
Abstract
Background:
Being the caregiver of a pediatric patient with a complex or serious illness can be emotionally intense and stressful. Caregiver burden significantly affects the biopsychosocial well-being of both the child and the caregiver. Interventions such as Narrative Medicine (NM) may help alleviate this burden by enhancing emotional resilience and strengthening support networks.
Objectives:
This review aimed to explore which NM interventions can reduce the emotional burden of caregivers of pediatric patients under the age of 18.
Methods:
A systematic literature review was conducted to examine the benefits of NM interventions on caregiver well-being. Primary studies were included if they described NM interventions involving active written narration by caregivers (e.g., diaries, digital writing). Studies relying solely on oral storytelling or third-party facilitation (e.g., interviews, dignity therapy) were excluded. Only studies in English or Italian were considered; studies focusing on adult patients or targeting the patient rather than the caregiver were excluded. The review followed PRISMA guidelines. A comprehensive search was conducted in MEDLINE, Embase, CINAHL, Cochrane Library, and APA PsycInfo in July 2024 with no time limits. Study quality was assessed using JBI and NIH tools, and data were synthesized narratively and in tables.
Results:
The search identified 1078 unique references. After screening, four studies met the inclusion criteria. Interventions ranged from narrative diaries in pediatric intensive care units to online journaling. All studies showed feasibility and acceptability, with reported benefits including emotional expression, perceived support, improved coping, and greater self-reflection. Most participants were women (85%), although the review included all caregivers regardless of gender.
Conclusions:
In conclusion, NM appears to be a promising tool to support caregivers of pediatric patients with complex or serious conditions. While preliminary findings are encouraging, further research is needed to assess long-term outcomes. Structured workshops and the involvement of NM facilitators may further support caregiver well-being and reduce psychological burden.
Introduction
Caring for children with serious illnesses is an emotionally demanding and highly stressful experience for parents, who report significantly higher levels of parental stress compared with those with healthy children (p ≤ 0.0001). 1 Serious illnesses, such as degenerative chronic conditions eligible for pediatric palliative care, require parents to devote significant physical and psychological effort to the care of their child, both in the daily management—such as caring for a gastrostomy, tracheostomy, or permanent central venous access—and in managing emergencies that may require repeated visits to emergency services, leading to longer or shorter hospitalizations that disrupt the delicate family balance. 2 Childhood hospitalization represents a particularly challenging period for parents, marked by intense stress and emotional burden. During these times, parents must cope not only with the hospitalization itself but also with the separation from other family members, disruptions to their work, limited personal time, and the challenges of adequately caring for their other children. 3 Additionally, parents often experience a deep sense of guilt and uncertainty about how to navigate the treatment process, particularly when faced with complex diagnostic situations. 4 This stress can, in turn, contribute to caregiver burden, which may negatively affect parents’ health 5 and lead to psychological consequences for children, suggesting that parental stress may also interfere with the management of the child’s chronic illness.6,7
Caregiver burden, a concept first introduced by Hoenig and Hamilton, 8 was categorized into subjective burden, relating to caregivers’ personal feelings during caregiving, and objective burden, referring to negative caregiving experiences. Zarit et al. 9 further defined burden as the perceived impact of caregiving on emotional, physical, social, and financial health, while Collins et al. 10 associated it with psychological distress, physical health problems, financial and social strain, family conflicts, and feelings of despair. 11 To date, the literature supports the hypothesis that caregiver burden is a complex concept due to its multidimensional nature, characterized by three key attributes: the caregiver’s self-perception, its multidimensional structure, and its close connection with the dynamic nature of caregiving over time, including experiences of change and overload. 12
Psychosocial needs due to the emotional and physical demands of caregiving are effectively addressed by Narrative Medicine (NM), which serves as a valuable intervention by focusing on the patient as a whole person rather than merely their symptoms or medical condition. According to the National Institute of Health’s (ISS) 2015 guidelines, 13 NM is defined as a methodology that integrates patient narratives and the communication skills of health care professionals to enhance the quality of care. These guidelines emphasize NM’s potential to foster a more compassionate and holistic approach to care by acknowledging the emotional and social experiences of both patients and caregivers. Using skills such as active listening, empathy, and compassion, NM helps caregivers and health care professionals gain a deeper understanding of the illness experience, thus enabling them to build more meaningful therapeutic relationships. Furthermore, by focusing on illness narratives, NM interventions offer caregivers a platform to share their personal experiences, which can not only alleviate stress but also enhance their sense of agency and strengthen their support network. 14 Therapeutic writing sessions provide a space for caregivers to express their emotions, share their perspectives, and make sense of their reality, fostering greater emotional resilience and well-being. 14
While various studies have explored NM’s potential in different health care areas, 14 a comprehensive review focusing on its benefits for women caregivers—especially those of pediatric patients—has yet to be conducted, revealing a significant gap in research. This underscores the need for further exploration of this topic.
This systematic review seeks to answer the research question: “To what extent can NM interventions impact the caregiving burden experienced by caregivers of pediatric patients with complex or serious illnesses?” To address this question, a comprehensive systematic literature review was conducted to describe the potential benefits of NM interventions on the well-being of caregivers of pediatric patients with serious illnesses.
Methods
This systematic review was reported following the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement guidance. Preliminary searches of the main databases did not identify any existing or ongoing systematic reviews with this aim. The study protocol was previously registered on PROSPERO (registration number CRD42023483113).
Eligibility criteria and search strategy
This review included all primary studies with the following inclusion criteria:
Types of participants: caregivers of pediatric patients (0–18 years); Types of intervention: Only interventions involving active written narration by caregivers were included (e.g., diaries, digital writing). Interventions relying solely on oral storytelling or third-party facilitation (e.g., interviews, dignity therapy) were excluded. Narration remains the fundamental tool for acquiring, understanding, and integrating the different perspectives of those involved in the illness and care process;
13
Among the included studies, Grossoehme et al.
15
involved a NM Facilitator who proposed optional prompts and reflective materials; however, the narration was always produced directly by the caregivers themselves, aligning with the defined inclusion criteria. Types of outcomes: Caregiver burden defined as the strain or load borne by someone caring for a family member with a chronic illness.
11
Exclusion criteria included studies that were not published in English or Italian, studies utilizing NM interventions for patients rather than caregivers, and studies focused on caregivers of adult patients (>18 years old).
A comprehensive bibliographic search was performed on the PubMed, Embase, CINAHL, Cochrane Library, and APA PsycInfo databases in July 2024 with no time limits. Medical subject headings and free-terms were searched for the following keywords: pediatric caregiver, NM, caregiver burden (Appendix 1). Search strategies were checked by two reviewers (G.F. and A.S.).
Study selection and data collection
Study screening was conducted independently by two reviewers (A.S. and G.F.) using the “Rayyan” 16 application. First, titles and abstracts and then full-texts selected from the first round were reviewed based on the inclusion criteria. To maximize search sensitivity, a snowball method was used and the reference lists of the full-texts included were screened. Conflicts regarding study inclusion were resolved by mutual agreement between reviewers; if necessary, a third author was consulted (F.M.). The data from the full-texts selected were extracted independently by two authors (A.S. and G.F.) and checked by a third author (F.M.). The data were extracted from all included studies using a custom Microsoft© Excel© spreadsheet. The extracted data included the first author, year of publication, country, sample (clinical setting, patient age, and pathology), description of the intervention, intervention outcomes, and quality assessment tool used with scores.
Quality assessment
Two reviewers independently assessed the methodological quality and reliability of the findings using appropriate qualitative appraisal tools, including the Joanna Briggs Institute (JBI) “Critical Appraisal Checklist for Qualitative Research” 17 and the National Institutes of Health (NIH) tools, specifically the “NIH Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies” 18 and the “NIH Quality Assessment of Controlled Intervention Studies.” 19
The JBI Critical Appraisal Checklist for Qualitative Research is a tool developed by the JBI to assess the methodological quality of qualitative studies. It includes 10 criteria that examine aspects such as the clarity of the research question, the adequacy of the methodology, critical reflection on biases, the rigor of data analysis, and ethical implications.
The NIH Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies is a tool developed by the NIH to assess the methodological quality of observational cohort and cross-sectional studies. It includes 14 criteria that evaluate aspects such as the clear definition of the population and exposure, the accurate measurement of variables, the control of confounders, and the completeness of follow-up. 18
The NIH Quality Assessment Tool for Controlled Intervention Studies is a tool developed by the NIH to assess the methodological quality of controlled intervention studies, including randomized clinical trials. It includes 14 criteria that evaluate aspects such as randomization, the description of study groups, the level of blinding, the control of confounders, and the completeness of follow-up. 19
Data synthesis and analysis
Based on the guidelines outlined in the Cochrane Library manual, 20 the data from the included studies were synthesized narratively. The results were presented both in tables and within the text. To address the research question specifically, the results were organized by type of outcome. An in-depth descriptive statistical analysis was conducted, which involved calculating the mean, percentages, and frequencies to provide a comprehensive overview of the data distribution and patterns.
Results
Study selection
The bibliographic search in the databases identified 1078 unique references, of which 344 were eliminated due to duplicates. Of the 734 potentially relevant articles, 726 were excluded after reading the title and then the abstract. One article was added through manual search. Of the nine potentially relevant articles, five were excluded after reading the full text, as they did not meet the inclusion criteria. Finally, four studies were included in the review. The details of the study selection process are provided in Figure 1, which illustrates the study flow diagram according to PRISMA.
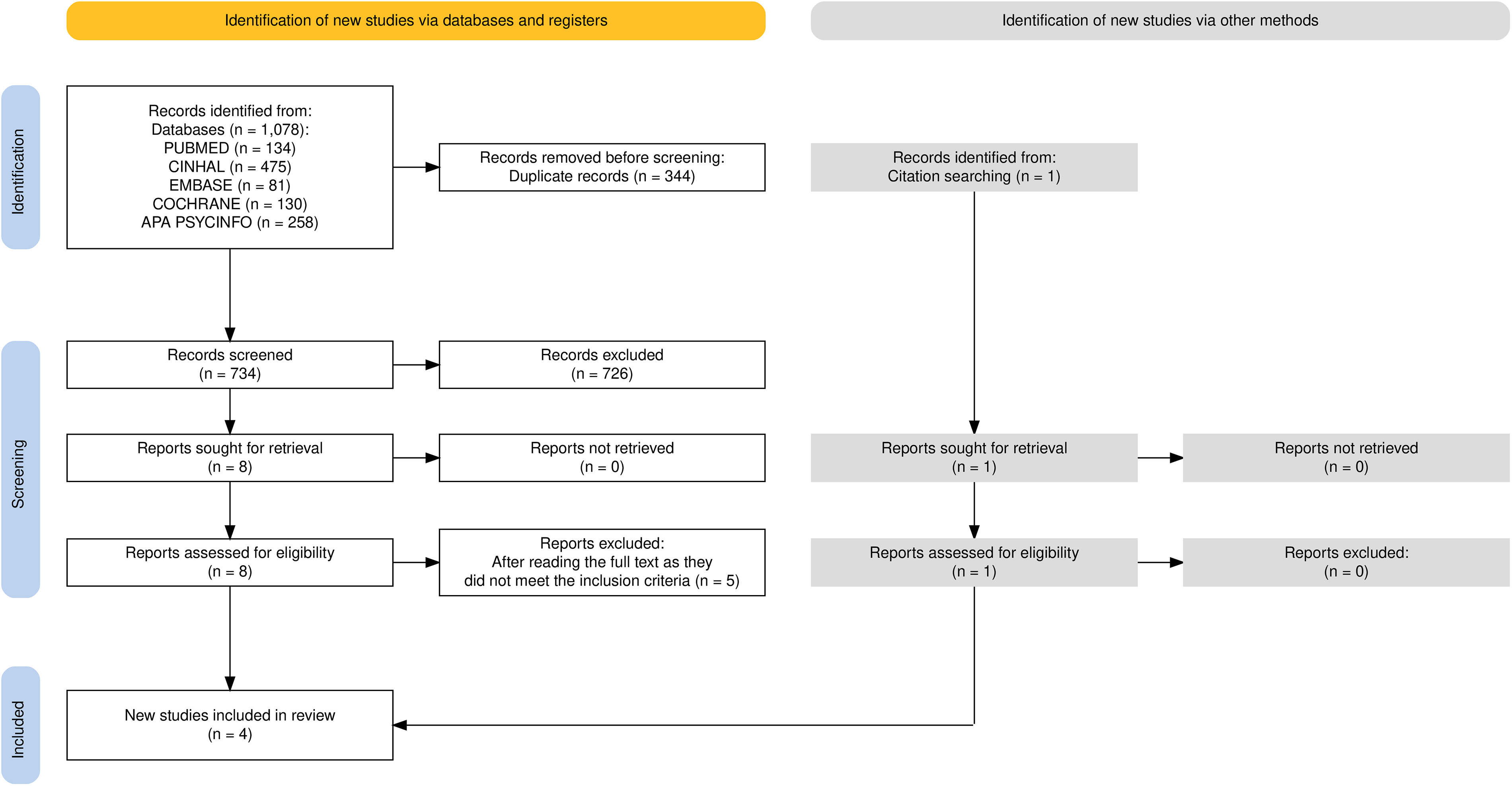
Flow chart of study selection according to PRISMA 2020 guidelines.
Quality assessment
The quality assessment of included studies is illustrated in Table 1.
Data Extraction Table with Qualitative Assessment of the Analyzed Studies
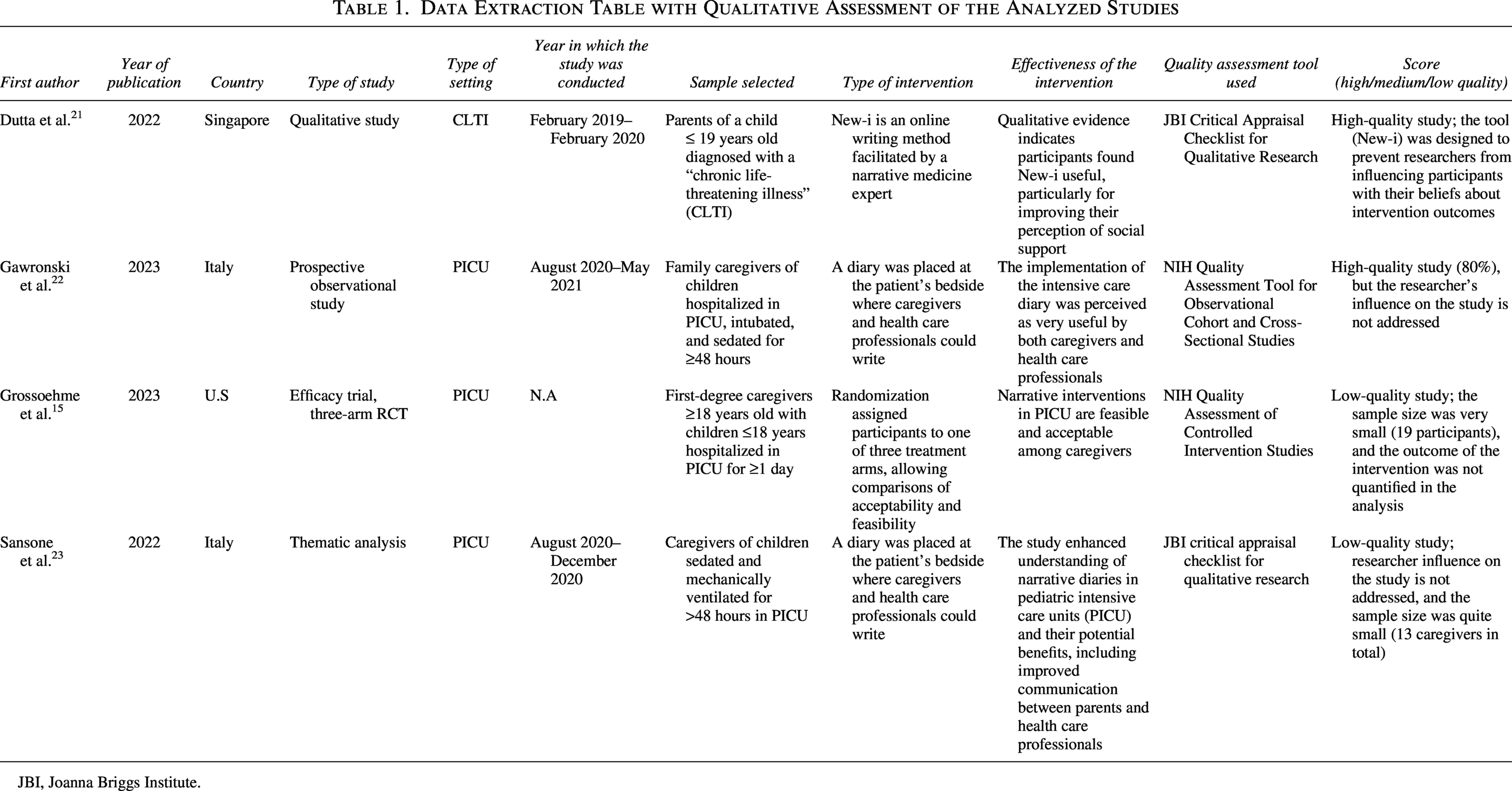
JBI, Joanna Briggs Institute.
The studies by Sansone et al. 23 and Dutta et al. 21 were both evaluated using JBI tools, specifically the “Critical Appraisal Checklist for Qualitative Research.” The first study was rated as low quality because the influence of the researcher on the study was not addressed, and the sample size was rather small (13 caregivers). In contrast, the second study by Dutta et al. was considered of high quality because the potential researcher bias was mitigated by conducting the intervention through an online application. For this reason, the study by Dutta et al. was rated as high quality. The two other studies examined, Gawronski et al. 22 and Grossoehme et al. 15 were assessed using the NIH tools, specifically the “NIH Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies” and the “NIH Quality Assessment of Controlled Intervention Studies.” Using these tools, the study by Gawronski et al. was rated as medium quality because the influence of the researcher was not addressed in the study, and there was no description of statistical power or estimates of variance and effects of the tested intervention. Regarding the last study reviewed, Grossoehme et al., the assessment was rated as low quality because the sample on which the intervention was tested was very small (19 participants). Additionally, the assessment of the intervention did not include comparative outcome measurements, such as using assessment scales to quantify the burden before or after the intervention or to assess any changes in the perception of the hospitalization of a loved one.
Study and sample characteristics
All the studies were published in English in peer-reviewed journals from 2021 and 2023 (Table 1). Two of these were conducted in Italy, namely the study by Gawronski et al. and Sansone et al., while the study by Grossoehme et al. was conducted in the United States, and the study by Dutta et al. was conducted in Singapore. In total, there were 79 caregivers involved in the NM intervention across the 4 studies reviewed. Of these, 67 (85%) were female and 12 (15%) were male, highlighting a greater participation of females compared with males. Caregivers had an average age of 41.9 years for men, while for female caregivers, it was 38.9 years. They came from Italy (N = 53; 67%), China (N = 17; 22%), India (N = 3; 4%), Malaysia (N = 4; 5%), and 2 caregivers did not specify their ethnicity. The level of education and employment status were reported in Dutta et al. and Gawronski et al. as follows: 13 (20.9%) caregivers had postgraduate education; 24 (38.7%) caregivers had a university degree; 6 (9.7%) caregivers had completed high school, including 5 (8.1%) with a polytechnic diploma and 1 (1.6%) with a vocational diploma; 13 (20.9%) caregivers had completed middle school; one caregiver (1.6%) had completed elementary school; and 5 (8.1%) caregivers did not specify their level of education. Regarding employment status, 22 (35.5%) caregivers were full-time employees,9 (14.5%) women and 13 (20.9%) men; one (1.6%) female caregiver worked part-time; 11 (17.7%) were self-employed, 4 (6.4%) women and 7 (11.3%) men; 21 (33.8%) caregivers were unemployed, 19 (30.6%) women and two (3.2%) men; and 7 (11.3%) women did not specify their type of employment (Table 2).
Description of the Caregiver: Gender, Average Age, Ethnicity, Level of Education, Employment Status
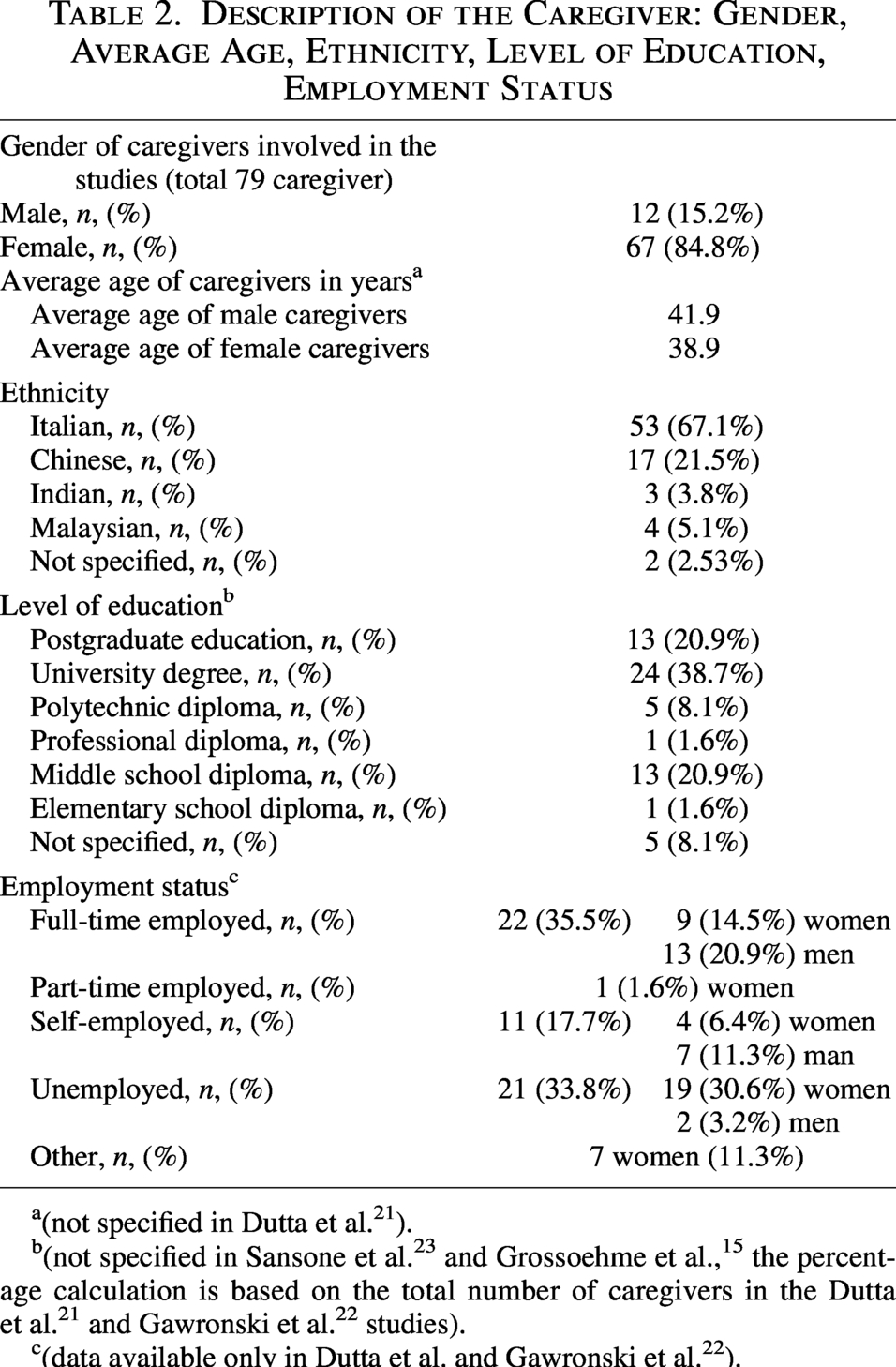
(not specified in Dutta et al. 21 ).
(not specified in Sansone et al. 23 and Grossoehme et al., 15 the percentage calculation is based on the total number of caregivers in the Dutta et al. 21 and Gawronski et al. 22 studies).
(data available only in Dutta et al. and Gawronski et al. 22 ).
There were 30 male and 23 female pediatric patients, with an average age of 7.6 years. In the studies by Sansone et al., Gawronski et al., and Grossoehme et al., patients were admitted to the intensive care unit for the following reasons: trauma (9 patients), neurological disorders (10 patients), respiratory diseases (14 patients), oncological diseases (5 patients), metabolic disorders (1 patient), infections (2 patients, unspecified), cardiovascular diseases (6 patients), 3 patients undergoing emergency dialysis, and 3 patients requiring extracorporeal membrane oxygenation. In Dutta et al.’s study, patients with chronic conditions and a reduced life expectancy had the following conditions: cerebral palsy (3 patients), neurodegenerative diseases (3 patients), epilepsy (1 patient), rare genetic diseases (5 patients), neuromuscular diseases (1 patient), renal diseases (2 patients), and one patient with an unspecified condition (Table 3).
Characteristics of Patients Included in the Systematic Review
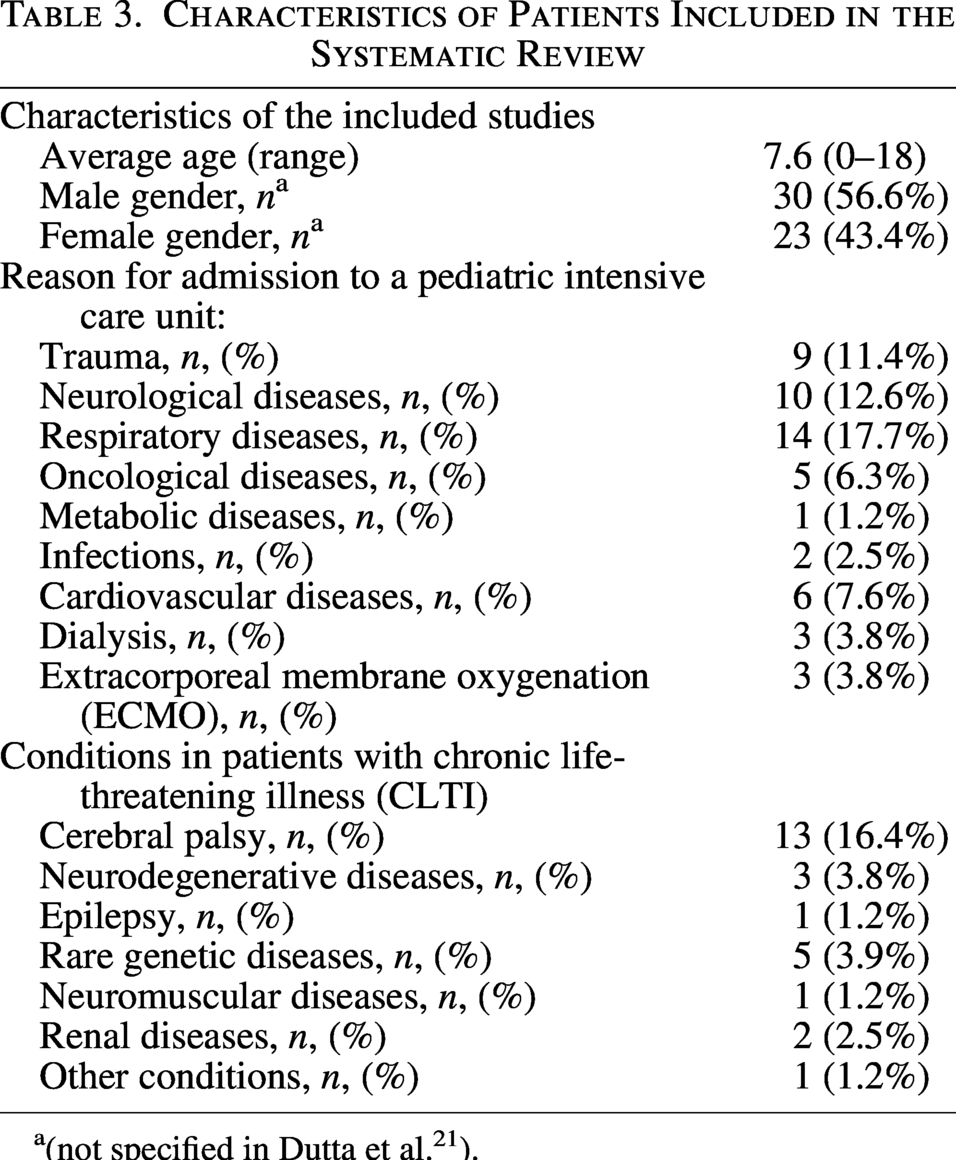
(not specified in Dutta et al. 21 ).
Intervention characteristics
In the study by Gawronski et al., conducted in a pediatric hospital between August 2020 and May 2021, the researchers tested the use of a narrative diary placed at the patient’s bedside. Caregivers and health care professionals could write their thoughts in this diary. The outcome of the intervention was evaluated one month after the hospital admission through direct phone interviews with both caregivers and health care professionals, as well as through analysis of the written texts. The data were then analyzed both quantitatively, in terms of categorical proportions, variables, means, and medians, and qualitatively, by grouping the main themes into different categories.
Dutta et al. implemented a pilot intervention using NeW-I, a narrative intervention facilitated by a trained therapist and conducted through a smartphone application, focusing on preventing caregiver burden for family members caring for children with “Chronic Life-Threatening Illness.” NeW-I was tested in an open-label, randomized controlled, two-arm study, with an intervention group (participants engaged in an online journaling exercise following the structured NeW-I protocol) and a control group (participants involved in an online journaling exercise not related to the child’s condition or the caregiver role).
Grossoehme et al. conducted a randomized trial without a control group to assess the feasibility and acceptability of an NM intervention for caregivers of patients admitted to a pediatric intensive care unit (PICU). Participants were randomly assigned to one of three treatment arms, allowing comparisons of acceptability and feasibility. The groups were divided as follows: in arm 1, participants were encouraged to write on a paper-based medium without any prompts; in arm 2, participants received a booklet with writing suggestions created by the NM facilitator (NMF). In arm 3, participants received an optional 30–60 minute weekly session, during which a text selected by the NMF (poetry/short prose) was read, discussed, and followed by an optional writing prompt created individually. Participants were invited to read their writings aloud in the presence of the facilitator and were then encouraged to write independently.
Finally, Sansone et al. conducted a qualitative study on the use of narrative diaries within PICU. A narrative approach was used for the research. During the child’s hospitalization in the PICU, family caregivers, relatives, friends, and health care professionals were invited to record events, thoughts, messages, and attach drawings/images for the child in the narrative diary placed at the patient’s bed. A thematic analysis of the diary contents was then performed.
Synthesis of findings
The themes presented in this section reflect recurrent patterns reported within the included studies. These thematic patterns derive from the authors’ analyses in the primary articles; no additional thematic analysis was conducted by the review team.
Across the four included studies, four recurrent thematic patterns were identified: (1) emotional expression and processing; (2) perceived social and spiritual support; (3) coping and adaptation to hospitalization; (4) acceptability and feasibility of narrative interventions.
Emotional expression and processing
All studies reported that narrative tools supported caregivers in expressing complex emotions such as fear, sadness, hope, and gratitude. This theme was particularly evident in the diary-based interventions used in pediatric intensive care units, where caregivers were encouraged to externalize their experiences through writing and reflection15,22,23
Perceived social and spiritual support
In the studies by Sansone and Dutta, caregivers highlighted a strengthened sense of social connection and spiritual well-being. Writing provided not only a space for introspection, but also a way to feel less alone, improving caregivers’ sense of support and meaning-making during care.21,23
Coping and adaptation to hospitalization
Several caregivers described the narrative interventions as useful tools to reinterpret their experiences in the hospital setting. For example, Gawronski and Grossoehme reported that caregivers used narrative tools to process the stressful environment of the PICU and to develop a more constructive and hopeful perspective.15,22
Acceptability and feasibility
All studies confirmed the overall feasibility and high acceptability of NM interventions. Participants expressed a willingness to recommend the experience to others and appreciated the emotional and reflective benefits. At the same time, some limitations were noted—especially in digital interventions—regarding time constraints and emotional isolation, which could reduce sustained engagement15,21
These recurring themes suggest that NM interventions can address multiple dimensions of caregiver burden, helping participants process their emotional experience, increase their resilience, and feel supported both emotionally and spiritually.
Benefits of NM for Caregivers of Pediatric Patients
Across the 4 studies analyzed, a total of 79 caregivers participated in the NM intervention, of whom 67 were women (85%), and 12 were men (15%).
Feasibility and acceptability studies of NM interventions with women caregivers of pediatric patients yielded positive outcomes, demonstrating the potential for emotional and reflective support. Dutta et al. highlighted how online narrative writing through the NeW-I app provided a significant opportunity for reflection, aligned with caregivers’ needs, and proved compatible with their daily responsibilities. However, caregivers faced challenges completing weekly writing sessions in a single 30-minute sitting, suggesting the need for features like a “Pause” button and “Save as Draft” to improve usability and long-term implementation. In addition, over 85% of participants agreed that NeW-I was helpful in improving their spiritual well-being and hope for the future (52%), enhancing their perception of social support, which was the greatest benefit of the intervention (76%), and reducing feelings of sadness and depression (62%).
Gawronski et al. also reported similar results, with all caregivers describing the diary in the PICU as a helpful tool for reducing caregiver burden and expressing a willingness to recommend the intervention to other families. Three parents suggested extending the use of the narrative diary even after their children were discharged from the PICU and admitted to a regular ward to maintain continuity during hospitalization. For most parents (n = 14; 78%), the diary offered a unique opportunity to express their feelings and concerns, and 11 caregivers reported that the diary helped positively transform their perception of their child’s PICU admission.
Grossoehme et al. confirmed the high acceptability of NM interventions, as caregivers scored an average of 39.5 out of 42 on the modified “Treatment Acceptability Questionnaire.” Despite the high acceptability, no significant differences were observed among the three intervention groups. However, the study’s quality was considered low due to the lack of clear measurement of the intervention’s impact on caregiver burden.
Sansone et al.’s thematic analysis of diaries completed in the PICU highlighted the key benefits of NM for caregivers, including enhanced social and spiritual support, emotional processing (such as expressing pain, fear, hope, and the desire to connect with their child), and better coping with the PICU routine through engagement in activities and improved relationships with health care providers.
Discussion
This study explored the impact of NM on the psychological and emotional well-being of caregivers of pediatric patients with complex chronic conditions, focusing on the use of narrative tools to support them in hospital settings. Although the results of the studies included in the review are recent (from 2021 to 2023), NM in this field is an emerging topic, demonstrating how this approach is gaining attention in the scientific literature.
One of the most salient aspects emerging from these studies is the predominance of women among caregivers, who accounted for approximately 85% of participants. This finding aligns with previous research indicating that the caregiving burden often falls disproportionately on women, 3 with significant repercussions for their mental, physical, and social well-being.24,25 Nevertheless, the predominance of female participants in the included studies may also reflect recruitment bias rather than the actual distribution of caregiving responsibilities. Fathers’ experiences remain underexplored and may involve distinct challenges, such as balancing employment, supporting their partners, and participating in their child’s care, that are insufficiently represented in current research. Future studies should include more diverse samples to provide a more comprehensive understanding of caregiving dynamics.
Two of the four studies included were conducted in Italy, within the same hospital, highlighting particular attention to managing the caregiver burden and the willingness to explore new methodologies to support them more effectively. These studies, conducted by Gawroski et al. and Sansone et al., confirm the effectiveness of NM in the context of PICUs, with positive results regarding the possibility of expressing emotions through narrative journaling and suggestions from participants to extend the intervention even after discharge or transfer to other post-acute wards. In both studies, caregivers used the journals independently. Although none of the included studies tested this approach, future research could explore the potential role of a NM facilitator (NMF) to support more structured writing experiences and foster the sharing of caregivers’ narratives. Since not all caregivers may feel comfortable expressing emotions through writing, we hypothesize that the presence of an NMF could enhance participation and emotional safety—though this remains to be empirically tested. 26
Grossoehme et al.’s study also tested the effectiveness of NM interventions in a PICU. It emerged that narrative interventions in PICUs are feasible and acceptable to caregivers and differ from the “ICU diaries” used in adults, which are often used by patients themselves to reconstruct the hospitalization period after a critical event with prolonged sedation. 27
A common limitation in the three narrative writing experiences in the PICU is the short duration of the hospital stay: once patients are stabilized, they are transferred to postacute units, making it difficult to continue using the journal. 28
Dutta et al.’s study, which explored the use of online narrative writing for caregivers of pediatric patients with limited life expectancy, offered interesting insights into the dynamics of individual writing in digital contexts. Although individual writing through an app can offer an opportunity for reflection and was generally appreciated by caregivers, this method risks being depersonalizing, leaving the participant isolated and without the necessary emotional support. The lack of social interaction and emotional connection with others could fail to provide a significant reduction in psychological burden, as the solitary writing process does not offer the opportunity to share emotions, experiences, or difficulties with others in the same situation. 29
In general, NM emerged as a valuable approach to enhancing communication and emotional awareness among caregivers, thereby supporting better management of emotions and stress. However, the methodological challenges highlighted suggest that further research is needed to fully understand its long-term effectiveness. Implementing NM workshops, even in an online-synchronous format, could help reduce both emotional burden and the creation of a support network among participants, promoting a virtuous circle of mutual self-help. Often, families of children with complex chronic conditions find themselves increasingly isolated from their social and family contexts, and guided sharing could provide significant support. 30
Consideration of cultural contexts
The four included studies were conducted in Italy, Singapore, and the United States—contexts with distinct health care systems, family dynamics, and cultural norms around caregiving and emotional expression. As Charon (2006) emphasized, the interpretation and impact of illness narratives are inherently shaped by cultural and social factors. These differences may influence how caregivers engage with NM interventions and what kinds of narrative practices are most meaningful or effective. 31 Future studies should consider culturally sensitive adaptations to ensure the relevance and acceptability of NM approaches in diverse populations.
Limitations
This review has several limitations. First, the number of studies included was limited (only four), which may reduce the generalizability of the findings. Second, the heterogeneity in the type of interventions, outcome measures, and study populations made it difficult to perform a meta-analysis. Third, some of the studies included had low or medium methodological quality, further limiting the strength of the conclusions drawn.
Future directions
The limited number of eligible studies highlights a broader gap in the literature regarding structured and evaluable NM interventions targeting pediatric caregivers. Future research should address the lack of standardized approaches, insufficiently disaggregated caregiver data, and the limited focus on long-term outcomes and caregiver–clinician dynamics. Moreover, it is essential to promote such interventions, as parental stress—widely discussed in the literature—is a crucial factor that significantly affects both caregiver well-being and the health of the assisted child.
Another important aspect that emerged is the potential role of Narrative Medicine facilitators (NMFs), who could enhance the effectiveness of interventions by fostering greater caregiver engagement in the process. The involvement of a NMF may warrant further investigation as a strategy to improve the structure and sustainability of such interventions; however, this remains a theoretical consideration, as none of the included studies specifically evaluated this component. Additionally, integrating other narrative forms, such as visual arts or music, could help better address the diverse expressive needs of caregivers.
The use of online platforms for narrative writing demonstrated promising results, particularly in terms of increased perceived social support and reduced negative emotions such as sadness and depression. Nevertheless, challenges in time management and the impersonal nature of these platforms may limit user engagement. Therefore, future studies could explore ways to improve these platforms by incorporating interactive features that foster connection and peer support among caregivers.
Finally, NM may also hold particular promise within pediatric palliative care settings, where caregiver involvement is especially intense and characterized by frequent hospitalizations and the management of complex chronic conditions. Implementing NM workshops, even in synchronous online formats, could help reduce caregiver burden and facilitate the creation of mutual support networks, fostering a virtuous cycle of shared understanding and emotional resilience.
Conclusions
NM appears to be a promising approach to supporting the emotional well-being of caregivers of pediatric patients with complex or serious illnesses. The included studies indicate that narrative tools, such as diaries and reflective writing, are generally well-received and can help caregivers express emotions, manage anxiety, and strengthen resilience. Preliminary evidence suggests that NM interventions may enhance communication, emotional awareness, and coping within the caregiving experience. However, the current literature remains limited in number, scope, and methodological rigor. Further high-quality studies are required to confirm these preliminary findings and to better define the role of NM in supporting caregivers in pediatric health care settings.
Authors’ Contributions
A.S. and G.F. developed the study concept and design. A.S. and G.F. independently screened articles and performed data acquisition. F.M. resolved discrepancies as the third reviewer. A.S., F.M., and M.S. analyzed and interpreted the data. A.S. and G.F. drafted the article with input from all authors. G.F. and E.T. supervised the study and contributed with a critical review. All authors meet the authorship criteria stated by the International Committee of Medical Journal Editors.
Footnotes
Author Disclosure Statement
The authors declare no conflicts of interest in connection with this article.
Funding Information
No external funding was received for the conduct of this study.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.