
Abstract
Background:
Little is known about how Mozambicans feel about end-of-life preferences, especially their preferences for truth-telling in serious illness.
Aim:
To understand the end-of-life preferences and priorities of Mozambicans in Maputo City Province and their preferences for truth-telling in serious illness.
Design:
A face-to-face community-based street survey was performed with Mozambican nationals, aged ≥18, and fluent in Portuguese.
Methods:
Using convenience sampling, structured interviews investigated preferences in a hypothetical scenario of serious illness such as cancer. Descriptive analysis examined variations. General data were collected about illness understanding/steps in treatment, experiences/preferences with death, preferences in decision making, and end-of-life priorities.
Setting/Participants:
The sample (n = 397) was stratified by province, age, and gender. Participants were from five districts of Maputo City Province.
Results:
The primary analysis was truth-telling. Binary logistic regression analyses were performed to explore the influence of age, gender, education, religion, and ethnicity on preferences for truth-telling. There was a statistically significant association with higher education and all variables examined: assessing the association between education/religion and the preference for truth-telling over all other responses (OR = 3.6, p = 0.002), as well as, education/religion and the preference of truth-telling to the individual, versus family (OR = 3.627, p = 0.020), and the association between education/ethnicity and the preference of telling-telling to the individual, not family (OR = 3.832, p = 0.015). Catholics were more likely to desire truth-telling to the individual versus family (OR = 2.975, p = 0.042).
Conclusions:
Those with higher education and Christian religion were more likely to desire doctors to tell the truth about diagnosis.
Key Message
Currently, there is no information about the end-of-life preferences and priorities of community-dwelling Mozambicans. This is the first look at what these are within Maputo City Province. This article will aid in the continued formation of palliative care in Mozambique. Knowing what the population wants, resources can be prioritized.
Introduction
Mozambique is located on the south-eastern coast of Africa. The official language is Portuguese, but over 40 languages are spoken. A 2023 census reported the population at 32,419,747. 1 Maputo City Province is the capital with a population of 1,133,235. 2 Only about one-third of the population resides in urban areas. 3 Over half of the country identifies with some form of Christianity, and about a fifth is Muslim. 3
An estimated 62% of the Mozambican population lives at or below the poverty level (US equivalent of $0.63/day). 4 The national health system covers less than half the population.5,6 Consequently, various diseases, such as cancer, are discovered late and are no longer curable. 7 In these cases, palliative care offers improved quality of life through pain control, spiritual attentiveness, emotional support, as well as a reduction of the overall cost of care. 8
Palliative care in Mozambique is in its infancy. 9 In Maputo, there is only one stand-alone pain unit in the central hospital offering palliative care, with a few non-governmental organizations doing small works. 10 For palliative care service to be effective, it is important to understand beliefs about illness origins and health-seeking behaviors to tailor support and care to match the needs of patients and their communities. To foster trust when approaching the topic of palliative care with the patient and family, medical professionals need to know if there is a general preference for truth-telling and what the comfort level is for discussing end-of-care and death.
This study gathered information about the end-of-life care preferences and priorities of community-dwelling individuals in Maputo City Province. With this information, it will be possible to design a program with priorities that match. Information collected creates a knowledge base that future research may build, both benefitting Mozambique and palliative care in southern Africa, as many cultural similarities exist across borders.
Methods
Study design and participants
A face-to-face community-based street survey was performed with Mozambican nationals, aged ≥18, and fluent in Portuguese. Using convenience sampling, structured interviews investigated preferences in a hypothetical scenario of serious illness such as cancer. The survey was conducted on 15 streets across five of the seven districts of Maputo City Province. Two districts were excluded due to lower population and access (accessible only by boat or tolled bridge).
Measures
The preliminary questionnaire was developed by the first author (L.D.H.) with input from coauthors. Questions were formed using previous research both of already established end-life surveys and end-of-life in sub-Saharan Africa, and the 15 years of experience of L.D.H. living and working in Mozambique alongside the health department. Once an initial draft was established, two focus groups were used to critique and refine the survey. The first focus group included four professionals working within Maputo Central Hospital, with frequent experience with end-of-life patients. The second group included five Mozambican nationals. Given that the official language of Mozambique is Portuguese, the survey was initially developed in English, the first-language of the primary researcher (L.D.H.), then translated into Portuguese using Google Translate. Wording was honed during focus groups. The finalized version was certified by a professional translator. A full version is available in Supplementary Appendix SA1.
The final survey covered topics of demographics, illness understanding, patient practices, preferences in decision making, patient/physician communication, comfort talking about death, personal experience with death, preferred location of death, importance ratings of topics at the end-of-care, preferences if treatment stops working, imagining a “good death,” and about afterlife and ancestralism. Most were multiple-choice or yes/no questions, though there were a few open-ended questions which the interviewers summarized.
Sampling and data collection
A street survey methodology was used, modeled after surveys done in Kenya and Namibia.11,12 Sixteen Mozambican interviewers were hired, trained, and sent in teams of two, over four days in March of 2025 to 15 different locations across 5 of the 7 districts on Maputo City Province. The locations were divided across the districts based primarily on population concentration but also depending on the busyness of streets/markets and the safety of interviewers. Interviews were conducted in the mornings due to traffic and favorable temperatures. Each interview typically took 15–20 minutes to complete. Study size was determined by Cochran’s formula and the population. More information in . Interviewers used convenience sampling, approaching passersby appearing to meet the eligibility criteria: ≥18 years old, a Mozambican national, and fluent in Portuguese. After eligibility confirmation, the interviewer explained the purpose of the survey. If interested, an informed consent form was read to the potential participant, and verbal consent was acquired.
Given the low literacy rates in Mozambique, the questionnaire was read aloud to participants and responses were manually recorded by interviewers. 13 Once the interview was completed, participants were offered a 50 mt (0.80 USD) phone credit.
Data analysis
SPSS (v20) was used for analyses. Categorical data were summarized using frequencies and percentages. For comparison purposes, univariate binary logistic regression analyses were used to determine unadjusted odds ratios for individual variables. Multivariate binary logistic regression analyses were conducted to explore the influence of age, gender, education, religion, and ethnicity on the preference of community-dwelling Mozambicans from Maputo City Province for doctors to tell them the truth when imagining a serious illness, such as cancer, if treatment stopped working. The multivariate analysis models were as follows (note: models are referenced differently, numerically versus alphabetically, to distinguish between models involving different outcomes):
Age was grouped into five categories (Table 3), with “18–24” as the reference. Gender used “male” as the reference. Education was categorized as no schooling/primary (reference), secondary, and higher education (including professional certificates and university degrees). Religion was grouped as Christian (reference), Catholic, and other/no religion; although Catholicism is a form of Christianity, it was analyzed separately due to local distinctions in Mozambique. Ethnicity was categorized as Changana (reference), Tsonga, Chuabo, and other.
Each model’s statistical significance was evaluated using the Omnibus Tests of Model Coefficients. Goodness-of-fit was assessed via the Hosmer–Lemeshow test. Variance explained was measured using Cox & Snell R2 and Nagelkerke R2, with odds ratios and 95% confidence intervals reported.
Results
Participants’ characteristics
See Table 1.
Weighted Characteristics of Participants (n = 397)
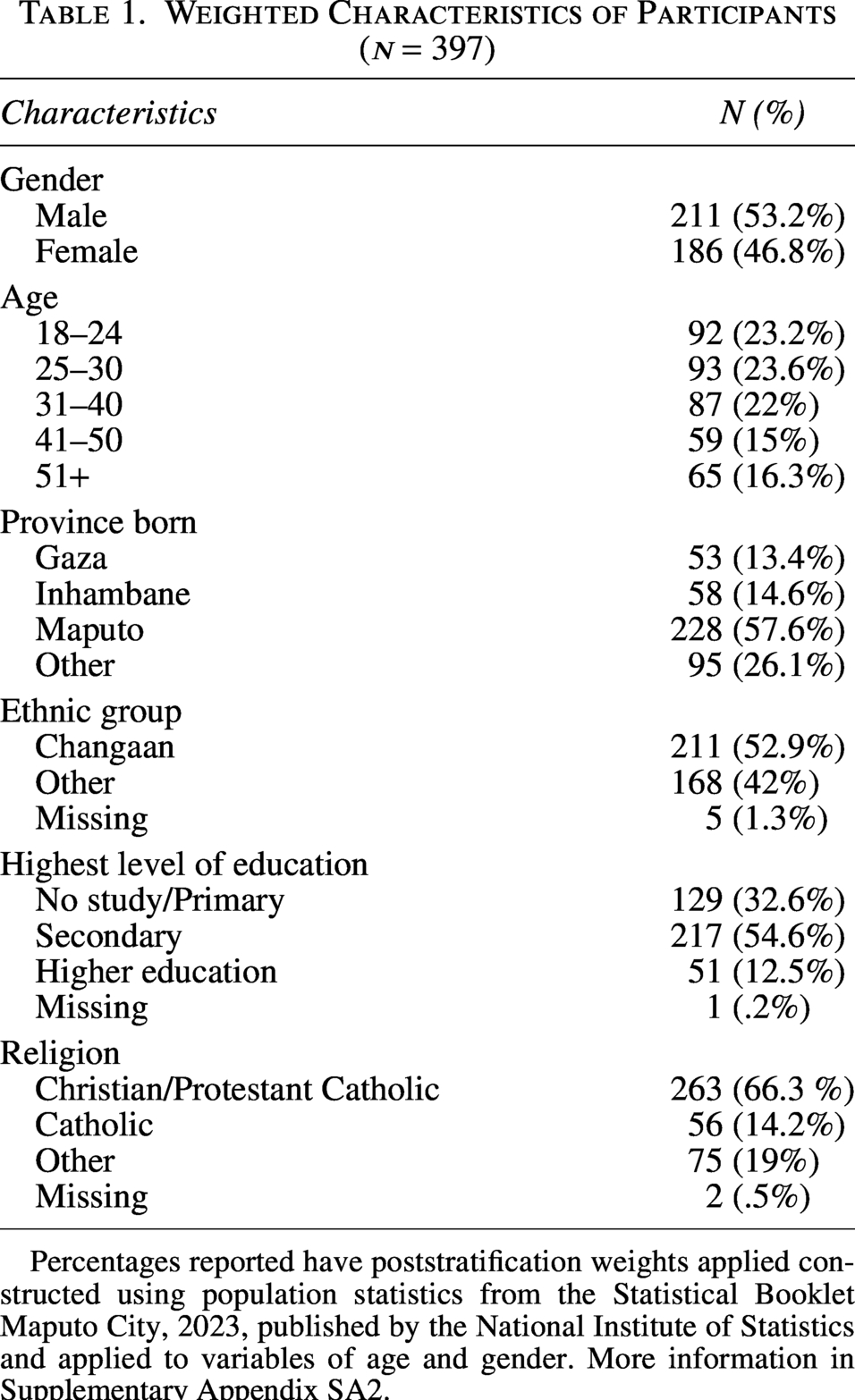
Percentages reported have poststratification weights applied constructed using population statistics from the Statistical Booklet Maputo City, 2023, published by the National Institute of Statistics and applied to variables of age and gender. More information in Supplementary Appendix SA2.
Categorical summaries
The categorical summaries provided an overview of the reported beliefs, experiences, practices, preferences, and priorities of Mozambicans in Maputo City Province. Table 2 provides complete details.
Summary of Categorical Survey Results (N = 397)
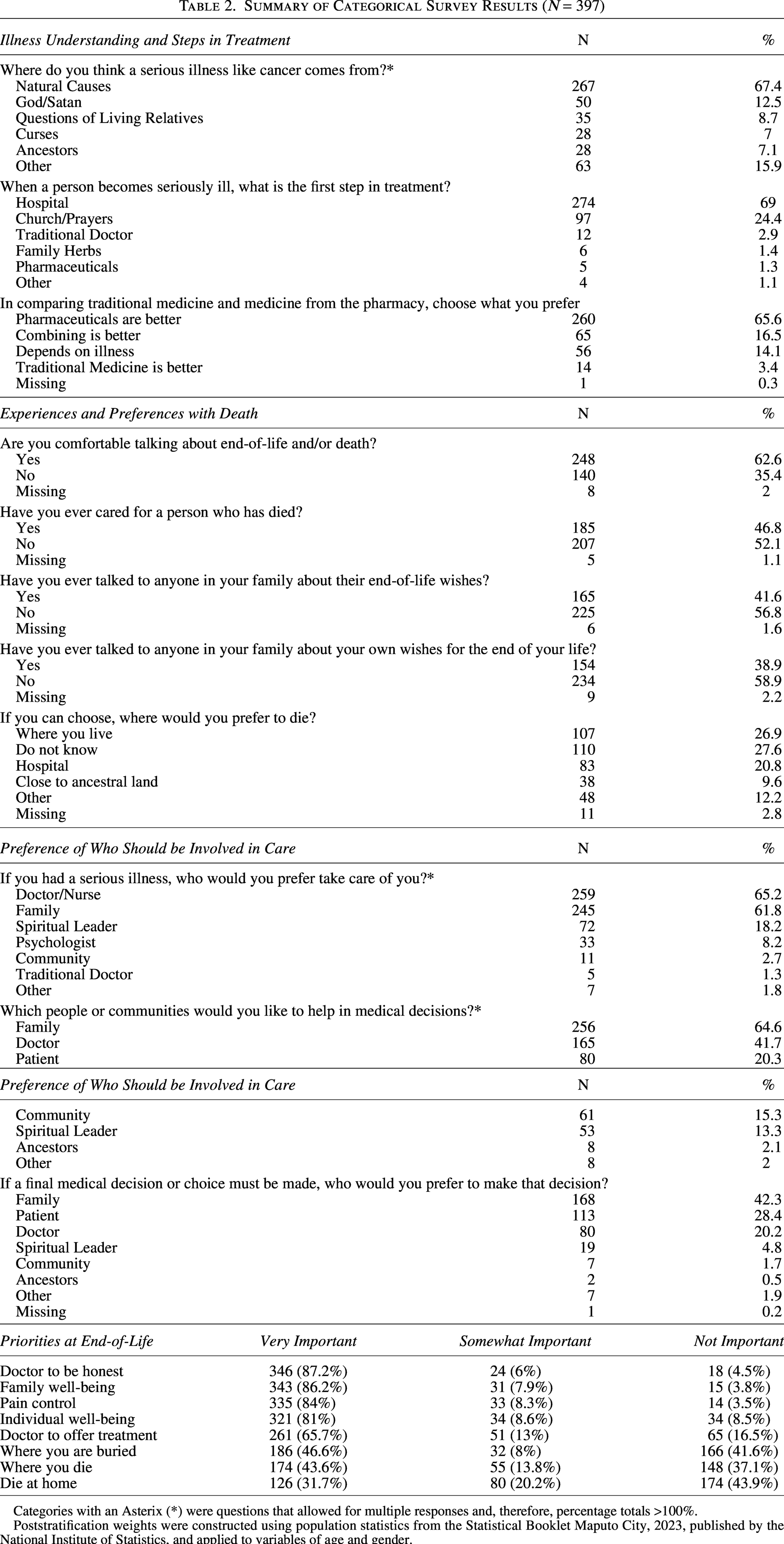
Categories with an Asterix (*) were questions that allowed for multiple responses and, therefore, percentage totals >100%.
Poststratification weights were constructed using population statistics from the Statistical Booklet Maputo City, 2023, published by the National Institute of Statistics, and applied to variables of age and gender.
Primary analyses
For the primary analyses, the outcome was truth-telling. Adjusted Models 1 and 2 used binary logistic regression to compare “doctor to tell me the truth and let me decide” versus all other responses. Adjusted Models A and B compared “doctor to tell me the truth and let me decide” with “doctor to tell my family, not me” (Table 3).
Logistic Regression Models Predicting Preferences for Doctor Communication About Terminal Illness
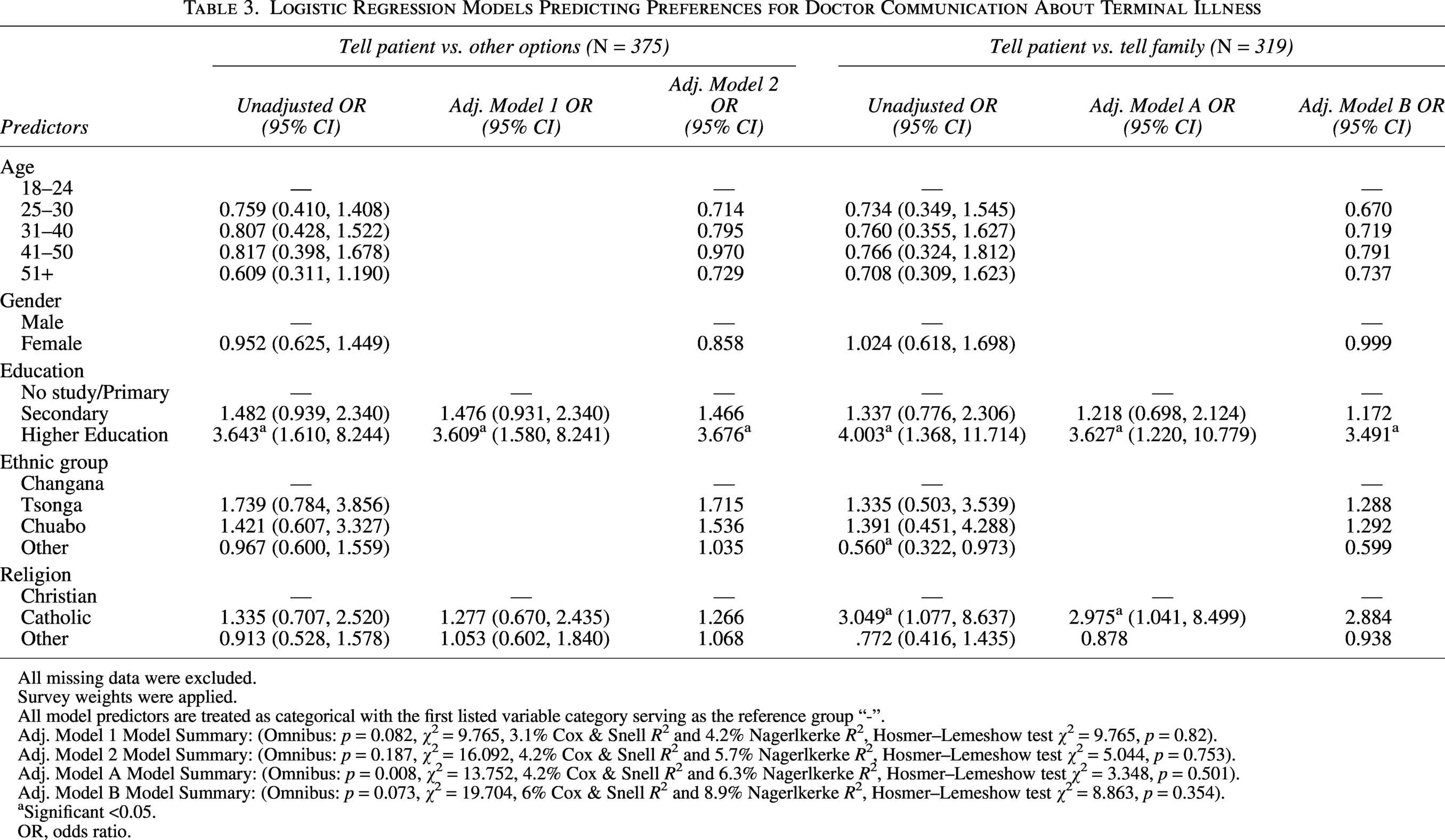
All missing data were excluded.
Survey weights were applied.
All model predictors are treated as categorical with the first listed variable category serving as the reference group “-”.
Adj. Model 1 Model Summary: (Omnibus: p = 0.082, χ2 = 9.765, 3.1% Cox & Snell R² and 4.2% Nagerlkerke R², Hosmer–Lemeshow test χ2 = 9.765, p = 0.82).
Adj. Model 2 Model Summary: (Omnibus: p = 0.187, χ2 = 16.092, 4.2% Cox & Snell R² and 5.7% Nagerlkerke R², Hosmer–Lemeshow test χ2 = 5.044, p = 0.753).
Adj. Model A Model Summary: (Omnibus: p = 0.008, χ2 = 13.752, 4.2% Cox & Snell R² and 6.3% Nagerlkerke R², Hosmer–Lemeshow test χ2 = 3.348, p = 0.501).
Adj. Model B Model Summary: (Omnibus: p = 0.073, χ2 = 19.704, 6% Cox & Snell R² and 8.9% Nagerlkerke R², Hosmer–Lemeshow test χ2 = 8.863, p = 0.354).
Significant <0.05.
OR, odds ratio.
Adjusted Model 1: Truth-telling versus all other options (education, religion)
This model examined how education and religion influence preferences among respondents imagining a serious illness—specifically, whether they prefer doctors to disclose the truth and allow them to decide versus other options. Education beyond secondary school was significant, indicating a stronger preference for being told the truth about ineffective treatment. Respondents with higher education were 3.6 times more likely to prefer truth disclosure than those with the lowest education level. See Table 3 for details.
Adjusted Model 2: Truth-telling versus all other options (age, gender, education, ethnic group, religion)
Adjusted Model 2 was similar to Model 1 but added age, gender, and ethnicity. The overall model was not significant, yet results were similar: only higher education predicted a preference for truth-telling when treatment is ineffective. Age, gender, and ethnicity showed no influence.
Adjusted Model A: Truth-telling to the patient versus truth-telling to the family, not the patient (education, religion)
This model examined how education and religion influence preferences among respondents imagining a serious illness—specifically, whether doctors should tell them the truth or inform their family instead. Being Catholic was significant (OR = 2.975, p = 0.042), with Catholics 2.975 times more likely than non-Catholic Christians to prefer direct disclosure. Higher education was also significant (OR = 3.627, p = 0.020), with respondents 3.627 times more likely to prefer being told the truth rather than their family. See Table 3 for details.
Adjusted Model B: Truth-telling to the patient versus truth-telling to the family, not the patient (age, gender, education, ethnic group, religion)
As with Models 1 and 2, Model B was not statistically significant, but results trended similarly to Model A.
Discussion
Our innovative survey exploring public preferences and experiences about life-threatening illness is the first of its kind in Mozambique.
Illness understanding and steps in treatment
Beliefs about illness causation often determine health-seeking behaviors.14–17 Understanding these can help doctors better support individual decision making. 18 Though most participants reported they would go to the hospital first, almost a third reported they would try something else first. Presentation to the hospital may only happen after disease progression.19–21
More than a third of people believed that combining traditional medicine and pharmaceuticals is better, that certain illnesses are better treated by traditional medicine, or that traditional medicine is best. Many factors contribute to the use of traditional medicine, but rural and low socioeconomic patients tend to have a higher usage.22–24 This is important because of the known potential for adverse reactions and interactions.25,26 Patients often will not disclose use of traditional medicine on their own; thus, it is important for doctors to ask whether they have tried anything else, providing a more complete patient history, and aiding in future medical decisions.26–28
Experiences and preferences with death
This study is the first to ask Mozambicans about their comfort talking about death. A majority expressed comfort with the topic (62.6%), despite the thought of death as a taboo topic in African countries and often avoided by providers.29–31 Research from non-Mozambican samples shows many Africans want to know their prognosis.32,33 Similarly, our survey found 63.5% of respondents want the truth when treatment stops working.
Almost half of the respondents had cared for someone who died. When asked where the respondent preferred to die, home was most frequently preferred, followed closely by “unknown” and preference for the hospital. With 28% of people not knowing, and given the willingness to discuss death, the potential for education and conversation facilitation is highlighted.
Preference of who should be involved in care
Respondents most commonly chose doctors and families to be involved in caring for the patient. As in other African countries, respondents preferred for the family to be involved in decision making and final decisions.11,12 This reinforces the importance of having family members involved in medical consults.
Priorities at end-of-life
Respondents indicated their priorities at the end-of-life to be: the doctor to be honest, family well-being, pain control, and individual well-being were most commonly selected to be “very important,” in that order. Given the communal nature of African societies, an emphasis on family well-being was expected. Less expected was that 87% of people said it was very important for the doctor to be honest. Doctors need to trust the public to handle information about serious illness and should be adequately trained to facilitate difficult conversations and navigate patient emotions. 34 Less important to respondents were dying at home, location of death, and burial location. This appears somewhat contrary to the cultural significance of burial sites in Africa.35–37 More exploration is needed to understand Mozambican preferences for burial and beliefs about the afterlife. If the importance of burial location is indeed shifting, urbanization and religion are possible contributors.38–40
Discussion multivariable models
Education was significant across all models with odds ratios ranging from 3.4 to 3.64, indicating that higher education is associated with a preference for truth-telling to the individual. This is consistent with other studies globally.32,41–45 Being able to understand information given regarding an illness may contribute to this association. More educated patients may be better able to understand prognoses and potential treatment options, due to greater health literacy. 46 While this survey question asked about a preference for telling the patient the truth directly, more research is necessary to explore whether truth-telling is preferred directly to the individual or mediated through relatives.
Religion was significant in Adjusted Model A, where Catholics in Maputo City Province had 3× the odds as non-Catholic Christians to prefer truth-telling to the individual over telling the family. This could be due to doctrinal influences or other culturally catholic beliefs or expectations. The Catholic church values truth; however, there are conflicts between truth-telling and a concern for hurting patients. 47 There is still an encouragement to tell the truth in a compassionate, slow manner. More research is needed to understand Catholics in Maputo City Province’s preference for truth-telling to the individual.
Reflections, strengths, and limitations of the study
This research has several limitations. The study was limited to Maputo City Province, thus, findings cannot be extrapolated to all Mozambicans. Another limitation is the use of convenience sampling, which may limit generalizability. Streets and locations were selected based on foot traffic, and diverse locations were selected to reduce bias. Nonresponse bias may further limit the representativeness of findings, as those who participated in the survey were likely more socially outgoing and willing to communicate openly than nonparticipants. Because the questionnaire was administered face-to-face to elicit respondents’ subjective perspectives, there was the potential for response bias, such as social desirability bias and recall bias. The questionnaire also used a hypothetical situation; however, preferences and priorities may shift when the individual is actually sick.
Conclusion
This study gives the first glimpse into what Mozambicans prefer and prioritize during serious illness and at the end of life. In Maputo City Province, while most people report that illness comes from natural causes, that they go to the hospital first, and that they view pharmaceuticals as best, illness can also be viewed as spiritual in nature, and as such, treatment may include options outside the medical system, including traditional and spiritual interventions.
Mozambicans view family as an integral part of care and decision making, even more so than the individual. Decision making should involve family members. There seems to be general comfort talking about the concept of death, and thus, there is potential for growing the field of advance care conversations. Though a majority of people want their doctors to be honest with them and prefer to die where they live, there are still individuals who feel differently. Conversations must happen early enough to understand what the patient and family want and support these wishes.
Education and religion influence a Mozambican’s preference for truth-telling. This understanding can help guide doctors in their end-of-care conversations and guide the goal of care. If a patient has a higher education and/or is a Catholic, the likelihood of wanting to know the truth is higher and thus should be explicitly explored.
Ethical Considerations
The study was approved by the Institutional Bioethics Committees for Health, Faculty of Medicine, Maputo Central Hospital (approval no. CIBS FM&HCM/142/2024 on November 26, 2024) and was determined exempt by the Institutional Review Board of the University of Maryland Baltimore in March 2025 (approval no. HP-00110555 on February 17, 2025).
Consent to Participate
Informed consent was obtained verbally from all participants and documented on questionnaire forms before proceeding with the questionnaire. Data were collected anonymously.
Data Availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Footnotes
Acknowledgments
The authors want to acknowledge and thank the data collection team: Amélia Tembe, Pedro Mutumane, Lino Eduardo Sicavele, Marta Didele, Suneida Chongola, Chelsia Chiúre, Rita Adélia António, Fátima Meiva Tamele, Nirma Herculano Rungo, Arsolina Carlos Baptista, Nelson Afonso, Maria António Ouana, Moisés Isac Mabjaia, Salomé C.U.F. Chaúque, Isabel Sarifo, and Celia Do Chingola.
Author Disclosure Statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
Funding was through the nonprofits Voices of the World Mozambique and Quiettime Ministries.
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.