective single-arm study of a DOTA-functionalized antimicrobial peptide radiolabeled with 177Lu in immunocompromised patients with cancer with severe pneumonia. The study evaluated the radiochemical performance, in vitro stability, clinical biodistribution, pulmonary lesion localization, quantitative uptake kinetics, lesion dosimetry, short-term clinical response, and safety. The full cohort included 50 patients, with imaging- and dosimetry-evaluable subgroups of 5 and 15 patients, respectively.
Results:
The radiopharmaceutical demonstrated high radiochemical purity (98.5%) and favorable labeling efficiency, with optimal radiolabeling achieved at 60°C. Whole-body planar imaging and thoracic SPECT/CT revealed persistent pulmonary lesion uptake with improved delayed lesion conspicuity. In the imaging subgroup, the lesion-to-blood pool and lesion-to-normal lung ratios increased over time, indicating progressive lesion contrast. Dosimetric analysis showed the highest absorbed dose in pulmonary lesions (∼4.5 Gy/GBq), exceeding the doses to the kidneys, liver, normal lung, and blood. Eleven of the 15 dosimetry-evaluable patients exceeded the predefined lesion-to-kidney dose ratio threshold of >2.0. Clinically, 35 of the 50 patients (70%) improved, 10 (20%) remained stable, and 5 (10%) worsened. No grade 4 adverse events were observed, and treatment-related toxicities were predominantly grades 1–2.
Conclusions:
177Lu-labeled antimicrobial peptide imaging demonstrated favorable radiochemical characteristics, persistent pulmonary lesion targeting, clinically relevant dosimetric selectivity, and an acceptable short-term safety profile in immunocompromised patients with cancer with severe pneumonia. These findings support the translational potential of this peptide-based radiopharmaceutical as a theranostic platform for imaging-guided dosimetry-informed precision management.
Keywords
Introduction
Immunocompromised patients with cancer frequently develop pneumonia as a severe clinical complication, which is associated with significantly higher morbidity and mortality than that in patients without immune compromise.1,2 Active pulmonary infections in this population are difficult to detect accurately because of the increasing number of cases in which radiological findings are false and vague, host inflammatory responses are often downregulated, and opportunistic or atypical pathogens are frequently observed. 3 These restrictions lower the accuracy of standard diagnostic and treatment methods and necessitate the use of additional specific molecular techniques to localize the infection. Antimicrobial peptides, such as ubiquicidin, have demonstrated selective affinity for microbial membranes and desirable focalization at sites of infection, making them potentially useful as targeted imaging agents.4,5 Specifically, radiolabeled ubiquicidin analogs have been explored as methods for differentiating between infectious lesions and sterile inflammation, thereby increasing the application of molecular imaging in infection-oriented clinical decision-making. 6
In the context of the wider concept of precision oncology, theranostic radiopharmaceutical approaches offer the opportunity to unite lesion imaging, quantitative biodistribution measurements, and personalized dosimetric evaluation into a single platform.7,8 This is of special interest in immunocompromised patients with cancer, where early and correct detection of the infectious burden can affect treatment choice, supportive care, and risk assessment.9,10 Therefore, the authors hypothesized that a DOTA-conjugated antimicrobial peptide labeled with 177Lu could enable quantitative imaging of pneumonia-associated lesions while providing a radiopharmaceutical platform for patient-specific evaluation.11,12 Accordingly, the present study investigated the radiochemical characteristics, in vivo biodistribution, lesion dosimetry, and early clinical performance of 177Lu-labeled antimicrobial peptide imaging in severely ill cancer patients with pneumonia.
Materials and Methods
Study design and patients
This prospective single-arm study evaluated a novel 177Lu-labeled radiopharmaceutical in immunocompromised patients with cancer and pneumonia. Patients were enrolled consecutively over the study period based on predefined inclusion and exclusion criteria, without additional screening or randomization steps. The overall cohort comprised 50 patients, and their baseline demographic, oncologic, and clinical characteristics are summarized in Table 1. Among these patients, five had complete serial imaging datasets for detailed imaging assessment, and 15 were included in the dosimetry-evaluable subgroup. Eligible patients had active malignancies with treatment- or disease-related immunosuppression, clinical and radiographical evidence of pneumonia, and an inadequate response to standard antimicrobial therapy. The exclusion criteria were pregnancy, hemodynamic instability, and contraindications for SPECT/CT imaging.13,14 The study was approved by the Ethics Committee of the First Hospital of Zhangjiakou, Zhangjiakou, China (Approval No. 2026-LW-06). Written informed consent was obtained from all patients/participants involved in this study prior to enrollment and radiopharmaceutical imaging procedures.
Baseline Demographic, Oncologic, and Clinical Characteristics of the Study Cohort

Radiopharmaceutical preparation
A synthetic antimicrobial peptide was conjugated with DOTA to enable 177Lu radiometal chelation. Under aseptic conditions, peptide-DOTA (20 µg) was incubated with 177LuCl3 (5–10 mCi) in 0.4 M ammonium acetate buffer (pH 5.5) for 30 min under optimized labeling conditions. The radiolabeling process was performed within a controlled pH range of 4.5–5.5 to ensure optimal chelation efficiency and complex stability. To mitigate the potential radiolysis effects associated with 177Lu decay, the reaction was conducted under low-oxygen conditions with minimal exposure to light, and the preparation time was kept as short as feasible. No significant radiolysis-related degradation products were detected on radio-HPLC analysis. The reaction mixture was purified using a C18 cartridge. Radiochemical purity was assessed using radio-high-performance liquid chromatography to distinguish free 177Lu from peptide-bound 177Lu. The final radioconjugate exhibited a radiochemical purity of 98.5%. The preparation and quality control of the radiopharmaceutical were performed according to the well-established principles of developing and characterizing radiolabeled peptides.15,16 As this study was conducted as a feasibility investigation with limited synthesis batches, formal batch-to-batch reproducibility assessment was not performed and represents an area for future validation. However, the consistent radiochemical purity and labeling efficiency across preparation runs suggested acceptable process stability within the scope of this feasibility study.
In vitro stability
The purified 177Lu-DOTA-peptide was assessed in vitro in 0.9% saline and 100% human serum. Aliquots of the radioconjugate with approximately 1 mCi of radioconjugate were incubated at 37°C, and three replicas were examined in each medium. Cultures were sampled at 1, 4, and 24 h, and radio-high-performance liquid chromatography was used to determine the percentage of intact radioconjugates. Stability remained >95% at 24 h in saline, while a modest decline in the intact radioconjugate fraction was observed in serum at later time points, supporting the suitability of the radioconjugate for delayed imaging and dosimetric analysis. 17 Although a gradual decline in serum stability was observed at later time points, the residual intact fraction appeared to be sufficient to support lesion visualization, while potential degradation products were likely cleared more rapidly, thereby preserving the lesion-to-background contrast.
Imaging protocol and dosimetry
Patients received ∼3.5–3.8 GBq of 177Lu-DOTA-peptide via intravenous administration. Whole-body planar imaging in the anterior and posterior projections was performed at 2 and 24 h after injection to assess biodistribution. The selected time points were chosen to balance early-phase biodistribution assessment with delayed imaging for improved lesion-to-background contrast, reflecting a trade-off between tracer kinetics and clinical interpretability. Thoracic SPECT/CT imaging was performed using a hybrid system for lesion localization and semiquantitative analysis. Image reconstruction incorporated attenuation correction using low-dose CT data and scatter correction using vendor-specific energy window-based methods, enabling improved quantitative accuracy of regional uptake measurements. Specifically, image reconstruction was performed using an ordered-subsets expectation maximization (OSEM) algorithm with 2–3 iterations and 8–10 subsets, incorporating resolution recovery and postreconstruction Gaussian filtering to improve signal-to-noise characteristics. Regions of interest were drawn for the pulmonary lesions, normal lung parenchyma, mediastinal background, blood pool, kidneys, and liver. Time–activity data derived from serial imaging were used to generate organ- and lesion-specific activity curves for each patient.
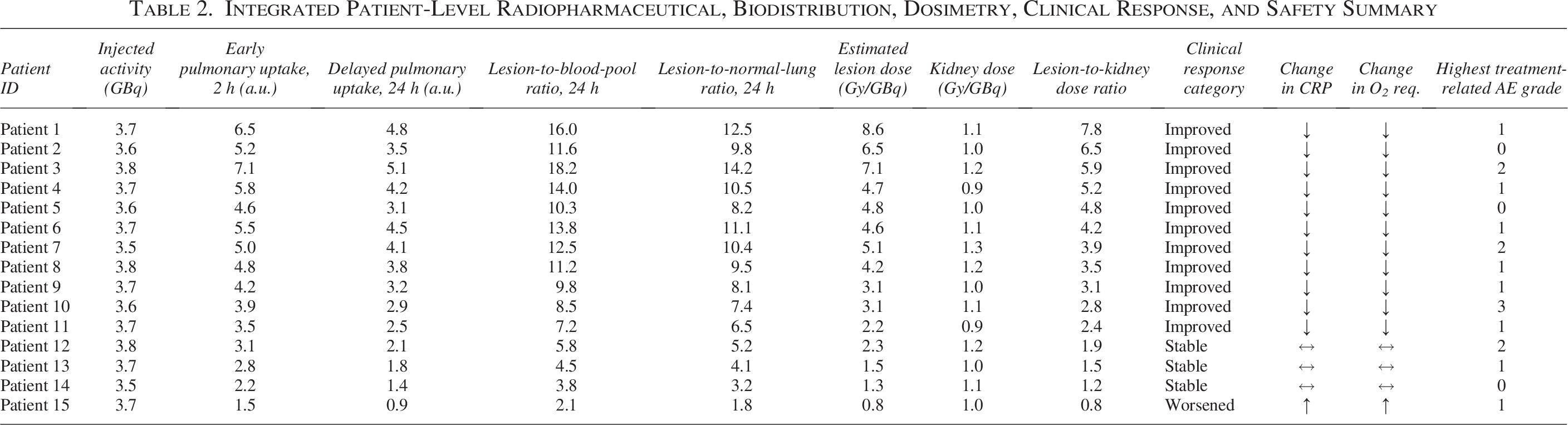
Patient-specific dosimetry was estimated by fitting the time–activity curves and integrating the area under the curve according to the standard internal dosimetry methodology. 18 Time–activity curves were fitted using a monoexponential decay model based on serial imaging time points, and numerical integration was performed to estimate the cumulated activity for each region of interest. The monoexponential model was selected as a pragmatic approximation, given the limited number of imaging time points, balancing model stability and physiological interpretability in a clinical feasibility setting. This approach is consistent with the established clinical dosimetry workflows for radionuclide imaging. The absorbed doses to the pulmonary lesions and major organs at risk were calculated using OLINDA/EXM and expressed in Gy/GBq.17,18 The lesion-to-organ dose ratios were subsequently derived. A lesion-to-kidney absorbed dose ratio >1.0 was predefined as a planning threshold to identify patients with favorable lesion targeting for radiopharmaceutical-guided therapeutic consideration. For consistency with subsequent patient-level stratification and visualization, a secondary threshold of >2.0 was evaluated to identify patients with more pronounced dosimetric selectivity. This threshold was selected as a pragmatic indicator reflecting preferential lesion targeting relative to a critical organ at risk, consistent with general dosimetric principles in radionuclide therapy, where higher target-to-organ dose ratios are associated with an improved therapeutic index. Given the exploratory nature of this study, the threshold should be interpreted as a feasibility-oriented parameter rather than a validated clinical cutoff. The patient-level injected activity, pulmonary uptake, lesion-to-background ratios, lesion absorbed dose, kidney absorbed dose, and lesion-to-kidney dose ratios are summarized in Table 2.
Integrated Patient-Level Radiopharmaceutical, Biodistribution, Dosimetry, Clinical Response, and Safety Summary
Clinical response and safety assessment
Clinical and laboratory parameters were recorded at baseline and again at follow-up 2–4 weeks after radiopharmaceutical administration. The evaluated parameters included C-reactive protein, procalcitonin, and oxygen requirements. Clinical outcomes were categorized as improved, stable, or worsened based on a composite assessment integrating clinical status and radiographical findings (Table 2). The composite assessment incorporated predefined directional changes in key parameters, including reductions in C-reactive protein, procalcitonin, and oxygen requirement, together with an imaging-based evaluation of the pulmonary lesion burden. Classification requires concordant trends across these domains to minimize subjective interpretation. This approach was designed to minimize subjective bias by requiring agreement between biochemical, clinical, and imaging indicators, rather than relying on a single parameter. Safety evaluation included serial hematological and biochemical testing, including complete blood count, serum creatinine, blood urea nitrogen, aspartate aminotransferase, and alanine aminotransferase levels. Adverse events were graded according to the Common Terminology Criteria for Adverse Events version 5.0. 19
Statistical analysis
Continuous variables are presented as mean ± standard deviations. Paired comparisons between baseline and follow-up clinical markers were performed using a paired t test. The normality of the paired differences was assessed using the Shapiro–Wilk test prior to applying parametric methods. In cases where normality assumptions were not strictly met, the results were interpreted with caution, given the exploratory nature of the study and the limited sample size. Categorical variables are presented as frequencies and proportions of the variables. A two-sided p-value < 0.05 was considered statistically significant. Statistical analyses were performed using GraphPad Prism and R software. No formal power calculation was performed owing to the exploratory and feasibility-oriented design of the study, and the sample size was selected to provide initial translational insights rather than definitive statistical inference.
Results
Radiopharmaceutical design and radiochemical characterization
The DOTA-functionalized antimicrobial peptide was successfully radiolabeled with 177Lu at high efficiency. The overall radiopharmaceutical design and preparation workflow is summarized in Fig. 1A. Radio-high-performance liquid chromatography demonstrated clear separation between free 177Lu and the radiolabeled peptide, with a single dominant product peak and radiochemical purity of 98.5% (Fig. 1B). In vitro stability studies demonstrated excellent stability in saline and acceptable stability in human serum over 24 h, with saline retaining >95% of the intact radioconjugate at 24 h and serum showing a progressive decline in the radiolabeled fraction during incubation (Fig. 1C). The radiolabeling efficiency was dependent on the reaction temperature, and optimum values were 60°C, where the labeling efficiency was >95% (Fig. 1D). Collectively, these data attest to the effective production of a radionuclide-tagged 177Lu-labeled and relatively stable 177Lu-labeled antimicrobial peptide that can be used in the future as a precursor for in vivo imaging and dosimetric studies.
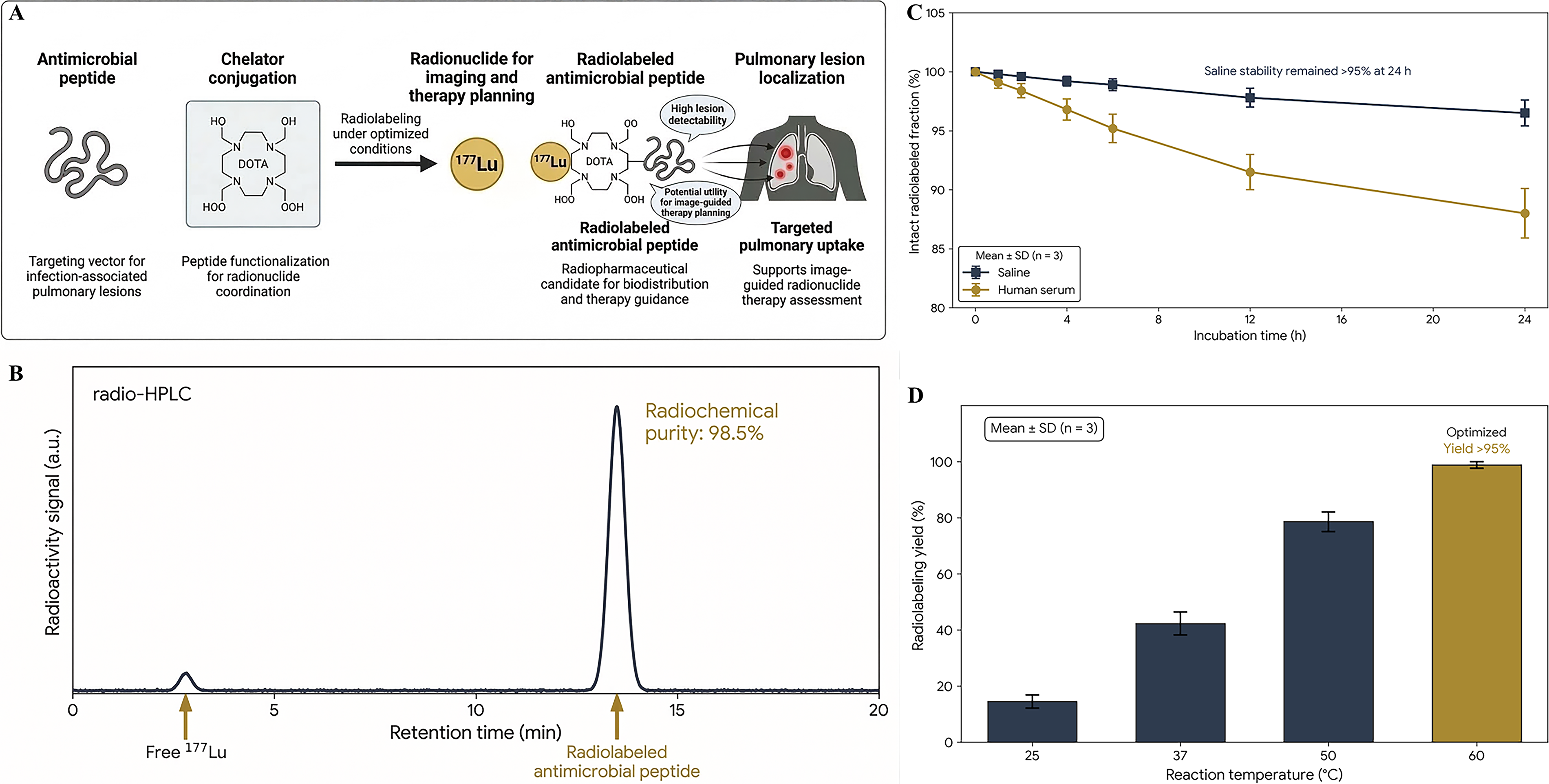
Radiopharmaceutical design, radiochemical characterization, in vitro stability, and labeling efficiency of the radiolabeled antimicrobial peptide.
Clinical biodistribution imaging and pulmonary lesion localization
Planar imaging of the entire body 2 h posttracer transmission showed systemic biodistribution of the radiopharmaceutical with high physiological uptake in the kidneys and focal uptake in the pulmonary regions of known radiological lesions (Fig. 2A). Background activity was reduced at 24 h, and lesion-related uptake in the lung lesion was still observed, which led to better conspicuity of lesions in delayed imaging (Fig. 2B). Accuracy in localizing tracer accumulation within CT-defined lung infiltrates in thoracic SPECT/CT was achieved. An example of interpatient data variability is the representative fused images that demonstrated a case with a high focal pulmonary uptake (Fig. 2C) and moderate pulmonary uptake (Fig. 2D), illustrating the interpatient variability in lesion avidity. Quantitative analysis was performed using the lesion, normal lung, and background regions of interest defined on the fused images (Fig. 2E). Overall, these imaging findings demonstrated persistent and detectable pulmonary lesion uptake of radiolabeled antimicrobial peptides in this patient population. At early time points, the lesion-to-background contrast was limited owing to circulating tracer activity, indicating that early imaging primarily reflects biodistribution rather than optimal lesion delineation. Delayed imaging provides improved contrast and is, therefore, more suitable for clinical interpretation.
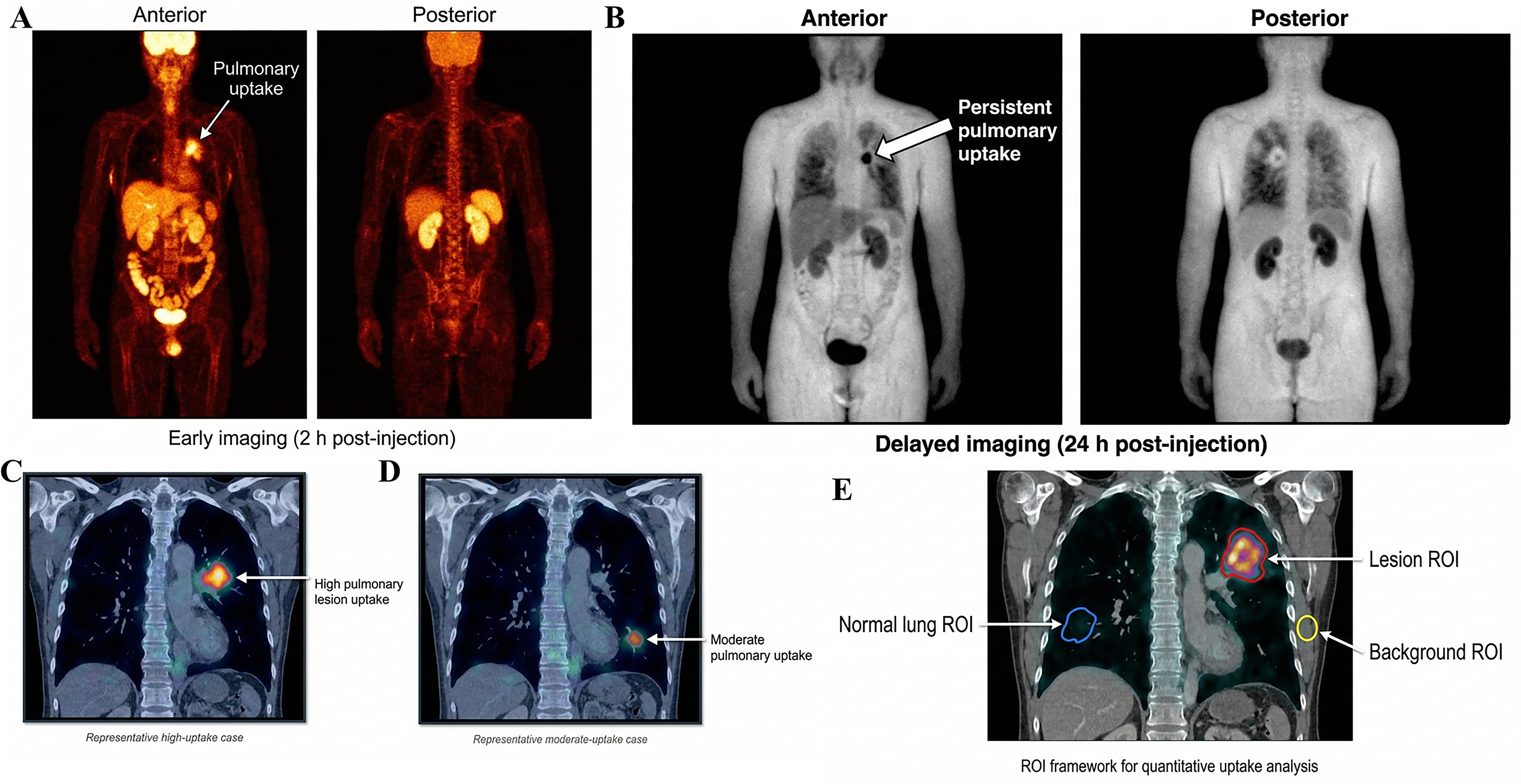
Representative clinical imaging of biodistribution and pulmonary lesion localization of the radiolabeled antimicrobial peptide.
Quantitative biodistribution and pulmonary lesion targeting
Serial region-of-interest analysis demonstrated rapid clearance of the tracer from the blood pool and a progressive decline in activity in nontarget tissues. Early uptake was observed in the kidneys and liver, whereas the pulmonary lesions showed sustained retention over the imaging interval (Fig. 3A, B). In the imaging subgroup (n = 5), the mean relative pulmonary lesion uptake remained elevated across serial time points, increasing from ∼.5 a.u. at 2 h to 5.2 a.u. at 4 h, followed by a gradual decline to 4.8 a.u. at 12 h and 3.9 a.u. at 24 h (Fig. 3B). Lesion contrast improved over time, as reflected by progressive increases in the lesion-to-blood-pool and lesion-to-normal-lung uptake ratios (Fig. 3C). Specifically, the lesion-to-blood-pool ratio increased from 1.3 at 2 h to 4.9 at 24 h, and the lesion-to-normal-lung ratio increased from 3.7 to 7.8 over the same interval. Patient-level heterogeneity in tracer distribution and lesion contrast was further illustrated by the uptake heatmap, which showed variable combinations of lesion uptake and background organ activity across individuals (Fig. 3D). Given the limited sample size of the imaging subgroup, formal statistical measures of variability, such as confidence intervals, were not calculated, and the analysis remained primarily descriptive. Together, these findings indicate favorable pulmonary lesion targeting with progressive improvement in lesion conspicuity during follow-up. The observed uptake pattern reflected an initial accumulation phase followed by a gradual washout rather than absolute sustained retention. This kinetic behavior is consistent with target-specific binding combined with progressive systemic clearance, resulting in relative retention within the lesions compared to the declining background activity.
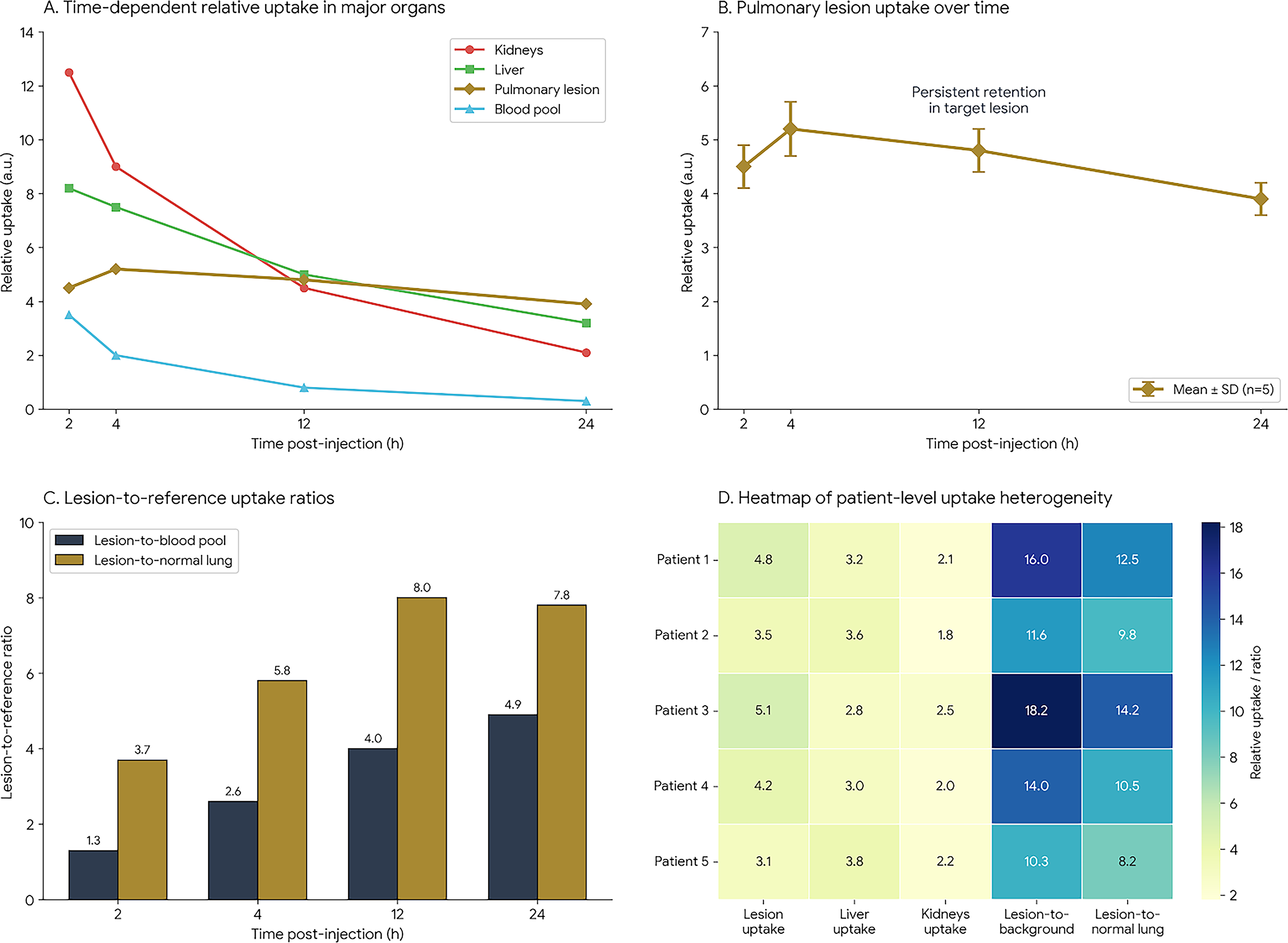
Quantitative biodistribution and pulmonary lesion targeting profile of the radiolabeled antimicrobial peptide.
Patient-specific dosimetry and treatment-planning relevance
Time–activity curve analysis demonstrated high early activity in the kidneys, consistent with renal clearance, and sustained activity in pulmonary lesions over the imaging interval (Fig. 4A, B). Dosimetric analysis showed that pulmonary lesions received the highest estimated absorbed dose, ∼4.5 Gy/GBq, compared with 1.2 Gy/GBq for the kidneys, 0.8 Gy/GBq for the liver, 0.2 Gy/GBq for the normal lung, and 0.1 Gy/GBq for the blood (Fig. 4C). Correspondingly, the lesion-to-kidney, lesion-to-liver, and lesion-to-lung dose ratios were 3.8, 5.6, and 22.5, respectively (Fig. 4D), demonstrating marked dosimetric selectivity for pulmonary lesions compared to nontarget tissues. At the individual patient level, 11 of 15 dosimetry-evaluable patients exceeded the predefined planning threshold of a lesion-to-kidney absorbed dose ratio of >2.0 (Fig. 4E). This higher threshold was used to identify patients with more pronounced dosimetric selectivity and should be interpreted as an exploratory stratification parameter, rather than a validated clinical cutoff. Taken together, these findings support the feasibility of patient-specific imaging-based dosimetric stratification and indicate favorable lesion targeting in most patients. Given the observed renal uptake and absorbed dose, kidney exposure represents an important consideration consistent with the known biodistribution patterns of peptide-based radiopharmaceuticals, and careful monitoring of renal function remains warranted in future studies.
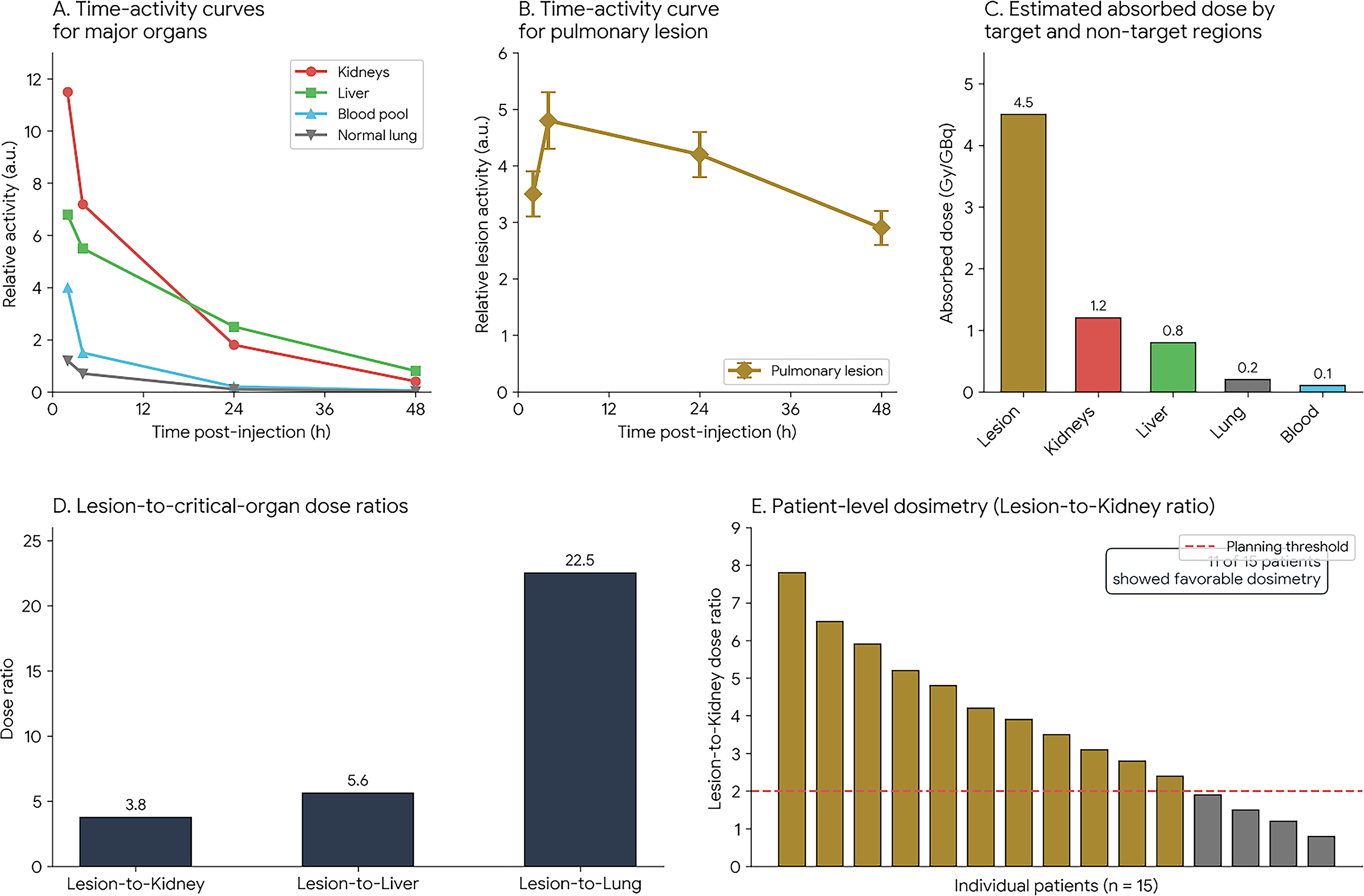
Patient-specific dosimetry and image-guided radionuclide therapy planning based on biodistribution analysis.
Clinical response and treatment-associated changes
Representative follow-up imaging demonstrated a marked reduction in pulmonary lesion-associated tracer uptake relative to baseline, consistent with interval lesion improvement (Fig. 5A). Paired analysis of selected inflammatory and clinical parameters showed consistent decreases in C-reactive protein, procalcitonin, and oxygen requirements at follow-up, supporting an overall trend toward clinical improvement (Fig. 5B). At the cohort level, 35 of 50 patients (70%) were classified as improved, 10 (20%) remained stable, and 5 (10%) worsened at follow-up (Fig. 5C). Together, these findings suggest a favorable short-term clinical evolution in most patients following radiopharmaceutical-guided management. However, these clinical outcomes should be interpreted in the context of concurrent antimicrobial therapy and supportive care, and the observed improvements cannot be attributed solely to radiopharmaceutical intervention.
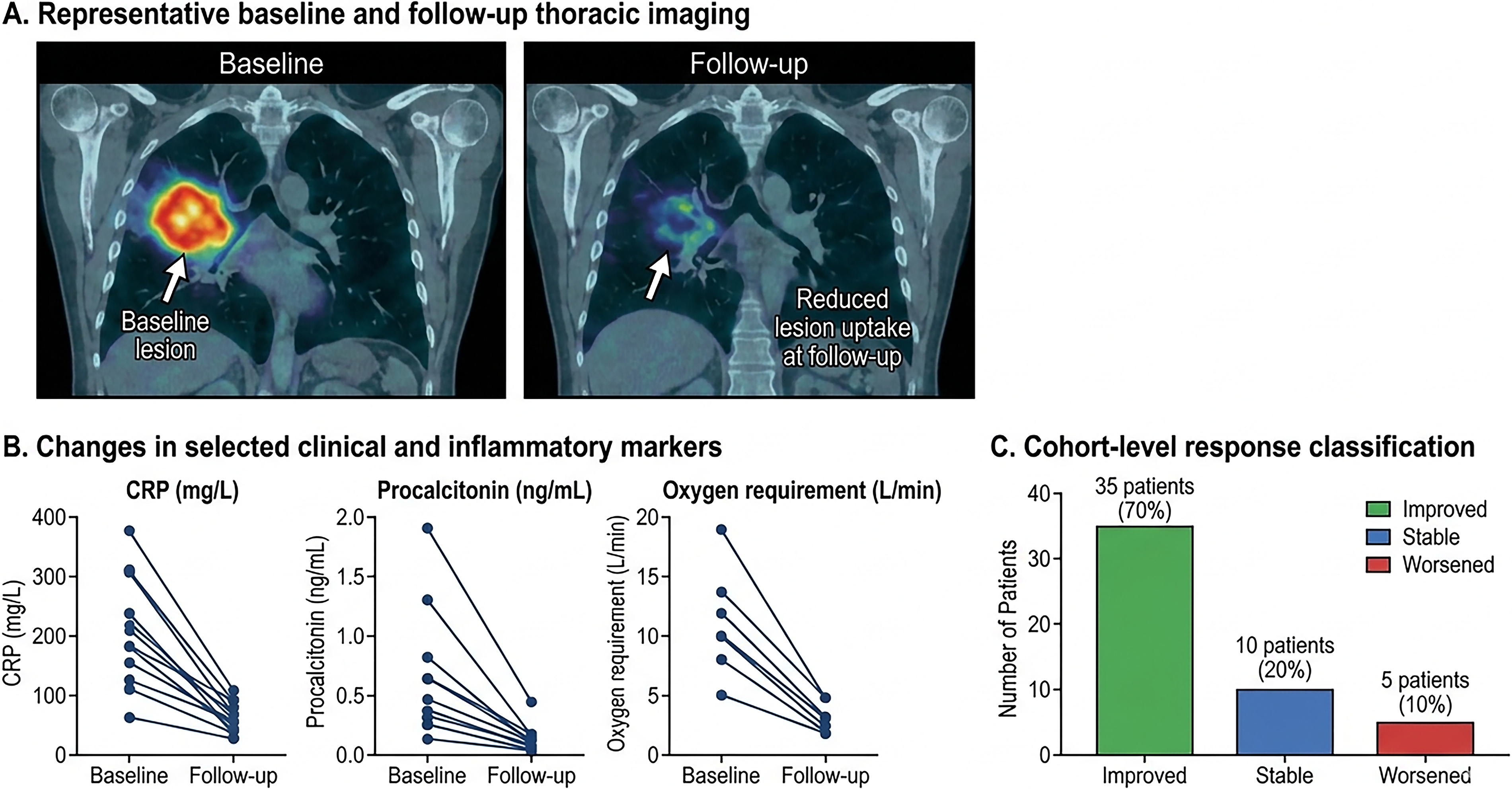
Clinical response and treatment-associated changes following precision radiopharmaceutical-guided radionuclide therapy.
Safety and translational assessment
Paired hematological assessments showed that hemoglobin, white blood cell count, and platelet count were generally maintained between baseline and follow-up, without evidence of major overall deterioration (Fig. 6A). Renal and hepatic biochemical indices, including creatinine, blood urea nitrogen, aspartate aminotransferase, and alanine aminotransferase levels, also showed no marked overall worsening during the observation period (Fig. 6B). No grade 4 adverse events were observed, and treatment-associated toxicities were predominantly grades 1–2 (Fig. 6C). The safety assessment in this study was limited to short-term follow-up, and delayed or cumulative toxicity associated with radionuclide exposure was not evaluated systematically. Longer-term monitoring is required in future studies to fully characterize the late safety profiles. Integrated benefit-risk assessment showed that most patients clustered within the quadrant characterized by favorable dosimetry and clinical improvement, supporting an overall favorable translational profile for this radiopharmaceutical approach (Fig. 6D, Table 2).
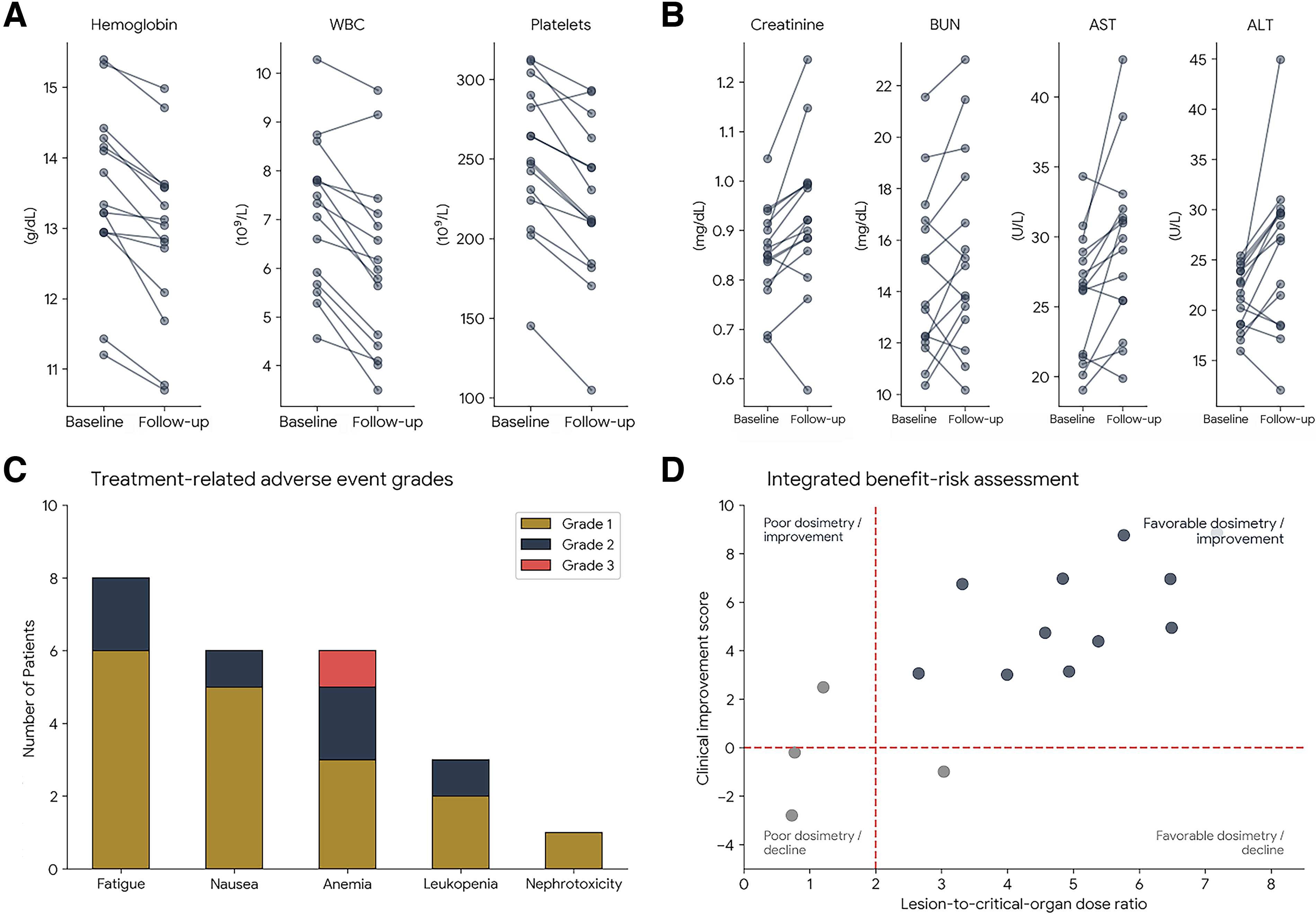
Safety profile and translational assessment of precision radiopharmaceutical-guided radionuclide therapy.
Discussion
The present study demonstrates that a DOTA-functionalized antimicrobial peptide labeled with 177Lu can be prepared with high radiochemical purity and adequate in vitro stability while maintaining favorable in vivo lesion localization characteristics in immunocompromised patients with cancer and severe pneumonia. From a radiopharmaceutical perspective, these findings are important because peptide-based targeting vectors offer rapid tissue penetration, relatively straightforward radiolabeling workflows, and the potential to integrate diagnostic imaging with individualized dosimetric assessments. In the current study, pulmonary lesions demonstrated an initial uptake phase followed by a gradual washout, with relative retention compared to background tissues, contributing to improved delayed lesion contrast and supporting the suitability of this platform for lesion-focused imaging and follow-up evaluation.20,21 This behavior is consistent with the broader theranostic principle that target retention combined with declining nontarget activity can improve the clinical usefulness of radiopharmaceutical-guided decision-making.
A major strength of this study is the incorporation of patient-specific dosimetry into the evaluation framework. The dosimetric results showed that pulmonary lesions received the highest estimated absorbed dose relative to major nontarget tissues, and most dosimetry-evaluable patients exceeded the predefined lesion-to-kidney planning thresholds. This is highly relevant to modern radionuclide therapy, which increasingly depends on individualized biodistribution and dose estimation rather than fixed empirical activity administration. Therefore, the findings support the concept that infection-associated pulmonary lesions in immunocompromised oncologic patients can be characterized not only qualitatively by imaging but also quantitatively through lesion-to-organ dose relationships that may inform radiopharmaceutical-guided treatment stratification. In this regard, the study extends the role of antimicrobial peptide imaging beyond lesion detection toward a more integrated theranostic and planning-oriented model.22,23
Clinical and translational findings also warrant attention. Most patients showed favorable short-term clinical evolution, accompanied by decreases in inflammatory markers and oxygen requirements, while the safety profile remained acceptable, with no grade 4 toxicities and predominantly grade 1–2 adverse events. These observations suggest that the radiopharmaceutical platform is clinically feasible and well tolerated in high-risk populations. Nevertheless, the study should be interpreted in light of several limitations, including the single-arm design, modest imaging and dosimetry subgroup sizes, and the challenge of attributing clinical improvement solely to radiopharmaceutical-guided intervention in patients receiving complex, multidisciplinary care. Accordingly, the present data should be viewed as evidence of translational feasibility, biodistribution selectivity, and clinical promise, rather than as definitive proof of therapeutic efficacy. Future studies should include larger prospective cohorts, standardized paired radionuclide planning workflows, and direct comparisons with conventional infection imaging and management strategies to better define the role of this platform in precision oncology and radionuclide therapy pathways.24,25 Additionally, the absence of formal power calculation and confidence interval estimation limits the statistical generalizability of the findings, reinforcing the exploratory nature of this study. In addition, future investigations should explore the correlations between imaging uptake patterns, clinical outcomes, and underlying pathogen characteristics to better understand the interpatient variability in tracer behavior. Potential contributors to interpatient variability may include differences in renal function affecting tracer clearance, prior oncologic treatments influencing the tissue microenvironment, and demographic factors such as age and baseline disease severity.
Conclusions
177Lu-labeled antimicrobial peptide imaging showed high radiochemical quality, persistent pulmonary lesion targeting, favorable lesion-to-organ dosimetric selectivity, and an acceptable short-term safety profile in immunocompromised cancer patients with severe pneumonia. The integration of radiopharmaceutical design, SPECT/CT-based lesion localization, patient-specific dosimetry, and clinically relevant follow-up supports the translational value of this approach as a theranostic platform for radiopharmaceutical-guided precision therapy. Although larger controlled studies are required to confirm the therapeutic utility and define its place in clinical practice, the present findings provide a strong rationale for further development of peptide-based radionuclide strategies in oncology patients with infection-related pulmonary complications.
Authors’ Contributions
X.N.: Conceptualization, methodology, investigation, data curation, formal analysis, and writing—original draft. X.Y.: Software, validation, visualization, data curation, and writing—review and editing. J.J.: Conceptualization, supervision, project administration, and writing—review and editing.
Footnotes
Disclosure Statement
The authors declare that they have no conflicts of interest related to this research.
Funding Information
There is no funding involved in this study.