
Abstract
Objective:
Endoscopic bariatric therapies, including intragastric balloons (IGBs) are effective minimally invasive options for obesity management, particularly for patients who are not candidates for bariatric surgery. This study aimed to compare the safety profiles, weight loss outcomes, and tolerability of three fluid-filled IGB systems used in routine clinical practice.
Methods:
We conducted a retrospective cohort study of adults who underwent intragastric balloon placement at a single private bariatric center between January 2023 and January 2025. Data were derived from a prospectively maintained clinical database. Patients received one of three fluid-filled balloons: Allurion, Medsil, or Spatz3. Baseline demographic and anthropometric characteristics, weight loss outcomes, premature balloon removal, and readmission rates were assessed through completion of treatment. Comparative analyses across balloon types were performed using appropriate parametric and nonparametric statistical tests.
Results:
A total of 113 patients were included (mean age 34.9 ± 9.3 years; 91.2% female). Mean baseline body mass index (BMI) was 40.0 ± 7.9 kg/m2. Balloon distribution was Allurion (n = 13), Medsil (n = 40), and Spatz3 (n = 60). Overall mean absolute weight loss was 14.0 ± 8.3 kg, corresponding to a mean BMI reduction of 5.0 ± 3.0 kg/m2. Mean percentage total body weight loss was highest in the Spatz3 group (13.1 ± 7.3%), followed by Medsil (12.0 ± 6.2%) and Allurion (9.8 ± 3.9%); however, differences were not statistically significant (P = .33). Premature balloon removal due to intolerance occurred in 10.6% of patients, with no significant differences between balloon types. No major complications were observed.
Conclusion:
All three fluid-filled intragastric balloons demonstrated meaningful weight loss with acceptable safety and tolerability profiles. While the Spatz3 balloon achieved numerically greater weight loss, outcomes were comparable across devices without major adverse events. These findings support the role of IGBs as effective endoscopic bariatric therapies within a comprehensive obesity management framework.
Introduction
Obesity remains one of the most pressing global public health challenges, with prevalence rates continuing to rise across both high-income and low- to middle-income countries. 1 The condition is associated with increased all-cause mortality and a broad spectrum of cardiometabolic, oncologic, and musculoskeletal complications. 2 In sub-Saharan Africa, rapid urbanization, dietary transitions, and declining physical activity have contributed to a growing burden of obesity. 3 In Nigeria, adult obesity prevalence has been reported to be as high as 14.5%, with over one-quarter of adults classified as overweight, underscoring the urgent need for scalable and effective treatment strategies. 4
Contemporary obesity management follows a multimodal approach encompassing lifestyle modification, antiobesity pharmacotherapy, endoscopic bariatric therapies, and metabolic bariatric surgery (MBS).5–7 Glucagon-like peptide-1 receptor agonists and related pharmacotherapies have transformed medical obesity treatment but their long-term use may be constrained by gastrointestinal side effects, adherence, availability and cost challenges particularly in resource-limited settings. 8 Though MBS remains the most effective intervention for obesity across all body mass index (BMI) for sustained weight loss and metabolic improvement, its uptake is limited by cost, reduced access to specialized care, and apprehension about surgery and anesthesia.9,10
Intragastric balloons (IGBs) represent a minimally invasive, reversible endoscopic bariatric therapy that induces weight loss primarily through delayed gastric emptying, and neurohormonal modulation of appetite and satiety.11–13 Multiple randomized trials and real-world studies have demonstrated their efficacy as safe short-term weight loss tools and as bridges to MBS.12–14 Importantly, IGBs may be particularly relevant for patients who are not candidates for MBS due to medical contraindications or who have significant concerns regarding operative procedures and anesthetic exposure.9,10
Several fluid-filled IGB systems such as the Allurion, Spatz3 and Medsil balloons are currently in clinical use in Nigeria, differing in insertion technique, duration of implantation, adjustability, and removal requirements. The Spatz3 balloon is an endoscopically placed, adjustable balloon approved for up to 12 months of implantation.12,14 The Medsil balloon is a nonadjustable, endoscopically placed device intended for 6 months of use, 15 while the Allurion balloon is a procedureless, swallowable balloon that does not require endoscopy or anesthesia and is naturally excreted after approximately 4 months. 16 Despite increasing adoption, comparative data evaluating the effectiveness and safety of these devices particularly in African populations remain limited.
To address this gap, we conducted a single-center retrospective cohort study comparing safety, weight loss outcomes, and tolerability among patients receiving Allurion, Medsil, or Spatz3 intragastric balloons for obesity management in Nigeria. This study would provide guidance to physicians looking to choose the most appropriate IGB for their patients.
Materials and Methods
Study design and setting
This study was a retrospective analysis of a prospectively maintained clinical database, conducted in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology guidelines. The study was performed at a single private bariatric center in Abuja, North-Central Nigeria and included patients treated between January 2023 and January 2025. Informed consent was obtained from the patients and Ethical approval for this study was gotten from the Federal Capital Territory Health Research Ethics Committee, with approval reference FHREC/2025/01/134/190525. The study was conducted following the principles outlined in the Declaration of Helsinki and adhered to institutional guidelines for research involving human participants.
Patient selection
Adult patients (≥18 years) with a BMI ≥27 kg/m2 who underwent intragastric balloon placement for obesity management were eligible for inclusion. Patients were excluded if they had contraindications to balloon therapy, including active peptic ulcer disease, severe gastroesophageal reflux disease, large hiatal hernia, prior gastric surgery, or significant gastrointestinal pathology. Patients eligible for MBS were offered surgical treatment; those who declined surgery and opted for IGB therapy were included. All patients had anthropometric measurements taken at the first consultation. This included the weight, height and BMI at insertion, at follow-up visits and at balloon removal.
Balloon selection
Following multidisciplinary consultation, patients received one of three fluid-filled intragastric balloons (Allurion, Medsil, or Spatz3). Device selection was based on shared decision-making between the patient and bariatric surgeon, considering device characteristics, duration of therapy, need for endoscopy or anesthesia, and patient preference.
Description of intragastric balloon procedures
Allurion balloon
The Allurion balloon (Allurion Technologies, Natick, MA, USA) is a swallowable, procedureless balloon that does not require endoscopy or anesthesia. The balloon capsule attached to a thin tube was swallowed under medical supervision. In cases where patients experienced difficulty swallowing the capsule, a stylet was used to aid the process. Correct gastric positioning was confirmed by abdominal X-ray after placement was done, and the balloon was inflated with 550 mL of the recommended Allurion infusion fluid. The balloon is designed to undergo spontaneous deflation about 16 weeks from the insertion date, and it is subsequently excreted from the body via the gastrointestinal tract. 16 The Allurion balloon was introduced into our practice in December 2023 and came later than other balloons.
Medsil balloon
Medsil Balloon (CSC MEDSIL, Moskovskaya oblast, Russia) is a nonadjustable endoscopic balloon that can stay for up to 6 months in the stomach. Balloon placement was preceded by an endoscopy to assess the stomach and rule out any contraindication. Following this, the deflated balloon was passed through the mouth into the stomach, with correct positioning confirmed endoscopically. Thereafter, the balloon was inflated with 600 mL of sterile normal saline with 1% methylene blue. After inflation, the balloon catheter was extracted, completing the procedure. 15
Spatz3 balloon
Spatz3 Balloon (Spatz FGIA, Great Neck, NY, USA) is an adjustable endoscopic balloon. As with the Medsil balloon, placement was preceded by a diagnostic endoscopy to rule out any contraindications. The balloon was attached to the endoscope using the facilitator and lubricated. The balloon together with endoscope was then passed gently through the mouth into the stomach under direct visualization. Balloon inflation was done with normal saline mixed with 10 mL of 1% methylene blue up to an initial 600 mL volume. After inflation, the filling catheter was pulled into the mouth and then covered with the valve cap. The valve was reinserted into the mouth and gently pushed down into the stomach to complete the procedure.17,18
Postprocedure care
Following IGB insertion, patients were maintained in an anesthesia recovery room for approximately 2 hours until they had fully recovered from sedation. Subsequently, they were discharged on antiemetics (ondasetron tablets 8 mg 8 hourly), buscopan tablets 10 mg 12 hourly, paracetamol 1 g 8 hourly for the first 72 hours. Patients were prescribed proton pump inhibitors (omeprazole tablets 20 mg 12 hourly) starting a week before placement of the balloon and continued for the duration of the balloon therapy. A structured dietary protocol was implemented, beginning with a liquid diet and progressing to a hypocaloric solid diet (∼1200 kcal/day).
All patients were provided with a monthly follow-up appointment to follow up with weight, and potential side effects with a multidisciplinary team, which included bariatric surgeon, nurses and dietician. Physical activity of at least 150 minutes per week was encouraged. Patients who had significant side effects and problems tolerating orally were admitted for intravenous fluids and antiemetics.
Outcome variables
Primary outcomes included absolute weight loss, BMI reduction, percentage total body weight loss (%TBWL), and percentage excess body weight loss (%EBWL) assessed at balloon removal corresponding to the intended implantation duration of each device. Secondary outcomes included premature balloon removal due to intolerance, major complications, and hospital readmission. Balloon intolerance referred to patients who had prolonged persisting symptoms such as nausea, vomiting, abdominal discomfort or cramps despite medications that were severe enough to warrant early removal.
Statistical analysis
Statistical analyses were performed using SPSS version 25 (IBM Corp., Armonk, NY, USA). Continuous variables were summarized as means ± standard deviations. Pre- and post-intervention comparisons were assessed using paired t-tests. Between-group comparisons were performed using one-way analysis of variance (ANOVA) with post-hoc adjustment where applicable. Categorical variables were compared using chi-square or Fisher’s exact tests. A two-sided P value <.05 was considered statistically significant.
Results
Study population and baseline characteristics
A total of 113 patients met the study eligibility criteria and were included in the analysis (Table 1). The cohort was predominantly female (103
Baseline Characteristics of the Study Cohort (N = 113)
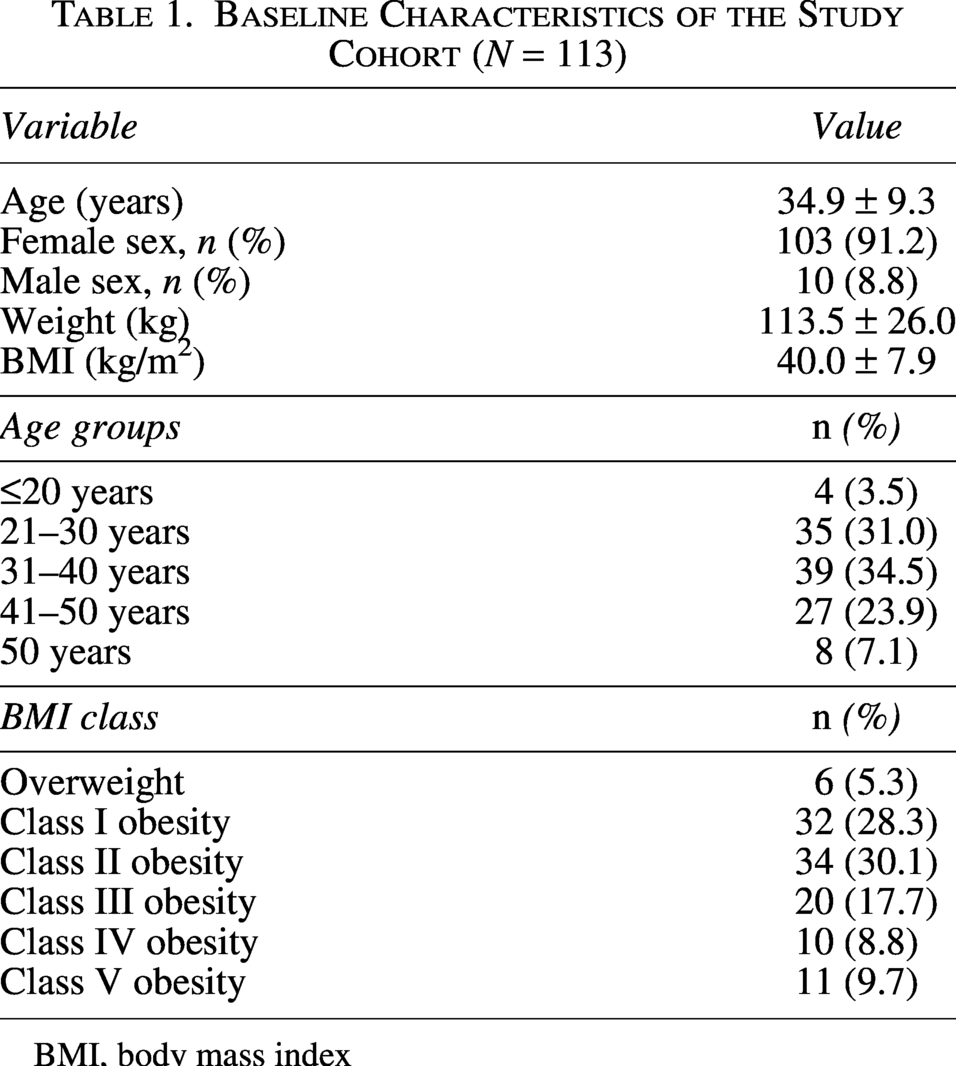
BMI, body mass index
At baseline, mean body weight was 113.5 ± 26.0 kg (range: 72–220 kg) and mean BMI was 40.0 ± 7.9 kg/m2 (range: 27.30 –66.18 kg/m2). Class II obesity represented the largest BMI category (30.1%), while 5.3% of patients were overweight.
Balloon type distribution and baseline comparisons
Three fluid-filled IGB devices were used: Allurion (n = 13, 11.5%), Medsil (n = 40, 35.4%), and Spatz3 (n = 60, 53.1%). As seen in Table 2, significant baseline differences were observed in baseline among groups (P = .003). Post hoc analysis demonstrated that patients in the Allurion group were significantly older that those in both the Medsil (44.1 ± 12.0 versus 34.6 ± 8.5 years, P = .006) and the Spatz3 groups (44.1 ± 12.0 versus 34.0 ± 8.8 years, P = .002) while no significant difference was observed between the Medsil and Spatz3 groups (P = .95). Baseline body weight also differed significantly between groups (P = .009). Post hoc analysis showed that the patients treated with the Spatz3 balloon had significantly greater baseline weight compared with those treated with Medsil (117.0 ± 29.1 versus 102.4 ± 16.5 kg, P = .02). No significant differences were observed between Allurion and Medsil (P = .22) or between Allurion and Spatz3 (P = .99).
Baseline Characteristics by IGB Type

Differences between groups were assessed using one-way ANOVA with Tukey post hoc correction.
Weight loss outcomes
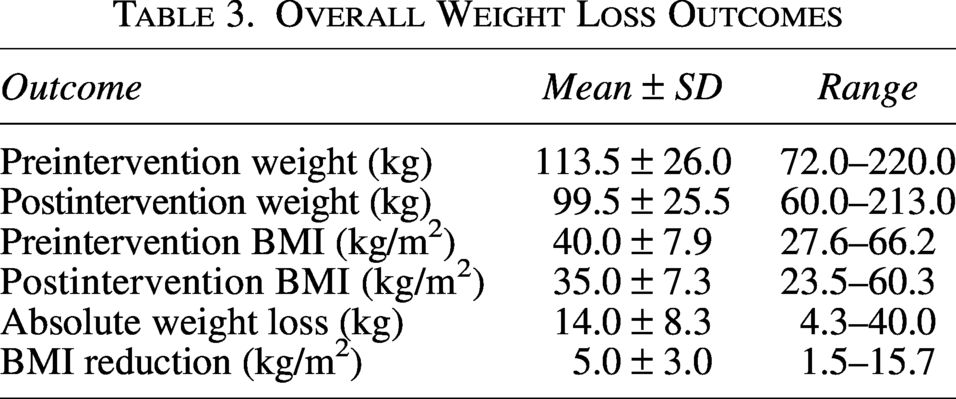
Following balloon placement, significant weight reduction was observed across the cohort. Mean absolute weight loss was 14.0 ± 8.3 kg, corresponding to a mean BMI reduction of 5.0 ± 3.0 kg/m2 (Table 3).
Overall Weight Loss Outcomes
Comparison of weight loss outcomes by balloon type
Weight loss outcomes stratified by balloon type are shown in Table 4 and Figure 1. Although numerical differences were observed across balloon types, no statistically significant differences were detected in %EBWL, %TBWL, or absolute weight loss.
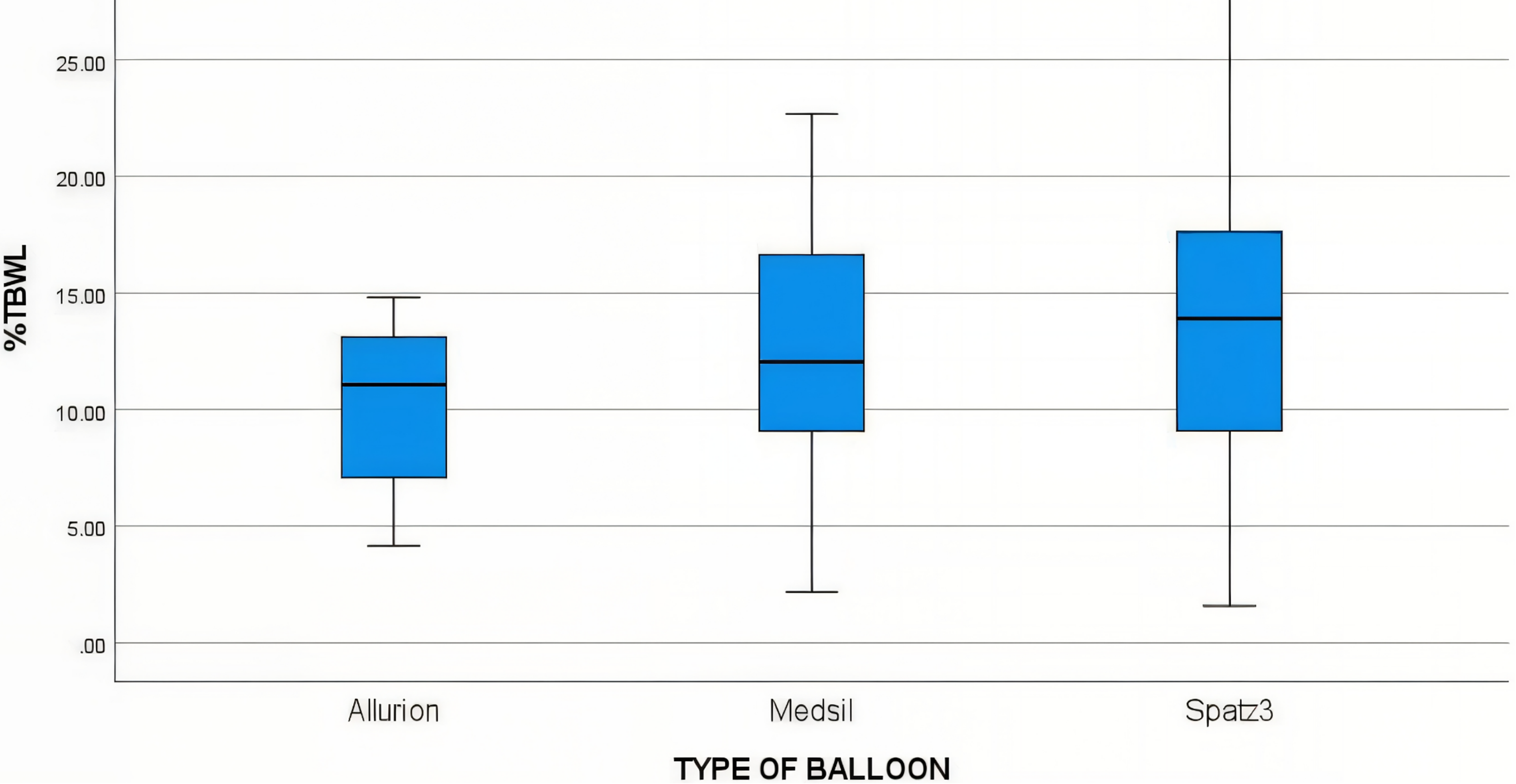
Comparison between the percentage total body weight loss (%TBWL) of the Allurion, Medsil and Spatz3 balloons at balloon removal. %TBWL, percentage total body weight loss.
Weight Loss Outcomes by IGB Type
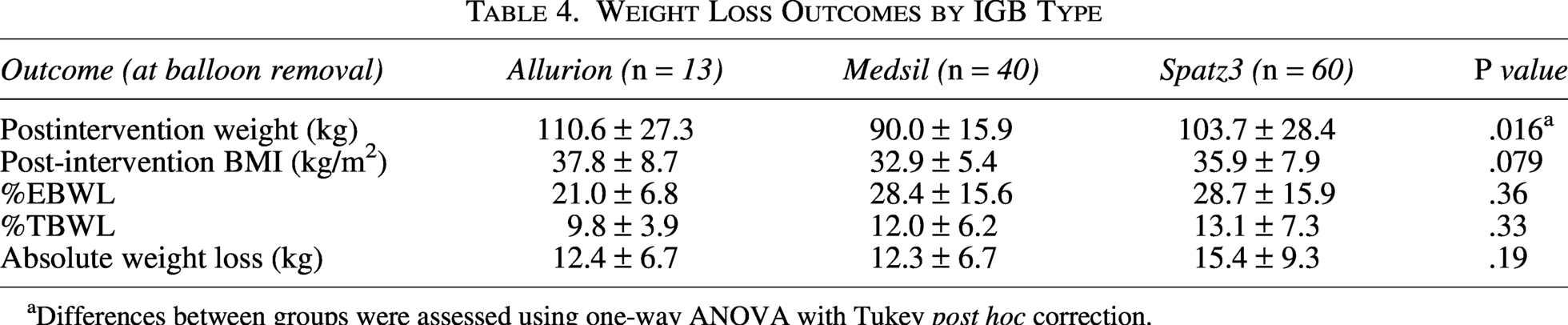
Differences between groups were assessed using one-way ANOVA with Tukey post hoc correction.
Postintervention body weight differed significantly across groups (P = .016), reflecting baseline differences rather than differential treatment effect as these values tracked the preintervention weight. Post hoc pairwise comparisons demonstrated greater post intervention weight in the Spatz3 group compared with Medsil (0.03), whereas differences between Allurion and Medsil (P = .07) and between Allurion and Spatz3 (P = .71) were not statistically significant. Percentage total body weight loss did not differ significantly among groups (P = .33).
Treatment tolerance and readmission
Premature balloon removal due to intolerance occurred in 12 patients (10.6%). Rates were comparable across devices as seen in Table 5. Hospital readmission occurred in five patients (4.4%), with no significant differences between balloon types.
Safety and Tolerability Outcomes

Discussion
IGBs are temporary, reversible, non-surgical interventions used as adjuncts in obesity management and are generally considered safe. 15 In this real-world cohort, we evaluated and compared the effectiveness and safety profiles of three commonly used fluid-filled intragastric balloons in Nigeria, including Medsil, Spatz3, and Allurion. Across all devices, clinically significant weight loss was observed. However, there was no statistically significant difference in primary weight-loss outcomes between balloon types.
The study population was predominantly female (91.2%), with a mean age of 34.9 years and a mean baseline BMI of approximately 40 kg/m2. This demographic pattern is consistent with prior reports from bariatric and endoscopic weight-loss programs, in which women are more likely to seek surgical and non-surgical obesity interventions.19–23
All balloon types were associated with comparable reductions in body weight by the end of the implantation period. Mean post intervention total weight loss ranged from approximately 12.3 kg to 15.4 kg across groups. Although patients treated with the Spatz3 balloon experienced numerically greater weight loss, approximately 3 kg more than those treated with Medsil or Allurion, this difference did not reach statistical significance. The findings indicate that Medsil, Spatz3, and Allurion balloons achieve comparable short-term weight loss with acceptable safety profiles in this population.
Percent EBWL ranged from approximately 21% to 28.7%, while total weight loss ranged from 9.8% to 15% across all balloon types. These outcomes are consistent with previously published data on fluid-filled intragastric balloons and support our findings.16,18,19,23–26 Notably, the magnitude of weight loss observed in this cohort is comparable to reports from other geographic regions, suggesting that short-term IGB effectiveness is broadly reproducible across diverse populations and healthcare settings.23,24,26
The Allurion balloon constituted the smallest subgroup, and patients receiving the Allurion balloon were older and had higher baseline body weight compared with those treated with Medsil or Spatz3 balloons. This difference likely reflects clinical selection patterns, as the procedureless nature of the Allurion balloon was preferentially considered for patients with higher perceived procedural or anesthetic risk and represents a useful option for patients in whom avoidance of sedation or endoscopy is a clinical priority. Device selection should therefore be individualized based on patient characteristics, procedural considerations, and shared decision-making rather than expectations of differential weight-loss efficacy.
Balloon intolerance leading to premature removal occurred in 10.6 percent of patients, with no statistically significant differences observed between balloon types. Similarly, 4.4% of patients required readmission for management of dehydration, nausea, or pain. These events are commonly reported during the early post-placement period of intragastric balloon therapy.26,27 The overall readmission rate observed in this study falls within and toward the lower end of ranges reported in prior real-world and clinical studies, which vary between 5% and 20% depending on patient selection, balloon type, and postprocedure care protocols.24,26–28 No major adverse events such as gastrointestinal perforation, obstruction, or mortality were observed.
No statistically significant associations were identified between premature balloon removal or intolerance and baseline patient characteristics, including age, sex, body weight, BMI, or presence of comorbidities. These findings suggest that intolerance may be influenced by factors not captured in this dataset, including early symptom management, visceral sensitivity, behavioral adaptation, or psychosocial factors.28,29
Limitations
This study has several limitations. Its retrospective, single-center design and non-randomized allocation introduce the potential for selection bias and residual confounding. Balloon choice was influenced by device availability, time period, and clinical considerations rather than standardized assignment as in a randomized controlled trial. Long-term outcomes following balloon removal were not systematically assessed, limiting conclusions regarding durability of weight loss. In addition, the smaller sample size of the Allurion subgroup reduces statistical power for detecting between-group differences, particularly for premature removal and major complications.
Despite these limitations, this study provides the first real-world comparative evaluation of three commonly used intragastric balloons in Nigeria and sub-Saharan Africa. Future studies should explore the integration of intragastric balloons with contemporary anti-obesity pharmacotherapy and standardized behavioral interventions to assess whether combined approaches improve durability and magnitude of weight loss. Also, a randomized controlled trial and long term follow up would provide more data to guide the use of these balloons in our environment.
Conclusion
In this real-world cohort, all three fluid-filled intragastric balloons evaluated in this study, namely Medsil, Spatz3, and Allurion, were associated with clinically meaningful short-term weight loss and acceptable safety profiles, with no statistically significant differences in weight-loss outcomes between devices. Rates of intolerance and readmission were comparable across balloon types and aligned with existing literature. These findings support the use of intragastric balloons as effective non-surgical options within multidisciplinary obesity management programs, with device selection guided by individual patient characteristics, procedural considerations, and shared clinical decision-making.
Authors’ Contributions
All authors meet the criteria for authorship and have approved the final version of the article. All authors agree to be accountable for all aspects of the work and ensure that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. A.T.A.: Conceptualization, methodology, data curation, investigation, writing (original draft), writing (review and editing), project administration, and supervision. O.W.A.: Methodology, data curation, writing (original draft), and writing (review and editing). N.C.B.-U.: Data curation, formal analysis visualization, and writing (review and editing). G.I.P.: Data curation and writing (review and editing). I.O.A.: Methodology, investigation, software, and writing (review and editing). S.I.A.: Conceptualization, methodology, and writing (review and editing). T.A.: Writing (original draft) and writing (review and editing).
Footnotes
Author Disclosure Statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
The author(s) received no financial support for the research, authorship, and/or publication of this article.