
Abstract
Modern cardiac surgery has rapidly evolved to treat complex cardiovascular disease. This past year boasted noteworthy advances in xenotransplantation, prosthetic cardiac valves, and endovascular thoracic aortic repair. Newer devices often offer incremental design changes while demanding significant cost increases that leave surgeons to decide if the benefit to patients justifies the increased cost. As innovations are introduced, surgeons must continuously aim to harmonize short- and long-term benefits with financial costs). We must also ensure quality patient outcomes while embracing innovations that will advance equitable cardiovascular care.
Keywords
Introduction
The first documented cardiac surgery was performed in 1893 by Dr Daniel Hale Williams in a Chicago hospital after a man endured a stab wound to the chest. The procedure was performed under crude anesthesia on a beating heart prior to the advent of cardiopulmonary bypass. 1 From 1893 to the present, the history of cardiac surgery is one defined by innovation in both surgical techniques and devices. Noteworthy innovations in 2022 include the first transplantation of a genetically modified pig heart into a human, new options for prosthetic cardiac valve replacement, and novel devices in endovascular aortic repair. Cardiac xenotransplantation has the potential to overcome the limited supply of hearts available for donation. Novel devices for cardiac valve, aortic arch, and thoracic aortic repair have the potential to reduce operative time, reduce perioperative complications, and potentially offer options to those previously considered too high risk for surgery. This article will discuss these innovations in the context of how surgeons and other providers may evaluate the benefits vs. costs of these advances.
Xenotransplantation
There have been three noteworthy operations involving cardiac xenotransplantation, with the most recent taking place in 2022. 2 The first was performed in 1964 by Dr James Hardy, who transplanted a chimpanzee’s heart into Boyd Rush, a 68-year-old upholsterer, at the University of Mississippi Medical Center (Jackson, MS). 3 Unfortunately, the graft failed within 60–90 min of reperfusion. The second cardiac xenotransplantation was performed in 1984 by Dr Leonard Bailey at Loma Linda University Medical Center (Loma Linda, CA). He transplanted a baboon’s heart into Stephanie Beauclair (also known as “Baby Fae”), who was just 12 days old with hypoplastic left heart syndrome. 4 Stephanie’s xenotransplantation occurred when the outcomes for hypoplastic left heart syndrome were dismal, and Norwood’s operation was in its early stages with long-term results still accruing. 5 Unfortunately, Stephanie received an ABO mismatched xenograft, and she died on postoperative day twenty from progressive graft necrosis complicated by acute renal and pulmonary insufficiency. As an aside, the next year Dr Bailey performed the first successful orthotopic heart transplantation in an infant. 6
Given ethical concerns with the use of non-human primate donors and the accepted agricultural use of pigs as livestock, pigs subsequently became the focus of attention to expand the donor pool for xenotransplantation. However, as described by Singh et al. in a review of cardiac xenotransplantation, natural preformed antibodies against pig antigens trigger complement activation leading to hyperacute rejection and acute humoral rejection. Most of these antibodies target porcine carbohydrate antigens found on cardiomyocyte cell membranes. For this reason, initial attempts of xenotransplantation had graft survival measured in minutes or days. 7
Genetic engineering can prevent activation of these preformed antibodies and thus prevent early graft failure from coagulation dysfunction, as demonstrated by Mohiuddin et al. 8 Novel gene-editing technologies like CRISPR-Cas9 permit the development of knock out strains that lack immunogenic epitopes—such as α1-3-galactose, Sda blood group antigen, and N-glycolylneuraminic acid—while also inserting human complement inhibitory proteins and thrombomodulin. Reviewing the impressive progress made by genetic engineering in further detail is beyond the scope of this review. However, the importance of these milestones cannot be overstated.
On January 7, 2022, Dr Bartley Griffith at the University of Maryland Medical Center (Baltimore, MD) transplanted the heart of a genetically modified pig into 57-year-old David Bennet who suffered from non-ischemic cardiomyopathy.
2
This xenotransplantation was broadly made possible by three separate and equally important advances: (1) the use of a 10-gene-edit pig donor heart, (2) an ex vivo heart perfusion system to provide non-ischemic preservation, and (3) costimulation blockade-based immunosuppression using a humanized anti-CD40 monoclonal antibody.9,10 The graft was able to adequately support Mr. Bennet for 7 weeks before developing sudden diastolic failure and global myocardial thickening. Increased levels of porcine cytomegalovirus cell-free DNA were identified on routine testing, but it is unclear whether this finding played a direct role in graft failure. On postoperative day sixty, compassionate withdrawal of further advanced supportive care led to Mr. Bennet’s passing (Figure 1). Surgeons evaluate technologic advancements with risks, benefits, and costs to optimize patient outcomes and responsibly steward innovation.
Cardiac Valve and Thoracic Aortic Endograft Advancements
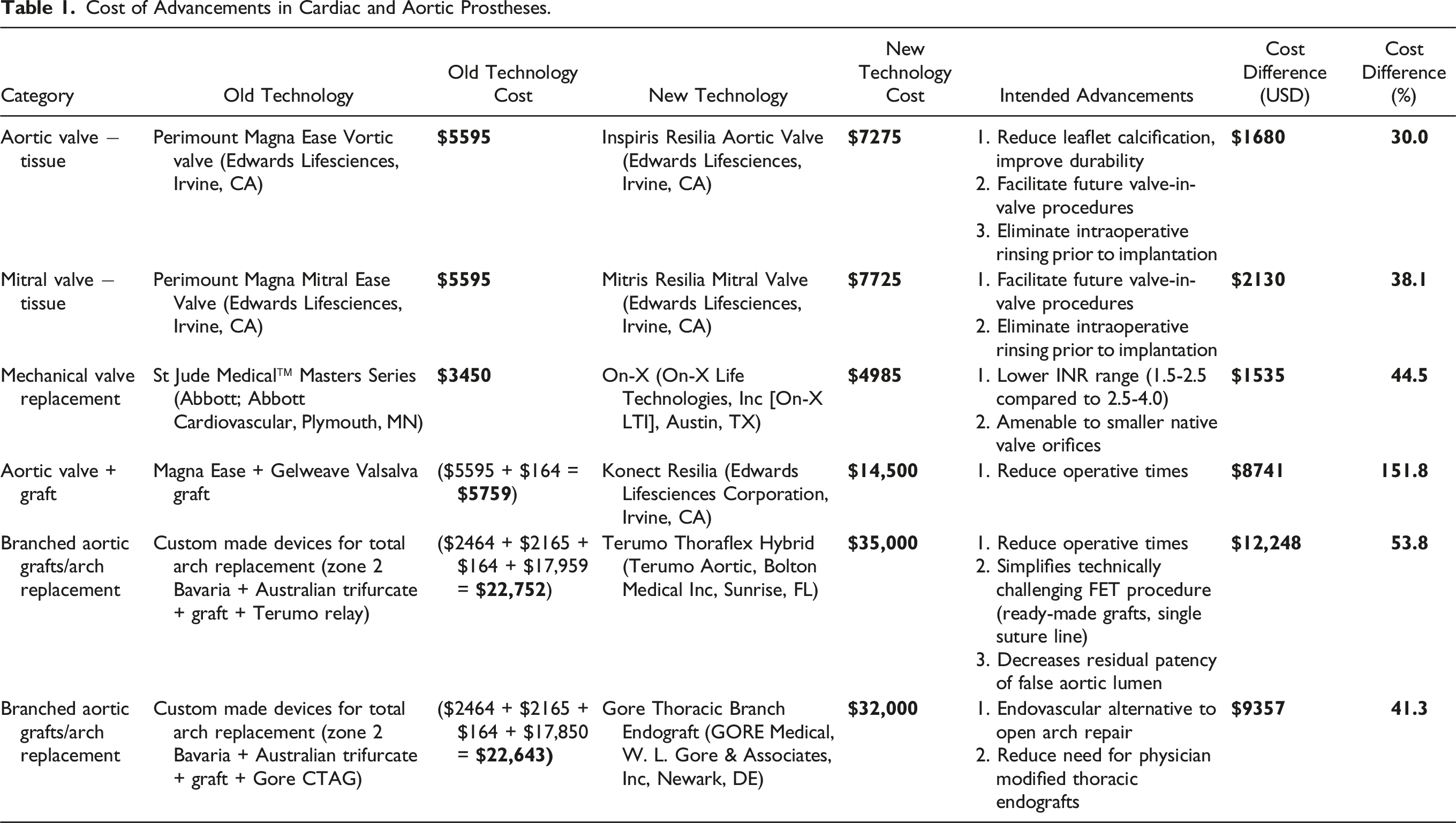
Cost of Advancements in Cardiac and Aortic Prostheses.
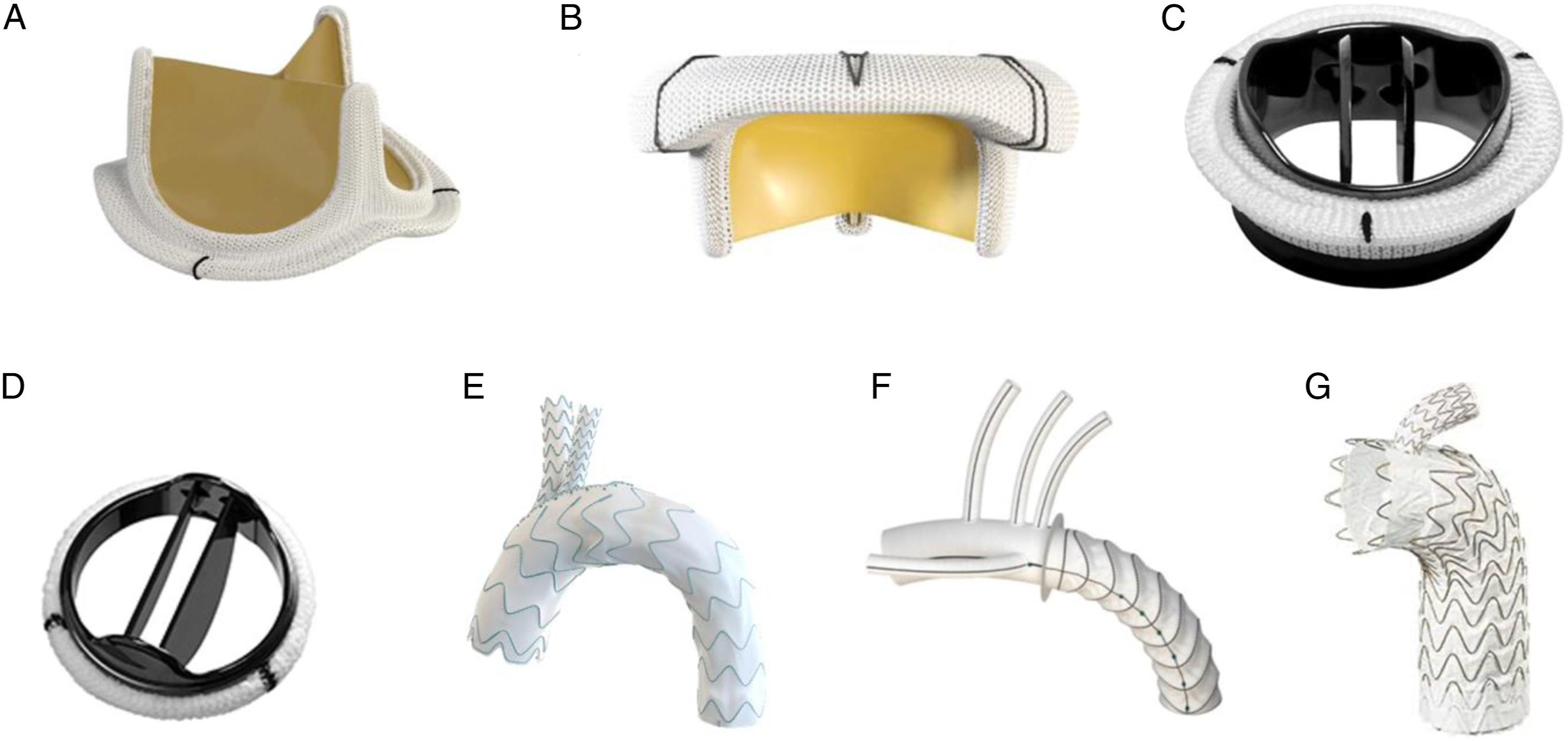
Cardiac valve and thoracic aortic endograft images.44-50 Cardiac valve prostheses: (A) Inspiris Resilia (Edwards Lifesciences, Irvine, CA)
44
a newer class of pericardial tissue valve for the aortic position, FDA approved in 2017 (B) Mitris Resilia (Edwards Lifesciences, Irvine, CA),
45
a newer class of pericardial tissue valve for the mitral position, FDA approved in 2022. (C) On-X Aortic Valve (On-X Life technologies, Inc, Austin, TX),
46
FDA approved in 2015 for patients to be managed at an international normalized ratio level of 1.5–2.0 starting three months after surgery (D) St. Jude medical™ masters series (Abbott; Abbott Cardiovascular, Plymouth, MN),
47
long-standing mechanical prosthesis for aortic and mitral positions. Thoracic aortic endografts: (E)
Prosthetic Cardiac Valves
Prosthetic heart valves, both mechanical and bioprosthetic, revolutionized the treatment of valvular heart disease. The first prosthetic valve had a ball-in-cage design that was inspired by a water bottle stopper and was implanted in the aortic valve position in the 1960s. 11 This was followed by the tilting disc and bileaflet valve designs, which provided enhanced hemodynamics, durability, and implantability but did not eliminate the need for long-term anticoagulation. Important considerations for valve prostheses include mitigating valve calcification, thrombus formation, infective endocarditis, and hemolysis. Individual factors like patient age, bleeding risk, and comorbidities are considered when choosing appropriate heart valves for patients, balancing an increased risk for leaflet calcification and limited durability in bioprosthetic valves against a lifetime dependence on anticoagulation for mechanical valves.
The Carpentier-Edwards Perimount Magna Ease aortic valve (Edwards Lifesciences, Irvine, CA) is a third generation bioprosthetic valve introduced to the United States (US) market in 2005 claiming reduced leaflet calcification and deterioration over time while allowing implantation in patients with small aortic roots by having a reduced profile height.12,13 Several studies demonstrate excellent mid-term functional and structural outcomes ranging from 5 to 12-year follow-up, including an 8-year follow-up published in 2022 by Tsui et al.14,15 The Inspiris Resilia tissue valve (Edwards Lifesciences, Irvine, CA) was introduced to the US market in 2017 touting even greater reduction in leaflet calcification and increased durability. These claims were validated by the COMMENCE Trial—a single-arm, multicenter observational study demonstrating encouraging 5-year outcomes. 16 The expandable stent within the Inspiris valve allows for more predictable results and better control during transcatheter valve-in-valve procedures, with the first report of this application published in July 2022.17,18 Another benefit of this valve’s design is the elimination of glutaraldehyde preservation, which enables dry storage and therefore eliminates the need for rinsing prior to implantation. Although introduction of the Inspiris Resilia tissue valve was intended to provide a more durable aortic valve, long-term data is not available and there has been no head-to-head comparison with other valves on the market. The only definite difference is the ability to implant the Inspiris Resilia tissue valve without having to rinse intraoperatively, which is arguably of minimal difference to the surgeon and patient.
Mirroring advancements in the aortic valve market, the Mitris Resilia mitral valve (Edwards Lifesciences, Irvine, CA) received FDA approval in March 2022. This is the next generation valve of the Carpentier-Edwards Perimount Magna Mitral Ease (Edwards Lifesciences, Irvine, CA), which was introduced to the US market in 2009. 19 Intended advancements include cobalt chromium bands, which provide good visibility under fluoroscopy for future transcatheter procedures and dry storage, eliminating the need for intraoperative rinsing. It has a cinch mechanism to prevent sutures from looping the posts during implantation and is designed to minimize the risk of left ventricular outflow tract obstruction. There are no studies to demonstrate superior outcomes compared to prior generation valves and data to support its use is extrapolated from the Perimount Magna Mitral Ease.
For patients requiring a tissue valve aortic root replacement, the Konect Resilia Aortic Valved Conduit (Edwards Lifesciences, Irvine, CA) is the first Food and Drug Administration (FDA) approved composite valve graft (CVG), receiving approval in July 2020. 20 In 2022, DeRoo et al published a case series describing their experience with this new device. 21 Prior to its availability, surgeons would combine a preferred aortic valve with a preferred prosthetic aortic graft. The aortic valve and aortic graft would be sutured together on the back table, increasing operative, cardiopulmonary bypass and aortic cross clamp times. In addition to saving a step during root replacement surgery, the Konect Resilia uses the same Resilia tissue as the Inspiris Resilia, intended to reduce calcification and increase durability of the aortic valve. This too, is stored dry and therefore does not require intraoperative rinsing prior to implantation. Although this new device is undoubtedly more convenient for the surgeon and eliminates the step of back table preparation, there has been no evaluation of outcomes or reduction in operative times. However, there is certainly an increased cost (Table 1, Figure 2) associated with this new technology that is to be considered by surgeons adopting this newer technique. 22
Regarding both aortic and mitral mechanical valve replacement, the St. Jude Medical™ Masters Series Valve (Abbott Cardiovascular, Plymouth, MN) has been a reliable mechanical prosthesis for placement in the aortic and mitral positions for over 40 years (Figure 2). The newer On-X valve (On-X Life Technologies, Inc, Austin, TX) has comparable hemodynamic performance but may be beneficial for patients with increased risk for major bleeding due to the ability to maintain patients at a lower INR in the aortic position compared to the St. Jude Medical™ Masters valve (1.5–2.5 compared to 2.5–4.0, respectively), or for patients with physiologically smaller valve orifices.27-29 This potential benefit also comes with increased cost (Table 1). Similar to the Konect, the On-X is also available in a valve/graft combination for a mechanical valve root replacement.
Thoracic Aortic Endografts
Dr Charles Dubost and his team in Paris, France completed the first successful replacement of an abdominal aortic aneurysm with a homograft in 1953. 23 It was not long afterward that Dr Michael DeBakey, in collaboration with Professor Thomas Edman, a textile engineer, developed the first version of seamless elasticized woven Dacron grafts that are standard today. 24 This groundbreaking invention together with significant surgical innovation initiated a cascade of advancements to create methods for safe repair of the entire aorta.
In 1983, the elephant trunk technique was introduced as a dual-stage, open approach to repair pathologies of the distal aortic arch and descending aorta. One decade later, the frozen elephant trunk (FET) was introduced, which combines traditional tube graft replacement of the distal aortic arch with stent grafting of the descending thoracic aorta in a single operation. Compared to the previous dual-stage procedure, the FET eliminates the need for a second procedure while reducing operative time, circulatory arrest time, technically involved steps, and residual patency of the false aortic lumen.25,26 Ready-made hybrid surgical grafts further simplify and standardize this approach. Ready-made grafts were primarily implemented in Europe and Canada before FDA approval of the Thoraflex Hybrid (Terumo Aortic, Sunrise, FL) in the United States in April 2022. 27 A US-based multicenter clinical trial of the Thoraflex Hybrid device showed comparable or better outcomes in permanent stroke, paraplegia/paresis, unanticipated aortic reoperation and all-cause mortality at one year compared to the traditional elephant trunk method.28-30 Notably, early thrombus is a concern for FET devices, and is associated with larger aneurysms, smaller FET grafts, and conservative management of bleeding. These concerns can be mitigated somewhat by early transthoracic endovascular aortic repair (TEVAR) completion, slight FET oversizing, and early reintervention for major bleeding. 31 Prior to the approval of industry-made hybrid devices in the United States, the innovative Buffalo Trunk technique allows for immediate single-stage FET repair at the time of circulatory arrest without compromising patient outcomes compared to hybrid devices. 32
In cases of aortic arch pathologies, traditional TEVAR requires covering the aortic arch branch vessels with subsequent anatomic bypass. Alternatively, branched endografts maintain the patency and perfusion of branched vessels while preserving the completely endovascular approach that is instrumental for managing patients who are not surgical candidates. The Gore TAG Thoracic Branch Endoprosthesis (TBE) (Gore, Flagstaff, AZ) is the only device currently approved for this approach in the United States and is only approved for Zone 2 placement to preserve the left subclavian artery.33,34
The accelerating pace of innovation will only continue to drive up costs in healthcare in the near future. Table 1 outlines the cost differences for the new devices described above compared to prior models. Each incremental innovation contributes to an additive cost impact. What is the cost of innovation, surgeon time, short-term and long-term patient benefit, and who pays? Increasing transparency and surgeon awareness of cost is critical to helping surgeons perform better in their roles as stewards of patient care, innovation and healthcare dollars.
Cardiac Surgeons as Stewards of Care
Cardiothoracic surgeons have long been at the forefront of innovation in healthcare, developing new techniques, developing new devices, and leveraging technology to improve patient outcomes. As healthcare evolves and becomes increasingly complex, the role of the surgeon has also evolved. Today, surgeons are providers of care, innovators, partners with industry, and stewards of these innovations. Performing these new roles is crucial for delivering cost-effective care and improving patient outcomes.
The volume of aortic surgery in the United States has increased significantly while the outcomes for patients have dramatically improved. Hirji and colleagues 35 examined the National Inpatient Sample and identified a 40% increase in the volume of open proximal aortic surgery between 2002 and 2014 and a 50% decrease in in-hospital mortality. These findings are probably the consequence of multiple factors: the increasing population size, higher prevalence of risk factors such as hypertension, the increased availability of high-resolution imaging studies, standardization of operative technique, hospital-level quality improvement processes, regionalization of surgical care to high-performing centers, increased rates of discharge to rehabilitation facilities, and the arrival of new devices to treat these patients. The latter has gained particular importance in the past couple of years as the surgical device space is booming. For example, three of the previously mentioned devices became more widely available in 2022: the Thoraflex Hybrid graft (Terumo Aortic, Bolton Medical Inc, Sunrise, FL), 36 the GORE TAG Thoracic Branch Endoprosthesis (GORE Medical, W. L. Gore & Associates, Inc, Newark, DE), 37 and the Konect Resilia aortic valved conduit (Edwards Lifesciences Corporation, Irvine, CA). 38 While these devices have been in existence for several years under investigational use, they only recently gained FDA approval and have become accessible at most tertiary centers. 39 Furthermore, there are ongoing clinical trials to closely monitor patient outcomes with their widespread use and/or to expand the approved indications for these devices.40-42
The cost of these new devices and obtaining their benefits is financially significant. For this reason, the Thoraflex device received approval from the Centers for Medicare and Medicaid Services for add-on payment which covers approximately 65% of the cost of the device in addition to the payment made for the current procedural terminology code of that operation. 43 While the use of these new devices may be very profitable in the short term at the hospital level, they will quickly amass an increased expenditure on the healthcare system. In addition to these more expensive devices, other innovations have been more readily adopted, such as the Cor-Knot (LSI Solutions, Greenwood Village, CO), AtriClip (AtriCure Inc, Mason, OH), and a variety of hemostatic agents, all which may increase the cost of providing surgical care without providing a proven and tangible benefit towards the patient’s outcome. Acknowledging that these noteworthy devices and new technology add expense, each surgeon must weigh the cost vs benefit of using them.
It is here where a surgeon’s determination of justified use becomes paramount to finding the balance between obtaining the short-term benefits of using these devices cost-effectively without compromising the patient’s long-term outcomes (Figure 1). Which patient will benefit enough from shaving a couple of minutes off their circulatory arrest time or cardiopulmonary bypass time to justify adding several thousands of dollars to the cost of their care? Which patient populations benefit the most from a one-stage repair vs a two-stage repair for thoracic aortic disease? Answering such questions has become the responsibility of cardiothoracic surgeons as stewards of patient outcomes and the added expense generated by these new technologies. It is most likely that with selective use in appropriate patients, the cost of these technologies may be absorbed by the healthcare system given that they yield good long-term outcomes.
Conclusion
Cardiothoracic surgeons are responsible for ensuring that new devices are used safely and cost-effectively. This includes evaluating the evidence supporting the use of these products, determining which patient populations are best served by them, and which patients do not see an added benefit in their use. In 2022, new clinical results became available for several of these noteworthy devices, and some also became more widely available resulting in greater use. These devices may help surgeons achieve enhanced patient outcomes through measures such as decreasing circulatory arrest time, bypass time, and the number of surgical stages required for intervention. However, these perceived benefits will likely incur a significant long-term cost to the healthcare system that will require cardiac surgeons to evaluate which candidates are appropriate to undergo procedures with these devices based on individual expected benefit. Cardiac xenotransplantation was another noteworthy innovation from 2022 that will require equal scrutiny to ensure optimal patient benefit is achieved with maximal efficacy, equity and safety considerations. As cardiac surgery continues to rapidly evolve, cardiac surgeons must harmonize the dynamic tension between patients, innovation, and impacts on the greater healthcare system. This requires surgical expertise, historical knowledge of the specialty, and the ability to anticipate future impacts of modern techniques.
Footnotes
Acknowledgments
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.