
Abstract
Background:
Clinical guidelines recommend naldemedine for opioid-induced constipation in patients with cancer, either with conventional laxatives or as a first-choice option. Making prophylactic naldemedine a new standard treatment for opioid-induced constipation requires a demonstration of its value for money.
Objectives:
We aimed to evaluate the cost-effectiveness of prophylactic naldemedine in patients with cancer initiating strong opioid therapy.
Design:
We conducted a cost-effectiveness analysis of prophylactic naldemedine replacing standard, nonprophylactic use from the payer’s perspective, using a decision tree model based on data from a multicenter, double-blind, randomized controlled trial in Japan.
Setting/Subjects:
The study population included patients aged ≥20 years and initiating strong opioid therapy for the first time.
Results:
The incremental cost-effectiveness ratio of prophylactic naldemedine for opioid-induced constipation was 1,445,276 Japanese yen (¥) or 9,635 United States dollars (USD) with an exchange rate of 1 USD = 150 ¥ per quality-adjusted life year. Using the official value of social willingness-to-pay threshold in Japan of 5 million ¥ or 33,333 USD per quality-adjusted life year gained, prophylactic naldemedine was found to be cost-effective.
Conclusions:
This is the first global cost-effectiveness analysis of prophylactic naldemedine in patients with cancer. Prophylactic naldemedine for opioid-induced constipation in patients with cancer initiating strong opioid therapy could be justifiable as an efficient use of finite health care resources.
Key Message
This is the first global cost-effectiveness analysis of prophylactic naldemedine for opioid-induced constipation in patients with cancer. The results suggest that this strategy could be justifiable as an efficient use of finite health care resources.
Introduction
Opioid-induced constipation (OIC) is the most common adverse effect of opioid analgesics, occurring in approximately 97% of patients with cancer receiving opioids.2–6 OIC can greatly impact quality of life (QOL), reduce opioid analgesic adherence, and interfere with pain relief.3–5 Clinical guidelines generally recommend prophylactic use of conventional laxatives, including osmotic or colon-stimulating laxatives, to prevent OIC.3–5,7,8 Naldemedine is a novel peripheral-acting µ-opioid receptor antagonist (PAMORA) that specifically alleviates OIC.9–11 Moreover, naldemedine is recommended for the treatment of patients with unresolved or refractory OIC, either in combination with conventional laxatives or as first-choice treatment.3–5,7,8
In a recent multicenter, double-blinded, randomized controlled trial (RCT) by Hamano et al., 12 the effects of prophylactic naldemedine for OIC were evaluated in patients with cancer initiating strong opioid therapy. The findings were that 14 days of prophylactic naldemedine resulted in: (1) a higher proportion of patients without symptoms of constipation (bowel function index [BFI] < 28.8) on day 14 in the cohort treated with prophylactic naldemedine, in addition to standard osmotic or colon-stimulating laxatives (64.6%; 95% confidence interval [CI]: 51.1–78.1) compared with those treated with placebo in addition to standard laxatives (17.0%; 95% CI: 6.3–27.8); and (2) a markedly better constipation-related QOL in the naldemedine cohort than that in the placebo cohort during days 1–14. 12 However, prophylactic naldemedine is tried by some physicians, 13 because preventive use before the occurrence of OIC is not covered by the Japanese health insurance system in 2024, and is not included in the Japanese clinical guidelines.7,8
Japan provides universal health coverage to all citizens. The health care system is considered one of the most accessible in the world and provides comprehensive care, with palliative care covered by social health insurance. 14 The widespread use of resource-consuming treatments, including those not covered by social health insurance, raises concerns regarding cost-effectiveness, 15 because of the rapidly rising health care expenditure. The justifiability of using prophylactic naldemedine with limited health care resources remains uncertain, owing to a lack of sufficient economic studies. Therefore, in this study, we aimed to evaluate the cost-effectiveness of prophylactic naldemedine in Japanese patients with cancer initiating strong opioid therapy. The results have implications for the current treatment of OIC in this population.
Materials and Methods
Study design
We conducted a cost-effectiveness analysis of prophylactic naldemedine for OIC in patients with cancer initiating strong opioid therapy, using a decision tree. The incremental cost-effectiveness ratio (ICER) was estimated from the payers’ perspective, which included social insurers and patients, and compared with the cost-effectiveness threshold in Japan. 16 In constructing the model, we conducted a methodological literature survey to identify the best available evidence from Japan within the last 5 years. The PubMed database and Igaku Chuo Zasshi, a Japanese medical literature database, were searched using combinations of relevant search terms, such as OIC, laxatives, opioids, and cancer. Ethics approval and the requirement for patient consent were not applicable, as this study used secondary data.
Target population
The target population was patients aged ≥20 years with cancer who were initiated on regularly administered strong opioid therapy. Patients with gastrointestinal obstruction who had undergone interventions affecting gastrointestinal function were excluded. 12
Decision tree model
A decision tree model was constructed to evaluate prophylactic use of naldemedine, replacing standard, nonprophylactic use (Fig. 1). For days 1–14, both courses were modeled based on the study by Hamano et al. 12 After day 14, prophylactic use was based on assumptions, whereas standard use was modeled using data from the phase III RCT and extension studies by Katakami et al. 9
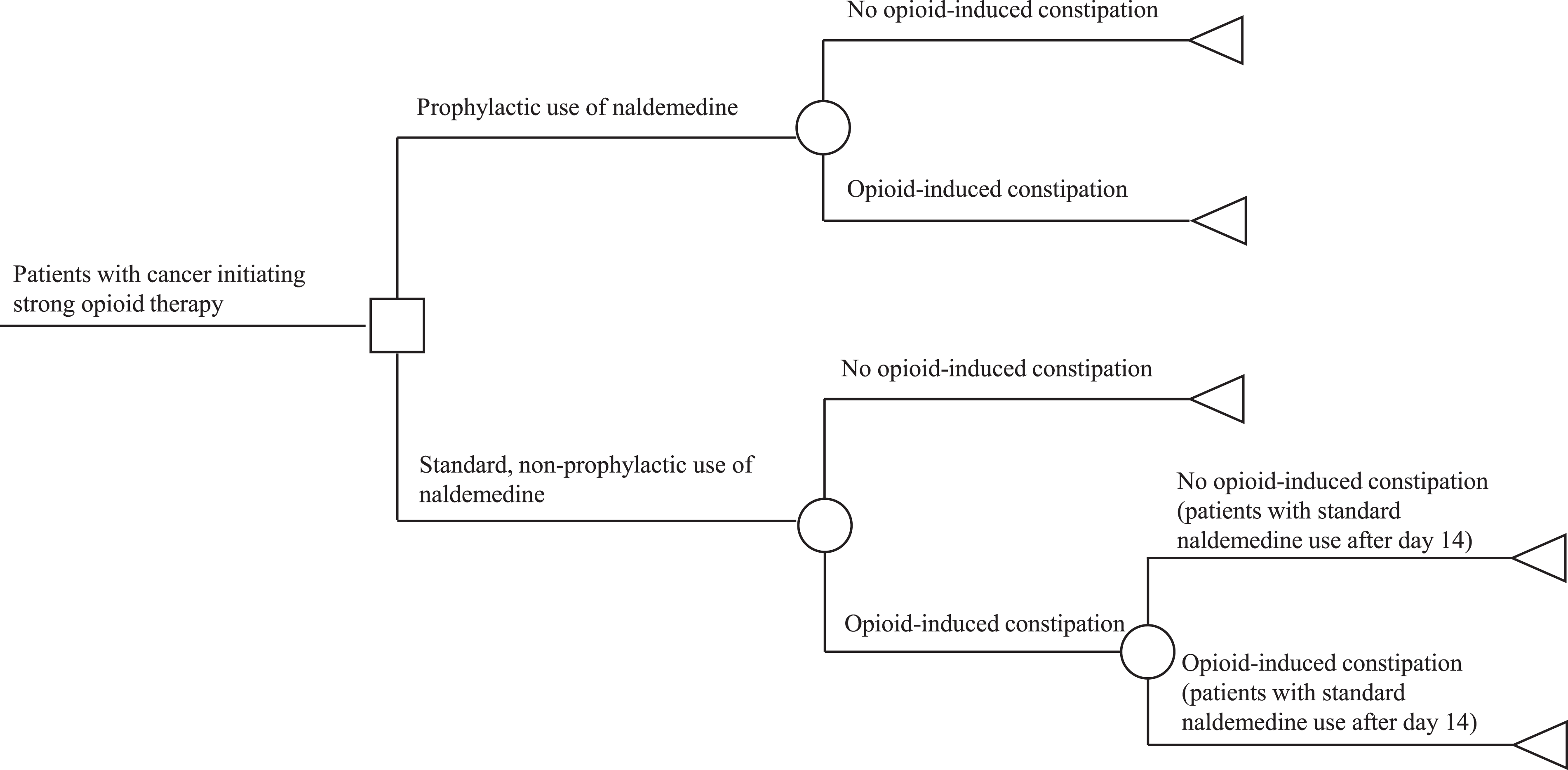
Decision tree model estimating the cost-effectiveness of prophylactic naldemedine use for opioid-induced constipation (OIC). White square: decision node (choice of strategy for evaluation); white circle: chance node (probabilities of ≥ two possible events); white triangle: terminal node (endpoint to be evaluated). The decision tree compares the prophylactic and standard, nonprophylactic use of naldemedine. In the prophylactic-use cohort, patients received prophylactic naldemedine in addition to standard osmotic or colon-stimulating laxatives throughout their lifetime. In the standard-use cohort, patients were not treated with prophylactic naldemedine but received standard laxatives for days 1–14. After day 14, patients who developed OIC were initiated on naldemedine.
The decision node represented the choice of naldemedine, with subsequent branches for prophylactic and nonprophylactic use. For patients receiving naldemedine as a prophylactic, health states such as the presence or absence of OIC were modeled using a chance node. Thereafter, branches led to terminal nodes indicating patient death. Thus, patients stayed in these health states for a lifetime.
The presence or absence of OIC was similarly modeled for patients receiving standard treatment. After day 14, an additional chance node was added for patients with OIC on standard treatment, with terminal nodes indicating death. Patients without OIC on standard treatment remained in their health states lifelong, whereas those with OIC stayed for 14 days. After day 14, patients with OIC stayed in their health states lifelong.
Regarding the prophylactic-use branch, we assumed that patients with or without OIC would receive prophylactic naldemedine (0.2 mg once daily) for a lifetime. 12 Concerning the standard-use branch, we assumed that patients would not receive prophylactic naldemedine during the first 14 days. Those who developed OIC would initiate naldemedine after day 14. This approach aligns with clinical guidelines for OIC, recommending naldemedine with conventional laxatives.3,7,8
Regarding the decision tree model, we made assumptions based on previous research concerning naldemedine.10,11,13,17 These assumptions were as follows: (1) patients would continue lifetime naldemedine treatment once initiated on either prophylactic or nonprophylactic use; (2) constipation under prophylactic or standard use of naldemedine would be alleviated with rescue laxatives; and (3) the dosages of regular laxatives and strong opioids would remain unchanged throughout the analysis period. TreeAge Pro Healthcare 2024 (TreeAge Software, LLC, Williamstown, MA, USA) was used for modeling.
Outcomes estimation
The outcomes of each course in terms of quality-adjusted life years (QALYs) were estimated by assigning probabilities and utility weights to a decision tree obtained from existing literature.18,19
The probability of 35.4% for patients with OIC receiving prophylactic naldemedine in the prophylactic-use branch was adopted from the study by Hamano et al. 12 The probability of 83% for patients with OIC not receiving prophylactic naldemedine at the first chance node in the standard-use branch was obtained from this study as well. 12 Additionally, the probability of 28.9% for patients with OIC receiving naldemedine at the second chance node in the standard-use branch was adopted from the study by Katakami et al. 9
To estimate the outcomes in terms of QALYs, utility weights were assigned to various health states during the clinical course of the patients.18,19 These weights were calculated from the Patient Assessment of Constipation–QOL (PAC-QOL) questionnaire scores 20 reported in the study by Hamano et al., 12 utilizing the conversion formula developed by Hatswell et al. 21 Health states, defined by the presence or absence of OIC, were determined based on the BFI scores. A BFI score ≥ 28.8 indicated the presence of OIC, whereas a BFI score < 28.8 indicated its absence, as outlined in previous clinical studies.9,12,22 These variables are presented in Table 1. We assumed the time horizon to be a lifetime, based on a median survival of 74 days for patients with cancer initiating strong opioids, as reported by Maeda and Ikoma. 23
Model Assumptions
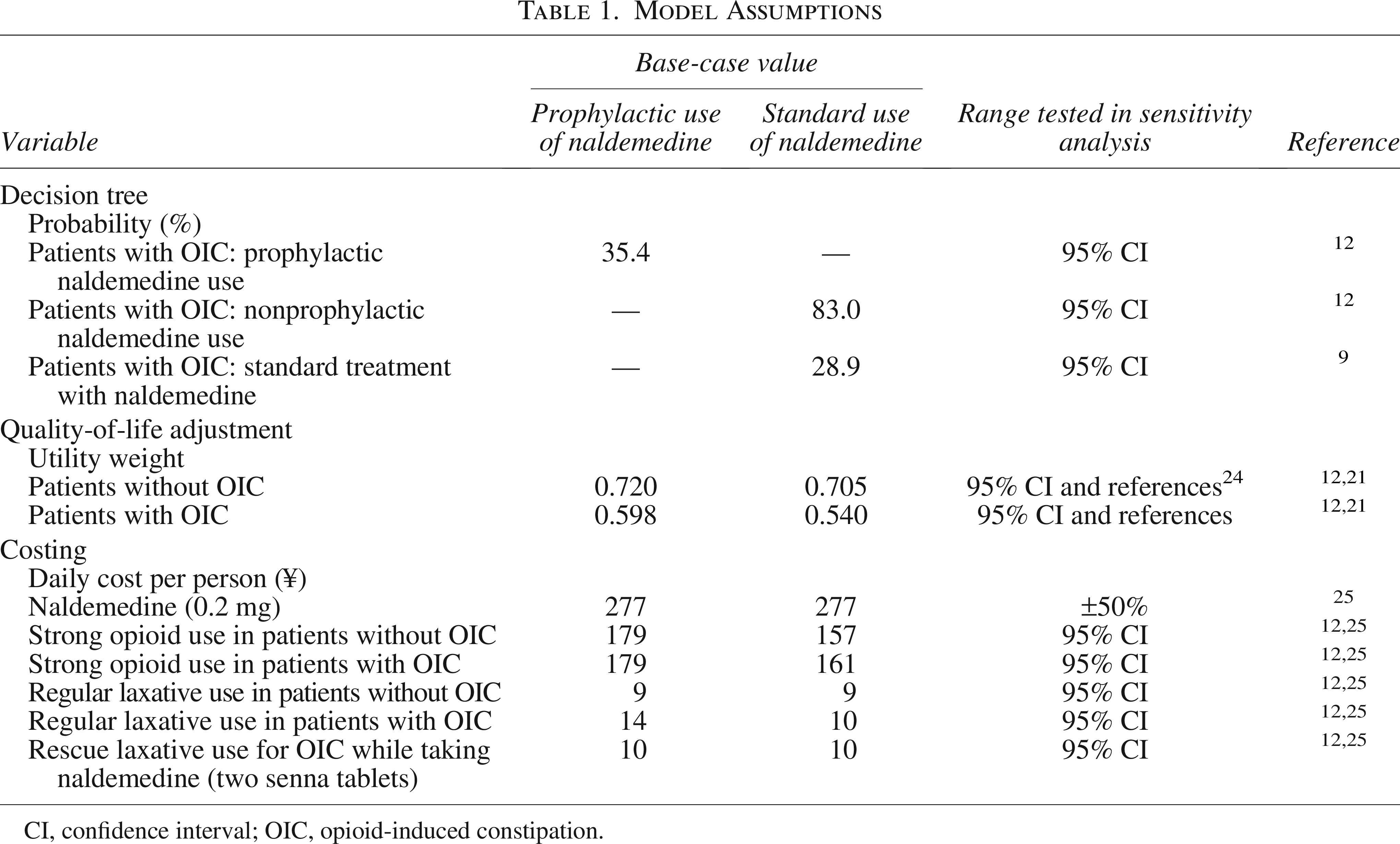
CI, confidence interval; OIC, opioid-induced constipation.
Costing
In the Japanese health care system, health care costs are shared between social insurers, who provide reimbursements, and patients, who make copayments. The estimated costs were derived from the direct payments made to health care providers by both social insurers and patients. Conversely, non-direct medical and long-term care costs were not considered. Cost items associated with treatment and health status were identified using an economic model.
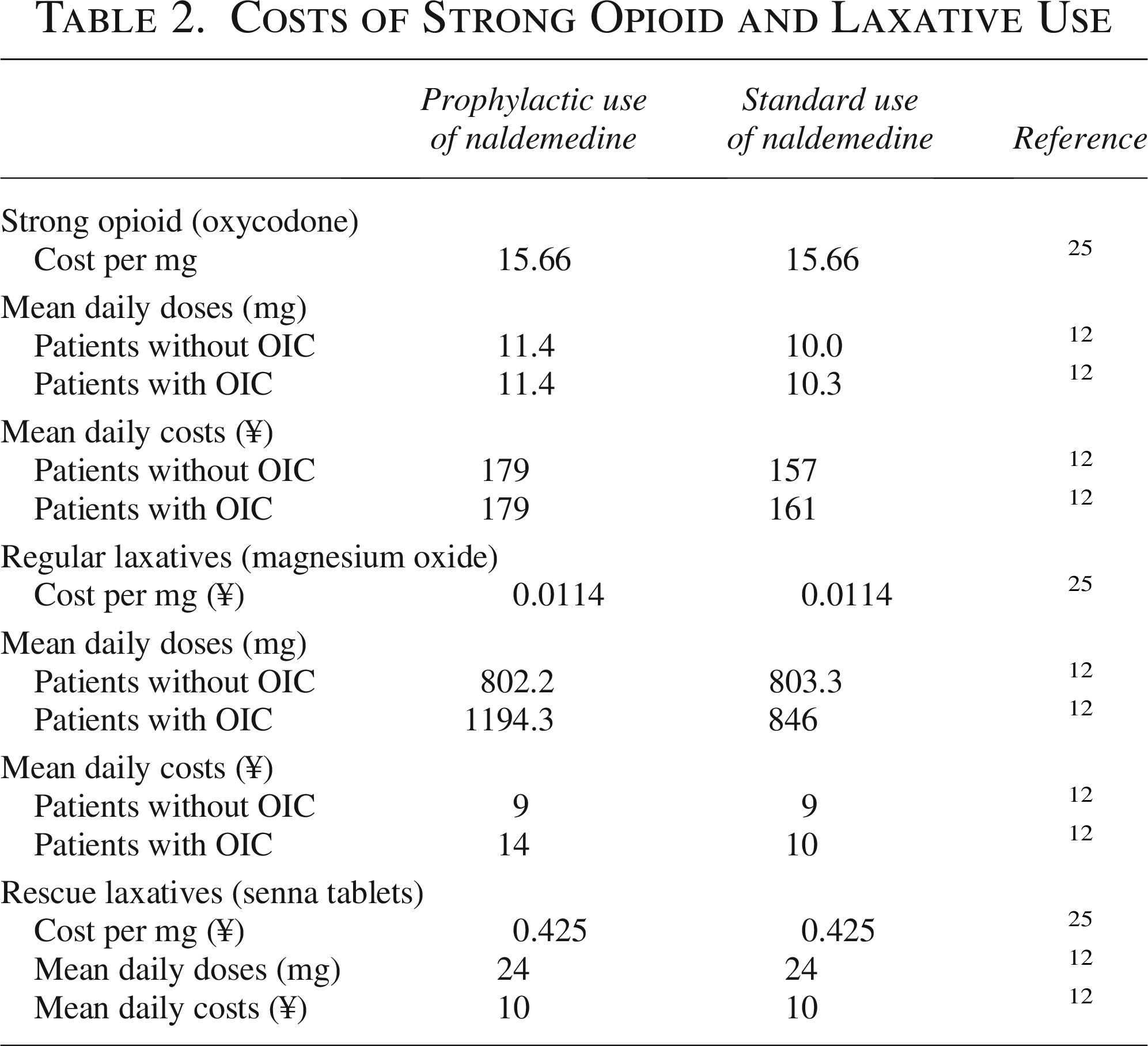
The daily cost of 0.2 mg of naldemedine was estimated at 277 Japanese yen (¥) per person, which was approximately 1.8 United States dollars (USD), based on an exchange rate of 1 USD = 150 ¥. 25 The daily costs of strong opioids and regular and rescue laxatives for each cohort were calculated using secondary data reported by Hamano et al. 12 These values are presented in Tables 1 and 2.
Costs of Strong Opioid and Laxative Use
Discounting
Because the time horizon was <1 year, the costs and effects were not discounted in this analysis.
Comparison
We calculated two summary measures, the ICER and net monetary benefit (NMB), for each treatment using our economic model.18,19 The ICER is defined as follows:
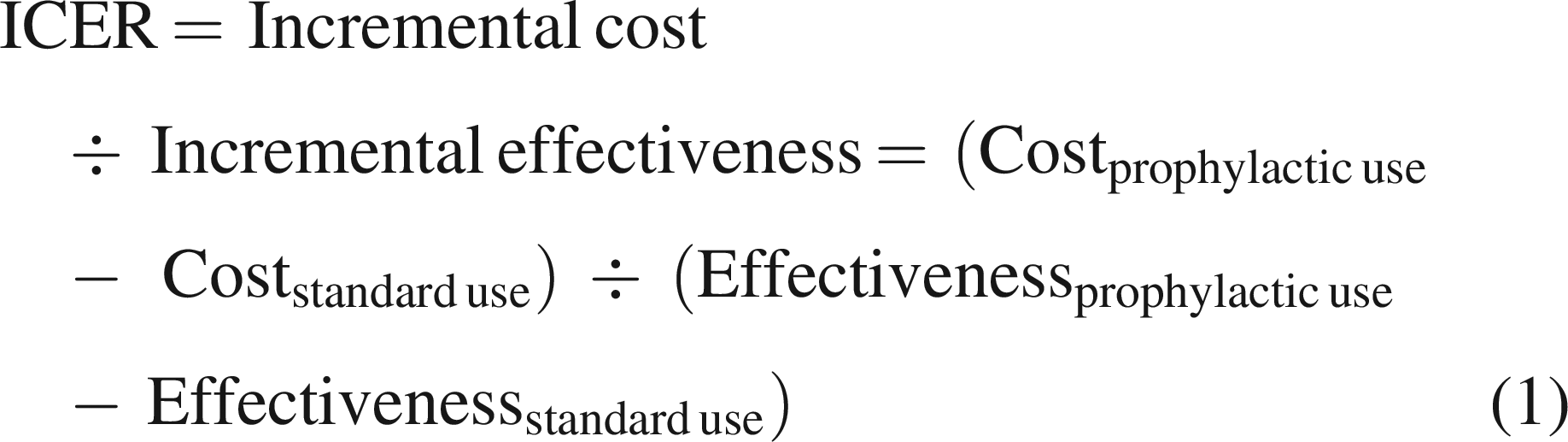
This measure represents the additional cost required to gain one more QALY under the new treatment. In Japan, an official threshold exists for judging the cost-effectiveness of public health programs; therefore, a willingness-to-pay threshold of 5 million ¥, or 33,333 USD, per QALY gained was applied. 16 This applies to all cost-effectiveness analyses for new treatments or programs, regardless of the level of cost.
The NMB is defined as follows:

The NMB is a summary statistic that expresses the value of a new treatment in monetary terms, with the willingness-to-pay threshold defined by a unit of benefit, such as the QALY in this study. A positive incremental NMB signifies that the new treatment is cost-effective compared with the alternative at the given specified threshold, indicating that the cost of achieving the benefit is less than the maximum amount a decision maker would be willing to pay for it.
Sensitivity analysis
Economic modeling relies on a series of assumptions derived from various sources. Therefore, assessing the stability of the model was essential. To evaluate the impact of the variables on cost-effectiveness, we conducted one-way and probabilistic sensitivity analyses using 1,000 Monte Carlo simulations. The lower and upper limits for probabilities and cost items, excluding naldemedine, were based on the 95% CIs from the clinical trial. 12 The cost of naldemedine varied by 50%. The range of utility weights was derived from 95% CIs in the clinical trial 12 and previously reported utility weights in patients with cancer.24,25 The survival time ranged from 31 to 277 days, based on the 95% CIs from the study by Maeda and Ikoma. 23 A triangular distribution was applied to each variable in the probabilistic sensitivity analysis.
Results
Cost-effectiveness findings
We present the results of the cost-effectiveness analysis in Table 3. The incremental cost of prophylactic use was 8,257 ¥, or 55 USD. Moreover, the incremental effectiveness of prophylactic use was 0.00571 QALY when compared with the standard, nonprophylactic use. The estimated ICER was calculated as 1,445,276 ¥ or 9,635 USD per QALY for the base case. Based on 5 million ¥ or 33,333 USD per QALY as a willingness-to-pay threshold, 16 the incremental NMB prophylactic use was 20,293 ¥ or 135 USD.
Results of Cost-Effectiveness Analysis
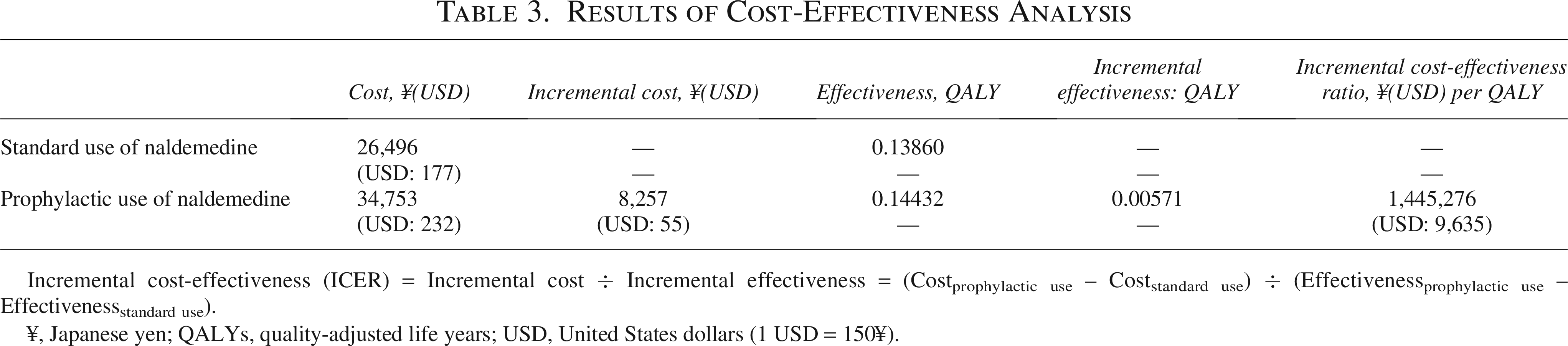
Incremental cost-effectiveness (ICER) = Incremental cost ÷ Incremental effectiveness = (Costprophylactic use – Coststandard use) ÷ (Effectivenessprophylactic use – Effectivenessstandard use).
¥, Japanese yen; QALYs, quality-adjusted life years; USD, United States dollars (1 USD = 150¥).
Sensitivity analysis results
Figure 2 presents the results of the one-way sensitivity analysis. This tornado diagram shows 10 variables that are sensitive to changes in the assumptions. Moreover, a threshold for judging cost-effectiveness was drawn, following the official social willingness-to-pay value of 5 million ¥, or 33,333 USD, for one QALY gain in Japan. 16 The survival time was the most sensitive to changes in assumptions, followed by the cost of naldemedine.
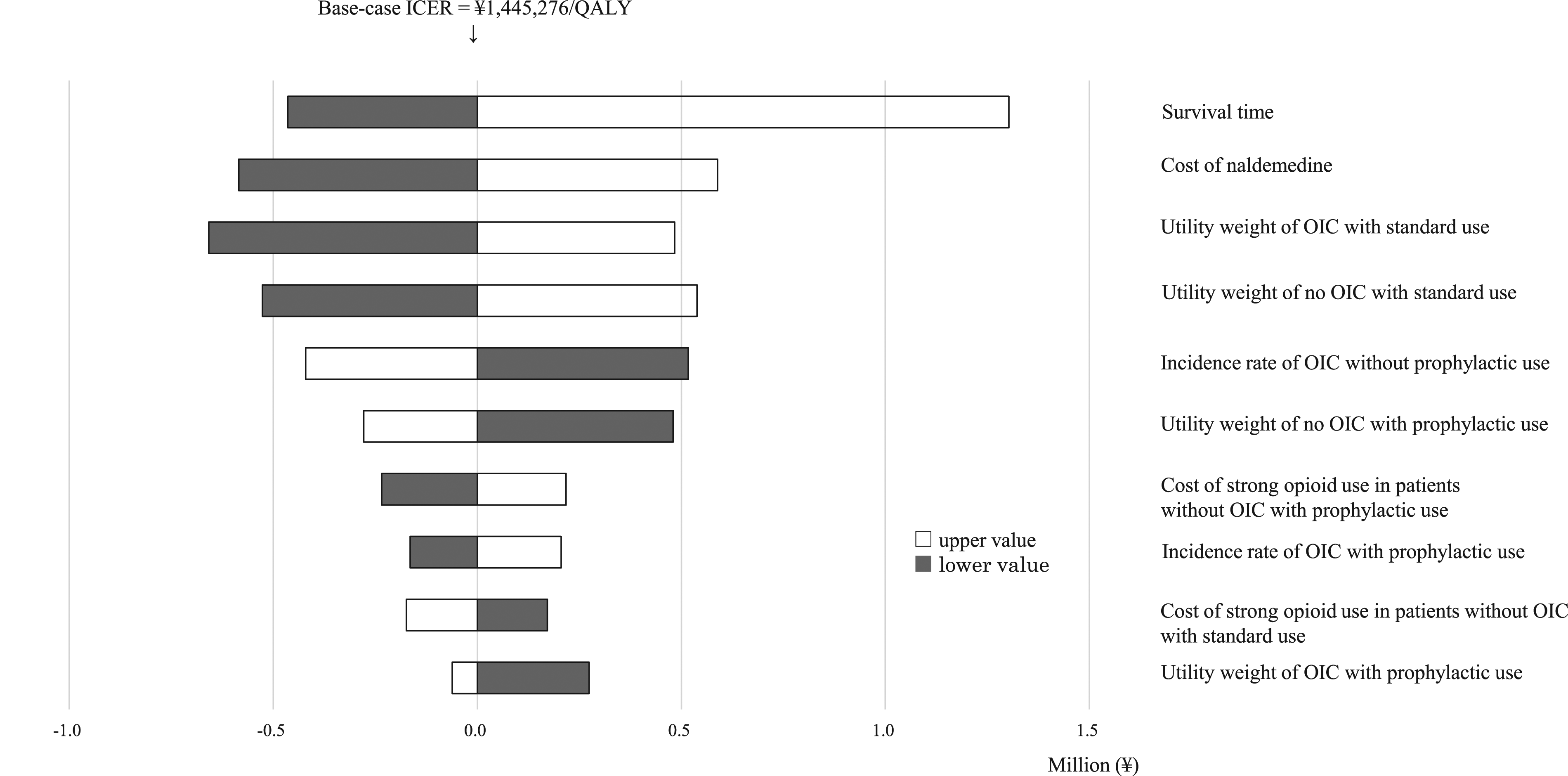
Tornado diagram. The tornado diagram depicts the results of the one-way sensitivity analysis. The 10 variables are ordered according to the magnitude of the ICER change, from largest to smallest. ICER changes are represented by white bars for increases and black bars for decreases in the variables, relative to the base-case value. ICER, incremental cost-effectiveness ratio; OIC, opioid-induced constipation; QALY, quality-adjusted life year.
Cost-effectiveness acceptability curve
As per the probabilistic sensitivity analysis, Figure 3 presents the cost-effectiveness acceptability curve. The probability that the ICER was < 5 million ¥ or 33,333 USD per QALY gained was 99.2%.
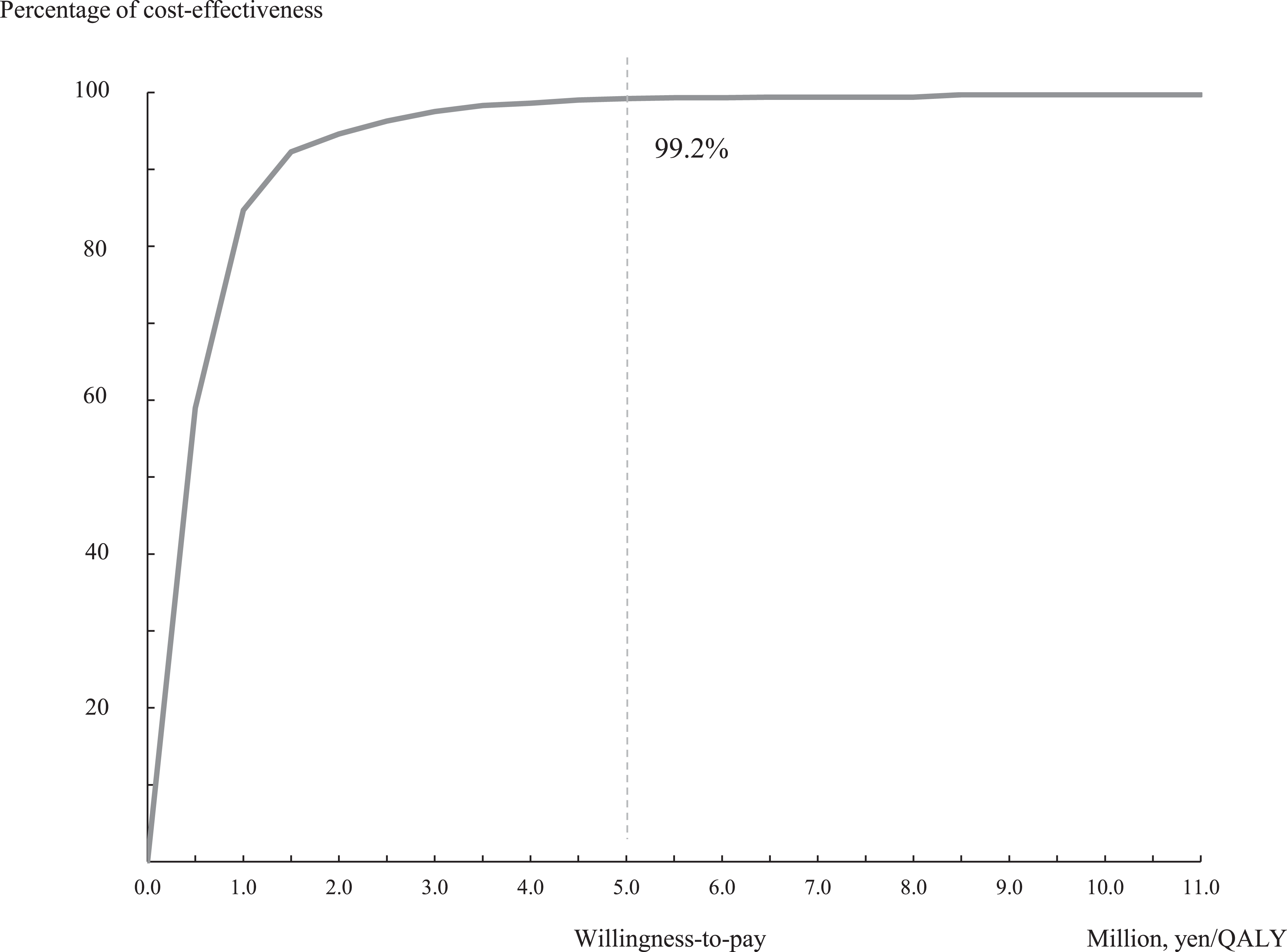
Cost-effectiveness acceptability curve. Of the 1,000 incremental cost-effectiveness ratios (ICERs) generated by the Monte Carlo simulation, the probability is 99.2%. This probability indicates that the ICER for the intervention, when compared with standard care, falls below the cost-effectiveness threshold of 5 million Japanese yen (\) or 33,333 United States dollars (USD), per quality-adjusted life years gained.
Discussion
We conducted a cost-effectiveness analysis of prophylactic naldemedine for OIC in patients with cancer initiating strong opioid therapy. Our base-case analysis indicated that prophylactic naldemedine would cost more and gain more. The estimated ICER was 1,445,276 ¥, or 9,635 USD, per QALY, which is below Japan’s official willingness-to-pay threshold of 5 million ¥ or 33,333 USD for one QALY gain from resource-consuming interventions. 16 Prophylactic naldemedine for OIC in patients with cancer was found to be cost-effective.
This is the first global cost-effectiveness analysis of prophylactic naldemedine for OIC in patients with cancer. Economic evaluations are essential for novel, more expensive agents that have demonstrated efficacy and safety4,6; however, few studies have addressed cost-effectiveness, particularly in palliative care.26,27 Owing to recent clinical evidence supporting the use of PAMORAs, including naldemedine,9–12 cost-effectiveness analyses are required. A report from the Netherlands investigated the cost-effectiveness of treating OIC with methylnaltrexone, one of the PAMORA, in patients with advanced illness, including cancer. The authors reported that methylnaltrexone plus standard care (including colon-stimulating laxatives, osmotic agents, and stool softeners) was cost-effective based on the acceptable threshold for the country. 26 In another cost-effectiveness analysis conducted by the UK National Institute for Health and Care Excellence as part of its health technology assessment process, naldemedine for the treatment of OIC was described as dominant, which was less costly and more effective. 27 Considered together with these studies,26,27 our findings provide important economic evidence for preventing OIC and improving palliative care worldwide.
Moreover, our study has implications for the current clinical guidelines on managing constipation in patients with advanced cancer.3–5,7,8 Guidelines are informed by the best available research evidence to support decision makers, clinicians, and patients in improving the quality of care and optimizing the use of limited resources. Economic evaluations should be integrated into the guideline development process to address cost and resource allocation considerations. 27 Magnesium oxide, a conventional laxative, is the most commonly used drug for the treatment of OIC, owing to its safety, widespread availability, and low cost.3–5,10,11,13 Our study on prophylactic naldemedine provided important economic evidence, inferring that prophylactic naldemedine should be strongly considered as the new standard management for OIC in the next revision of the clinical guidelines.3–5,7,8
Our sensitivity analysis revealed the robustness of this economic model based on clinical trial data, 12 as changes in all variables remained below the threshold for cost-effectiveness. 16 The utility weights for OIC, ranging from 0.540 to 0.598 and calculated from the PAC-QOL scores, were higher than the 0.39–0.41 range reported in previous studies.24,25 Notably, 80% of study participants in the RCT by Hamano et al. 12 were outpatients with abdominal cancer, who might have experienced a better QOL, even in the terminal stages. Our sensitivity analysis on utility weights, including previously reported values,24,25 showed that variations within these ranges did not affect the base-case results.
This study has some limitations. First, we did not consider adverse events 10 or the potential preventive effects of naldemedine on opioid-induced nausea and vomiting, 29 as these were not evaluated over a long-term study period.9–12
Second, we did not account for newer drugs in palliative care, such as hydromorphone and lubiprostone, where generic alternatives were not available. Third, the ICER reported in this study may not be directly applicable to other countries, owing to differences in health systems and willingness-to-pay thresholds for novel resource-consuming treatments. Nevertheless, our findings are relevant for high-income countries.
Conclusions
Our results revealed that prophylactic naldemedine for OIC in patients with cancer initiating strong opioid therapy is cost-effective. We recommend its inclusion in the clinical guidelines as a new standard for managing OIC, based on its value for money. Proper management of OIC with prophylactic naldemedine may enhance opioid adherence and improve pain control in patients with cancer.
Authors’ Contributions
R.O.: Conceptualization, formal analysis, methodology, software, visualization, and writing—original draft. T.H.: Conceptualization, data curation, formal analysis, and writing—review and editing. M.K.: Conceptualization, funding acquisition, and writing—review and editing. T.K.: Data curation, resources, and writing—review and editing. J.H.: Conceptualization, funding acquisition, project administration, resources, supervision, and writing—review and editing.
Data management and sharing
The datasets used and/or analyzed in the current study are available from the corresponding author upon reasonable request.
Footnotes
Acknowledgments
The authors thank the patients, their families, the study coordinators and investigators, and the study team.
Author Disclosure Statement
The authors declare that there are no conflicts of interest.
Funding Information
This study was funded by the University of Tsukuba: Grant for Implementation of Advanced Medicine (GIAM) and a Grant for Research Advancement on Palliative Medicine, Japanese Society for Palliative Medicine (No. 192).