
Abstract
Background:
Although racial and ethnic disparities in serious illness conversations have been documented, the experiences of racially and ethnically marginalized patients in nurse-led conversations remain underexplored.
Aim:
To explore racially and ethnically marginalized patients’ experiences of nurse-led serious illness conversations and their engagement in discussions about goals and future care.
Design:
A mixed-methods convergent study using surveys and semi-structured interviews.
Setting/Participants:
Racially and ethnically marginalized patients ≥18 years old from a single U.S. health care system.
Measurements:
The Advance Care Planning Engagement Survey, Serious Illness Conversation Patient Experience Survey, and semi-structured interviews.
Results:
Fifteen patients participated in the study. Participants felt confident engaging in advance care planning (mean: 4.35/5.00) but were less ready to act (mean: 3.40/5.00). Nearly half reported that nurse-led serious illness conversations increased hopefulness about their quality of life, closeness with the nurse, sense of control over medical decisions, and understanding of their future health. The mean “heard and understood” score was 3.00, indicating that nurse-led conversations moderately helped participants feel heard and understood. Integrated analysis showed that nurse-led serious illness conversations supported participants feel comfortable and confident engaging in discussions about their goals and future care. Nurse-led conversations also helped foster a better understanding of participants’ future health. However, confidence did not translate into readiness in the context of multifaceted distress.
Discussion:
Nurse-led serious illness conversations facilitated greater confidence among racially and ethnically marginalized patients to discuss their goals and future care and fostered understanding of their future health; however, additional support is needed to address multifaceted distress affecting readiness.
Key Message
Among racially and ethnically marginalized patients, nurse-led serious illness conversations facilitated confidence in discussing their goals and future care and fostered understanding of their future health. However, interdisciplinary collaboration to address multifaceted distress, along with expanded nurse training in serious illness communication, is needed to support readiness.
Introduction
Serious illness conversations are structured discussions that include sharing prognostic information, eliciting preferences, understanding fears and goals, exploring trade-offs, and clarifying desired family involvement. 1 They are associated with greater concordance between patient wishes and care received, less use of nonbeneficial life-sustaining treatment, reduced family distress, and lower health care utilization.2–11 However, only one-third of patients in their last year of life report having serious illness conversations, and they often occur too late in the illness trajectory.2,7–11
Clinicians at our study sites have participated for more than a decade in system-wide serious illness conversation training, 11 which includes an evidence-based conversation guide, clinician training, systematic patient identification, an electronic medical record documentation module, and ongoing coaching.1,12–15 Since 2013, we have worked with the Integrated Care Management Program, which supports complex patients and trains clinicians such as registered nurse care coordinators, social workers, and primary care physicians to conduct serious illness conversations as part of primary palliative care.
Studies show that the program leads to earlier and higher-quality conversations and reduces patient anxiety and depression.2,11 Nurses are well-suited to lead serious illness conversations given their expertise in care coordination, relationship building, and interdisciplinary collaboration.16–22 Prior studies have used nurse-led approaches to facilitate early serious illness conversations, which increased advance care planning (ACP) documentation and showed mixed effects on readiness to engage.23,24 For example, nurse-led serious illness conversations in emergency departments increased documentation of values and goals but did not improve patients’ readiness to engage in ACP. 23 A collaborative care model–based intervention involving nurse- and social worker–led serious illness conversations for patients with advanced cardiopulmonary disease improved readiness to engage in ACP. 24 A recent study found no racial differences in readiness to engage in ACP among seriously ill non-Hispanic Black and non-Hispanic White older adults; however, predictors of readiness varied across groups. 25 Furthermore, our prior work examining nurses’ perspectives on conducting serious illness conversations with racially and ethnically marginalized patients emphasized the importance of addressing unmet needs. 22
However, the perspectives of racially and ethnically marginalized patients on nurse-led serious illness conversations remain underexplored,26–30 despite persistent disparities in end-of-life care, hospice utilization, and quality of conversations about values and care preferences.21,26,31–34 We conducted a mixed-methods study to explore racially and ethnically marginalized patients’ experiences of nurse-led serious illness conversations and their engagement in discussions about goals and future care.
Methods
Study design
This mixed-methods convergent study was conducted between July 2021 and June 2022 at four sites within a large health care system located in Greater Boston. We used mixed methods to explore patient engagement and readiness to discuss goals and future care through surveys and patients’ experiences with nurse-led conversations through semi-structured interviews. Quantitative and qualitative data were collected in parallel with equal priority, and findings were integrated to provide a more comprehensive understanding of patient experiences with nurse-led serious illness conversations. Constructs and measures are summarized in Supplementary Data S1. This study received approval from the Institutional Review Board, and reporting followed the Good Reporting of a Mixed Methods Study and the Consolidated Criteria for Reporting Qualitative Research (Supplementary Data S3 and S4).35,36
Study participants and recruitment
Adults aged ≥18 years who had received a nurse-led serious illness conversation within the prior three months were eligible if they self-identified as Black, Hispanic/Latino, or Native American and Alaska Native patients and spoke English, Spanish, or Haitian Creole. Nurse-led conversations were conducted by either Integrated Care Management Program registered nurse care coordinators or palliative care nurse practitioners, in person or virtually. We used purposive sampling to capture a range of experiences across gender, race and ethnicity, and preferred language. Eligible patients were identified through a serious illness conversation dashboard and referrals from nurse care coordinators. Study staff mailed recruitment letters and conducted follow-up calls to provide additional information and confirm interest. Recruitment calls for non-English-speaking patients used an institutionally approved, Health Insurance Portability and Accountability Act-compliant interpretation service.
Data collection
Trained nonclinician researchers (MTK [masami tabata-kelly] , EK, CS [Christina Sheu]) conducted virtual interviews with participants. To ensure consistency, interviewers completed mock interviews, and the principal investigator (R.E.B.) reviewed the first interview conducted by each interviewer. Interviewers shared brief summaries with the research team after each interview.
Each interview included two components: an interviewer-administered survey (∼15 minutes) and a semi-structured interview (∼30 minutes). Interviewers introduced themselves as trained researchers not involved in participants’ clinical care. The interview guide and survey questionnaires were professionally translated. For Spanish-speaking participants, a trained Spanish interpreter (BL) was used; for Haitian Creole-speaking participants, a third-party telephone interpreter was used. Charlson Comorbidity Index scores 37 were calculated using diagnostic codes from the two years preceding the serious illness conversation. 38
The validated, 15-item Advance Care Planning Engagement Survey 39 was utilized to measure advance care planning (ACP) self-efficacy and readiness across four topics: (1) medical decision makers or surrogates, (2) deciding what matters most in life, (3) flexibility for a medical decision maker, and (4) asking doctors questions. Items were scored on a 5-point Likert scale, with higher scores indicating greater ACP engagement. The survey has been validated in English and Spanish but not in Haitian Creole. 40 Missing, refused, and “not sure” responses were excluded from mean score calculations.
The 5-item Serious Illness Conversation Patient Experience Survey41–44 assessed how worthwhile patients found the conversation and its impact on hopefulness, closeness with the clinician, sense of control over medical decisions, and understanding of their health. Worthwhileness was rated on a 4-point scale (4 = extremely worthwhile), and the remaining four items were rated on a 7-point scale (1 = decreased a lot to 7 = increased a lot). The “Heard and Understood” item used a 5-point scale to assess how much the conversation helped patients feel heard and understood, with higher scores indicating that patients felt more heard and understood. 44
The 4-item BRIEF Health Literacy Screening Tool 45 was used to characterize the level of health literacy among the study sample, with items scored on a 5-point scale and summed to obtain a total score, where higher scores indicate greater health literacy.
The interview guide was iteratively developed with input from the research staff and principal investigators (Supplementary Data S1) and focused on the acceptability of nurse-led serious illness conversations and barriers and facilitators to engagement. Study participants were asked to reflect on their most recent nurse-led serious illness conversation.
Survey data were collected using Research Electronic Data Capture. 46 Interviews were audio-recorded and transcribed by an independent transcription service. Participants received a $50 gift card.
Data analysis
Descriptive statistics summarized demographic and survey data using frequencies and percentages for categorical variables and means with standard deviations (SDs) for continuous variables. Missing data were excluded.
Qualitative data were coded using ATLAS.ti. We used a framework approach, 47 with an initial coding structure informed by survey domains and iterative refinement of codes through team discussion (M.T.-K., C.S., A.L.B.). Inductive analysis was then conducted to identify themes from participant experiences. 47 To develop integrated meta-themes, we used a pillar-building approach to examine convergence and complementarity between survey and qualitative findings. 48
Results
Participant characteristics
A total of 126 potentially eligible patients were identified. Of these, 81 were excluded due to being unapproachable, death during the study window, or other reasons (Supplementary Data S2). Among the remaining 45 eligible patients who were approached, 30 declined participation for various reasons, including health-related reasons, being too busy or overwhelmed, or lack of interest (Supplementary Data S2). A total of 15 participants enrolled in the study, corresponding to an enrollment rate of 33.3%. Survey questions were completed by 13 of 15 participants, with two participating only in interviews. Mean participant age was 63 years, with 47% (7 out of 15) identifying as female. Sixty-seven percent (10 out of 15) identified as Black, and 27% (4 out of 15) identified as Hispanic/Latino. Twenty-seven percent (4 out of 15) reported a primary language other than English (n = 3 Spanish, n = 1 Haitian Creole). Nearly half (47%; 7 out of 15) had a high school diploma or less, and 42% (5 out of 12) reported annual household income below $35,000. Mean BRIEF Health Literacy score was 13 (SD: 5.69), indicating a marginal level of health literacy. Additional participant characteristics are presented in Table 1.
Study Participants’ Characteristics (N = 15)
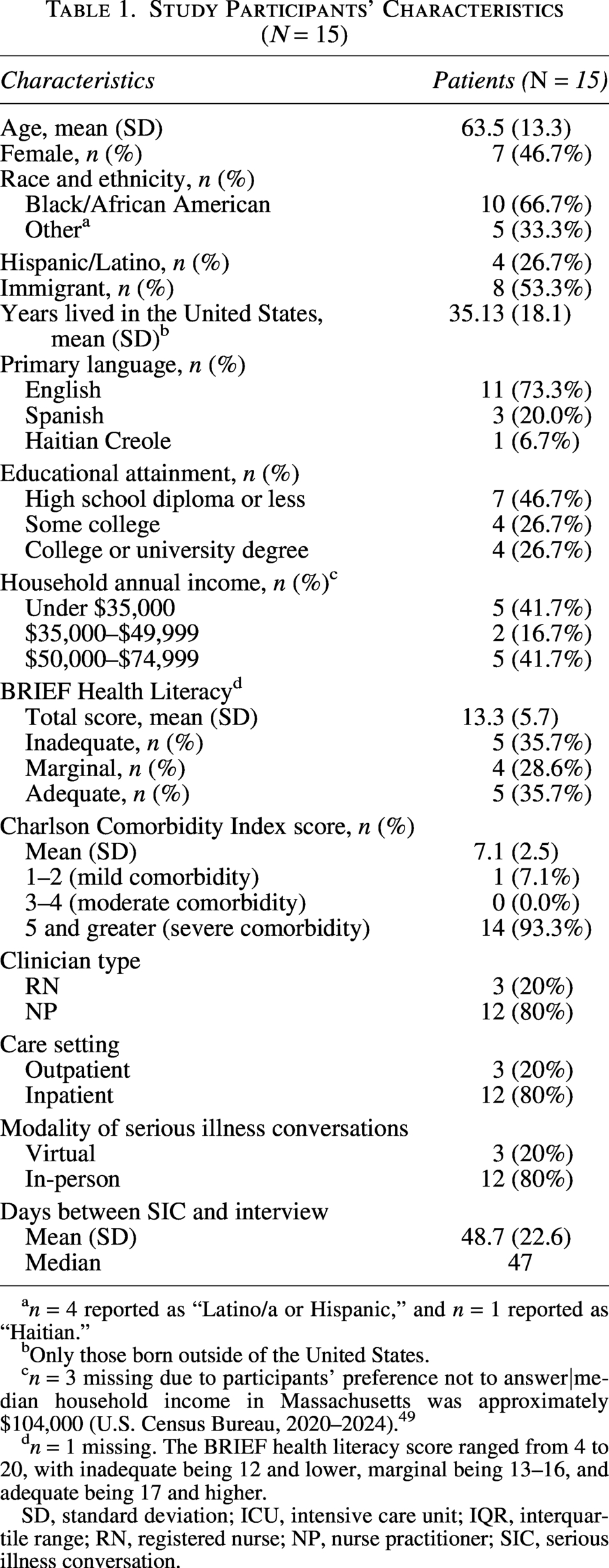
n = 4 reported as “Latino/a or Hispanic,” and n = 1 reported as “Haitian.”
Only those born outside of the United States.
n = 3 missing due to participants’ preference not to answer|median household income in Massachusetts was approximately $104,000 (U.S. Census Bureau, 2020–2024). 49
n = 1 missing. The BRIEF health literacy score ranged from 4 to 20, with inadequate being 12 and lower, marginal being 13–16, and adequate being 17 and higher.
SD, standard deviation; ICU, intensive care unit; IQR, interquartile range; RN, registered nurse; NP, nurse practitioner; SIC, serious illness conversation.
Survey results
15-item ACP Engagement Survey
The mean total score for the ACP Engagement Survey was 4.07 (SD: 0.56), with subscale means of 4.35 (SD: 0.18) for self-efficacy and 3.40 (SD: 0.33) for readiness (Table 2).
Fifteen-Item Advance Care Planning Engagement Survey (n = 13) a
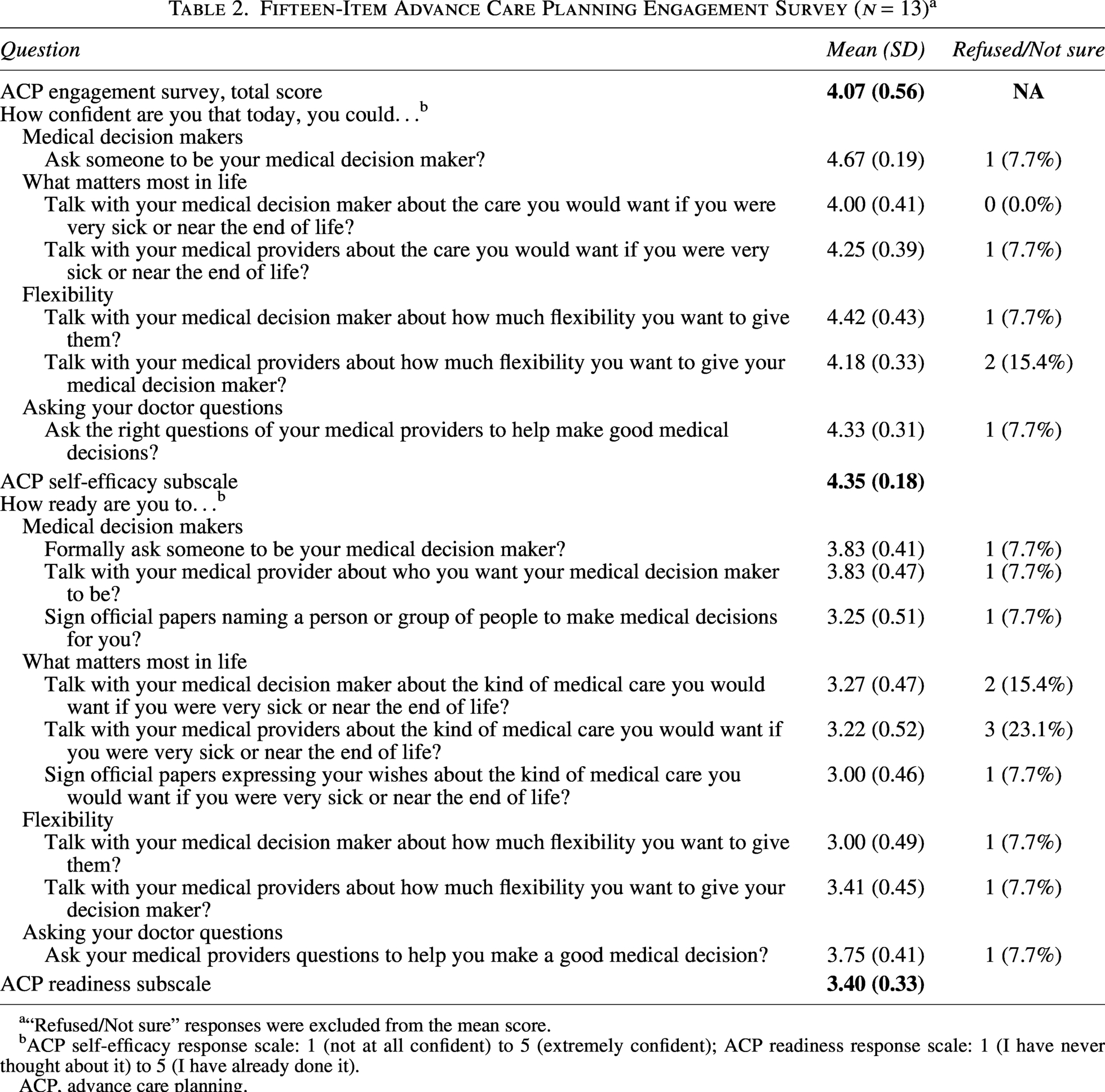
“Refused/Not sure” responses were excluded from the mean score.
ACP self-efficacy response scale: 1 (not at all confident) to 5 (extremely confident); ACP readiness response scale: 1 (I have never thought about it) to 5 (I have already done it).
ACP, advance care planning.
Patient Experience Survey and Heard and Understood Item
Participants generally found serious illness conversations worthwhile, with 46% (6 out of 13) rating them as extremely worthwhile (Fig. 1). Participants also reported that the conversation increased their hopefulness about quality of life (54%; 7 out of 13), closeness with their clinician (46%; 6 out of 13), sense of control over medical decisions (50%; 6 out of 12), and understanding of illness trajectory (58%; 7 out of 12; Fig. 2). The mean “Heard and Understood” score was 3, indicating moderate level of feeling heard and understood (Fig. 3).
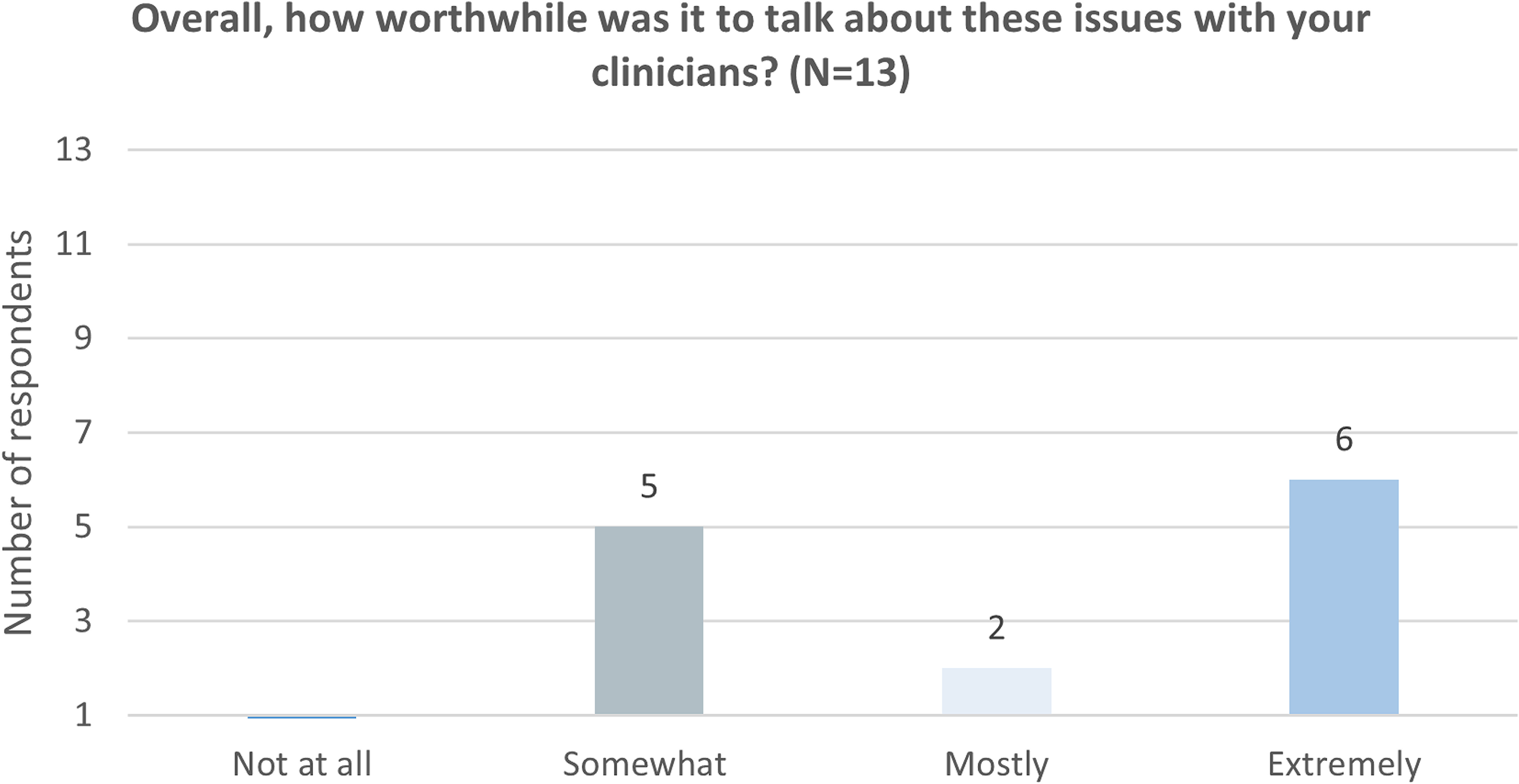
Serious Illness Conversation Patient Experience Survey Panel A (n = 13).
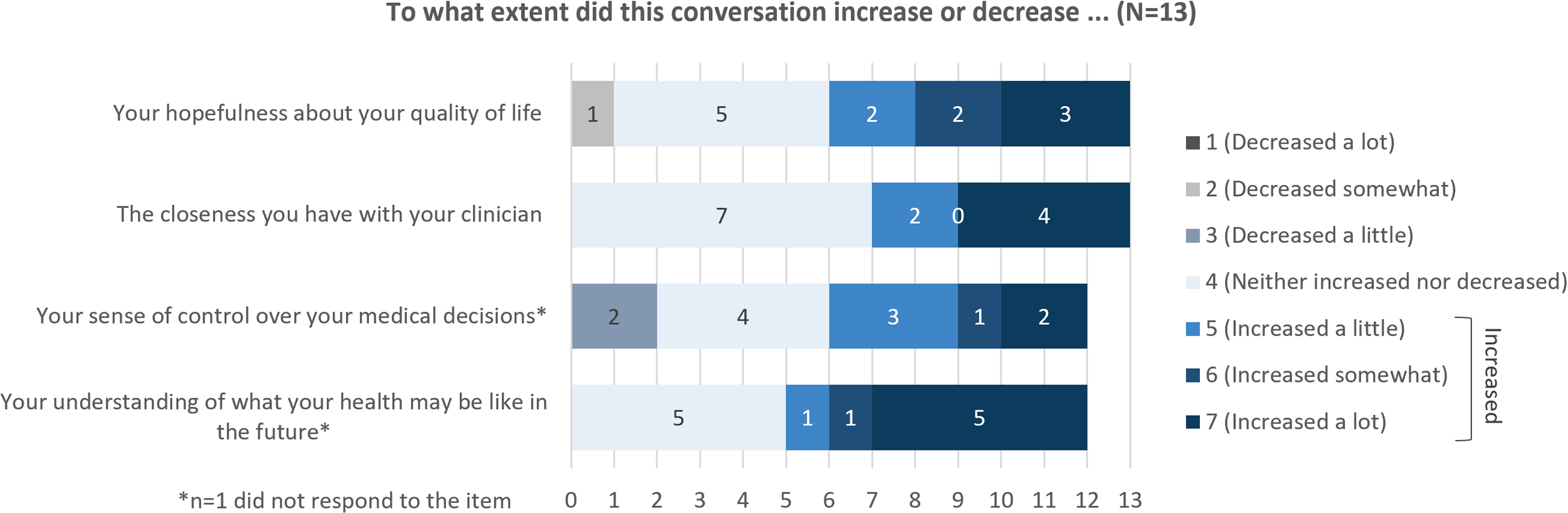
Serious Illness Conversation Patient Experience Survey Panel B (n = 13).
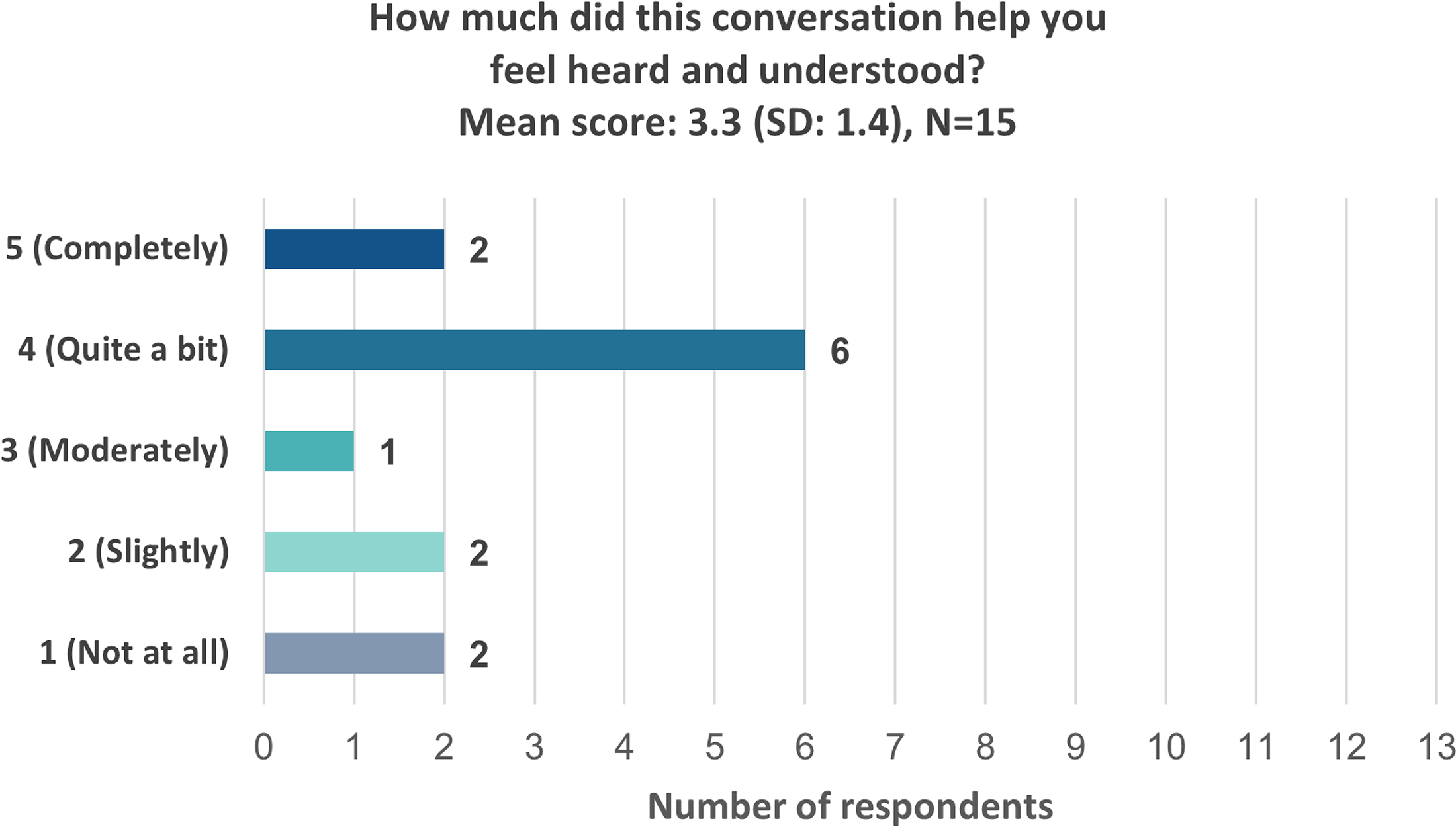
Heard and Understood Item (n = 13).
Integrated meta themes
Participants found nurse-led serious illness conversations helpful and valued discussing their values, goals, and wishes with nurses. ACP engagement and self-efficacy scores were high (above 4 out of 5), whereas readiness scores were lower. Integrating survey and qualitative findings, we identified three overarching meta-themes shaping participants’ experiences (Table 3). The research team discussed and determined that thematic saturation had been reached, as no additional themes emerged from the data.
Joint Display of Integrated Findings on Patient Experiences of Nurse-Led Serious Illness Conversations
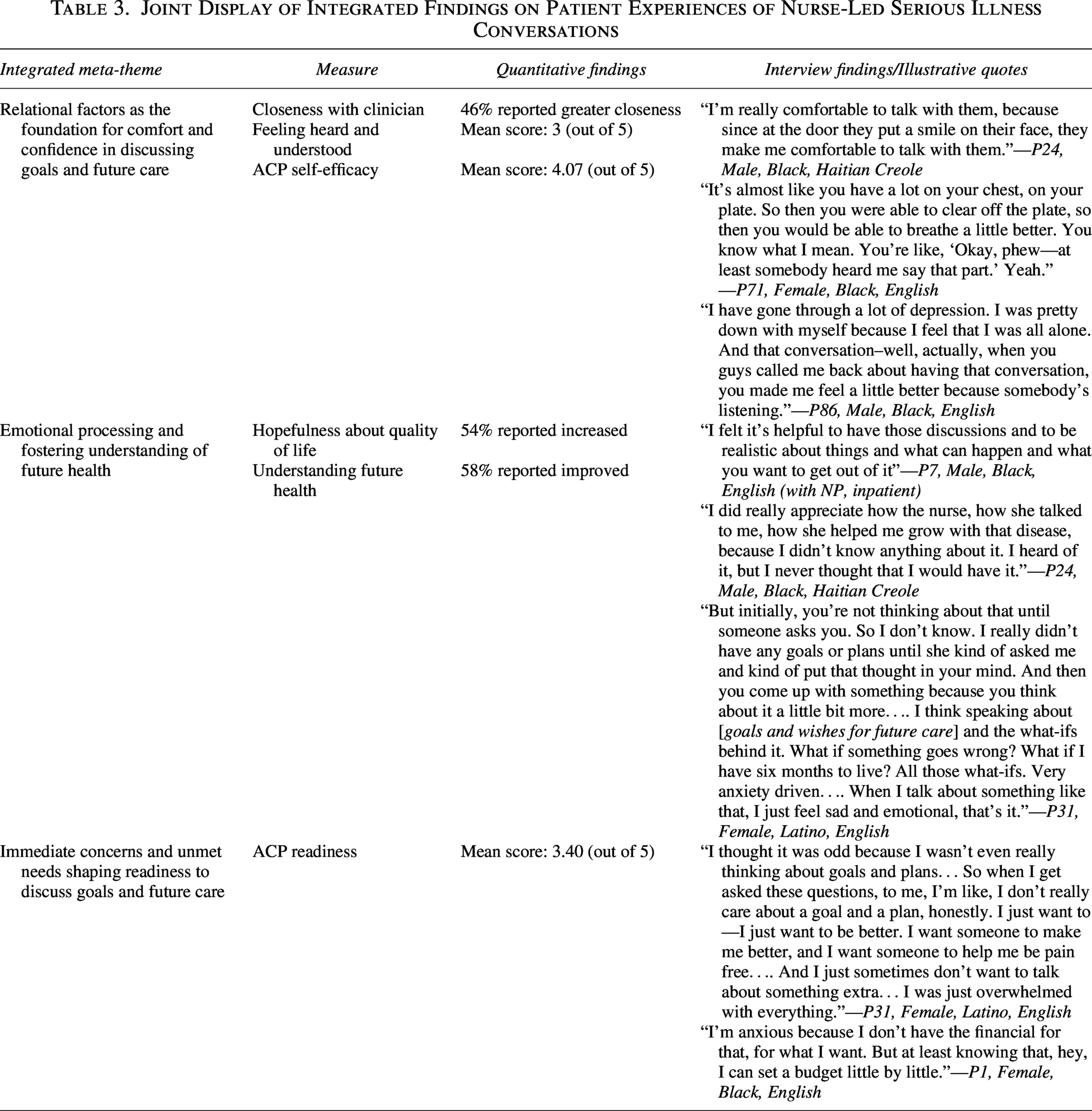
Theme 1: Relational factors as the foundation for comfort and confidence in discussing goals and future care
Participants shared their experiences with serious illness conversations by describing how their nurses made them feel comfortable. They described how nurses’ demeanor helped them feel comfortable engaging in serious illness conversations: “I felt like she seemed very sincere, and she listened to everything I had to say, which obviously, is very helpful when you try to explain your situation. So yeah, in that sense I thought she was very helpful. I thought she listened, and I thought she gave good advice.”—P25, Male, Black, English
Participants also reflected on the therapeutic effects of feeling heard: “If you talk to somebody and the way they treat you, then you feel good.”—P27, Male, Latino, Spanish
These experiences illustrated how nurses’ compassionate demeanor and active listening shaped participants’ experiences with serious illness conversations.
Theme 2: Emotional processing and fostering understanding of future health
Engaging in serious illness conversations elicited a wide array of emotions. Many described the experience as “hard,” “uncomfortable,” “weird,” “unsettling,” “stressful,” “anxious,” and “sad.” Despite the intensity of these emotions, participants noted that the conversations provided a space to process their feelings and reflect on their illness and future care: “It was hard. It was emotional for me. Hard, emotional. Just tough. I broke down a couple of times. I broke down probably for the whole conversation we were having. It was just hard. I’d say it was just hard.”—P31, Female, Latino, English
Another participant also expressed: “It felt okay, but then on the other hand it felt unsettling because of talking about your health and what may happen.”—P7, Male, Black, English
Retrospectively, participants came to recognize the value of this emotional processing as an essential step toward greater readiness and understanding: “I would say that the conversation was definitely uncomfortable, but sometimes you need to have those uncomfortable conversations…. We’ve come to terms with it more as the conversation is repeatedly brought up, I guess.”—P1, Female, Black, English
Participants also described how nurse-led conversations supported them not only in grappling with difficult emotions but also in developing a clearer understanding of their illness and future priorities: “She helped me to go through that difficult time, where with that disease, most of the times they would tell you there’s no cure for it, where a lot of people would die from it. But they helped me to understand it and live happy with it.”—P24, Female, Black, Haitian Creole
Nurse-led conversations initially evoked discomfort and strong emotions, but they eventually helped participants feel more ready to consider future care and develop a better understanding of their illness trajectory at their own pace.
Theme 3: Immediate concerns and unmet needs shaping readiness to discuss goals and future care
Participants’ experiences highlighted how immediate concerns, such as physical pain and important personal plans, occupied their thoughts. Many expressed feeling unready to discuss goals or future care because physical pain and emotional distress left them overwhelmed: “I thought it was odd because I wasn’t even really thinking about goals and plans… So when I get asked these questions, to me, I’m like, I don’t really care about a goal and a plan, honestly. I just want to– I just want to be better. I want someone to make me better, and I want someone to help me be pain free…. And I just sometimes don’t want to talk about something extra… I was just overwhelmed with everything.”—P31, Female, Latino, English
For some, financial constraints prompted reflection on their goals and a desire to make decisions in a way that would not burden their family members. One participant shared: “I’m anxious because I don’t have the financial for what I want…. I’ve seen a lot of elderly dying from COVID and sickness, and their family probably already buy their plot 20 years ago…. I feel like for me, I don’t have those kind of money some people have or whatever thing. But it’s good for me to know that I’m not having my kids tossing their heads left and right…. So I need to act on what I would want, not what they can provide for me.”—P1, Female, Black, English
Participants also expressed existential distress: “I wanted to hurry up and get it (conversation) over with because I really don’t like talking about myself…. I can’t see myself dying. I don’t want that…. I was such an outgoing person, physically fit. And just being the way I am, very depressive.”—P86, Male, Black, English
These experiences illustrated how multifaceted and salient concerns and needs shaped readiness to engage in serious illness conversations.
Discussion
This mixed-methods study explored the experiences of racially and ethnically marginalized patients with nurse-led serious illness conversations. We identified three integrated themes showing that relational factors fostered comfort and confidence in discussing goals and future care; conversations created space for emotional processing and a better understanding of future health; and immediate concerns and unmet needs shaped patients’ readiness to engage. These themes were interdependent, with feeling “heard and understood” central across all three. While survey results suggested increased confidence, readiness scores and qualitative findings showed that this did not always translate into action when immediate concerns and emotional distress were present.
Patients’ perspectives on serious illness conversations have been increasingly explored, with growing efforts to elevate the voices of racially and ethnically marginalized communities. Consistent with prior studies highlighting the importance of relational aspects, participants similarly valued these aspects in our study. Patients were willing to engage in nurse-led serious illness conversations primarily because of nurses’ relational communication approaches that helped them feel at ease.41,50,51
Our finding that immediate concerns and needs shaped patients’ readiness to engage in conversations aligns with prior research. 52 We extend this work by demonstrating how multifaceted distress and concerns, particularly among patients from marginalized communities, serve as critical contextual factors shaping readiness. Although nurse-led serious illness conversations fostered confidence in discussing goals and future care, that confidence did not consistently translate into readiness to engage. This is similar to prior findings from nurse-led models of serious illness conversations in emergency department settings, which improved documentation of conversations but not patients’ readiness to engage in ACP. 23 Participants in our study described feeling overwhelmed by multilayered stressors that made it harder to engage in serious illness conversations. A growing body of literature suggests that interdisciplinary, team-based approaches may help mitigate these challenges.53,54 For example, a nurse- and social worker–led multicomponent intervention integrating serious illness conversations with symptom management and psychosocial support improved ACP readiness. 24 As such, to support ACP engagement, strategies should include tailored, personalized approaches that are attentive to individuals’ social and personal contexts and address immediate needs.22,54,55 A systematic review of ACP interventions for vulnerable adult populations across eight countries also highlighted the importance of holistic, personalized, relational, and trust-building approaches that are attentive to individuals’ health literacy. 56 In line with this, a recent study of ACP interventions similarly emphasized the need for culturally tailored strategies to support equitable ACP engagement. 25 Our prior work examining nurses’ perspectives on conducting serious illness conversations with racially and ethnically marginalized patients also identified the importance of addressing unmet needs and approaching conversations with cultural humility. 22 Future studies can further explore multifaceted distress as a potential moderating factor and evaluate multicomponent interventions that combine serious illness conversations training with interdisciplinary collaboration, supportive resources, and culturally tailored approaches.57,58
Our study cohort reflects not only racially and ethnically marginalized patients but also intersects with social vulnerability, with about half having a high school diploma or less and limited health literacy. Individuals from socially marginalized backgrounds remain underrepresented in serious illness care research.34,59–61 Research that better captures and reflects the experiences of this population plays a critical role in developing and implementing serious illness care interventions and practices that address socioeconomic, cultural, and linguistic needs.62–65
Prior studies note that nurses often face challenges in discussing prognostic information because of role ambiguity, emotional tensions, and limited training.66–68 In our study, most participants reported improved understanding of their illness trajectory after nurse-led conversations, suggesting greater awareness of functional prognosis. 69 With appropriate training and support, nurses can leverage their relational strengths to revisit these conversations and foster better functional prognostic understanding. Therefore, future studies should explore this pathway as a potential mechanism for improving patient- and family-centered outcomes and for addressing multilevel factors, including serious illness communication skills, documentation workflows, and team-based care processes.17,51,70,71
This study has several limitations. It was conducted within a single health system, which may limit generalizability. We recognize that registered nurse care coordinators and nurse practitioners differ in training, roles, and clinical context (outpatient vs. inpatient), which may shape how they conduct serious illness conversations. However, our analysis focused on shared patient experiences across nurse-led conversations. This study did not focus on a specific serious illness but instead sought to capture broad perspectives from individuals living with serious illness; therefore, the applicability of these findings to specific conditions requires further study. We did not collect information on whether participants had previously received prognostic information from their physicians. Although nurse-led serious illness conversations were conducted in the context of interdisciplinary care practice, in which nurses often include elements related to prognostic information, prior exposure to physician-led prognostic discussions may have varied. This study reflects the experiences of a relatively small sample of seriously ill patients from racially and ethnically marginalized communities, which may limit generalizability of the findings. Barriers to participation, including health-related challenges, are consistent with those previously reported in recruiting seriously ill populations. 72 To support the inclusion of racially and ethnically marginalized populations, future research may benefit from community-engaged and relationship-centered recruitment strategies.73,74 Finally, our study did not fully capture the diverse array of experiences among racially and ethnically marginalized populations, including groups such as Native American and Alaska Native patients, individuals with non-English language preference, and recent immigrants, whose inclusion remains critical to advancing serious illness communication research.61,75,76 Importantly, participants in this study represent a socially vulnerable population with limited health literacy, lower educational attainment, and economic disadvantage, which have shaped their engagement and experiences in serious illness conversations.
Conclusions
Nurse-led serious illness conversations facilitated greater confidence among racially and ethnically marginalized patients to engage in discussions about their goals and future care and fostered a better understanding of their future health. Interdisciplinary collaboration to address multifaceted distress, along with expanded nurse training in serious illness communication, is needed to support readiness.
Authors’ Contributions
M.T.-K.: Conceptualization, data curation, formal analysis, investigation, methodology, project administration, software, visualization, writing—original draft preparation, and writing—review and editing. C.S.: Data curation, formal analysis, investigation, software, visualization, writing—original draft preparation, and writing—review and editing. A.L.B.: Funding acquisition, investigation, methodology, supervision, and writing—review and editing. M.R.: Formal analysis. K.B.: Supervision. T.F.G., B.J.H., and L.W.: Resources and writing—review and editing. R.E.B.: Formal analysis, funding acquisition, investigation, methodology, resources, supervision, validation, and writing—review and editing.
Ethical Approval and Informed Consent Statement
This study was approved by the Institutional Review Board of Mass General Brigham (#2021P001220). All participants provided verbal informed consent prior to participation.
Data Availability Statement
To protect the confidentiality of study participants’ data, raw data will remain confidential and will not be shared. Data will not be publicly available. All data reported within the article have been anonymized and de-identified.
Footnotes
Acknowledgments
The authors would like to express their gratitude to Emma Kerr, Dr. Muhammad Abbas, and Jeenn Alain Barreiro-Rosado for their project administrative support. The authors thank Dr. Erica Wilson, Dr. Coleen Reid, Dr. Kosha S. Thakore, and Dr. Dany Hilaire for their support and guidance in recruitment and extend their appreciation to Belin Lazaro for her support with Spanish interpretation. The authors also express appreciation to Dr. Jolie Haun and her team for generously providing the Spanish translation of the BRIEF Health Literacy Screen Tool for this study. The authors further extend their appreciation to Dr. Joanna M. Paladino and Ariadne Labs for providing the Serious Illness Conversation Patient Experience Survey for use in this study. The authors acknowledge Haley Szewczuga, a Science Writer/Editor at the Dana-Farber Cancer Institute, for her support in the preparation of this article.
Author Disclosure Statement
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
The authors disclose the receipt of the following financial support for research, authorship, and/or publication of this article: the Rita and Alex Hillman Foundation.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.