
Abstract
Background:
Clinicians place comfort measures only (CMO) orders for hospitalized patients at the end-of-life when a decision has been made to focus on patient comfort and allow the natural dying process to occur.
Objectives:
Our primary aim was to assess the associations of specialty palliative consults (SPC) or documented goals of care conversations (GOCC) with in-hospital mortality among patients with CMO orders.
Design:
We completed a retrospective cross-sectional study of data from the electronic medical record.
Setting/Participants:
We assessed all adult patients with CMO orders admitted to four hospitals in the United States between 2022 and 2024.
Measurements:
We used descriptive statistics and multivariable logistic regression and linear regression models to identify the association of SPC and documented GOCC with patient outcomes.
Results:
Of 6789 hospitalized patients with CMO orders, 48% were female, and these patients had median age 71 years. Seventy-three percent died in-hospital, and 22% were discharged with hospice. SPC placed anytime during hospital admission were associated with lower in-hospital mortality (aOR 0.4, 95% CI 0.3–0.6, p < 0.0001) and higher discharge with hospice (aOR 2.4, 95% CI 1.8–3.2, p < 0.0001). In contrast, documented GOCC anytime during admission were associated with higher in-hospital mortality (aOR 1.8, 95% CI 1.3–2.4, p = 0.0004) and lower discharge with hospice (aOR 0.5, 95% CI 0.4–0.7, p = 0.0003).
Conclusions:
For patients with CMO orders, SPC, rather than documented GOCC, were associated with lower in-hospital mortality and higher receipt of hospice. Future research should explore reasons why only SPC, and not documented GOCC, were associated with these findings.
Keywords
Key Message
This multihospital study suggests that specialty palliative consults rather than documented goals of care conversations alone may aid in transitioning patients with comfort measures only orders to receive hospice care.
Introduction
Clinicians place comfort measures only (CMO) orders for hospitalized patients at the end-of-life (EOL) when a decision has been made to focus on patient comfort and allow the natural dying process to occur. 1 Previous studies have assessed the frequency and predictors of CMO orders in hospitalized adult patients.2,3 Less is known about what happens to patients after CMO orders are placed, such as the rate of in-hospital mortality and discharge with hospice.
Although most Americans prefer to die at home, many die during an acute care hospital admission.4,5 While previous studies identified that both specialty palliative consults (SPC) and documented goals of care conversations (GOCC) were associated with higher hospice enrollment for hospitalized patients, the relationship between these interventions when assessing only hospitalized patients with CMO orders where these patients are in the dying process and the focus is solely on comfort-focused care is unclear.6,7 These relationships should be assessed to better understand whether SPC and documented GOCC may be associated with a higher likelihood that patients with CMO orders receive EOL care outside of an acute care hospital admission or whether these interventions have little effect on this outcome for patients who have started the dying process.
Thus, our primary aim was to examine the associations of SPC or documented GOCC with in-hospital mortality among a sample of patients with CMO orders. We hypothesized that both SPC consults and documented GOCC would be associated with lower in-hospital mortality and higher discharge with hospice care for patients with CMO orders, as these interventions may increase the detection of patients with preferences to receive EOL care outside of an acute care hospital inpatient admission. We additionally aimed to examine the association of SPC or documented GOCC with other patient outcomes, including discharge with hospice and hospital length of stay among patients with CMO orders.
Methods
Overview and study design
We completed a retrospective cross-sectional study assessing only adult patients with CMO orders admitted to four acute care hospitals between 2022 and 2024. Hospitals included quaternary care and community hospitals. SPC services existed at all four hospitals and included physicians, advanced practice providers, social workers, music therapists, and chaplains. We did not assess hospitalized hospice patients admitted only for general inpatient care through hospice. The University of Pittsburgh Medical Center Quality Improvement Review Committee provided approval to pursue this study (project ID 2629).
Patient characteristics
We identified patient demographics from the electronic health record (EHR), including age, race, sex, and insurance status. We assessed comorbidity burden using the Charlson Comorbidity Index. We assessed patient severity of illness using the Serious Illness Risk Indicator (SIRI) score and intensive care unit (ICU) admission status. The SIRI score was created by the health system and calculated at admission to predict 90-day mortality risk at the time of the patient’s hospital admission, as has previously been described. 8 Patients with SIRI scores were stratified into four categories: having low (<30%), intermediate (30%–60%), or high (>60%) predicted risk of 90-day mortality or having no score. Some patients lacked a SIRI score due to having insufficient data within the EHR to calculate an accurate score on hospital admission. ICU admission included patients admitted to an ICU at any point during their hospital stay. We identified each patient’s hospital location (Hospital A, B, C, or D). We assessed patient outcomes including in-hospital mortality, discharge location including to hospice, and hospital length of stay. We also assessed the time from hospital admission to placement of a CMO order and time from CMO order placement to hospital death or discharge.
Identification of SPC and documented GOCC notes
We identified SPC by assessing completion of a palliative consult note in the EHR. We documented the time of completion of the palliative consult note to determine whether the SPC occurred early (defined as within 48 hours of hospital admission). 9 We identified documented GOCC by assessing for completion of a GOCC template note in the EHR. These GOCC notes were tracked by the health system with time of completion recorded in a standardized health system database. Documented GOCC occurring within 48 hours from hospital admission were defined as early GOCC. These GOCC notes included: (1) surrogate information, (2) discussion of prognosis, (3) patient values and preferences, (4) decisions made, and (5) next steps. 10 Clinicians at all study hospitals were actively encouraged by hospital leadership to document all GOCC conversations using this template note. Any type of physician or advanced practice provider (primary team or consulting teams including specialty palliative clinicians) was eligible at each study hospital to document GOCC using this template note. When multiple clinicians were present at a GOCC (e.g., ICU resident and SPC attending), it was recommended that only one clinician present at the meeting document the GOCC in the template note. Clinicians needed to address all five documented components of the GOCC note template to sign the note. We assessed all documented GOCC written by all clinician types (including specialty palliative clinicians and non-specialty palliative clinicians) and did not assess the quality of these notes. Template notes were commonly documented within this health system, with over 70% documentation rate for patients with >60% predicted risk of 90-day mortality and over 25% for patients with 30%–60% risk of 90-day mortality. 10
Statistical analysis
We described categorical variables as quantity and percent and continuous variables as median and interquartile range (IQR). We used Fischer’s exact, chi-square, and t tests as appropriate to compare categorical and continuous variables. We used multivariable logistic and linear regression models to assess the association of SPC and documented GOCC on patient outcomes. Models included the following factors: patient age, race, sex, insurance, Charlson comorbidity index, SIRI score, SPC status, documented GOCC status, the interaction of SPC status with documented GOCC status, and hospital location. We also used regression models to assess the association of early SPC and early documented GOCC on patient outcomes. These models included the following factors: patient age, race, sex, insurance, Charlson comorbidity index, SIRI score, early SPC status, early documented GOCC status, the interaction of early SPC status with early documented GOCC status, and hospital location. We completed these analyses both on the overall cohort of patients with CMO orders and the cohort of patients with CMO orders surviving greater than 48 hours into hospital admission. We chose to also specifically assess patients with CMO orders who survived greater than 48 hours to evaluate the population of patients who had adequate opportunity to receive an SPC, have a GOCC note documented, and be discharged with hospice care. All models included the interaction term between SPC status and documented GOCC status to address the relationship that may exist between these variables.
Results
Three percent (n = 6789/267,375) of adult patients hospitalized at the four study hospitals had a CMO order placed during hospital admission. The 6789 patients with CMO orders had median age 71 years, were 48% female, and were 8% Black, 2% Other, and 90% White race. Forty-five percent of patients with CMO orders were admitted to an ICU, 73% died in-hospital, 22% were discharged with hospice care, and 5% were discharged without hospice care. For patients 22% of patients with CMO orders who were discharged with hospice, 56% were transitioned to inpatient hospice care, and 44% were discharged home with hospice. Of those transitioned to inpatient hospice, 67% had an SPC. The median length of hospital stay was 7.1 days (Table 1). The median time from hospital admission to CMO order placement was 6.4 days and from CMO order placement to discharge was 0.2 days (Supplementary Table S1).
Patient Characteristics by Specialty Palliative Consult Status for Patients with Comfort Measures Only Orders
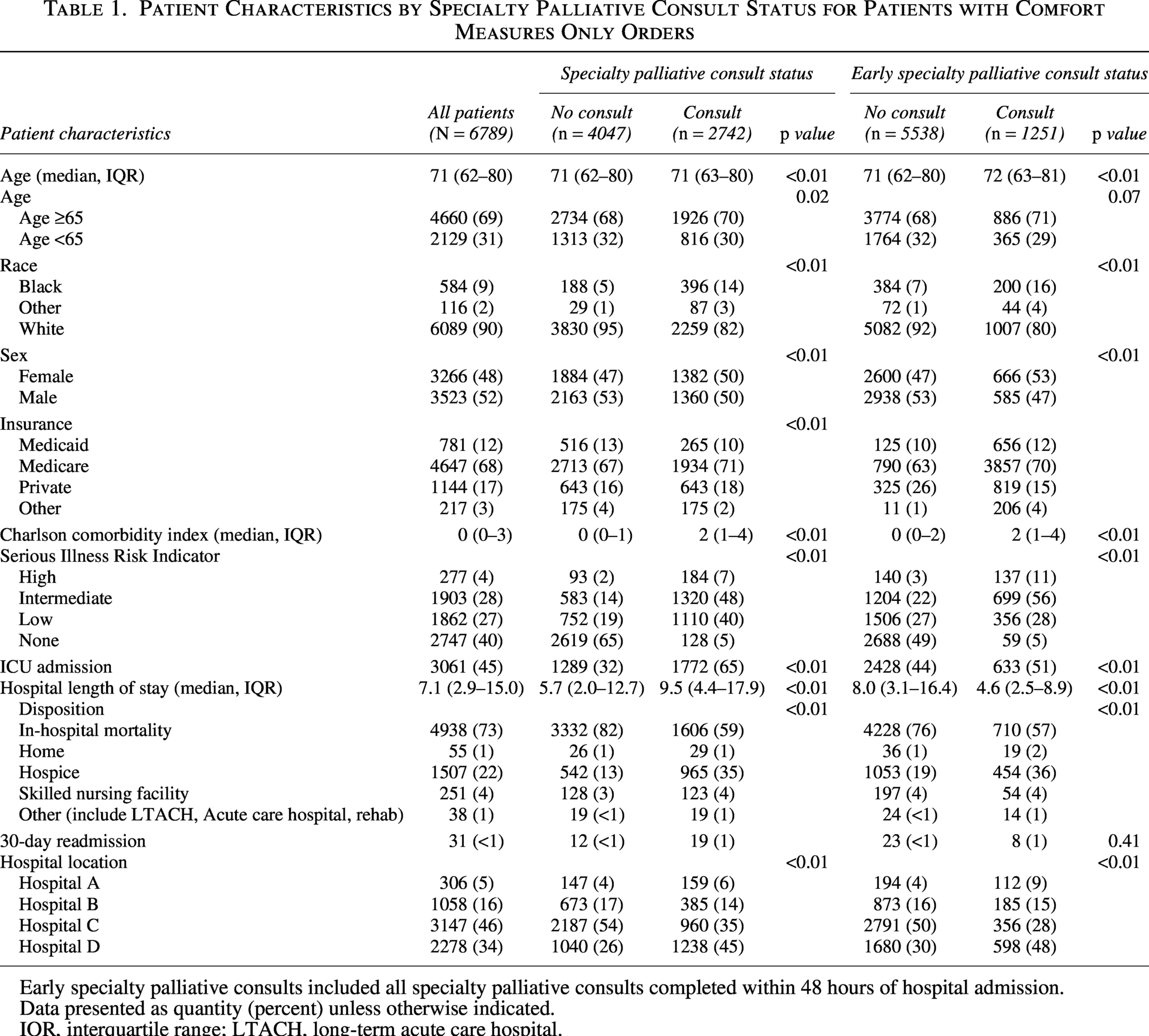
Early specialty palliative consults included all specialty palliative consults completed within 48 hours of hospital admission.
Data presented as quantity (percent) unless otherwise indicated.
IQR, interquartile range; LTACH, long-term acute care hospital.
SPC for patients with CMO orders
SPC were placed for 40% of patients with CMO orders (n = 2742). SPC involvement in the care of patients with CMO orders varied from 31% at Hospital C to 54% at Hospital D. For patients with an SPC, 46% of these consults occurred within 48 hours from hospital admission. For patients with an SPC, the SPC occurred a median of 2.4 days (IQR 0.6–6.6) prior to the CMO order, with 88% of SPC placed before the CMO order and only 12% of SPC placed following the CMO order. The median time from CMO order to hospital discharge was slightly longer for patients with versus without SPC (0.5 days vs. 0.0 days) (Supplementary Table S1).
In the unadjusted analyses of patients with CMO orders, patients with versus without SPC were more likely to be Black (14% vs. 5%, p < 0.0001), female (50% vs. 48%, p = 0.002), admitted to an ICU (65% vs. 32%, p < 0.0001), and discharged with hospice care (35% vs. 13%, p < 0.0001). They were less likely to die during inpatient hospital admission (59% vs. 82%, p < 0.0001). While patients with versus without SPC had an overall higher median length of hospital stay (9.5 vs. 5.7 days, p < 0.0001), if these consults were completed within 48 hours of hospital admission, they were associated with lower hospital length of stay (4.6 vs. 8.0 days, p < 0.0001) (Table 1).
In the adjusted analyses of patients with CMO orders, SPC placed anytime during hospital admission were associated with lower in-hospital mortality (aOR 0.4, 95% CI 0.3–0.6, p < 0.0001) and higher discharge with hospice (aOR 2.4, 95% CI 1.8–3.2, p < 0.0001) (Fig. 1). Early SPC were similarly associated with lower in-hospital mortality and higher discharge with hospice. In the secondary analysis of only CMO patients with hospital length of stay greater than 48 hours, we also found that SPC placed early or anytime during hospital admission were associated with lower in-hospital mortality and higher discharge with hospice (Supplementary Fig. S1). For patients with both SPC and documented GOCC (n = 2286), similar findings of lower in-hospital mortality (aOR 0.3, 95% CI 0.2–0.4), p < 0.0001) and higher discharge with hospice (aOR 4.1, 95% CI 2.7–6.3, p < 0.0001) were observed.
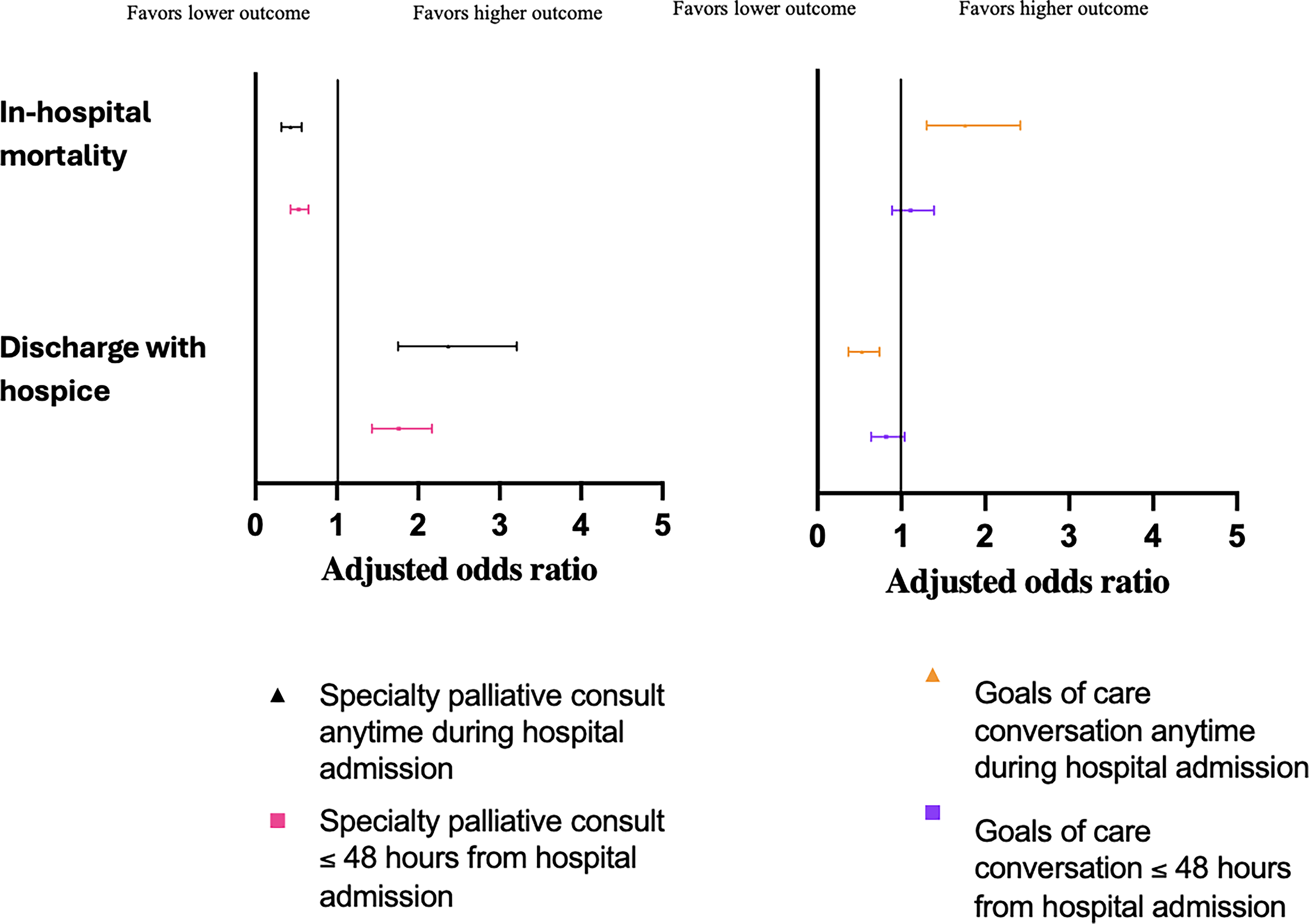
Adjusted odds ratio of (1) in-hospital mortality and (2) discharge with hospice for patients with comfort measures only orders.
In addition, in the adjusted analyses of patients with CMO orders, early SPC within 48 hours of hospital admission were associated with decreased hospital length of stay (adjusted log-linear coefficient (β) −0.4, 95% CI −0.5 to −0.3, p < 0.0001). In contrast, SPC anytime during hospital admission were associated with a higher hospital length of stay (β 0.4, 95% CI 0.2–0.5, p < 0.0001). SPC early or anytime during admission were associated with a shorter time from hospital admission to placement of a CMO order and a longer time from CMO order to hospital discharge (Fig. 2).
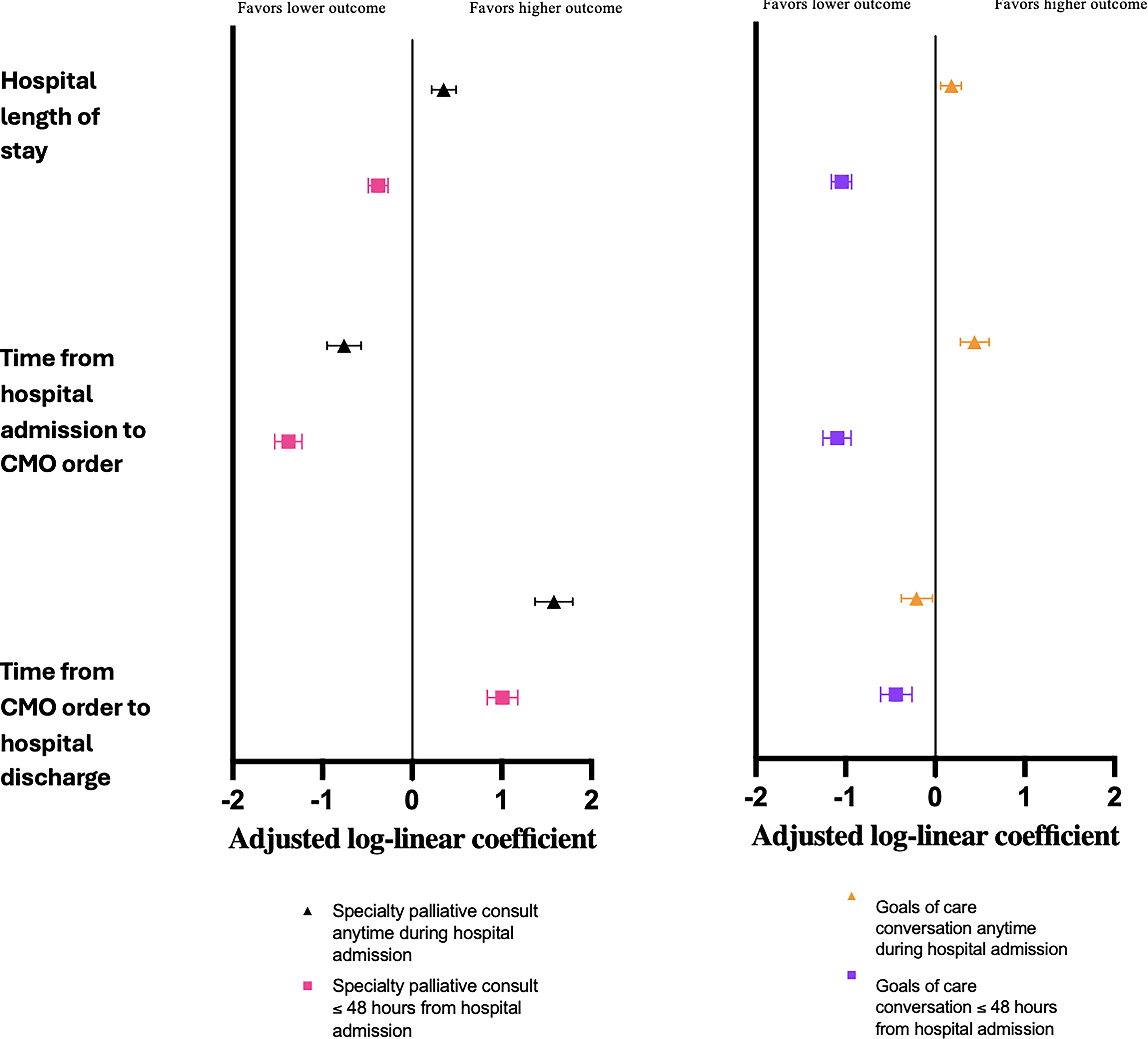
Association of specialty palliative consults or documented goals of care conversations on (1) hospital length of stay, (2) time from hospital admission to CMO order, and (3) time from CMO order to hospital discharge for patients with CMO orders.
Documented GOCC for patients with CMO orders
GOCC were documented for 46% of patients with CMO orders (n = 3142). Thirty-seven percent of patients with these notes had them documented within 48 hours of hospital admission. GOCC documentation varied across hospitals, ranging from 34% at Hospital B to 54% at Hospital D.
In the unadjusted analyses of patients with CMO orders, patients with versus without documented GOCC were more likely to be Black (14% vs. 3%, p < 0.0001) and admitted to an ICU (74% vs. 20%, p < 0.0001). They were also less likely to die during hospital admission (65% vs. 79%, p < 0.0001) and more likely to discharge with hospice care (29% vs. 16%, p < 0.0001). While patients with documented GOCC had an overall higher median length of hospital stay (9.2 vs. 5.6 days, p < 0.0001), if these notes were documented within 48 hours of hospital admission, they were associated with a lower hospital length of stay (3.8 vs. 8.2 days, p < 0.0001) (Table 2).
Patient Characteristics by Goals of Care Documentation Status for Patients with Comfort Measures Only Orders
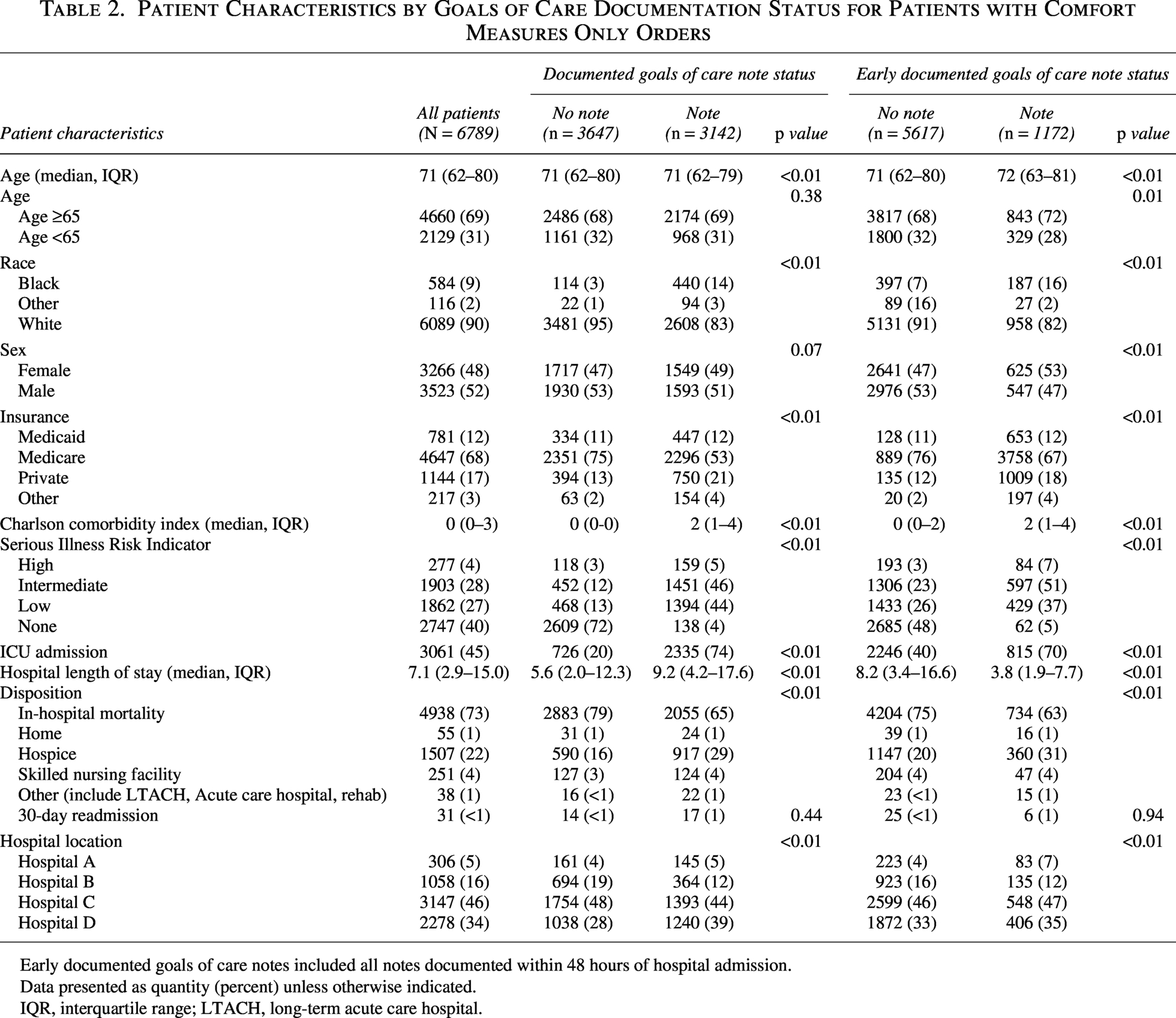
Early documented goals of care notes included all notes documented within 48 hours of hospital admission.
Data presented as quantity (percent) unless otherwise indicated.
IQR, interquartile range; LTACH, long-term acute care hospital.
In the adjusted analyses of patients with CMO orders, documented GOCC anytime during hospital admission were associated with higher in-hospital mortality (aOR 1.8, 95% CI 1.3–2.4, p = 0.0004) and lower discharge with hospice (aOR 0.5, 95% CI 0.4–0.7, p = 0.0003) (Fig. 1). In the secondary analysis of only CMO patients with hospital length of stay greater than 48 hours, we similarly found documented GOCC anytime during hospital admission were associated with higher in-hospital mortality and lower discharge with hospice (e-Fig. 2). In contrast, early documented GOCC were not associated with a difference in in-hospital mortality nor discharge with hospice.
In addition, in the adjusted analyses of patients with CMO orders, early documented GOCC within 48 hours of hospital admission were associated with decreased hospital length of stay (β −1.0, 95% CI −1.2 to −0.9, p < 0.0001). In contrast, documented GOCC anytime during hospital admission were associated with a higher hospital length of stay (β 0.2, 95% CI 0.1–0.3, p = 0.003). Early documented GOCC during admission were associated with a shorter time from admission to CMO order. In contrast, documented GOCC anytime during hospital admission were associated with a longer time from admission to CMO order. Documented GOCC early or anytime during hospital admission were associated with a shorter time from CMO order to discharge (Fig. 2).
Discussion
In this cross-sectional study of patients with CMO orders across four hospitals, we found that most patients died in-hospital, with only a quarter of these patients discharged for EOL care outside of an acute care hospital inpatient admission. Surprisingly, only 22% of patients with CMO orders received hospice care, a much lower percentage than the almost 50% of US Medicare decedents who received hospice care at the time of death. 11 In our adjusted analyses, SPC were associated with lower in-hospital mortality and higher discharge with hospice while in contrast, documented GOCC were associated with higher in-hospital mortality and lower discharge with hospice. Both early SPC and early documented GOCC were associated with decreased hospital length of stay.
While previous studies identified that both SPC and documented GOCC were associated with higher hospice enrollment for hospitalized patients, the relationship between these interventions and the unique subset of patients who had CMO orders was unclear.6,7 For other past studies that have assessed outcomes for patients with CMO orders, while they, similarly to our study, found that most patients died in hospital or were discharged with hospice, these studies did not assess whether patients with CMO orders received SPC or documented GOCC or whether these interventions were associated with patient discharge disposition.3,12,13 Our study is the first to assess how SPC and documented GOCC are associated with patient outcomes among hospitalized patients with CMO orders.
Many people prefer to receive EOL care outside of an acute care hospital inpatient admission (e.g., at their home). While these preferences may change once patients begin the dying process, some patients with CMO orders prefer to pursue inpatient hospital discharge in order to receive EOL care provided by hospice experts, even if risks may exist of them dying during the transition. In these situations, respecting patient autonomy can be an ethical approach when patients or their surrogates understand these risks. Our findings suggest that SPC, rather than documented GOCC alone, may increase the likelihood that hospitalized patients with CMO orders with preferences for EOL care outside of an acute care hospital inpatient admission can have these preferences honored. 4 Specialty palliative physicians are certified in both hospice and palliative care and have expert knowledge and experience with hospice care outside of an acute care hospital inpatient admission.14,15 This knowledge and experience may have led specialty palliative clinicians to more frequently offer patients and surrogates the option of hospice care and to describe hospice in a manner that influenced patients and surrogates to be more likely to choose this option. 16 Another possibility is that primary teams were more likely to consult specialty palliative clinicians for patients with longer life expectancies following CMO order placement to help with arranging hospice care. Because patients with longer life expectancies following CMO order placement had additional time and opportunity to enroll with hospice care, these patients may have been more likely to receive hospice care.
While we found involvement of SPC was associated with a shorter time from hospital admission to a CMO order being placed, we also found that these consults were also associated with a 0.5 day longer time from CMO order placement to hospital discharge. A possible reason for this is that SPC were more frequently associated with hospice discharge, and it takes time to enroll with hospice. While enrollment with hospice care can often occur within hours to days, for some patients, enrollment may take longer. 17 Longer time to hospice enrollment may occur when patients and/or surrogates decide to talk with multiple hospice agencies before picking one agency to enroll with. It may also occur when a patient’s family needs additional time to prepare their home for the patient, such as setting up a hospital bed and receiving EOL medications at their home. 18 It is less likely that the longer time from CMO order placement to hospital discharge for patients with SPC was related to late engagement of SPC, as 88% of patients with a CMO order had an SPC prior to CMO order placement, with these consults occurring on average 2.4 days prior to the CMO order placement. In contrast to SPC, documented GOCC anytime during hospital admission were associated with a longer time from admission to CMO order and shorter time from CMO order to discharge. One reason for this finding may be that documented GOCC were commonly used for CMO patients just prior to death rather than early in a patient’s hospital course to identify and align patient preferences for care with treatment options, as has been identified in other studies.19–21
Limitations
While this study assessed four unique hospitals with different rates of SPC and documented GOCC, all hospitals were located within one health system in the northeast United States, which may reduce the generalizability of our findings to other hospital systems. We did not assess the reason for differences in SPC and documented GOCC rates across hospitals, which is an important area for future research. It is possible clinicians had GOCC for patients that they did not document in a GOCC template note. We did not assess the content discussed during SPC and documented in GOCC notes, which may affect patient outcomes. 22 We did not assess patient preferences for location of death nor perceptions about stability for transfer for this patient population, many of whom were critically ill in ICU settings, which may affect EOL outcomes and should be assessed in future research.
Conclusion
For patients with CMO orders, SPC, rather than documented GOCC, were associated with lower in-hospital mortality and higher receipt of hospice. Future research should explore reasons why patients receiving SPC, and not documented GOCC, were associated with higher receipt of EOL care outside of acute care hospital admissions.
Authors’ Contributions
The authors confirm contributions to the article as follows: Study conception and design: G.P. Analysis and interpretation of the results: G.P., D.D., T.M., M.H., R.A., and J.S. Writing the original draft of article: G.P. Reviewing, editing, and interpretation: G.P., D.D., T.M., M.H., R.A., and J.S. G.P. had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. All authors have read and approved the final version of the article.
Human Ethics and Consent to Participate Declarations
Approval for this study was obtained by the University of Pittsburgh Medical Center Quality Improvement Review Committee, project ID 2629.
Footnotes
Author Disclosure Statement
No disclosures or conflicts of interest to report.
Funding Information
No funding for this project.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.