
Abstract
Keywords
ADHD is a common neurodevelopmental disorder that causes functional impairment in many different domains of life and leads to substantial suffering. The core symptoms of ADHD are age-inappropriate problems with inattention and hyperactive/impulsive behavior, in combination or separately. ADHD typically first appears in early childhood and by early adolescence and frequently co-occurs with other psychiatric disorders such as conduct disorder and substance use disorders (SUD). The presence of these co-occurring disorders, along with ADHD, clearly contributes to the risk for developing delinquent behavior. In a majority of cases, ADHD remains symptomatic into adulthood often combined with additional psychiatric disorders, such as personality disorders, SUD, as well as socioeconomic problems (Kessler et al., 2006; Kooij et al., 2010; Murphy & Barkley, 1996). A recent study by Gudjonsson et al. (2011) suggests that these disorders may serve as an important mediator between ADHD and criminal offending.
In the past decade, interest in the manifestations of ADHD in criminal offenders has been growing. Studies have shown a significantly earlier onset in criminality and a higher rate of recidivism in offenders with ADHD (Young et al., 2009, 2011).
In population-based studies, the estimated prevalence rates of adult ADHD, based on the Diagnostic and Statistical Manual of Mental Disorders (4th ed., DSM-IV; American Psychiatric Association [APA], 1994) range from 1% to 7.3% with a pooled prevalence of 2.5% (95% confidence interval = [2.1, 3.1]; Simon et al., 2009). Several studies suggest a substantially higher prevalence of childhood and adult ADHD in incarcerated males (Eyestone & Howell, 1994; Rasmussen, Almvik, & Levander, 2001; Rosler et al., 2004; Young, 2009), compared with the general population (14%-45% vs. 4.4%; Kessler et al., 2006), as could be expected given the well-established link between ADHD and various types of antisocial behavior (Moffitt, 1990).
Most prior studies have reported on males with ADHD, and much less is known about the prevalence and correlates of ADHD in females, especially in forensic and prison populations. In a recent German study of 110 adult female offenders, with a mean age of 34 years, the prevalence of ADHD was estimated to be 10% (Rosler, Retz, Yaqoobi, Burg, & Retz-Junginger, 2009), largely consistent with the prevalence of 14.3% reported previously by Gunter et al. (2008). The childhood prevalence of ADHD in incarcerated women was estimated to be 45.8% using the Utah criteria (Wender, Wolf, & Wasserstein, 2001) that include problems with temperament and affective lability (Hennessey, Stein, Rosengard, Rose, & Clarke, 2010).
Thus, reported prevalence rates of adult ADHD in incarcerated women have been comparable to those in men, but the studies have been few, and a better understanding of ADHD in female offenders is required.
In the present study, we used the adult ADHD Self-Rating Scale (ASRS; Kessler et al., 2005) as a screening instrument. The ASRS was developed for the World Health Organization (WHO) and consists of 18 items based on the diagnostic criteria for ADHD in DSM-IV (APA, 1994). A short 6-item version of ASRS predicts the diagnosis of ADHD in the general population with a sensitivity of 68.7%, a specificity of 99.5%, and a total classification accuracy of 97.9%. Hitherto, no prior study has explored the validity of the ASRS screener in prison populations.
The aim of the present study was to examine the prevalence of ADHD in incarcerated women in Sweden. In addition, the study aimed to investigate the prevalence of substance use and other psychiatric disorders in this population, in conjunction with ADHD. This is important because high rates of comorbidity between ADHD and these psychiatric disorders have been strongly suggested (Biederman, 2005; Wilens, 2004). Furthermore, we aimed to investigate the usefulness and validity of the ASRS as a screening instrument in this population.
Method
Participants
At the time of the study, October 2008, a total of 264 women were registered in a database as serving a prison sentence in Swedish prisons (see flowchart in Figure 1.). Of these, 184 (69%) were physically present and eligible to participate. Those serving the last part of their prison sentence in a treatment home or for other related reasons not physically present at the time of the screening were not included in the sample.
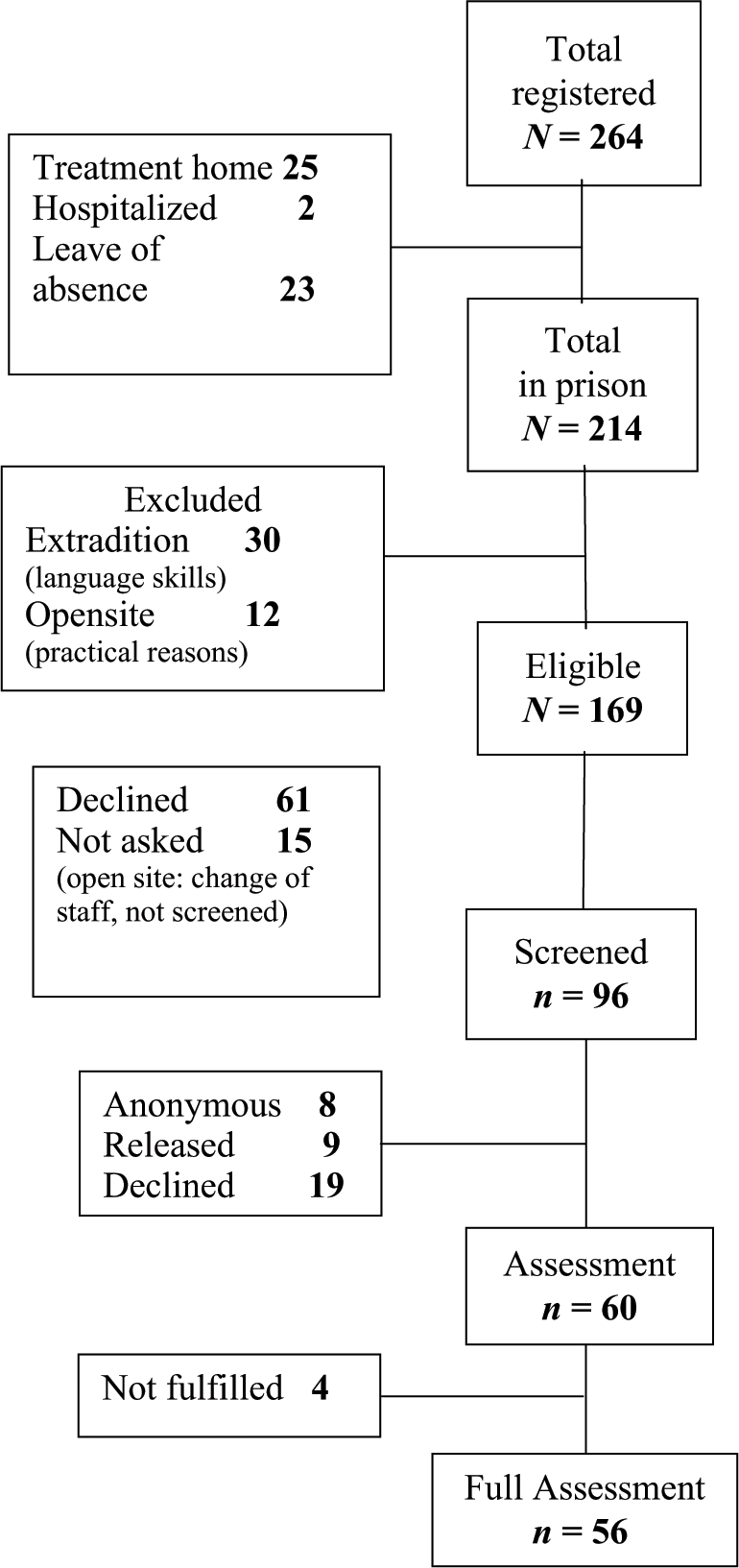
Flowchart of recruitment in the study.
Due to deficient skills in Swedish language, women who were to be extradited (n = 30) were excluded from the sample. An open site (n = 15) was excluded for practical reasons. The remaining 169 prisoners were invited to participate in the study, and 96 (57%) agreed to take part in the screening phase. Of these 96 screenings, 8 women were anonymous, 9 women were released before they could be interviewed, and 19 declined further participation for various reasons (e.g., feeling down, on leave, not interested). In the end, 60 women were included in the assessment phase, and 56 completed the full assessment.
There were no significant differences in the demographics including age, employment status, marital status, and housing (see Table 1) between women who participated only in the screening and those who also participated in the assessment phase. The participation was voluntary, and the participants did not receive any compensation.
Demographics, Preferred Substance of Use, Prevalence of Substance Use Problems and Psychiatric Disorders, IQ, and Their Covariance With ADHD.
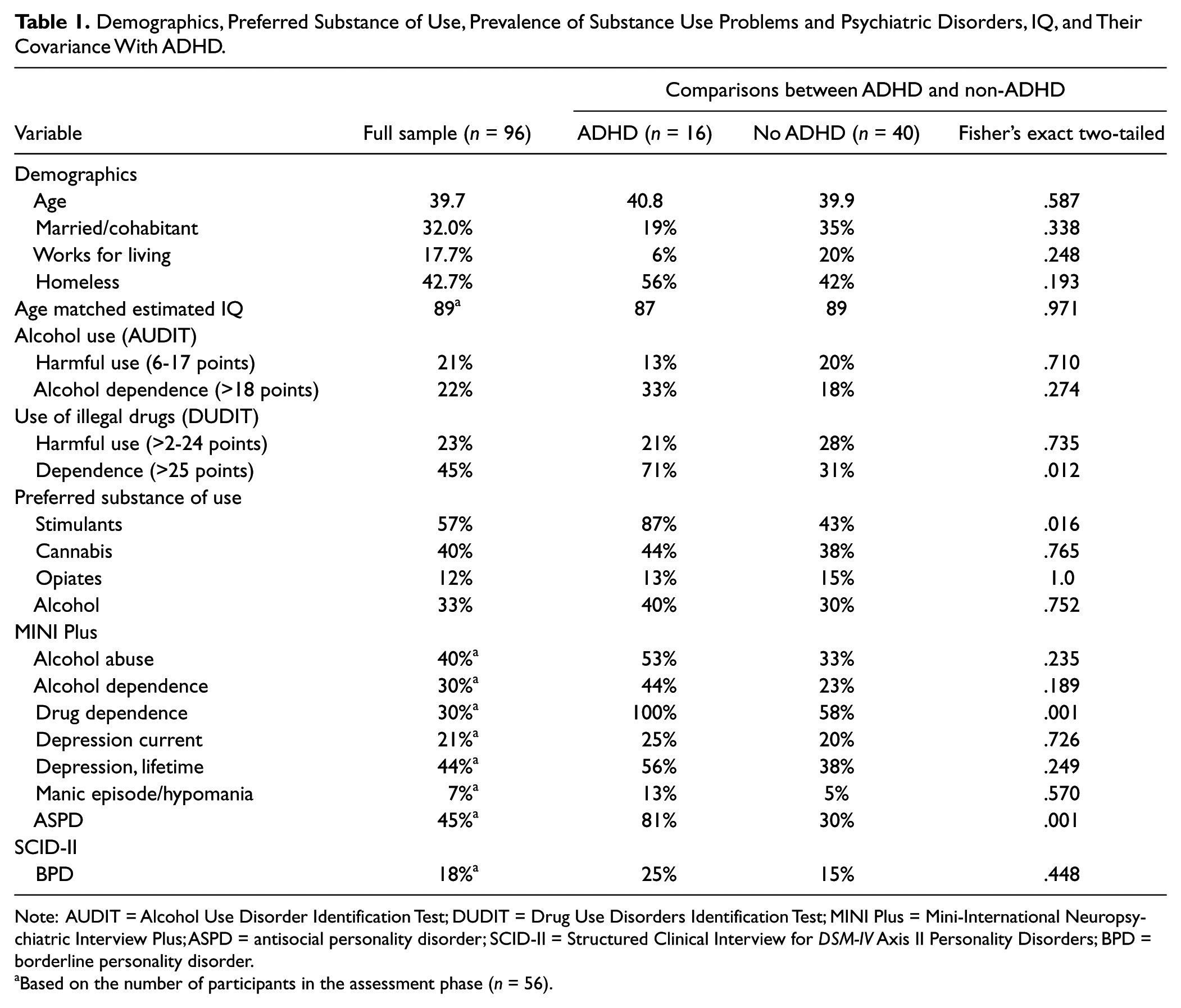
Note: AUDIT = Alcohol Use Disorder Identification Test; DUDIT = Drug Use Disorders Identification Test; MINI Plus = Mini-International Neuropsychiatric Interview Plus; ASPD = antisocial personality disorder; SCID-II = Structured Clinical Interview for DSM-IV Axis II Personality Disorders; BPD = borderline personality disorder.
Based on the number of participants in the assessment phase (n = 56).
Design and Procedure
This cross-sectional study included two parts: a screening phase and an assessment phase. The screening phase included self-report questionnaires to measure ADHD symptoms, substance use, and demographic data. The interview phase assessed current and childhood ADHD symptoms and co-occurring psychiatric disorders.
The project staff visited five of the six Swedish prisons for women to inform and coach the staff in managing the screening phase. All eligible women were asked by the prison staff to participate and fill in the screening instruments. Exclusion criteria consisted of insufficient language skills or repatriation after served sentence. All participants signed an informed consent and were asked whether they agreed to be contacted for the interview. The participants were then to enclose the screening questionnaires in an envelope and seal the envelope. The interviews were performed by qualified professionals: either licensed clinical psychologists or psychologist in the last phase of their internship, employed at the regional addiction clinic, and experienced in the assessment of ADHD in individuals with SUD. The interviewers received the recommended training to administer the interview used at the assessment phase (Epstein & Kollins, 2006). In addition, to attain an interrater agreement, the interviewers met on several occasions in the course of the study to discuss diagnostic issues. The interviews were conducted within a 2-month period following the screening.
Screening phase
ADHD symptoms were assessed using the Swedish version of the 18-item ASRS questionnaire (Kessler et al., 2005). Each item assesses how often a symptom occurred during the past 6 months on a 0 to 4 scale with responses of never (0), seldom/rarely (1), sometimes (2), often (3), and very often (4). In line with DSM-IV, 9 of the items in the ASRS reflect inattention symptoms and 9 items reflect symptoms of hyperactivity-impulsivity. If the sum score for one of the two scales is <17, then ADHD is unlikely, and a score ≥24 indicates highly probable ADHD. The 6-item screener of ASRS includes 4 items of inattention and 2 items of hyperactivity/impulsivity. A patient screens positive for ADHD if he or she answers four or more of the questions within predesignated ranges: “sometimes” to “very often” on the first 3 items and “often” to “very often” on the next 3 items.
Alcohol consumption was measured using the Swedish version of the Alcohol Use Disorder Identification Test (AUDIT; Bergman & Kallmen, 2002; Saunders, Aasland, Babor, de la Fuente, & Grant, 1993). AUDIT is designed to evaluate risky levels of alcohol use using items that assess frequency, degree of consumption (measured as glasses of alcohol), and risky behavior. The instrument consists of 10 items about alcohol consumption, symptoms of addiction, and harmful consumption (range = 0-40). For women, a total AUDIT scale score ≥18 indicates likelihood of dependence, whereas a score >6 indicates harmful consumption.
Drug use was measured using the Drug Use Disorders Identification Test (DUDIT; Berman, Bergman, Palmstierna, & Schlyter, 2005), which is an 11-item questionnaire designed to assess consumption patterns of illicit drugs and problems related to drug use (range = 0-44). For women, a total score >25 indicates SUD/substance use dependency, whereas a score >2 indicates drug-related problems. The DUDIT >25 cutoff has found to show a 90% sensitivity for a DSM-IV and for an International Classification of Diseases-10 (ICD-10) diagnosis of SUD (of illicit substances). The participants were asked to rate their consumption in AUDIT and DUDIT during the 12-month period prior to incarceration.
The participants also filled out a short questionnaire on demographics, prior diagnoses and/or treatment with ADHD, substance use, and the preferred substance (alcohol, stimulants, opiates, and cannabis).
Assessment phase
Conners’ Adult ADHD Diagnostic Interview for DSM-IV (CAADID; Epstein & Kollins, 2006), a semistructured interview, was used as the gold standard. The CAADID interview is divided into two parts. In Part I, information on demographic history, developmental course, ADHD risk factors, and psychopathology are collected. Part I is usually filled out by the participant but can be used as an interview, as was the case in this study. Part II of the interview is administered by a trained clinician and designed to evaluate the first four DSM-IV ADHD criteria: present ADHD symptoms (Criterion A), age of onset of the ADHD symptoms (Criterion B), pervasiveness of the symptoms (Criterion C), and impairment caused by the symptoms during childhood and adulthood (Criterion D). For each symptom, the interview contains examples of typical behavior associated with that symptom in adulthood and in childhood. The interviewer rates whether each symptom is present or absent.
The Mini-International Neuropsychiatric Interview (MINI) Plus psychiatric interview (Sheehan et al., 1998) was used to assess prior or current episodes of mood disorders (current and lifetime depression, manic episode/hypomania), SUD, and antisocial personality disorder (ASPD), whereas the Semi-Structured Clinical Interview for DSM-IV Axis II Personality Disorders (SCID-II; First, Gibbon, Spitzer, Williams, & Benjamin, 1997) was used to assess borderline personality disorder (BPD). As the women had been incarcerated for varying length of time, substance use in lifetime is reported instead of current use.
To explore whether inattention symptoms were associated with severe learning difficulties instead of ADHD per se, we also included assessments of IQ based on two tests (Vocabulary and Block Design) from Wechsler Adult Intelligence Scale–III (WAIS-III; Ringe, Saine, Lacritz, Hynan, & Munro Cullum, 2002; Wechsler, 1997).
All statistical analyses were performed with SPSS v. 17 and 18. Analyses used were chi-square and Fisher’s exact tests. For all analyses, p > .05 was regarded as statistically significant.
Results
ADHD Prevalence
Fifty-one percent of the total sample (M = 38 years) screened positive for ADHD according to the ASRS 6-item screener. Using the full 18-item version of the ASRS, 45% of the women fulfilled criteria for “highly probable ADHD”; that is, having a score ≥24 in either the inattentive or the hyperactive-impulsive symptom dimension. A majority (53%) of those with “highly probable ADHD” showed elevated scores in both symptom dimensions, whereas 35% showed high scores only in the inattentive dimension and 12% only in the hyperactive-impulsive dimension.
Of the 56 women (M = 39 years) who participated in the assessment phase, 16 (29%) fulfilled DSM-IV criteria for persistent ADHD in the CAADID interview (see Table 2). Of these16 women, 11 met criteria for the combined subtype of ADHD (69%), 3 met criteria for the primarily inattentive subtype (19%), 1 (6%) met criteria for the primarily hyperactive-impulsive subtype, and 1 met criteria for the combined subtype but had later symptom onset (at 10). One additional person fulfilled the criteria for childhood ADHD but not for adult ADHD (four of the nine symptoms of attention problems).
ADHD Prevalence at Screening (Self-Rated Symptoms in ASRS) and After Full Assessment (CAADID Interview) for Total Screened Sample and Those Interviewed.
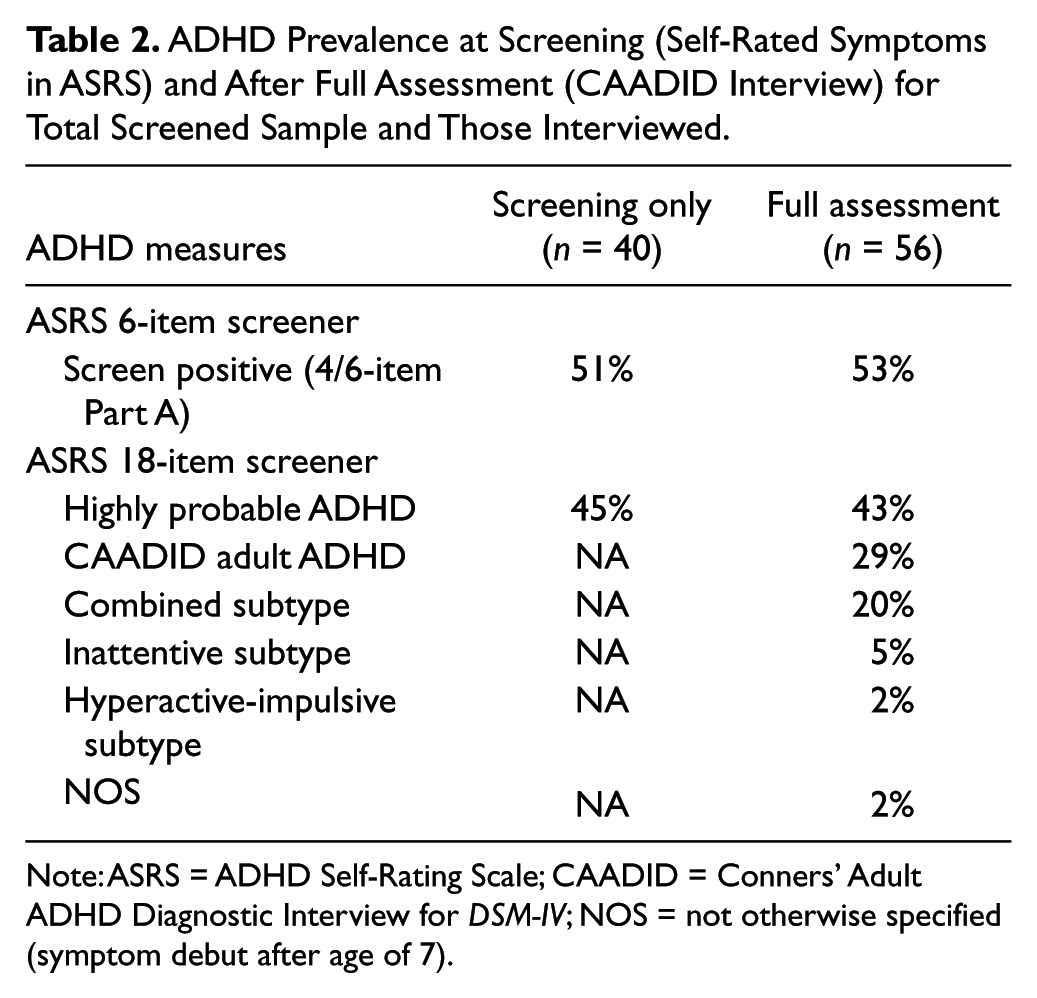
Note: ASRS = ADHD Self-Rating Scale; CAADID = Conners’ Adult ADHD Diagnostic Interview for DSM-IV; NOS = not otherwise specified (symptom debut after age of 7).
SUD and Other Psychiatric Disorders
The first column of Table 1 shows the prevalence of substance use problems and psychiatric disorders in the full-screening sample. As can be seen, 43% of the women reported harmful use of alcohol (21%) or alcohol dependence (22%) according to the AUDIT scale and 68% showed harmful use of narcotics (23%) and drug dependence (45%) according to the DUDIT scale. In total, 79% of the 96 women had scores indicating SUD on the AUDIT (i.e., >18 points) or the DUDIT (i.e., >25 points) and 58% had results indicating either dependence of alcohol or narcotics. Co-occurring alcohol use disorder and drug use disorder were found in 12% of the women (data not shown). According to the MINI Plus psychiatric interview, 40% of the participants in the assessment phase (n = 56) fulfilled criteria for alcohol dependence during lifetime, whereas the corresponding number for dependence of illegal drugs (stimulants and cannabis being the most frequently used illegal substances) was estimated as 30%.
A large number of the participants in the assessment phase fulfilled criteria for other psychiatric disorders. For example, a diagnosis of current depression was present in 21% of the women, whereas the prevalence of ASPD was estimated as 45%.
Table 1 compares the prevalence of substance use problems and psychiatric disorders in ADHD and non-ADHD cases. In particular, drug dependence was significantly more common in the ADHD cases (100%) compared with the non-ADHD cases (56%). All but one of the ADHD cases with co-occurring drug dependence showed preference for amphetamine. Significantly more women in the ADHD group (81%) met diagnostic criteria for ASPD compared with the non-ADHD group (30%). In general, women with ADHD showed higher rates of substance use problems and co-occurring psychiatric disorders compared with women without ADHD, but all these comparisons failed to reach the level of statistical significance possibly due to the small sample size. For example, manic episodes/hypomania was substantially more common among ADHD cases (13%) than in the non-ADHD group (5%); likewise, the BPD was more common among ADHD cases (25%) compared with non-ADHD cases (15%); however, these differences were not statistically significant.
Validity of the ASRS
The ASRS 6-item screener generated a sensitivity of 1.0, a specificity of 0.66, a positive predictive value (PPV) of 0.55, and a negative predictive value of 1.0.
The full 18-item ASRS generated a lower specificity (0.45) and a lower PPV (0.42) when the “highly probable ADHD” definition (i.e., having a score ≥24 in either the inattentive or the hyperactive-impulsive symptom dimension) was used.
Discussion
The estimated prevalence of adult ADHD was much higher (29%) in the present sample of incarcerated women compared with the estimated prevalence of 4.4% in general population. This is consistent with the results from prior cross-sectional studies of adult offenders (e.g., Gunter et al., 2008; Retz & Rosler, 2010) and of juvenile offenders a (Fazel, Doll, & Langstrom, 2008). Childhood prevalence of ADHD in the present study was similar to prevalence rate presented in the German study by Rosler et al. (2009; 30% vs. 24%, respectively). However, there is some discrepancy in the results concerning the prevalence of ADHD in adulthood, between the two studies. Rosler et al. (2009) found a 10% prevalence of persisting ADHD in female offenders at the (M) age of 34 years, a higher prevalence of 17.9% in young female offenders 19 to 25 years of age, and no cases of persisting ADHD in women above 40 years. In contrast, the present study found an ADHD prevalence of 29% in females aged 19 to 59 years (M = 39 years) and no significant difference in prevalence rates between the corresponding age groups; nine of the ADHD cases were 40 years or older (the oldest being 57 years). This discrepancy is intriguing as both studies used DSM-IV criteria and clinically structured (but different) interviews to assess ADHD. First, the use of different interview instruments can be a part of the explanation as the DSM-IV ADHD diagnostic criteria are based on childhood symptoms and need to be interpreted into adult behavior. Second, issues related to the differences in national criminal justice systems such as the type of offenses that lead to imprisonment is another possible explanation. However, apart from the age-related discrepancy discussed earlier, the results of the current study are in line with prior research.
A recent Swedish study (Edvinsson, Bingefors, Lindström, & Lewander, 2010) reported an ADHD prevalence of 50% based on self-ratings, corresponding closely to our finding (49%) using the ASRS 6-item screener. Screening based on self-rating typically yields higher prevalence rates compared with more thorough assessments using clinical interviews, a diagnostic procedure recommended by experts in the field (Mariani & Levin, 2007; Nutt et al., 2007; S. J. Young, Adamou, et al., 2011).
The ADHD combined type was the most common subtype in the current sample, a finding that has been reported in prior studies of female and male offenders (Ginsberg, Hirvikoski, & Lindefors, 2010; Rosler et al., 2004, 2009), by contrast to population-based studies that most often report higher rates of the primary inattentive type (Kessler et al., 2006).This finding concurs with earlier research linking impulsivity with SUD, ASPD, and criminality (Biederman, 2005; Disney, Elkins, McGue, & Iacono, 1999). Our results also support the well-established link between ADHD and SUD (Biederman et al., 1997; Carroll & Rounsaville, 1993; Wilens, Biederman, & Mick, 1998; Wilens, Biederman, Mick, Faraone, & Spencer, 1997). Significantly more women in ADHD group compared with non-ADHD group had results indicating dependence on illicit drugs (using MINI Plus).
In the present study, all but one of the women with ADHD met DSM-IV diagnostic criteria for DUD, this result is similar to observations in other studies on female offenders (Hennessey et al., 2010; Rosler et al., 2009). Interestingly, stimulant (mainly amphetamine) dependence was significantly more common in ADHD group compared with non-ADHD group, which is consistent with a study by Rosler et al. (2009) that reported significantly higher rate of stimulant use in female compared with male offenders. These results may suggest a possible element of self-medication with stimulants in the substance use of these female offenders. However, many reasons affect the choice of a substance of use: availability of drugs being an important factor.
Rates of psychiatric disorders are substantially higher in female and male offenders than in the general population (Coolidge, Marle, Van Horn, & Segal, 2011; Gunn, Maden, & Swinton, 1991; Teplin, Abram, & McClelland, 1996). Results from a prior study suggest that adult female offenders with ADHD show (compared with female offenders without ADHD) elevated rates of mood and anxiety disorders, BPD, and suicide risk (Westmoreland et al., 2010). By contrast, the present study did not find a significant difference in mood disorders or in BPD between ADHD cases and the non-ADHD cases, possibly due to the small sample size. However, in line with previous research, we observed a strong link between ADHD and ASPD (Biederman et al., 1995; Mannuzza et al., 1998; Murphy & Barkley, 1996), as significantly more women with ADHD met diagnostic criteria for ASPD in our study.
Our results indicate that the 6-item ASRS can be useful as a screening tool in female offenders. The results reported in this study show higher sensitivity than in general population (100% vs. 68.7%) but lower specificity (62.0% vs. 99.5%) similar to those reported in a recent Spanish study in a substance use population (Daigre Blanco et al., 2009; sensitivity: 100% vs. 87.5%, specificity: 66.0% vs. 68.6%), a result that may be expected given the high co-occurrence of SUD in prison population. In a study of 1,064 adults enrolled to a residential treatment facility for substance use treatment, the ASRS screener sensitivity and specificity were estimated as 100% and 96.1%, respectively (Adler, Guida, Irons, Rotrosen, & O’Donnell, 2009), with a PPV of 57.6% similar to our finding (PPV = 55.0%).
The full 18-item ASRS demonstrated sensitivity similar to that of the 6-item screening version but a lower specificity (45.0%), and also a lower PPV (0.42). In conclusion, our results support the utility of the 6-item ASRS to screen for ADHD in this population but indicate that a more careful assessment is required to obtain a correct diagnosis as the screener lacks the specificity to distinguish ADHD from other psychiatric disorders and substance use in this population. Furthermore, the potential role of chronic and severe substance use in the induction for screening and maintenance of ADHD symptoms needs to be investigated.
Collectively our findings highlight the importance of detecting ADHD in this high-risk population bearing in mind that ADHD is a disabling but also, to a high degree, a treatable disorder. Prisoners with ADHD account for more aggressive incidents than other prisoners, more than those with ASPD (Young, 2009). Efficient treatment strategies that take to account ADHD symptoms could enable the offenders to utilize the psychosocial treatment programs provided in prison. Recently, promising results have been reported from a medication trial in male inmates with ADHD (Ginsberg & Lindefors, 2012) and on psychosocial treatment program in adults with ADHD and severe personality disorders in forensic setting (Young et al., 2012).
Limitations
The results of the present study should be interpreted bearing in mind several limitations. First, due to the small sample, we had a limited power to detect significant differences between ADHD cases and the non-ADHD group, and the results should be considered as exploratory. Second, even if we aimed to generate a representative cross-sectional sample by including all Swedish, medium- and high-security female prisons, the response rate was relatively low (57%), indicating that a selection bias cannot be ruled out entirely. It should, however, be noted that that the participants included in the screening phase only and those involved in the screening and interview phases were comparable in the screening results, suggesting a random rather than a selective attrition. Third, we lack information regarding the interrater reliability of the diagnostic interviews.
Conclusion
ADHD is a common psychiatric disorder in female prisoners, and our results indicate that as many as one in three can be affected. ADHD is a treatable condition, and possible benefits of treatment during and after incarceration deserve more attention. Untreated ADHD is a disabling condition that affects every day functioning and thus could have a negative impact on participation in treatment programs available in prison. Our results suggest that the ASRS 1.v.1. (6-item ASRS) is a useful screening instrument even in prison populations. It is important to bear in mind that a positive screening result should be followed by careful diagnostic procedure to validate the diagnosis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Swedish Prison and Probation Service.