
Abstract
Background:
The role of routine preoperative upper gastrointestinal (GI) endoscopy in bariatric surgery remains controversial. This study aimed to evaluate the prevalence of endoscopic abnormalities and their impact on surgical decision-making.
Methods:
A retrospective analysis was conducted on 360 patients undergoing preoperative upper GI endoscopy prior to bariatric surgery. Demographics, GI symptoms, endoscopic findings, and subsequent changes in surgical planning were evaluated. Statistical analyses included chi-square and independent t-tests.
Results:
Of the 360 patients, 124 (34.4%) were symptomatic and 236 (65.6%) asymptomatic. Endoscopic abnormalities were detected in 215 patients (59.7%). These findings resulted in surgical plan modifications in 118 patients (32.8%).
Symptomatic patients had significantly higher rates of abnormal findings compared with asymptomatic patients (P < .001). Moreover, surgical modifications were significantly more frequent in symptomatic patients (51.6%) than in asymptomatic patients (22.9%) (P < .001).
Conclusions:
Although preoperative endoscopy detects a high rate of abnormalities in bariatric candidates, its clinical impact is predominantly observed in symptomatic patients. This suggests that while endoscopic abnormalities are common, their clinical relevance is predominantly confined to symptomatic patients. A selective, symptom-based approach may therefore be more appropriate than routine endoscopy for all patients.
Background
Obesity is a complex and rapidly growing global health problem associated with significant morbidity and mortality. 1 It is strongly linked to multiple comorbid conditions, including type 2 diabetes, cardiovascular disease, obstructive sleep apnea, and gastroesophageal reflux disease.2,3 Despite lifestyle interventions, sustained weight loss is often difficult to achieve, and bariatric surgery has become the most effective treatment for long-term weight reduction and metabolic improvement.4,5
A thorough preoperative evaluation is essential to optimize surgical outcomes and minimize perioperative risk. Upper gastrointestinal (GI) endoscopy is frequently incorporated into this assessment; however, its routine use in all bariatric candidates remains controversial. While several studies suggest that endoscopic findings rarely lead to changes in surgical management, others highlight its importance in identifying clinically significant conditions, such as severe esophagitis, hiatal hernia, peptic ulcer disease, or Barrett’s esophagus, which may alter surgical strategy.6–9
Despite extensive research, a critical gap persists regarding the clinical relevance of routine endoscopic findings, particularly in asymptomatic patients. Specifically, it remains unclear whether the high prevalence of detected abnormalities translates into meaningful changes in surgical decision-making.
Therefore, this study aimed to evaluate the prevalence of endoscopic abnormalities in bariatric surgery candidates, examine the relationship between GI symptoms and endoscopic findings, and determine the clinical impact of these findings on surgical decision-making. We hypothesized that, although endoscopic abnormalities are common, their clinical impact is predominantly limited to symptomatic patients.
Methods
This retrospective cohort study included 360 consecutive patients who underwent preoperative upper GI endoscopy prior to bariatric surgery between 2020 and 2023 at a single tertiary care center. All patients who were evaluated for bariatric surgery and underwent routine preoperative endoscopy were included in the study. Patients with incomplete clinical data or prior upper GI surgery were excluded.
Preoperative endoscopy was performed routinely as part of the institutional protocol. Demographic and clinical data, including age, sex, body mass index (BMI), and the presence of upper GI symptoms (gastroesophageal reflux, dyspepsia, epigastric pain or discomfort), were recorded. Endoscopic findings were categorized as gastritis, hiatal hernia, esophagitis, polyp, or ulcer.
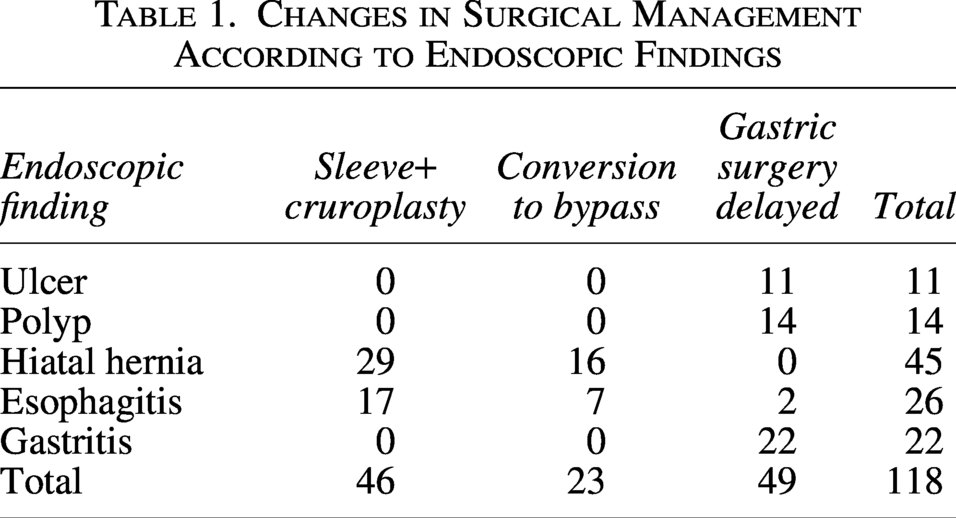
Surgical decision-making was performed by bariatric surgeons based on endoscopic findings and clinical presentation. Mild gastritis, Los Angeles grades A and B esophagitis, and hiatal hernias smaller than 1 cm were considered clinically regular findings because they did not lead to any complications in the planned bariatric procedure and were therefore not classified as clinically significant abnormalities in surgical decision-making analyses. Clinically significant findings, including severe esophagitis, large hiatal hernia, or peptic ulcer disease, were considered indications for modification of the planned surgical procedure, such as conversion to gastric bypass, addition of cruroplasty, or postponement of surgery. Among patients with gastric polyps, surgery was postponed until histopathological evaluation was completed to exclude neoplastic pathology. None of the polyps demonstrated malignant or premalignant features on final pathological examination. In patients with severe gastritis, surgery was temporarily deferred to allow appropriate medical treatment, with the aim of improving postoperative comfort and reducing symptom burden following bariatric surgery (Table 1).
Changes in Surgical Management According to Endoscopic Findings
The primary outcome of the study was the prevalence of clinically significant endoscopic abnormalities. Secondary outcomes included the impact of endoscopic findings on surgical decision-making and their association with patient characteristics such as age, sex, BMI, and the presence of upper GI symptoms.
Statistical analysis
The chi-square test was used for categorical variables, and independent t-tests were applied for comparisons between two groups (e.g., BMI < 40 versus ≥ 40 kg/m2). Statistical significance was set at P < .05.
A post hoc power analysis was performed using G*Power software (version 3.1.9.7; Heinrich Heine University, Düsseldorf, Germany), assuming a two-tailed test with an alpha level (α) of 0.05 and a moderate effect size (Cohen’s d = 0.5), based on previous literature. 10 Given the sample size of 360 patients, the calculated statistical power was 99.7%, indicating a high ability of the study to detect clinically meaningful differences.
Results
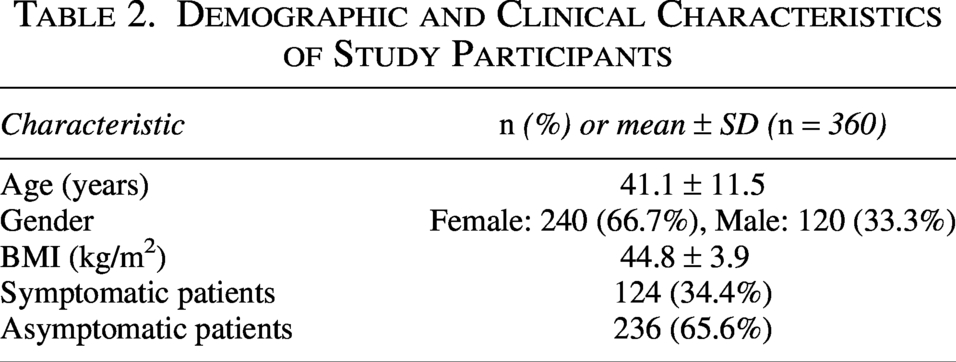
A total of 360 patients were included in the study, with a mean age of 41.1 ± 11.5 years. The cohort consisted of 240 (66.7%) female and 120 (33.3%) male patients. The average BMI was 44.8 ± 3.9 kg/m2. Furthermore, 34.4% of the patients exhibited upper GI symptoms, while 65.6% remained asymptomatic (Table 2). A total of 215 patients (59.7%) had at least one abnormal finding on preoperative endoscopy, the most common being gastritis (30.8%). The remaining patients had hiatal hernias (14.7%), esophagitis (12.2%), polyps (5%), or ulcers (3.1%). After exclusion of endoscopic findings deemed clinically insignificant and not expected to influence surgical planning, including mild-to-moderate gastritis, Los Angeles Grade A–B esophagitis, hiatal hernias <1 cm, and small mucosal protrusions, the rates of clinically relevant gastritis, hiatal hernia, esophagitis, polyps, and ulcers were 6.1%, 12.5%, 7.2%, 3.9%, and 3.1%, respectively (Table 3).
Demographic and Clinical Characteristics of Study Participants
Distribution of Clinically Relevant Endoscopic Findings Affecting Surgical Planning According to Symptom Status
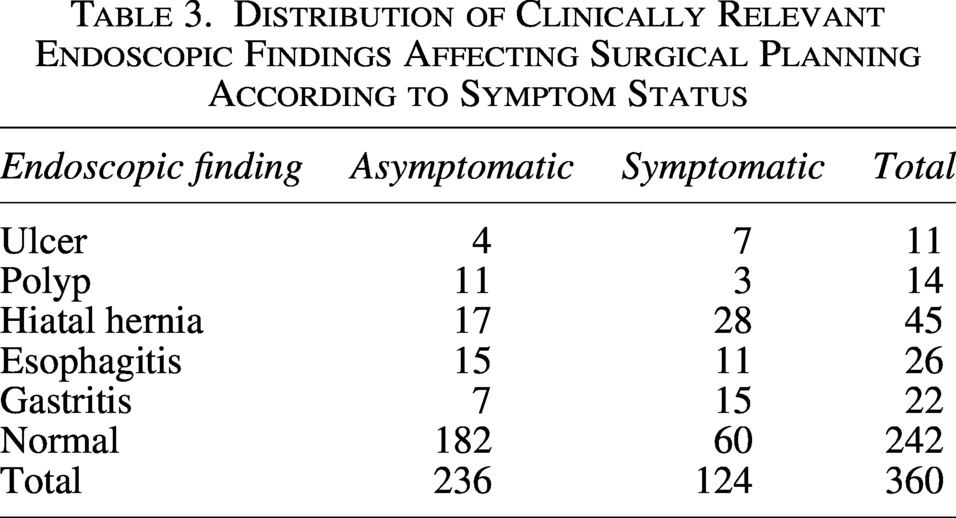
Chi-square analysis revealed a statistically significant association between the presence of GI symptoms and abnormal endoscopic findings (χ2 = 42.363, df = 5, P < .001). Symptomatic patients had significantly higher rates of gastritis, esophagitis, and hiatal hernia than asymptomatic patients did.
Surgical plan modifications were required in 118 (32.8%) patients. Among symptomatic patients, 64 of 124 (51.6%) underwent surgical changes due to endoscopic findings, compared with only 54 of 236 (22.9%) asymptomatic patients. This difference was statistically significant (χ2 = 30.455, P < .001).
The majority of surgical changes included switching to bypass procedures or adding cruroplasty to sleeve gastrectomy due to severe esophagitis or the presence of a hiatal hernia and postponement of surgery in ulcer cases. Symptoms are a strong predictor of whether endoscopic findings would alter the surgical approach.
Discussion
This study highlights the nuanced role of preoperative upper GI endoscopy in bariatric surgery candidates. Although a high overall prevalence of endoscopic abnormalities (59.7%) was observed, the clinical impact on surgical decision-making was largely confined to symptomatic patients. This distinction underscores a key finding: the detection of abnormalities does not necessarily translate into clinically meaningful changes in surgical management.
Consistent with previous studies,2,4 incidental findings such as gastritis, esophagitis, and hiatal hernia were frequently identified; however, these findings influenced surgical planning in only a subset of patients, particularly those presenting with upper GI symptoms. In our cohort, symptomatic patients had significantly higher rates of surgical modification compared with asymptomatic patients (P < .001). These modifications included conversion from sleeve gastrectomy to Roux-en-Y gastric bypass and the addition of cruroplasty to address reflux-related or anatomical abnormalities.
Our findings are in line with recommendations from major surgical societies, including the American Society for Metabolic and Bariatric Surgery 3 and the European Association for Endoscopic Surgery, 11 which support a symptom- and risk-based approach rather than routine screening. Notably, we found no significant association between BMI, age, or sex and the presence of clinically relevant endoscopic pathology, further emphasizing that symptomatology should guide preoperative evaluation.
While our results strongly support a selective screening strategy, it is important to consider opposing perspectives. Previous studies and meta-analyses have demonstrated that routine endoscopy can detect clinically significant conditions, including peptic ulcer disease, Barrett’s esophagus, and, rarely, early malignancies.12–15 These findings suggest that routine screening may serve as a safety measure, particularly in high-risk populations such as older individuals, smokers, or patients from regions with higher gastric cancer prevalence.
Additionally, recent multicenter studies have shown that even in asymptomatic patients, endoscopic findings may occasionally influence surgical strategy or postoperative surveillance. Although no malignancies were detected in our cohort—possibly due to the relatively younger mean age—this does not eliminate the potential value of routine endoscopy in selected populations.
Interestingly, the rate of surgical modification in our study (32.8%) was higher than that reported in previous literature.11,12 This variation may be attributed to institutional differences in clinical decision-making, endoscopic interpretation, and thresholds for modifying surgical plans. These findings highlight the importance of multidisciplinary evaluation and standardized clinical pathways.
Taken together, our results support a selective, symptom-based approach to preoperative endoscopy. In symptomatic patients, endoscopy frequently identifies findings that directly influence surgical planning or necessitate postponement. Endoscopy demonstrated a substantially higher clinical yield in symptomatic patients; however, clinically relevant endoscopic findings also influenced surgical planning in approximately one-quarter of asymptomatic patients. Therefore, the potential value of selective endoscopy should be interpreted with caution, as a meaningful proportion of asymptomatic patients may harbor findings that affect surgical management. From a clinical perspective, a tailored approach appears most appropriate. Preoperative endoscopy should be strongly considered in patients presenting with upper GI symptoms or other high-risk features. At the same time, routine screening of all bariatric candidates may identify clinically relevant abnormalities that could alter the planned surgical procedure. The potential benefits of routine endoscopy should therefore be balanced against its associated costs, procedural burden, and resource utilization. Future prospective multicenter studies are needed to develop validated risk-stratification models and to better define which patients are most likely to benefit from preoperative endoscopic evaluation.
Author’s Contributions
The author made significant contributions to the work reported, including conception, design, data acquisition and analysis, drafting or critically revising the article, approving the final version, and agreeing to be accountable for all aspects of this work.
Footnotes
Acknowledgment
The authors would like to thank the staff of the Endoscopy Unit, Sivas Cumhuriyet University Hospital, for their assistance during data collection.
Ethical Statement
This study was approved by the Ethics Committee of a University (approval number: 2024-10/40; date: 17.10.2024). All patients provided written informed consent before participation. This study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki.
Data Availability
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Author Disclosure Statement
The authors declare that they have no conflicts of interest.
Funding Information
No funding was received for this study.