
Abstract
Background:
Opioid-induced constipation (OIC) limits opioid titration in cancer care. Before the use of peripherally acting μ-opioid receptor antagonists (PAMORAs), OIC often required switching from oxycodone to lower-risk opioids, such as transdermal fentanyl. Whether naldemedine allows oxycodone escalation without switching remains unclear. We evaluated the maximum scheduled daily oxycodone dose as a surrogate for maintaining therapy without constipation-driven switching.
Methods:
We retrospectively reviewed adults with cancer pain who initiated oral oxycodone at Toyama University Hospital between June 2017 and December 2018. Patients receiving naldemedine were classified as Group A; others as Group B. The primary endpoint was the maximum scheduled controlled-release oxycodone dose during follow-up; rescue doses were excluded.
Results:
Among 217 patients, the median maximum dose was higher with naldemedine (40 mg/day [range 10–480] versus 20 mg/day [10–320]; p < 0.0001).
Conclusions:
Naldemedine enabled higher oxycodone dosing, suggesting OIC management reduces opioid switching.
Introduction
Opioids remain central to cancer pain management; however, opioid-induced constipation (OIC) is one of the most frequent and burdensome adverse effects, diminishing quality of life and often limiting dose escalation required for adequate analgesia.1,2 Conventional laxatives are used as first-line but are frequently insufficient for moderate-to-severe OIC in patients on sustained therapy.1,3 Before the adoption of peripherally acting μ-opioid receptor antagonists (PAMORAs), a pragmatic approach in routine care was opioid switching from oxycodone to agents perceived to cause less constipation, particularly transdermal fentanyl. 3
Naldemedine is an orally administered PAMORA designed to antagonize peripheral μ-opioid receptors in the gut without compromising central analgesia. Randomized phase 3 trials in cancer populations have shown improvements in bowel symptoms with acceptable safety. 4 Prophylactic use at opioid initiation reduces incident OIC in contemporary cohorts, 5 and meta-analyses confirm consistent benefits across diverse settings.6,7 Long-term safety and tolerability have also been demonstrated in noncancer populations. 8 While the benefit of OIC management is established, it remains unclear in real-world oncology practice whether naldemedine broadens the usable therapeutic window of scheduled oxycodone, that is, whether prescribing naldemedine allows clinicians to continue and escalate oxycodone instead of switching when constipation becomes dose-limiting.
Direct quantification of opioid switching in retrospective data is difficult because documentation is inconsistent and reasons for switching are multifactorial. Therefore, we selected the maximum scheduled daily dose of controlled-release oxycodone as a surrogate endpoint for the ability to maintain oxycodone without constipation-driven switching and compared this outcome between patients treated with and without naldemedine in a single-institution cohort.
Methods
Study design and setting
We conducted a single-center retrospective cohort study at Toyama University Hospital, Japan. Consecutive adults initiating oral oxycodone for cancer-related pain between June 1, 2017, and December 31, 2018 were identified from electronic medical records, capturing prescribing patterns in the early phase after national approval of naldemedine.
Eligibility
Inclusion criteria were age ≥18 years, cancer-related pain, and a new start of oral oxycodone within the study window. Non-cancer pain was excluded. No other exclusions were applied. Patients with short treatment duration were retained if the primary endpoint could be ascertained from records.
Exposure groups
Patients were classified by naldemedine exposure during oxycodone therapy. Group A received naldemedine 0.2 mg once daily at any time, either at initiation or after constipation onset. Group B did not receive naldemedine. Outcomes were not stratified by timing of initiation; this clinically relevant issue will be examined separately.
Endpoint definitions and follow-up
The primary endpoint was the maximum scheduled daily dose of controlled-release oxycodone, abstracted from records. Rescue immediate-release doses were excluded, and no conversion into scheduled equivalents was performed. Analyses were restricted to controlled-release dosing to reflect maintenance therapy and reduce noise from transient spikes. Observation ended at the earliest occurrence of opioid discontinuation, switching to another opioid, death, or transfer-related loss to follow-up, which was treated as the end point. Analyses were not adjusted for observation length in this short report.
Covariates
We extracted age, sex, Eastern Cooperative Oncology Group performance status (0–2 vs. 3–4), primary cancer site (lung, gastrointestinal, other), care setting at oxycodone initiation (inpatient vs. outpatient), and concurrent anticancer treatment (chemotherapy vs. best supportive care) to describe baseline comparability (Table 1).
Patient Characteristics of Group A (Naldemedine Administration) and Group B (Oxycodone Only Administration)
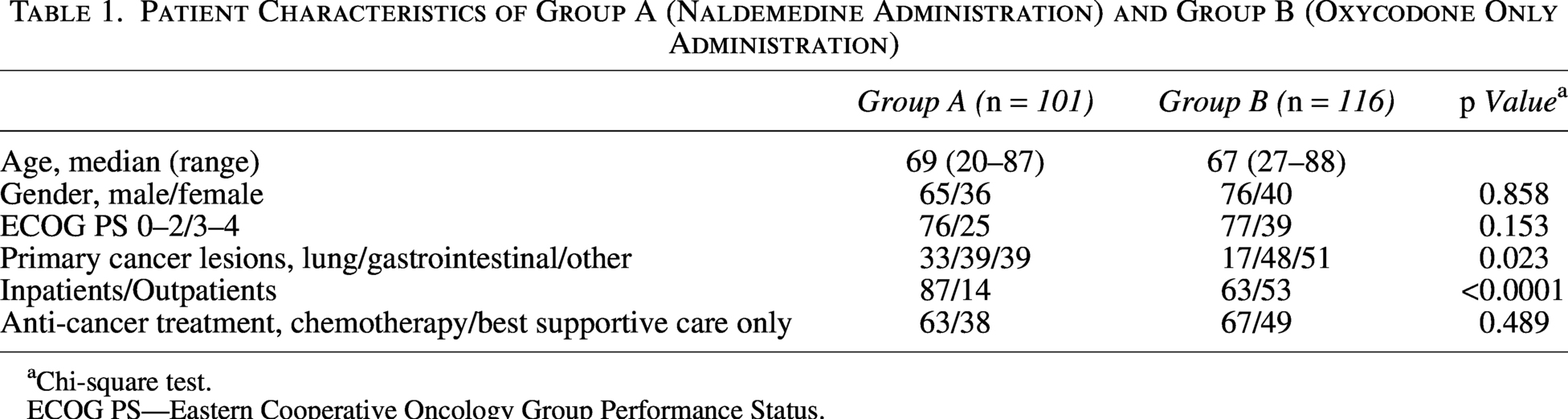
Chi-square test.
ECOG PS—Eastern Cooperative Oncology Group Performance Status.
Statistical analysis
Continuous variables were summarized as median (range). Categorical variables were summarized as counts (percentages) and compared using the chi-square test or Fisher’s exact test where appropriate. The primary endpoint, maximum scheduled daily dose, was compared using the Mann–Whitney U test. Two-sided p < 0.05 was considered statistically significant. Analyses were exploratory and descriptive, with no imputation performed.
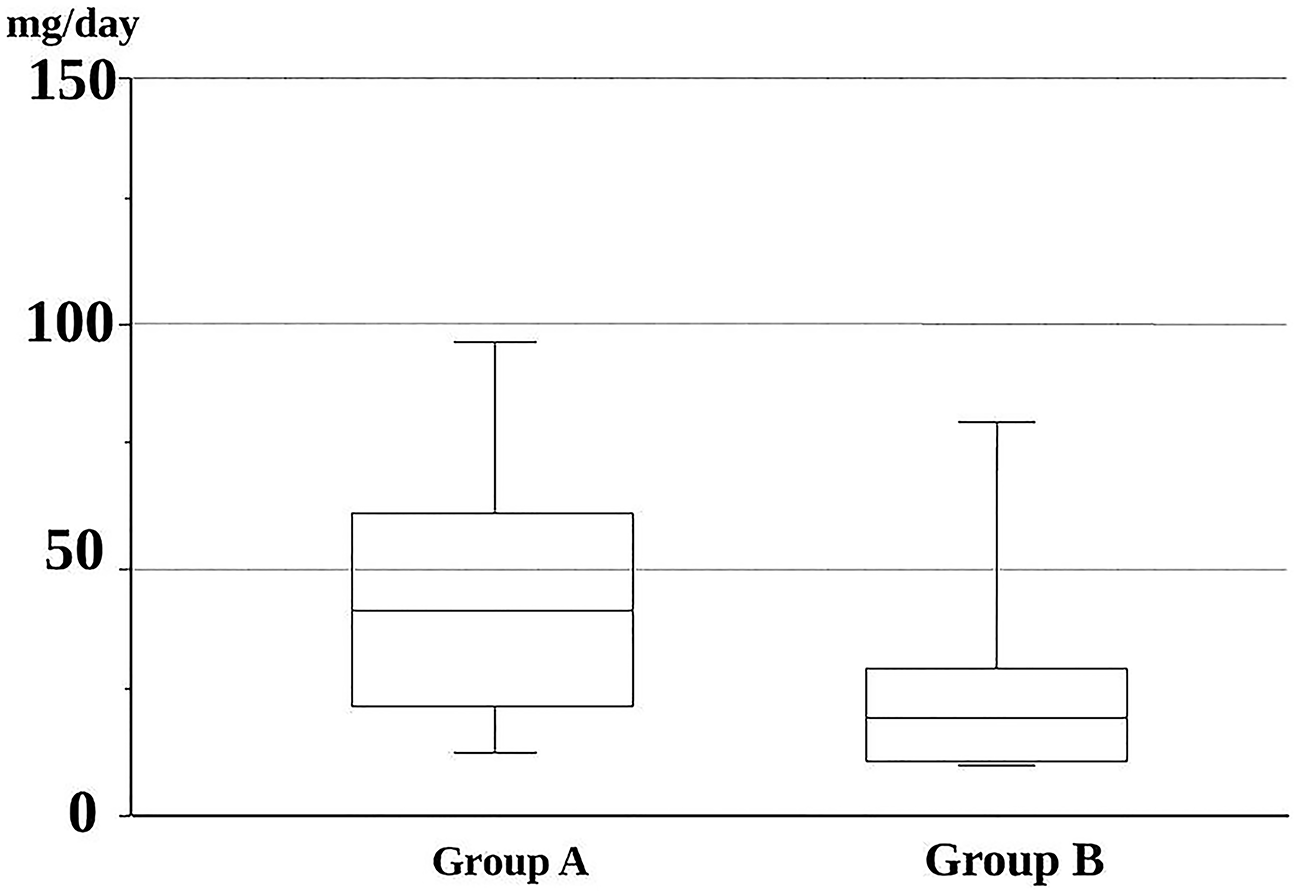
The maximum Oxycodone dose (mg/day). The maximum scheduled daily dose of controlled-release oxycodone (mg/day) is shown for patients receiving naldemedine (Group A, n = 101) versus those not receiving naldemedine (Group B, n = 116). Data are presented as medians with ranges. Statistical comparison was performed using the Mann–Whitney U test, with p < 0.0001 indicating a significant difference between groups. CR, controlled-release.
Ethics
The study protocol was approved by the Institutional Review Board of Toyama University (Approval No. Rin 29–117). Study information was publicly disclosed with an opt-out option; individual consent was waived because of the retrospective design and minimal risk. This study was conducted in accordance with the Declaration of Helsinki as revised in 2013.
Results
Patient characteristics
We included 217 patients: 101 in Group A (naldemedine) and 116 in Group B (no naldemedine). Median age was 69 years (range: 20–87) and 67 years (27–88), respectively. Sex distribution, performance status, and anticancer treatment were similar (sex p = 0.858; treatment p = 0.489; ECOG p = 0.153). Group A included more inpatients at oxycodone initiation than Group B (87/14 vs. 63/53; chi-square p < 0.0001) and had a different distribution of primary cancer sites (lung/gastrointestinal/other: 33/39/39 vs. 17/48/51; chi-square p = 0.023).
Primary endpoint
The median maximum scheduled daily dose of controlled-release oxycodone was 40 mg/day (range, 10–480) in Group A and 20 mg/day (10–320) in Group B, a statistically significant difference (Mann–Whitney U p < 0.0001; Fig. 1). The distribution was right-skewed, with several high-dose outliers in Group A, but inference based on medians was robust. By design, rescue immediate-release doses did not contribute to the endpoint.
Discussion
In this real-world cohort of patients with cancer receiving oral oxycodone, concomitant naldemedine use was associated with a two-fold higher median maximum scheduled daily dose compared with no naldemedine. Although this endpoint is a surrogate, it is clinically intuitive: when constipation is controlled without compromising central analgesia, clinicians can escalate scheduled oxycodone rather than switching opioids for tolerability. Interpreted through this surrogate, our findings suggest that effective OIC management with naldemedine may reduce the need for opioid switching to transdermal fentanyl while enabling ongoing titration of oxycodone and preserving regimen continuity.
These observations align with evidence that naldemedine improves bowel symptoms with acceptable safety in cancer populations, 4 that prophylactic administration at opioid initiation reduces incident OIC5, and that benefits are consistent across studies.6,7 Long-term safety in non-cancer settings supports the mechanistic plausibility of sustained PAMORA use. 8 Our analysis extends these findings by highlighting a practice-relevant consequence: with OIC managed by naldemedine, the usable therapeutic window of oxycodone appears larger in routine care, allowing clinicians to maintain an effective opioid rather than converting to an alternative with different pharmacologic characteristics. 3
Clinically, the ability to maintain and escalate scheduled oxycodone, with rescue excluded, is valuable for patients whose pain responds well to oxycodone, particularly in outpatient and home settings where regimen simplicity and continuity are critical. Reducing the need for opioid switching can stabilize analgesia, avoid the logistical and psychological burdens of a medication change, and potentially decrease unplanned health-care utilization by preventing OIC crises. These implications require confirmation in prospective studies that directly assess switching events and incorporate patient-reported outcomes, including constipation burden, satisfaction with bowel function, and quality of life.
Certain limitations warrant careful interpretation. First, the retrospective, single-center design limits generalizability and leaves room for unmeasured confounding. Second, a significant care-setting imbalance existed: Group A included more inpatients, who are typically monitored more closely and may undergo faster titration, potentially inflating differences. Third, prescriber bias is possible: clinicians more experienced in opioid management may have been both more likely to prescribe naldemedine and more willing to escalate oxycodone, conflating drug effect with practice style. Fourth, time-dependent exposure introduces potential immortal-time bias: some patients began naldemedine after oxycodone initiation, and surviving or continuing therapy until initiation increases escalation opportunity. We did not model time-varying exposure in this short report.
Fifth, the endpoint is a surrogate: we did not directly quantify switching events or reasons for switching, so inference regarding reduced transitions to fentanyl remains indirect and hypothesis-generating. Sixth, although documentation of prescribing timing (prophylactic vs. reactive) existed, we did not stratify outcomes here; a companion report will address this question. Seventh, concomitant laxative use was not systematically captured across groups, precluding assessment of its influence on the endpoint. Eighth, other potential effect modifiers, including brain metastases, blood–brain barrier disruption, organ dysfunction, CYP3A drug interactions, disease trajectory, and performance status, were incompletely captured. Finally, we did not analyze observation length, which could affect opportunities to escalate dosing if follow-up differed between groups.
Notwithstanding these limitations, our study has practical strengths. We prespecified a clear, reproducible endpoint—maximum scheduled daily dose excluding rescue—to reflect maintenance therapy while minimizing noise from transient dose changes. We examined consecutive real-world cases over a fixed calendar period immediately after national approval, reducing selection bias from evolving practice. The cohort size was reasonable for a brief report, and the observed twofold median difference was both statistically persuasive and clinically meaningful in the palliative oncology setting.
Conclusions
In summary, concomitant naldemedine use was associated with higher maximum scheduled doses of oral oxycodone in patients with cancer. Interpreted through a surrogate endpoint, these findings indirectly suggest that effective OIC management with naldemedine may reduce the need for opioid switching to transdermal fentanyl while supporting continued oxycodone titration. Prospective multicenter studies incorporating time-dependent analyses, systematic capture of laxative use, and direct switching metrics are needed to confirm causality and identify patients most likely to benefit from prophylactic versus reactive naldemedine.
Authors’ Contributions
S.K. and S.C.: Conceptualization and methodology. Y.Y. and N.R.: Data curation. T.M., M.K., A.Y., N.K., Y.M., R.Y., K.N., I.M., T.A., and I.Y.: Investigation and resources. S.K.: Formal analysis, writing—original draft preparation, and supervision. R.H.: Writing—review and editing. All authors: Visualization.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Data Availability Statement
Deidentified data for this study are stored on secure institutional servers at Toyama University Hospital. In accordance with institutional policies and privacy regulations, the data are not publicly available. Additional de-identified data may be available from the corresponding author (