
Abstract
Introduction
Treatment of psychiatric and neurological comorbidities is currently recommended as part of the overall management for patients with epilepsy (Kanner, 2016). ADHD is a common comorbidity with epilepsy (Ettinger et al., 2015; Ottman et al., 2011; Schubert, 2005; Williams, Giust, Kronenberger, & Dunn, 2016), occurring in up to 40% of children with epilepsy (Semrud-Clikeman & Wical, 1999) and up to 20% of adults with epilepsy (Babcock & Ornstein, 2009; Ettinger et al., 2015; Pineda et al., 2014). Identification of ADHD in patients with epilepsy is difficult because the symptoms and management related to epilepsy can directly contribute to attention deficits (Ettinger et al., 2015). In some patients, ADHD diagnosis is impeded by seizure related memory problems, but symptoms of inattention can persist even after seizures are controlled (Kälviäinen, Aikiä, Helkala, Mervaala, & Riekkinen, 1992; Masur et al., 2013). Cognitive side-effects of antiepileptic drugs (AEDs) can further complicate the recognition of underlying ADHD (Eddy, Rickards, & Cavanna, 2011; Schubert, 2005). Determination of effective screening tools could better equip clinicians to efficiently identify patients at a high risk of comorbid ADHD (Ettinger et al., 2015; Pineda et al., 2014; Semrud-Clikeman & Wical, 1999).
The Adult ADHD Self-Report Scale (ASRS) is a well-validated screening tool for ADHD symptoms in adults. The ASRS has been demonstrated to have high specificity and classification accuracy for a clinical ADHD diagnosis (Kessler, Adler, Ames, et al., 2005). This 18-item symptom checklist is based on the Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric Association, 1994) criteria of ADHD. The ASRS was developed by the World Health Organization (WHO) and can be easily self-administered. This screen relies solely on the patient’s subjective assessment of attention deficits and gauges the extent to which attention-related symptoms are interfering with the patient’s daily activities.
The Conners Continuous Performance Test (CPT) evaluates sustained attention, response time, and inhibition of response (Conners, Epstein, Angold, & Klaric, 2003). In the commonly utilized computerized version of this test, participants must discriminate between target and nontarget letters that appear on a computer monitor. The CPT provides an objective measure of performance variables related to attention deficits and impulsivity, and compounding of CPT performance variables has been shown to discriminate between adults with and without ADHD with moderate clinical utility (Cohen & Shapiro, 2007; Epstein, Conners, Sitarenios, & Erhardt, 1998).
No single ADHD screening instrument has in itself a high enough positive predictive value to validate the diagnosis of ADHD (Haavik, Halmøy, Lundervold, & Fasmer, 2010). When combined, a performance test and a self-report behavioral rating can be sufficient in detecting clinically significant deficits in executive functioning (Barkley & Murphy, 2010; Pettersson, Söderström, & Nilsson, 2018). We hypothesized that when administered together, the ASRS and CPT may effectively detect ADHD symptoms in an adult population.
Here, we describe the results of two validated ADHD screening tools in a population of adults with a history of refractory seizures. Among patients with epilepsy, we found that ADHD symptoms were reported (ASRS+) at a higher rate than expected (Ettinger et al., 2015; Ottman et al., 2011). The positive ASRS screen rate was even higher among patients with psychogenic nonepileptic seizures (PNES). Our findings support the use of the ASRS, with or without the CPT, to identify possible ADHD patients in the Epilepsy Monitoring Unit (EMU). Ultimately, the high number of positive screens coupled with the convenience of screening in this setting demonstrates the appropriateness of ADHD screening for this high-risk population.
Method
Study Design and Participants
Participants were recruited from a consecutive series of patients admitted to the EMU at Baylor St. Luke’s Medical Center (BSLMC) between June 2018 and September 2019 when at least one of the investigators was available. Patients were tested on the day of admission, typically prior to any withdrawal of medication. During this period, 101 patients, aged 18 to 78 years, were screened for ADHD. Exclusion criteria included insufficient fluency in English and cognitive constraints that prevented understanding of the consent process and testing protocol. Participants gave written informed consent. Patients who screened positive on the ASRS and/or CPT were instructed on how to request referral for further neuropsychological testing. Epilepsy type was based on video-electroencephalography (vEEG) and other clinical data by a board-certified epileptologist. To avoid bias, all patients were considered for testing, regardless of diagnosis. Handedness, previous and current ADHD diagnosis, previous and current ADHD medication use, and days since their most recent seizure were all specifically requested from each patient. Psychiatric conditions, such as comorbid mood and anxiety disorders, were identified through review of patient history. Detailed analysis was performed on patients who were diagnosed with either epileptic seizures (ES) or PNES. Due to the low sample size of the remaining patients (including mixed ES and PNES, nondiagnostic, and physiological events), we excluded these patients from detailed statistical analysis. Sample size was estimated with a power level set at 0.8 and alpha at .05, with a dichotomous endpoint. This study was approved by the Institutional Review Board at Baylor College of Medicine and affiliated hospitals.
ADHD Screening Instruments
ASRS version 1.1
Patients self-administered the 18-item ASRS version 1.1 (Kessler et al., 2007). For each question, participants indicated frequency of DSM-IV ADHD symptoms using a five-stepped Likert-type scale (0 = never and 4 = very often). Six of the 18 questions have been demonstrated to produce the highest clinical ADHD prediction accuracy (Kessler, Adler, Ames, et al., 2005). The responses to these six questions contribute to the screen score, and the remaining 12 items provide supplementary cues about patients’ symptoms. According to a prespecified scoring threshold, one point was assigned to each of the six items and then summed across the questionnaire, creating a score range of 0 to 6. The unweighted six-question score was dichotomized to indicate overall screen result: ASRS+ = ≥4 and ASRS– = 0 to 3.
CPT-III
CPT-III was utilized as an objective assessment of attention. Patients were seated in front of a laptop in their hospital room. Patients were asked to quickly press the space bar each time a letter appeared on the screen, except for the target letter “X.” Each letter was displayed for 250 ms, constituting a trial. The assessment contained 360 trials, lasting for a total of 14 min. The test was divided into six blocks, each containing three 20-trial sub-blocks with interstimuli intervals (ISI) of 1, 2, and 4 sec. Scores for the following variables were calculated from the composite of all trials:
Response style: Each individual’s natural tendency in the trade-off between speed and accuracy. Each respondent was classified as having one of the following response styles: conservative (emphasizes accuracy over speed), liberal (emphasizes speed over accuracy), or balanced (sensitive to both speed and accuracy).
Detectability: Ability to differentiate nontargets (the letter X) from targets (all other letters).
Omissions: Failure to respond to targets.
Commissions: Incorrect responses to nontargets.
Perseveration: Random or anticipatory responses.
Hit reaction time (HRT): Mean response speed of correct responses.
HRT standard deviation: Consistency of response speed during entire test.
Variability: Consistency of response speed within sub-blocks.
HRT block change: Change in mean response speed across blocks.
We analyzed standardized T-scores for each measure. Response style classified patients by the trade-off between speed and accuracy: conservative (T-score ≤ 40), liberal (T-score ≥ 60), or balanced (T-score = 41-59). For all other measures, T-scores were considered atypical if ≥60. For HRT, T-scores of ≤44 or ≥60 are atypical.
The CPT reports a likelihood (very high, high, moderate, or minimal) of the test subject having a disorder characterized by attention deficits, such as ADHD (Keith Connors, 2015). This likelihood is based on the number and magnitude of each subject’s T-scores compared with an age- and gender-matched normative sample. As previously reported, ADHD likelihood was dichotomized: CPT+ includes a moderate to very high likelihood of an attention disorder and CPT– includes a minimal likelihood of an attention disorder (Baggio et al., 2019).
Statistical Analysis
All data analyses were conducted using GraphPad Prism Version 7.01. We performed descriptive statistics on the participants’ characteristics, ASRS, and CPT test results. Unpaired t tests and Mann–Whitney U tests were utilized for inferential statistical comparisons. Chi-square and Fisher’s exact tests were conducted to compare frequency distributions. Statistical significance was set at p < .05.
Results
Out of 146 potentially eligible patients, 45 patients were excluded due to cognitive constraints (n = 14), physical constraints (n = 2), insufficient command of English (n = 4), or unwilling to participate (n = 25). A total of 101 patients were then recruited and consented for both the ASRS and CPT (Figure 1). Of the recruited patients, 54 were diagnosed with epilepsy and 22 were diagnosed with PNES. Other diagnoses included nondiagnostic (n = 18), mixed ES and PNES (n = 4), and physiologic events (n = 3). Of the patients diagnosed with epilepsy, 29 (53.7%) had temporal lobe epilepsy, 12 (22.2%) had frontal lobe epilepsy, six (11.1%) had genetic generalized epilepsy, and three (5.6%) had epilepsy with nonlocalizing seizures. There was one patient each with parietal lobe epilepsy, occipital lobe epilepsy, insular epilepsy, and multilobar epilepsy.
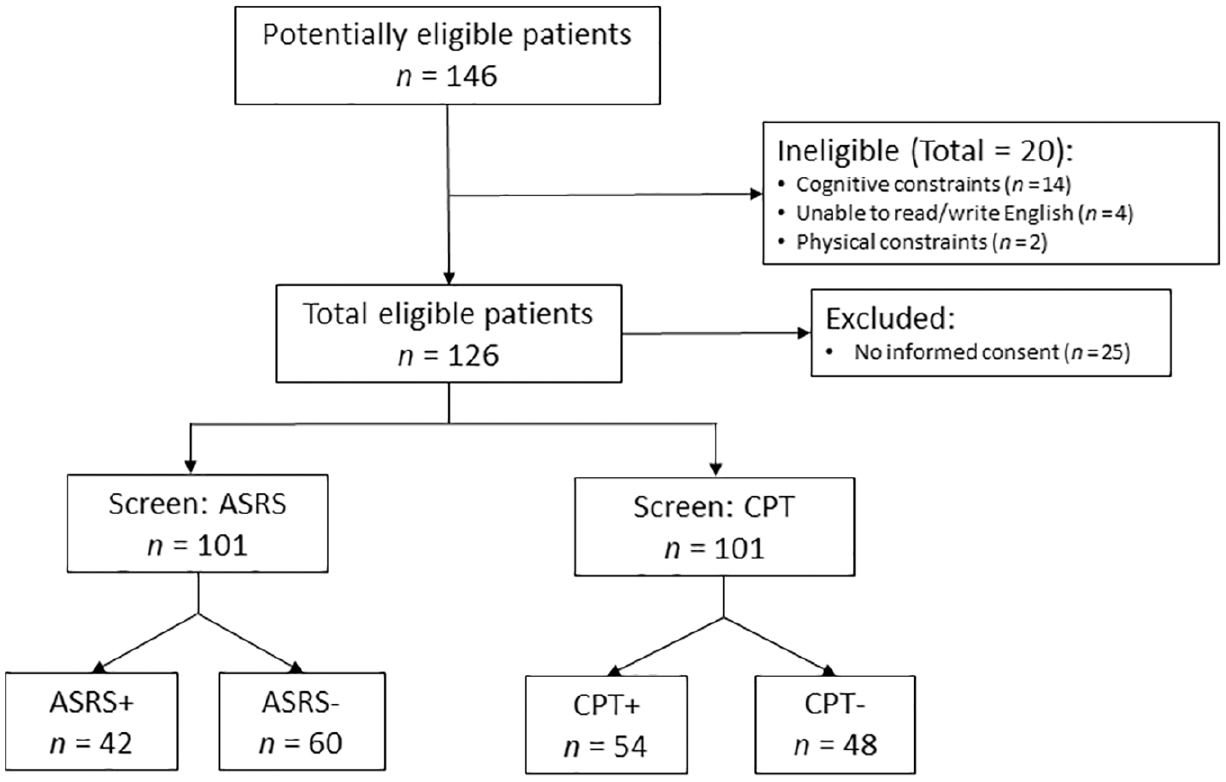
Flowchart of exclusion and inclusion criteria.
Between the patients with epilepsy and PNES, demographic characteristics including age, gender, handedness, and date of most recent seizure were not significantly different (Table 1). Interestingly, patients with PNES were significantly more likely than patients with epilepsy to have had a past history of ADHD (p = .011) as well as a history of taking medications for ADHD (p = .011). However, there was no significant difference between groups for either current diagnosis of ADHD or currently taking ADHD medications. Overall, four patients (one with epilepsy) had a current ADHD diagnosis, two of whom were currently taking ADHD medications. However, in both cases, their ADHD medication (atomoxetine and mixed amphetamine) was held during their EMU admission. There was no significant difference in the number of patients with a history of mood or anxiety disorders between the ES and PNES groups (p = .213). In addition, patients with PNES were significantly more likely to have a normal magnetic resonance imaging (MRI; 100% vs. 37.0%, respectively; p < .0001).
Demographic and Clinical Characteristics of All Participants, Participants With Epilepsy, and Participants With PNES.
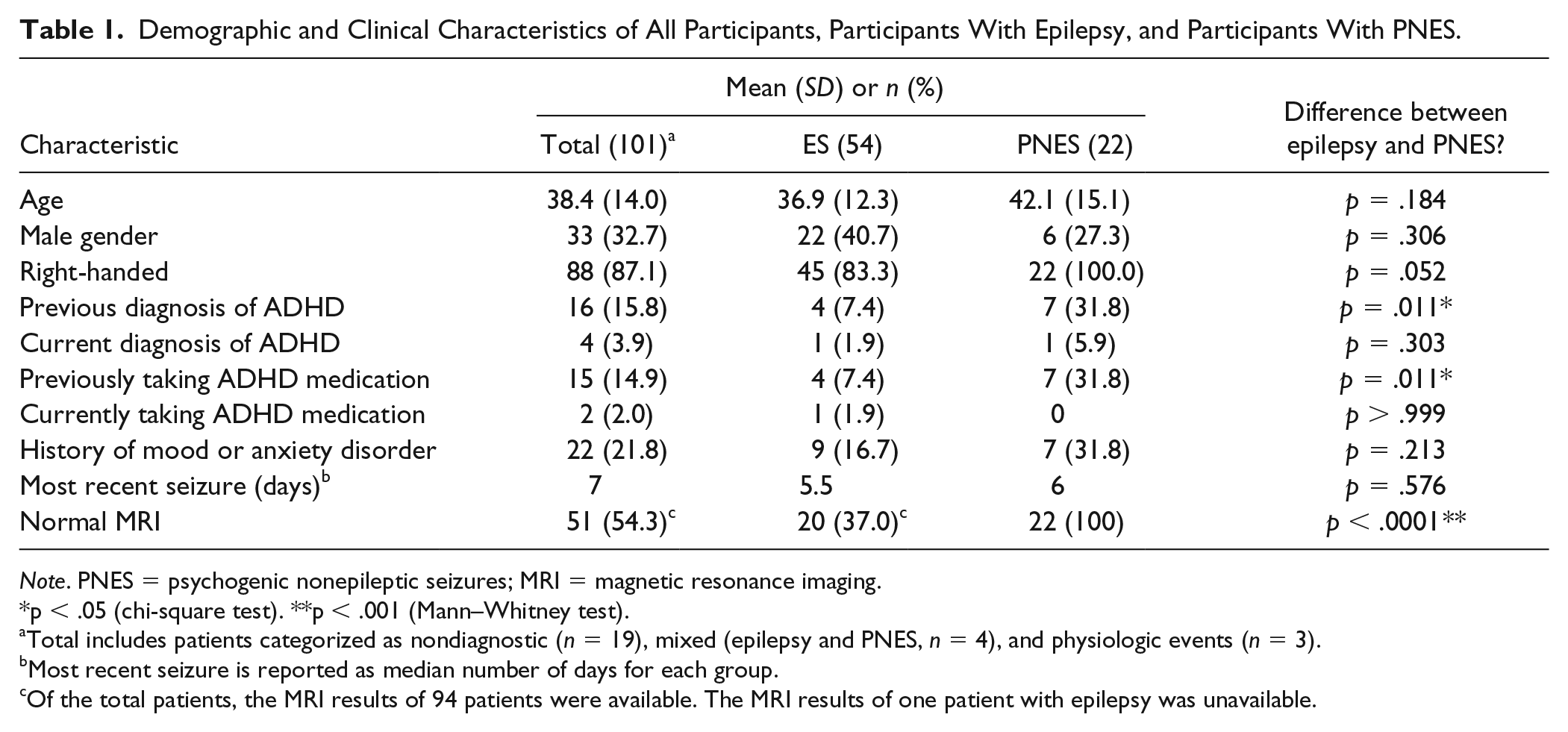
Note. PNES = psychogenic nonepileptic seizures; MRI = magnetic resonance imaging.
p < .05 (chi-square test). **p < .001 (Mann–Whitney test).
Total includes patients categorized as nondiagnostic (n = 19), mixed (epilepsy and PNES, n = 4), and physiologic events (n = 3).
Most recent seizure is reported as median number of days for each group.
Of the total patients, the MRI results of 94 patients were available. The MRI results of one patient with epilepsy was unavailable.
The ASRS was easily administered and took about 5 min for most participants to complete. Overall, 40.6% of patients were found to be screen positive (ASRS+: Part A score ≥4; Table 2). Patients with PNES were significantly more likely to be ASRS+ than patients with ES (63.6% vs. 27.8%, respectively; p = .005, chi-square test; Figure 2b). The CPT was administered in 14 min. Of note, there was one case where a patient was drowsy, and so the test was repeated after the patient was more awake, but altogether there were no logistical concerns with administering the test. Overall, 54.5% of patients screened positive for the CPT (CPT+). Although there was no significant difference between patients with PNES and patients with ES who screened CPT+ (54.5% vs. 53.7%, respectively; p > .999, chi-square test; Figure 2b), patients with PNES had significantly greater commissions and a higher HRT standard deviation (p = .037 and p = .036, respectively; Table 2). Furthermore, patients with PNES were more likely to score positively on both the ASRS and the CPT (45.5% vs. 12.9%, respectively; p = .002).
ADHD Screen Results of All Patients, Patients With Epilepsy, and Patients With PNES.
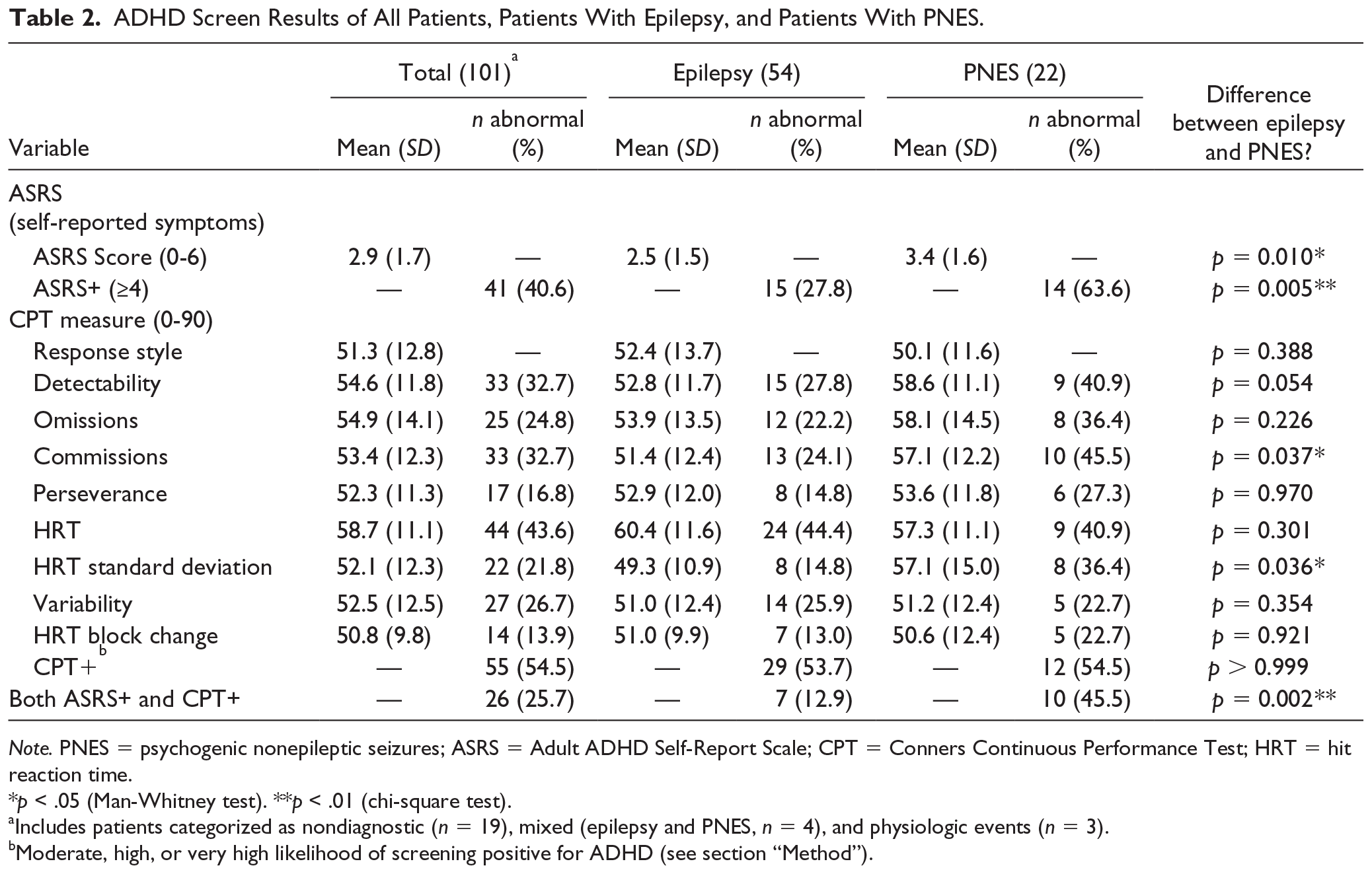
Note. PNES = psychogenic nonepileptic seizures; ASRS = Adult ADHD Self-Report Scale; CPT = Conners Continuous Performance Test; HRT = hit reaction time.
p < .05 (Man-Whitney test). **p < .01 (chi-square test).
Includes patients categorized as non-diagnostic (n = 19), mixed (Epilepsy and PNES, n = 4), and physiologic events (n = 3).
Moderate, high or very high likelihood of screening positive for ADHD (see Methods).

Patients with PNES score significantly higher on ASRS but not CPT compared with patients with ES: (a) distribution of ASRS score by clinical diagnosis (*p = .005, chi-square test); (b) distribution of number of atypical CPT T-scores by clinical diagnosis (n.s., chi-square test).
Results from the ASRS were not significantly predictive of overall performance on the CPT. Only 63.4% of ASRS+ patients were also CPT+, and 46.7% of ASRS– patients were also CPT+ (chi-square test, p = .146; Figure 3). The predictive value of the ASRS on CPT performance remained nonsignificant when looking only at ES or PNES patients. When comparing the performance of ASRS+ and ASRS– participants on specific CPT measures, poor detectability and a high commission error rate and fast HRT were the only three measures that independently correlated with ASRS+ (Mann–Whitney test, p = .004, p = .011, and p = .021, respectively; Figure 4).
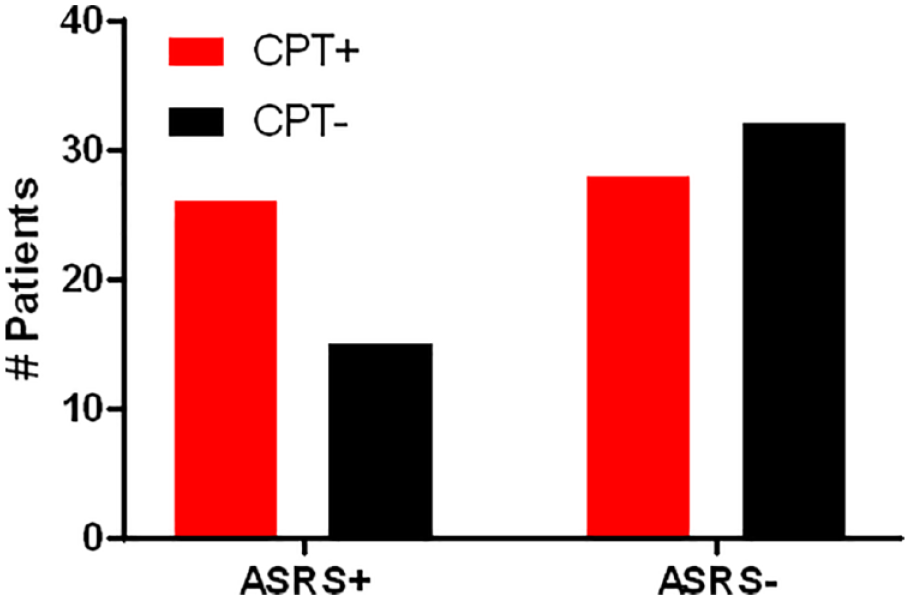
CPT performance is not associated with self-reported ADHD symptoms (n = 101, p = .146, chi-square test).
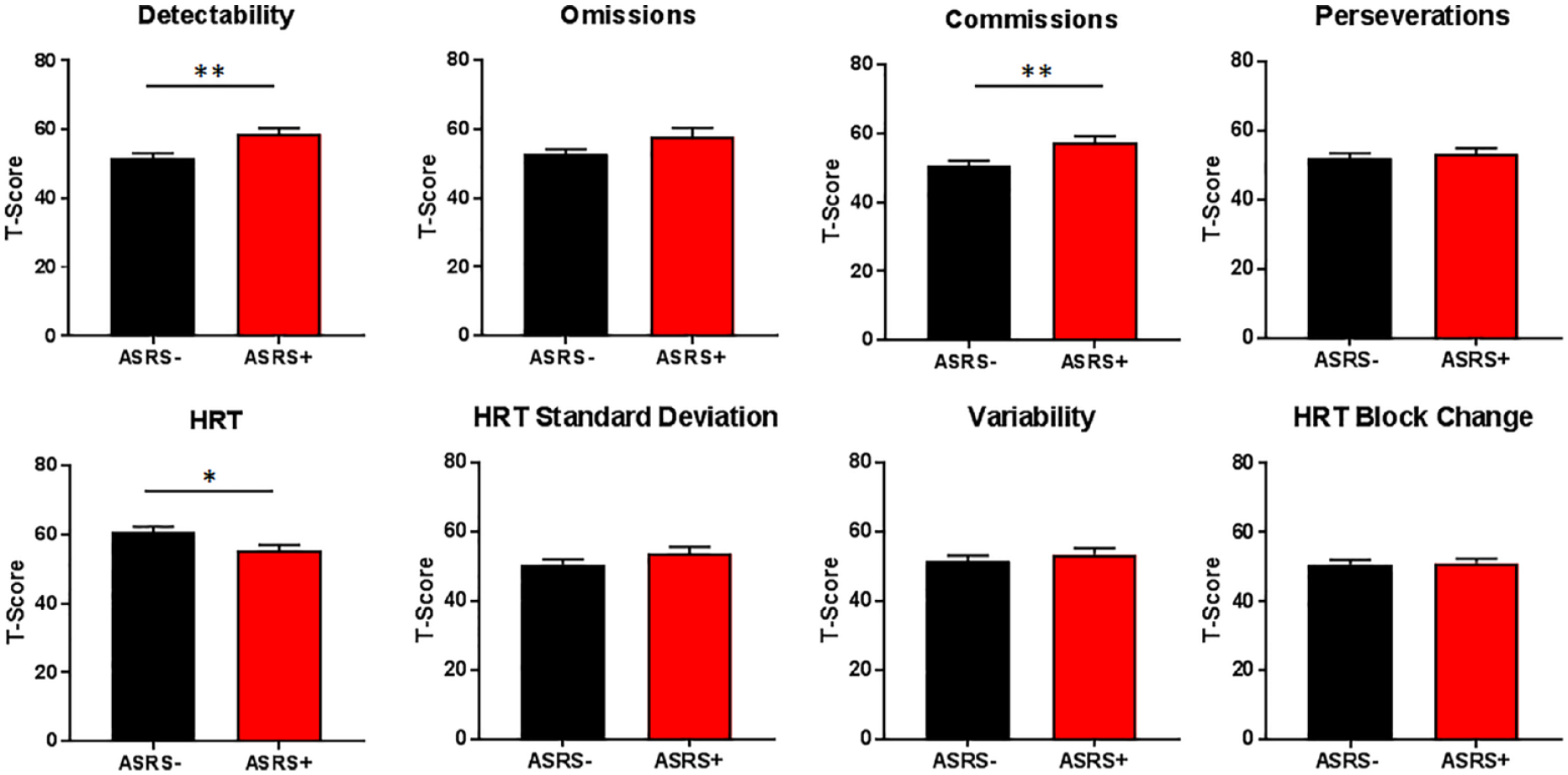
CPT measures of detectability, commissions, and hit reaction time are contingent on ASRS result. Bars depict mean score, and error bars represent standard error of the mean (n = 101, *p < .05, **p < .01, Mann–Whitney test).
When the personal characteristics of all subjects were analyzed, right-handedness and previous ADHD diagnosis were correlated with positive ASRS screen (Table 3). Older patients and female patients were more likely to screen CPT+ (chi-square test, p = .031 and p = .016, respectively). Of note, CPT performance was not significantly related to previous ADHD diagnosis (chi-square test, p = .762).
Demographic and Clinical Characteristics of Patients by ADHD Screen Result.
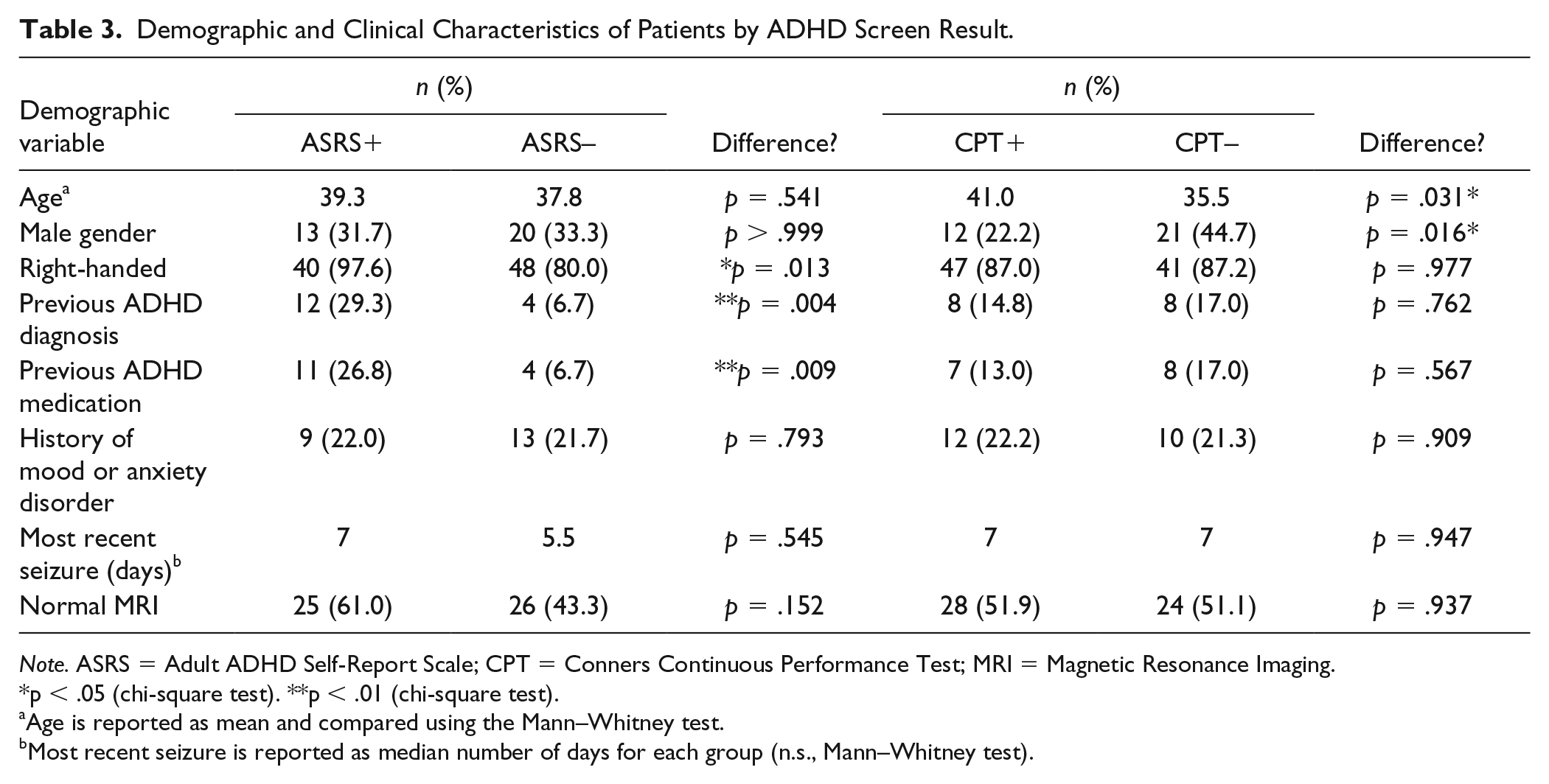
Note. ASRS = Adult ADHD Self-Report Scale; CPT = Conners Continuous Performance Test; MRI = Magnetic Resonance Imaging.
p < .05 (chi-square test). **p < .01 (chi-square test).
Age is reported as mean and compared using the Mann–Whitney test.
Most recent seizure is reported as median number of days for each group (n.s., Mann–Whitney test).
Discussion
Among adults admitted to an EMU, a striking proportion (40.6%) screened positive on the ASRS. Whereas previous studies were based on self-reported epilepsy, our investigation clarifies these findings with a definitive diagnosis of epilepsy. Our finding of 27.8% ASRS+ among patients with clinically determined ES is greater than the 13% to 18% previously reported ASRS+ rates for adults with self-reported epilepsy (Ettinger et al., 2015; Ottman et al., 2011). Importantly, our patient population is skewed toward patients with the greatest seizure burden, which may be associated with greater deficits in attention. Nonetheless, only 8.3% of patients with ES who scored ASRS+ had a current diagnosis of ADHD, providing further evidence that comorbid ADHD may be underdiagnosed among adults with epilepsy.
To our knowledge, we are the first to report a high rate of attention deficits (63.6%) among adults with PNES, a functional neurological disorder that is commonly misdiagnosed as epilepsy. Patients with PNES exhibit behavioral changes and convulsive episodes that can be difficult to distinguish from patients with ES. However, PNES is semiologically distinct from ES and can be differentiated by vEEG (Devinsky, Gazzola, & LaFrance, 2011; Salinsky et al., 2018). In the pediatric population, attention deficits are associated with PNES. Studies have reported that 7% to 28% of children with PNES are jointly diagnosed with ADHD (Rawat et al., 2015; Yi, Kim, Lee, Cheon, & Kang, 2014). However, the comorbidity of ADHD and PNES in adults has not been characterized. In addition, given that more than 10% of patients diagnosed with epilepsy may also be diagnosed with PNES, the epidemiology of comorbid ADHD, PNES, and ES may be even more complex (Salinsky et al., 2018).
Demographic predictors for ADHD screen performance were variable and unexpected. There was no difference in ASRS+ screening by gender, a finding that aligns with the previous findings in adult populations (Corbisiero, Hartmann-Schorro, Riecher-Rössler, & Stieglitz, 2017; Haavik et al., 2010; Kessler, Adler, Barkley, et al., 2005). Left-handed participants screened ASRS+ at a significantly lower rate than right-handed participants. This finding contrasts with findings in children where handedness is not associated with ADHD symptoms (Ghanizadeh, 2013). Our findings could be a consequence of low sample size and may have been influenced by the greater proportion of patients with epilepsy being left-handed compared with patients with PNES. Interestingly, older and female patients performed significantly worse on the CPT (Table 3), despite the fact that T-scores were already controlled for age and gender. These findings suggest that the EMU setting may enhance an underlying vulnerability in these populations, but further focused research would be necessary to draw any definite conclusions. Finally, despite the described reciprocal comorbidity of ADHD with mood and anxiety disorders (Biederman, 2004; Dunlop, Wu, & Helms, 2018; Perroud et al., 2014), we found no significant correlation between history of mood and anxiety disorder with either the ASRS or the CPT. Further study is warranted to dissect the complex interaction among psychiatric disorders, seizures, and ADHD.
Notably, 54.5% of patients in the EMU screened CPT+ (Table 2). Several lines of evidence point to the CPT as an unreliable screening tool in the EMU. First, the uniform CPT+ rate (~54%), independent of seizure type or history of ADHD diagnosis, was as high as adults with formally diagnosed ADHD (51.7%, Baggio et al., 2019). In addition, the CPT results had a low concordance with the ASRS (Figure 2), consistent with a previous study with similar methodology in adults (Baggio et al., 2019). We also found that patients previously diagnosed and treated for ADHD were significantly more likely to score ASRS+ but not CPT+ (Table 3). The CPT only predicted a minimal or moderate likelihood of attention deficits for all four patients with a current ADHD diagnosis. Finally, CPT performance may have been affected by distractions in an inpatient setting, medication changes, and occurrence of seizures. Altogether, these findings suggest that the CPT alone may not be an accurate predictor of attention deficits in this adult population.
Individual CPT variables have previously been associated with clinical ADHD diagnosis (Pettersson et al., 2018). A high commission error rate among adults with ADHD has been well described and is typically coupled with longer HRT, higher HRT standard deviation, and /or increased variability (Advokat, Martino, Hill, & Gouvier, 2007; Baggio et al., 2019; Pettersson et al., 2018). Similarly, compared with patients with ES, we found that patients with PNES had a significantly higher commission error rate and a higher HRT standard deviation (Table 2), providing further evidence for a higher proportion of attention deficits among patients with PNES. Among our EMU patients, a low detectability rate and a high commission error rate were associated with screening ASRS+ (Figure 4). The significantly faster HRT in the ASRS+ group may represent a greater degree of impulsivity compared with the ASRS– group, but this finding in isolation is difficult to interpret.
Our results suggest that the ASRS and CPT may be measuring different characteristics in the EMU. The association between ASRS screen performance and clinical ADHD symptoms in adults is well established across a variety of populations (Adler et al., 2006; Kessler et al., 2007; Kessler, Adler, Barkley, et al., 2005). Furthermore, as a retrospective assessment of chronic symptoms, the ASRS is less affected by medication side-effects, environmental distractors, and motivating pressures that can affect CPT performance (Baggio et al., 2019). Coupled with the convenience of ASRS administration, our findings suggest that administering the ASRS alone could be an efficient first-line screen for attention deficits of this population. The CPT may be useful to selectively administer to ASRS+ patients for further characterization. Additional investigation could elucidate the ability of individual CPT variables to detect ADHD (Pettersson et al., 2018), thus increasing the specificity of screening when co-administered. One advantage of performing the CPT while in the EMU is the ability to potentially examine electrographic correlates for attention during a task of sustained attention, which was outside the scope of this study but an important avenue to follow up in the future (Hasler et al., 2016; Lenartowicz & Loo, 2014; List, Rosenberg, Sherman, & Esterman, 2017).
There are several limitations to this study. Most importantly, a positive ASRS or CPT screen is not diagnostic of ADHD. According to the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; American Psychiatric Association, 2013), ADHD is identified by chronic and ongoing symptoms of inattention, impulsivity, and/or hyperactivity that interferes with functioning or development. Current diagnostic protocol requires a comprehensive clinical interview, rating scales for current and past symptoms, collateral information collected from multiple informants, and assessments for a spectrum of psychiatric and somatic disorders (Haavik et al., 2010). In contrast, a screening instrument such as the ASRS with a high negative predictive value can quickly determine concern for an attention-related disorder, identifying a need for further intensive neuropsychological testing for patients who screen positive. In addition, the cohort with epilepsy is fairly heterogeneous, including patients with focal, generalized, and unknown epilepsy etiologies. However, screening more patients with epilepsy could provide insight into the association of specific seizure types with ADHD symptoms. Another limitation is that this study did not consider the potential effect of medications on attention performance. Finally, this study did not include longitudinal follow-up on clinical diagnosis of participants who indicated ADHD symptoms. Investigation into the rate of formal ADHD diagnosis in this population could further clarify the nature of attention deficits in patients admitted to the EMU.
Here, we have demonstrated the high yield of screening for attention deficits in patients with a history of seizures in the inpatient environment. The EMU is an appropriate setting and opportunity to screen patients while they are actively seeking a comprehensive evaluation. There are also long periods of available time during an EMU admission as patients wait for seizures, contributing to the high rate of consent of eligible patients (80.2%) as a research protocol. The ASRS is a quick and effective screening tool which would likely have an even higher consent rate if performed without the CPT. In summary, our results suggest that the ASRS should be implemented more frequently and become common practice as the first step in the evaluation for ADHD in adult patients with seizures and/or epilepsy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.