
Abstract
Background:
When a child dies in a pediatric intensive care unit (PICU) from a sudden or unexpected cause such as trauma or sepsis, intense grief felt by the child’s family can cause sustained psychosocial impacts. Supporting unexpectedly bereaved families with evidence-based bereavement care is key to improving grief outcomes, and understanding their specific needs is essential to inform the delivery of bereavement care in PICUs.
Aim:
To understand what is known about (1) bereavement care needs of families who have experienced the unexpected death of a child in a PICU, and (2) approaches to address families’ needs.
Methods:
An integrative review was systematically conducted with the protocol registered a priori on the Open Science Framework. Original peer-reviewed research articles relating to relatives of children who died an unexpected death in a PICU were included from OVID Medline, PsycINFO, CINAHL, SCOPUS, and ProQuest, along with guidelines from Google© searching. Articles were critically appraised using Critical Appraisal Skill Program, Mixed Methods Appraisal Tool, and Appraisal of Guidelines, Research and Evaluation II checklists, and data were synthesized using the constant comparison method.
Results:
Twenty-nine original research articles (15 qualitative, 11 quantitative, 1 mixed method, and 2 secondary analyses) and five guidelines were included in this review. Three original articles focused on unexpected child death exclusively. From the findings of all 34 articles, four linked themes were identified: (1) connection and (2) communication with PICU clinicians, (3) awareness of the impacts of unexpected death, and (4) emotional and physical support for family members.
Conclusion:
Unexpectedly bereaved family members’ needs included close relationships with clinicians and caring support before and after their child’s death, including ongoing follow-up from the PICU. Further targeted research is needed to better understand the specific needs of unexpectedly bereaved families, gain diverse and representative evidence in this area, and develop innovative, evidence-based interventions to improve bereavement outcomes for the whole family.
Introduction
The death of any child is a catastrophic event, causing intense grief for the child’s family and community. 1 Those affected are at high risk of complex and sustained psychosocial effects of grief, often requiring professional support to navigate their lives after the child’s death.1,2 Effects can include intrapsychic crises stemming from grief that does not follow the natural order of life, where parents expect to die before their children, extending to interpersonal effects on marital, familial, and social relationships. 2 Additionally, physical effects can include increased rates of morbidity and mortality among parents and siblings. 2 When a death is sudden or unexpected, the psychosocial impacts of grief are compounded, and so the unexpected death of a child can be viewed as a uniquely challenging form of grief. 2
In middle- and high-income countries, most pediatric deaths occur in a hospital setting, and usually within a pediatric intensive care unit (PICU).3,4 The aim of PICU care is to provide comprehensive, multidisciplinary care to critically ill children, extending beyond stabilization and treatment to end-of-life care for children who do not survive and bereavement care for their families.3,5 In most cases, children who die in a PICU do so as a result of a known, life-limiting illness such as cancer or an inherited condition, often with the prior engagement of specialist palliative care services to ease the child’s suffering and provide support for their family before and after the death.6,7 In contrast, when a child dies from a sudden or unexpected cause such as trauma, burns, suicide, sepsis, drowning or choking, the death can occur as a sudden shock to the child’s family, experienced within the unfamiliar and highly medicalized PICU environment and surrounded by clinicians with whom the family may have no preexisting relationship.8–10 In this context, an unexpected death refers to a death occurring from a sudden, traumatic, or accidental cause other than a progressive illness, and generally relates to acute pathophysiology or injury. 11
Supporting grieving families with hospital-based bereavement care has been shown to improve parent-reported qualitative psychosocial outcomes, 12 such as reducing feelings of isolation, improving coping, and supporting personal growth. 12 However, existing bereavement literature has primarily focused on the experiences of families who received palliative care. 13 In-hospital provision of bereavement care across adult and pediatric intensive care and other inpatient settings, outside the scope of specialist palliative care services, has been shown to be ad hoc, often inequitable, and highly dependent on the skill and good will of clinicians involved. 14 This ad hoc approach to bereavement care in intensive care settings can leave suddenly bereaved families feeling unsupported and at increased risk of psychological, social, and physical impacts. 2 To inform the development of appropriate PICU bereavement support services, it is important to understand what is known about the experiences and bereavement care needs of families whose child’s death was sudden and unexpected. 15
Objectives
To describe what is currently known about:
Bereavement needs of families who experienced the unexpected death of a child in a PICU setting. Approaches to meet unexpectedly bereaved family members’ needs.
Design
A systematic integrative review was selected for a holistic synthesis of diverse literature, including qualitative and quantitative, medical, nursing, and allied health research.16,17 Integrative review methodology enables a comprehensive evaluation of both the scope and quality of available literature concerning a health phenomenon, and was preferred over a scoping review due to its potential for generating new insights beyond simply mapping the breadth of existing research.16,18 The review followed Whittemore and Knafl’s systematic approach, 18 expanded into a six-phase process by de Souza, 17 and is reported as per the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR). 19
Method
A search strategy was developed in consultation with a health science faculty librarian, and the review protocol was registered a priori with the Open Science Framework (DOI: https://doi.org/10.17605/OSF.IO/VF4UQ). A.J. undertook keyword searching via five electronic databases including OVID Medline, PsycINFO, CINAHL, SCOPUS, and ProQuest Central on January 21, 2025. Keywords and MeSH terms relating to relatives of children who died an unexpected death in a PICU were included, and are described in Table 1. A manual search using Google© to discover bereavement care guidelines from reputable bereavement organizations was also performed.
Search Strategy Keywords and Subject Headings
CINAHL, Cumulative Index to Nursing and Allied Health Literature; MeSH, Medical Subject Headings; PICU, pediatric intensive care unit.
Data collection
Search results were imported into Covidence© and duplicates were removed. Articles were title and abstract screened independently by A.J. and K.D. against predefined inclusion and exclusion criteria described in Table 2, followed by full-text screening of those deemed eligible in the initial screen. Ten initial full-text screenings were completed together by A.J. and K.D., with the remainder screened independently by both reviewers. Disagreements were resolved by a third reviewer, F.J.G. A data extraction template was drafted in Covidence© by A.J. and piloted by A.J. and K.D. independently, with suggested refinements from each reviewer included in the final extraction tool. Data were extracted from Covidence© into Microsoft Excel© for quality appraisal.
Inclusion and Exclusion Criteria
NICU, neonatal intensive care units.
Critical analysis
A.J. and K.D. completed independent quality appraisal of all articles using Critical Appraisal Skill Program (CASP) Checklists for qualitative and quantitative research, 20 the Mixed Methods Appraisal Tool (MMAT) for mixed method research, and the Appraisal of Guidelines, Research and Evaluation (AGREE II) tool for guidelines.21,22 Articles were not excluded based on quality. Rather, the quality and relevance of each article to unexpected death in the PICU setting informed the process of conclusion-drawing. Relevance was an informal assessment of the extent to which the article reported results relating specifically to the objectives of this review, and the degree of relevance was determined by consensus between A.J. and K.D., and was described as low, medium, or high. Levels of evidence were assessed using the Joanna Briggs Institute Levels of Evidence (JBI). 23
Data synthesis was performed using the constant comparison method described by Whittemore and Knafl for integration of findings from diverse methodologies. 18 First, data cleaning and organization of the Microsoft® Excel data table were performed by A.J. before importing into Nvivo15©. Initial coding of repeated concepts across the data set was undertaken by A.J., reviewed by K.D., A.E.B., and F.J.G. Codes were organized into descriptive themes before being condensed into analytic themes guided by the review aim. 18 A visual thematic figure was created by A.J. to synthesize the results of data display, comparison, and conclusion-drawing. 18 Descriptive statistics were used to analyze and report study demographics.
Results
Article characteristics
From 313 articles found in the initial search, 29 original research articles and five guidelines met inclusion criteria (see Fig. 1). Most original research was conducted in high-income settings including the United States of America (n = 22, 76%) and Australia (n = 4, 14%), while guidelines were primarily from the United Kingdom (n = 3, 60%). Four key primary authors (K.L.M., M.L.S., A.E.B., and J.M.Y.) contributed 69% of original research articles (n = 20). Most articles reported qualitative studies (n = 16, 55%), followed by cohort studies (n = 7, 24%) and cross-sectional surveys (n = 4,14%). Two studies (7%) reported secondary analyses; one a primary qualitative interview study, and the other using mixed methods to compare primary longitudinal survey data with a separate cross-sectional survey completed by members of the same families. Three articles (10%) reported only unexpected deaths,24–26 while the other 90% (n = 26) reported both expected and unexpected causes of death. Most studies were set exclusively in a PICU (n = 20, 69%), while the remainder (n = 9, 31%) also included deaths from other critical care settings, including neonatal intensive care units (NICU) and emergency departments (ED). Table 3 shows the characteristics of the included articles.
PRISMA-ScR flow diagram. PRISMA-ScR, Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews.
Table of Study Characteristics
*Percentage of the deaths reported that occurred in PICU.
CPCCRN, Collaborative Pediatric Critical Care Research Network; CPR, Cardiopulmonary Resuscitation; DCDD, Donation after Circulatory Determination of Death; EOL, End of life; HCP, Healthcare providers; HCS, Human Connection Scale; PPC, Paediatric Palliative Care; PTSD, Post Traumatic Stress Disorder; SIDS, sudden infant death syndrome; SUDI, Sudden Unexpected Death in Infancy; UK, United Kingdom; USA, United States of America.
All original research was assessed as JBI Level III evidence, and guidelines as Level IV evidence (JBI Level I represents the highest level of evidence and Level V the lowest). The majority of original research was assessed to be high quality (n = 16, 55%) and high relevance (n = 23, 79%). Of the guidelines, two were unable to be appraised for quality; one a resource map, 56 and the other a public information brochure from a reputable bereavement trust. 54 Of the three remaining guidelines, two were assessed to be moderate quality but highly relevant,10,53 and one was considered low relevance but high quality (see Table 4). 55
Critical Appraisal Results
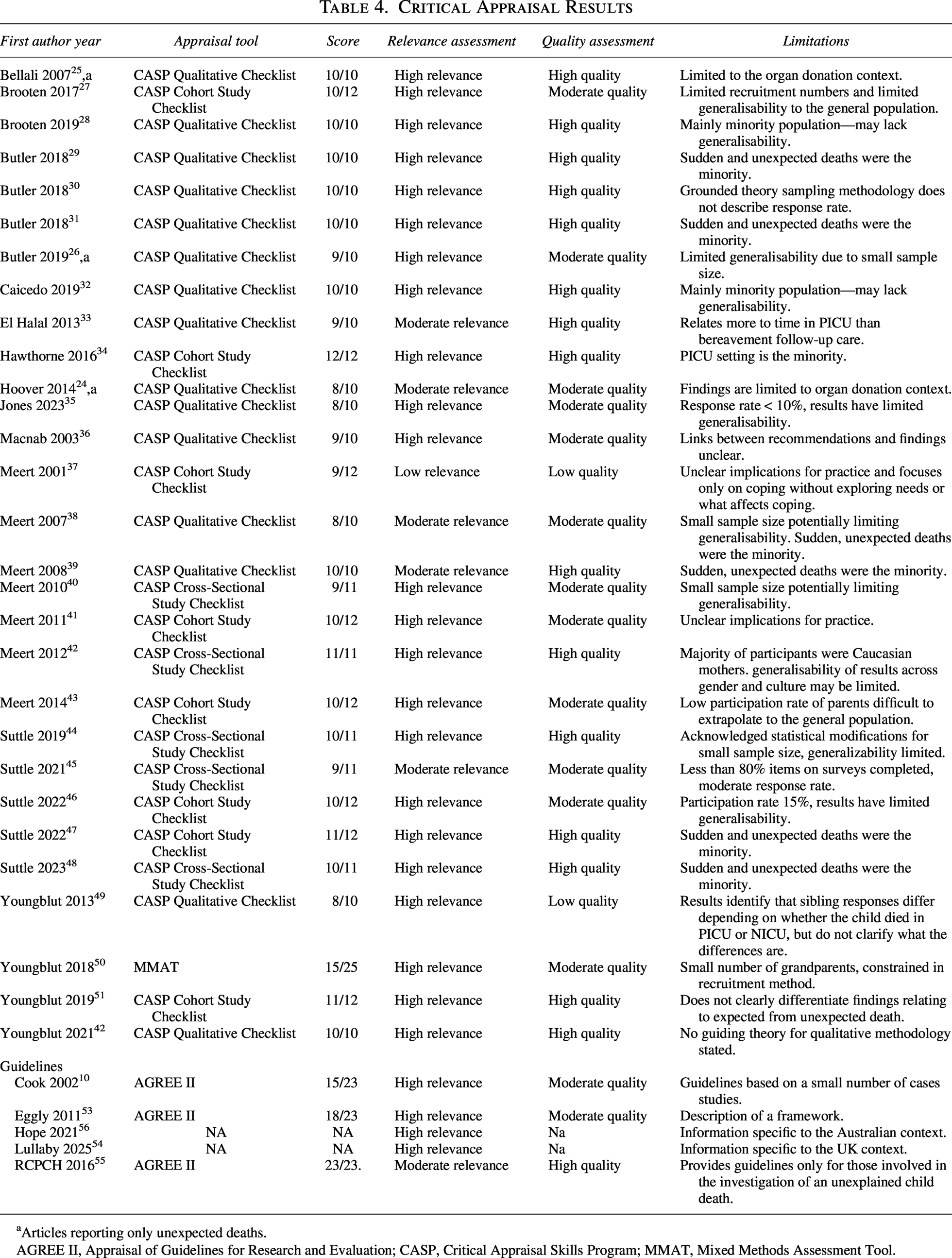
Articles reporting only unexpected deaths.
AGREE II, Appraisal of Guidelines for Research and Evaluation; CASP, Critical Appraisal Skills Program; MMAT, Mixed Methods Assessment Tool.
Findings
Included articles focused on grief and bereavement during and after a child’s death, primarily in the PICU setting. Thematic synthesis of key findings revealed four linked themes describing family bereavement needs and potential approaches to address these needs—connection, communication, awareness, and support. Within each theme were complex concepts, where needs and approaches intertwined, or were implied rather than explicitly stated. The relationship between themes and the separation of concepts into subheadings within each theme is shown in visual form in Figure 2 and condensed into recommendations for practice in Table 5.
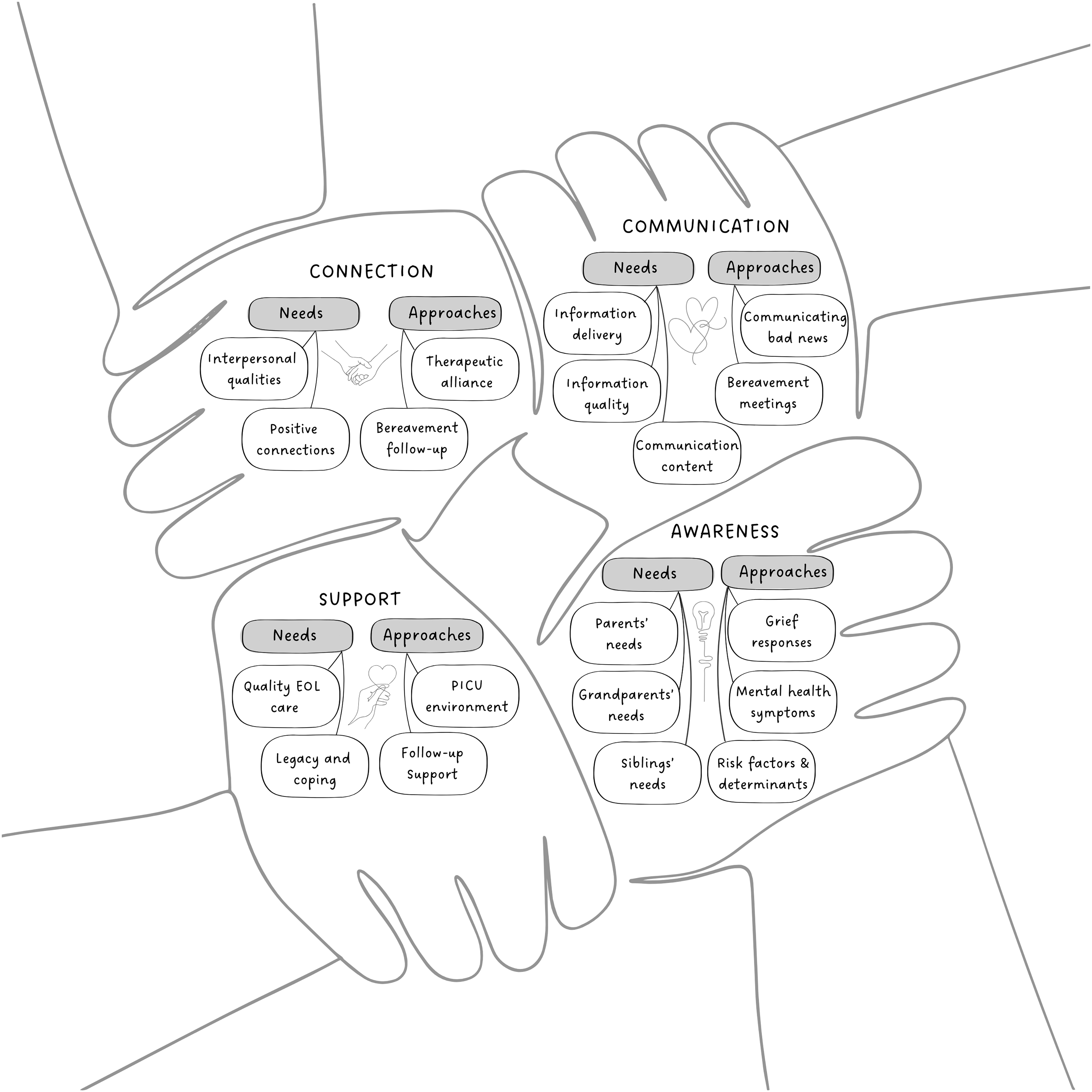
Thematic figure of review findings.
Family Bereavement Needs and Approaches to Meeting Needs—Recommendations for Practice
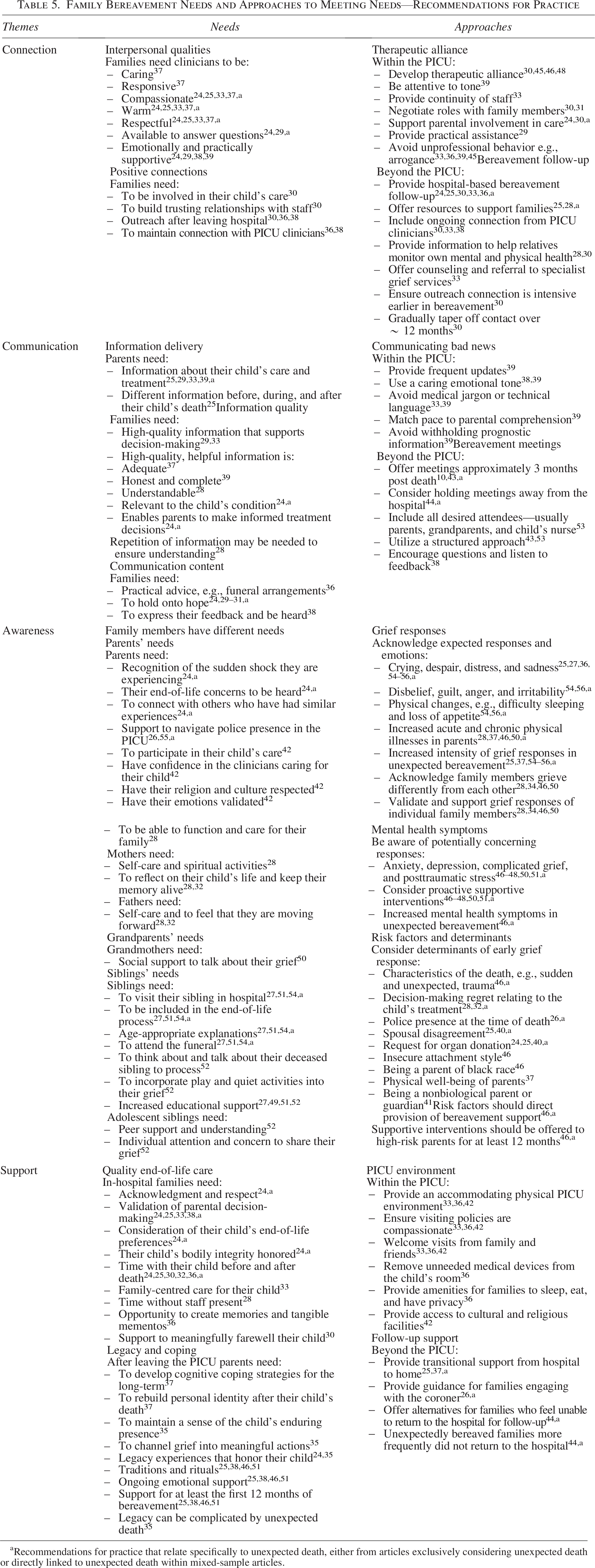
Recommendations for practice that relate specifically to unexpected death, either from articles exclusively considering unexpected death or directly linked to unexpected death within mixed-sample articles.
Connection
The first theme, connection, described interpersonal qualities bereaved family members felt supported the establishment of trusting relationships with clinicians, and ways PICU clinicians cultivated positive connections with families. Two key concepts articulated family needs—interpersonal qualities and positive connections, and two described approaches to meet these needs—therapeutic alliance and bereavement follow-up.
Interpersonal qualities
Ten articles described attributes families needed to experience within clinician interactions in the PICU to establish meaningful connections. One was a quantitative study by Meert et al., 37 who found families needed clinicians to be caring and responsive. A lack of caring emotional attitude displayed by PICU staff was associated with detrimental short-term and long-term parental bereavement outcomes, specifically elevated grief intensity scores near the time of death and two to five years afterward. 37 The remaining nine articles reported qualitative findings based on parental perspectives and experiences. Four articles reported the importance of compassion, warmth, and respect in clinician interactions with parents,24,25,33,37 while three found family members needed clinicians to be available to answer questions and provide emotional support.24,29,39 Of these, one article related specifically to unexpected death. 24 In the context of parents “negotiating a catastrophic loss,” Hoover et al. 24 reported parents felt clinician compassion, warmth, and respect eased “the emotional difficulty of their child’s impending death and organ donation” 24 (p. 110).
Positive connections
Three articles described positive connections needed by families.30,36,38 Butler et al. 30 found families needed to be involved in their child’s care to build trusting relationships with staff, and they also needed to maintain connection with known clinicians after leaving the hospital. Similarly, Meert et al. 38 found most parents wanted to meet with their PICU physician after leaving the hospital, while Macnab et al. 36 recommended ongoing connections with PICU nurses, finding more than 70% of their study participants found PICU nurses supportive during their bereavement.
Therapeutic alliance
Approaches to meeting family members’ need for connection included activities in the PICU and beyond. Four articles reported the value of developing a therapeutic alliance with family members.30,45,46,48 Therapeutic alliance describes the strength and quality of relationships between family members and clinicians. 48 Suttle et al. 48 found parents who developed stronger therapeutic alliance with PICU physicians demonstrated less severe symptoms of complicated grief during bereavement. Six articles described aspects that enhanced development of therapeutic alliance,24,29–31,33,39 including attention to tone, 39 continuity of staff, 33 role negotiation with family members,30,31 supporting parental involvement in care,24,30 and provision of practical assistance such as moving equipment to enable parents to get closer to their dying child. 29 Supporting parental involvement in care was particularly important in the context of unexpected death. 24 In Hoover et al.’s qualitative exploratory analysis, 24 parents realized “professionals cannot change the reality of the child’s death,” but could improve the provision of end-of-life care by appreciating parents’ preferences at end of life (p. 110). Additionally, four articles reported negative interactions that did not foster therapeutic alliance, including unprofessional behavior such as arrogance and dismissive or judgmental comments.33,36,39,45
Bereavement follow-up
Beyond the PICU setting, five articles recommended provision of hospital-based bereavement follow-up,24,25,30,33,36 with three identifying ongoing connection from PICU clinicians as a core component.30,33,38 Specifically for unexpectedly bereaved families, Bellali et al. 25 highlighted the importance of follow-up to reduce feelings of confusion and abandonment. During their PICU stay, parents reported “everything happened so fast” and this caused increased distress throughout the course of their bereavement afterward when they felt that they “were quickly forgotten” by clinicians involved in their child’s care (p. 221). Other aspects of follow-up included offering resources to support families,25,28 as well as counseling and referral to specialist grief services. 33 Butler et al. 30 recommended intensive connection in early bereavement, gradually tapering off over a period of ∼12 months. They found for parents, “ongoing contact demonstrated that their child meant something to the staff” (p. 95). 30 These findings showed a sense of connection with clinicians was needed by families during their time in the PICU, and should be maintained through bereavement follow-up after leaving the hospital.
Communication
The second theme, communication, focused on the two-way exchange of information between PICU clinicians and family members. Three concepts described family communication needs—information delivery, information quality, and communication content, and two described communication approaches—communicating bad news and bereavement meetings.
Information delivery
Four qualitative articles reported family perceptions of communication as key findings, each identifying parents needed information about their child’s care and treatment.25,29,33,39 In the context of organ donation, Bellali et al. 25 found parents needed different information before, during and after their child’s death, such as prognostic information beforehand and feedback about organ donation outcomes afterward. El Halal et al. 33 found the quality of communication in PICU was key to the best experience for children and families at end of life. 33 Similarly, Meert et al. 39 found that effective physician–parent communication was vital for parents to understand their child’s prognosis. Butler et al. 29 found “good” health care providers facilitated information sharing, whereas “poor” health care providers mishandled communication (p. 21). 29
Information quality
A further five articles—two quantitative and three qualitative—reported aspects that differentiated communication of quality information from poor communication.24,28,36,37,39 Quality information was characterized by adequacy, 37 honesty and completeness, 39 understandable language, 28 and relevance to the child’s condition, such that parents were able to make informed treatment decisions. 24 For unexpectedly bereaved families, information quality was very important because their hospital experience was a “blur,” during which they had difficulty “soaking in the information.” 24 (p. 108) When information was unclear, parents became confused about their child’s care options, especially when donation was discussed. 24 Despite other bereavement interventions receiving higher ratings in Macnab et al.’s survey study, 36 communication or provision of information was identified as the most critical bereavement care element. They recommended individualized communication to meet the needs of each family. 36 Importantly, Brooten 28 found the stress of being in the PICU affected retention of information, and parents needed information repeated several times to ensure understanding and prevent decision-making regret.
Communication content
Communication content was described in five original research articles.24,29,30,36 Macnab et al. 36 found parents needed practical information, such as advice about funeral arrangements and explanation of autopsy results. Four qualitative articles, one relating exclusively to unexpected death, described the way parents needed hope and how this affected communication.24,30,31 Butler et al. 30 found parents needed hope despite clear indications that their child was dying, and this need remained until “every bit of information comes in” (p. 29). 31 Mishandling communication by extinguishing hope too soon was found to be a hallmark of “poor” communication by health care providers. 29
Communication as a bidirectional process was described in two articles, with Meert et al. 38 finding families needed opportunity to provide reciprocal information by way of expressing their emotions and providing feedback to PICU staff. This feedback was seen as an important exchange of information whereby parents’ communicating their negative experiences could influence future staff communication and may prevent other families from experiencing similar problems. 38
Communicating bad news
A secondary analysis of a qualitative study focused on the way physicians communicated bad news to parents in the PICU. 39 In this study, bad news referred to sharing information about grave diagnoses, unfavorable prognosis, limitations of treatment options, or complications. 39 Although just one aspect of communication, Meert et al. 39 found communication of bad news was extremely important to most parents. Withholding prognostic information left parents feeling angry, betrayed, or distrustful. 39 Meert et al. 39 recommended physicians provide frequent updates so that bad news is understood incrementally, with a caring emotional tone and at a pace matching parents’ capacity to comprehend. These results were supported by two other qualitative articles, which recommended avoiding jargon or technical language, 33 and not using a callous, or “cold” insensitive tone (p. 4). 38
Bereavement meetings
One qualitative interview, 38 two quantitative observational studies,43,44 and two guidelines,10,53 focused specifically on bereavement meetings as an approach to meeting parents’ communication needs after their child’s death. Meert et al. 38 found provision of information was the most important feature of bereavement meetings and helped parents to make sense of what had happened to their child. In a separate study, Meert et al. 43 found that a structured approach to bereavement meeting arrangements was helpful for 92% of parents who participated. This concept was supported by a guideline that proposed a structured framework to guide bereavement meetings. 53 Most parents desired a meeting approximately three months after their child’s death,10,43 and they wanted their spouse or partner, parents, and child’s nurse to be present. 43 Suttle et al. 44 found parents of children who died of sudden and unexpected causes were statistically significantly less likely (p = 0.047) to attend bereavement meetings due to traumatic associations with the hospital setting, and recommended more research to develop targeted interventions to better support these families.
Awareness
The broadest theme described awareness, which related to aspects of grief literacy, or the ability to understand and respond to grief, 57 and how grief awareness affected clinicians’ ability to suitably support bereaved family members. Family members had varying bereavement needs, and to meet these needs, it was important that clinicians were aware of expected or “normal” grief responses as well as responses that might raise concern. Concepts within this theme focused on specific needs of family members including those of parents, grandparents, and siblings, as well as three aspects of awareness that were key to meeting family needs, including awareness of grief responses, mental health symptoms, and risk factors and determinants.
Parents’ needs
Parental experiences were specifically considered in seven research articles24,26,28,32,34,42,55 and one guideline. 29 Of these, three articles related exclusively to unexpected death.24,25,29 Hoover et al. 24 found parental experiences were affected by the sudden and unexpected nature of their child’s death. Parents needed clinicians to recognize the sense of shock that made their child’s death very difficult to cope with and to be responsive to their concerns at end of life. 24 Parents also needed to connect with others who had similar experiences. 24 Butler et al. 26 found parents needed support to navigate police presence in the PICU as part of a routine investigation into their child’s unexpected death, and these findings were consistent with the Royal College of Pathologists Guidelines.26,55
Including both expected and unexpected deaths, Meert et al. 42 validated a comprehensive Bereaved Parent Needs Assessment instrument, finding that parental bereavement needs included participating in their child’s care, having confidence in the professionals caring for their child, having their culture and religion respected, and having their emotions validated. Brooten et al. 28 found parents also needed to take care of themselves to be able to function, retain their employment, and care for their family.
Three quantitative articles separated the needs of mothers from fathers, exploring coping strategies at various time points after the death of their child.28,32,34 Brooten et al. 28 found mothers needed self-care most, followed by talking about and remembering their child. 28 Caicedo et al.’s 32 findings were similar but ranked religious activities as more important for mothers than self-care and remembrance. 32 Hawthorne et al. 34 found that engaging in spiritual activities was significantly associated with increased personal growth in mothers, but not fathers. 34 Fathers ranked self-care as their highest priority for coping, followed by the need to feel like they were moving forward after the death.28,32
Grandparents’ needs
One article reported findings about grandparent bereavement needs. 50 Youngblut et al. 50 compared the physical and mental health of grandmothers after the death of a child in an intensive care unit, mainly in the PICU but also NICU. They found that grandmothers showed grief close to that of mothers, similar levels of blame, anger, panic, and disorganization, but fewer acute illnesses and depression. 50 They reported grandmothers needed to talk through their grief, and relied on social supports such as family and friends for this support. 50
Siblings’ needs
Bereavement needs of siblings were examined in five research articles,27,49,51,52 and one guideline. 54 Youngblut et al. 51 found that children who did not see their sibling in the PICU or NICU around the time of death showed increased anxiety, and those who did not attend the funeral had higher depression scores at four and six months. Brooten et al. 58 found adolescent siblings felt shock and disbelief when they were not present at the hospital but heard their sibling had died. These findings, along with the Lullaby Trust guidelines, 54 suggested children needed to see their sibling in hospital, be included in the end-of-life process, receive age-appropriate explanations, and attend the funeral to understand and cope with the death.27,51,54
Brooten et al. 27 and Youngblut et al.49,52 surveyed and interviewed primary school-age and adolescent children, finding they needed to talk to their parents, family, friends, and even the deceased sibling, as well as to incorporate play and quiet activities into their grief. These studies did not separate sibling needs according to type of death; however, Youngblut et al.’s 52 study included 55% acute or violent deaths. Within this sample of primarily unexpectedly bereaved siblings, 13% wished they had saved or helped their sibling, such as “stopping the sibling from crossing the street into an oncoming car.” 52 (p. 230). Some siblings preferred to avoid their grief by focusing on other things, 49 while others wished to remember, 49 and some relied on prayer and faith. 27 School-age and adolescent siblings experienced changes in friendships, 49 activities, and school grades, indicating a need for increased educational support.27,49,51,52 Brooten et al. 27 found adolescents needed to talk about their grief but struggled to open up in the presence of their parents, suggesting adolescent siblings benefited from individualized attention and concern to share their grief.
Grief responses
Approaches to meeting the grief needs of different family members revolved around awareness and differentiating “normal” responses to grief from potentially concerning responses. Various expected grief responses were described in seven original research articles,25,27,28,34,36,37,46,50 and three guidelines.54–56 These included crying, despair, distress, and sadness,25,27,36,54–56 disbelief, guilt, anger and irritability, as well as physical changes such as difficulty sleeping and loss of appetite.54,56 Of these, two original research articles25,37 and three guidelines,54–56 specifically mentioned unexpected death, characterizing expected grief responses as “increased” 25 (p. 220) or “especially devastating” 54 (p. 31) for these families. The increased intensity of expected grief responses was attributed to the “profound effects of shock and trauma” that accompany unexpected death. 54 (p. 31) Three articles described increased rates of acute and chronic physical illnesses in bereaved parents,28,37,46,50 while three guidelines described grief as an experience unique to each person.54–56 The importance of acknowledging family members who grieved differently from each other and validating and supporting individual grief responses was implied but not explicitly reported in three research articles.28,34,46,50
Mental health symptoms
Potential pathological effects of grief and the mental health risks to bereaved parents and other family members were described in two guidelines,10,54 and five original research articles.46–48,50,51 These specifically considered mental health outcomes, finding increased risk of anxiety, depression, complicated grief, and posttraumatic stress among bereaved parents and siblings.46–48,50,51 Risk of developing these mental health symptoms was increased for those who grieved sudden and unexpected deaths. 46 Awareness of the risk factors for complex grief responses emerged as an important approach to enable the provision of proactive supportive interventions.10,46,54
Risk factors and determinants
Risk factors and determinants for complex grief responses were identified in nine research articles.24–26,28,32,37,40,41,46 Suttle et al. 46 found that sudden, unexpected death was a risk factor for increased mental health symptomology, along with black race and insecure attachment style, including attachment anxiety and avoidance of emotional closeness. Other determinants of complex early grief responses included decision-making regret relating to the child’s treatment,28,32 police presence in the PICU, 26 physical well-being of parents, 37 spousal disagreement,25,40 request for organ donation,24,25,40 and being a nonbiological parent or guardian. 41 Suttle et al. 46 concluded awareness of risk factors should direct the provision of bereavement support, and supportive interventions should be offered to parents at high risk for at least the first year after their child’s death.
Support
The final theme, support, encompassed the needs of families in and beyond their stay in a PICU to promote adaptive grieving. Before and during the dying period, support centered around care of their child, while after the death, support focused on the family and their grief journey. Two concepts articulated family needs—quality end-of-life care, and legacy and coping, and two described PICU environment factors and follow-up support.
Quality end-of-life care
High-quality end-of-life care for the child as an essential support need was reported in seven articles.24,25,30,32,33,36,38,42 Hoover et al. 24 recommended PICU clinicians respect parental perceptions of their child’s preferences at end of life, acknowledge parents as protectors, and honor their child’s bodily integrity. Specifically in the context of unexpected death, Bellali et al. 25 highlighted the importance of validating parental decision-making, a concept that was supported by three other studies.24,25,33,38 El Halal 33 reported that support centralized in the family was the key to quality of care for both expected and unexpected deaths. Having adequate or sufficient time was an important aspect of family-centered care, 42 including time to spend with their child at end of life,24,25,30,32,36 and time without staff present. 28 Memory-making was also identified as a valued component of end-of-life care, with Macnab et al. 36 finding creation of tangible mementoes such as hand or footprints highly appreciated. Finally, Butler et al. 30 found families also needed support to meaningfully farewell their child.
Legacy and coping
Seven research articles outlined aspects of support required to meet the ongoing needs of parental grief.24,25,35,37,38,46,51 Meert et al. 37 found parents needed to develop intrinsic strategies, such as cognitive coping, or the ability to preserve a positive self-concept and sense of self-worth, and to rebuild personal identity after the loss. Coping mechanisms were related to activities such as honoring their child’s legacy,24,35 maintaining a sense of their child’s continuing presence, 35 and channeling grief into meaningful actions. 35 Legacy refers to an enduring representation of the child’s life. 35 Jones et al. 35 found that unexpected death complicated perceptions of legacy because parents did not have time for meaningful experiences with their child prior to the death. Legacy-building activities after death, including family rituals, artistic expressions of their child’s life, and altruistic pursuits were described as important by parents who experienced an unexpected bereavement. 35 To develop coping strategies, build their child’s legacy, and achieve positive bereavement outcomes, parents needed ongoing emotional support for at least the first 12 months of bereavement.25,38,46,51
PICU environment
Three research articles reported the importance of a supportive PICU environment.33,36,42 Meert et al. 42 found parents who perceived greater bereavement need fulfillment experienced less complicated grief symptoms, but their needs were challenging to meet in the PICU setting due to physical and operational constraints. Approaches to meet bereavement needs included compassionate policies that welcomed visits from relatives and the child’s friends at end of life,33,36,42 and creation of accommodating PICU physical spaces.33,46 Examples included removal of excessive technology and medical devices from the child’s room, 36 amenities for parents to sleep near their child, 42 provision of private spaces for family at the end of life, 36 close proximity to food and refreshments, and access to cultural or religious facilities such as a chapel. 42 Environmental factors were not specifically linked to the experiences of unexpectedly bereaved families in these articles. However, Meert et al. 42 did note a non-statistically significant inverse relationship between death from trauma and the fulfillment of bereavement needs in the PICU, suggesting that the needs of parents who experience unexpected bereavement may not be adequately met in the current PICU environment.
Follow-up support
Approaches to supporting families after leaving the PICU were recommended in five original research articles.25,26,30,37,44 Butler et al. 30 concluded families benefited from close, supportive relationships with clinicians to facilitate the transition from hospital to home and a post-PICU reality.25,37 Important facets of support needed at this time included guidance for engaging with the coroner, 26 and support to return to the hospital for bereavement follow-up meetings. 44 Suttle et al. 44 recommended provision of alternative options for families who felt unable to return to the hospital due to traumatic memories of their time there, which was more frequently seen among unexpectedly bereaved parents.
Discussion
The review findings, synthesized from 29 research articles and five guidelines from five different countries, are the first to focus on unexpected child death in the PICU setting. Our findings show family bereavement needs centered around themes of connection, communication, awareness, and emotional and practical support, with specific insights within each theme drawing out the unique experiences of unexpectedly bereaved families, which to date have been underexplored. These insights differ from previous systematic reviews examining child death investigation, 59 PICU end-of-life care from a health care provider perspective, 60 and parental perspectives of pediatric palliative care.61,62 The rigorous methodology we employed sets our review apart from earlier narrative synthesis of PICU bereavement, 63 and our meticulous search strategy differed from previous systematic scoping and integrative reviews of parental bereavement experiences, which reported fewer articles and did not focus on unexpected death.62,64
Importantly, in this review, while we chose to include articles that reported both unexpected and expected deaths where data for unexpected deaths could be clearly differentiated, only three original research articles reported unexpected deaths exclusively.24–26 This highlights an important research gap, suggesting what is currently known about childhood bereavement reflects primarily the experiences of families of children who died an expected death. Not only are unexpectedly bereaved families under-represented, but the little that has been reported reflects the experiences of those who volunteer to participate in research, and may not be fully representative. Unexpected bereavement is experientially different from an anticipated grief journey, but we do not currently know enough to fully characterize the unique nature of grief for these families, and how sudden shock affects their capacity to engage with bereavement support. Further work is needed to separate the needs of unexpectedly bereaved families from other bereaved groups and to identify approaches suitable for their specific experiences. To this end, thoughtful and innovative strategies must be developed to engage effectively with bereaved families to conduct representative research that includes diverse experiences and contrary viewpoints.
Our findings demonstrate the importance of strong relationships between families and PICU clinicians that continue after the child’s death. Interconnectedness with clinical staff has been previously described in palliative care literature as a means to help grieving parents endure feelings of alienation and solitude, 65 with empathetic human encounters representing a universal need. 66 Relatives of children with known life-limiting illnesses often have greater time to develop such connections, 65 benefiting from relationships with clinicians formed both before and after the child’s death. For unexpectedly bereaved families, therapeutic alliance must be forged rapidly and under pressure in the PICU. 31 The intensity of such relationships may explain why many parents desired them to continue long after their child’s death. 67 Importantly, our findings showed that suddenly bereaved families wanted ongoing connection and support from PICU clinicians, but unlike palliative care services with well-established programs of family follow-up, there was often no one there to fill that need.
Conversely, the trauma of unexpected death may result in some parents not wanting continued relationships with clinicians from the PICU. Our findings showed that while unexpectedly bereaved families benefited from ongoing support after leaving the PICU, including guidance with traumatic administrative tasks and support to access post bereavement meetings, parents of children who died unexpectedly were less likely to attend these meetings. This suggests they experience higher levels of hospital-related trauma than other bereaved parents. 44 Correlation between Post Traumatic Stress Disorder (PTSD) and the level of threat to a child’s life has been reported in wider PICU literature 68 ; however, our results highlight the additional risk of mental health effects for unexpectedly bereaved parents and siblings. 39 To date, few interventions to reduce trauma for these families have been tested, and their perspective is potentially unrepresented in the literature, as such families may avoid participation in research due to fears of retraumatization. 69 Outpatient follow-up by PICU teams is not yet considered a routine aspect of bereavement care, 14 but could provide clinicians with an opportunity to identify symptoms of posttraumatic stress in relatives and initiate supportive interventions. 68 For families who do not desire ongoing connection with PICU clinicians, respecting personal choice is important, 12 and alternative options for bereavement support should be considered. 12 Given heightened risk of mental ill health among unexpectedly bereaved relatives remained for up to 13 months, 46 our findings identified the first year following the death as a key opportunity for these supportive grief interventions, such as PICU bereavement follow-up.
The importance of grief literacy, 57 specifically awareness of the varying potential impacts of unexpected death on family members, was also highlighted in this review. Pediatric deaths are an increasingly rare event, particularly in resource-rich nations, meaning bereaved parents’ networks of family and friends are often unprepared to anticipate and respond to their needs. 63 Awareness of the traumatic features of unexpected child death and their potential impact on families is consequently limited. Furthermore, the specific needs of different family members, including fathers, siblings, and grandparents, are underreported. Most articles focused on mothers or parents as a dyad, with only three focusing on siblings,27,51,52 one on grandmothers, 50 and none considering fathers alone. Yet, our findings highlight increased rates of mental health symptomology reported in bereaved parents and siblings, with unexpectedly bereaved family members demonstrating higher levels of complicated grief compared to relatives of children who died from expected causes.46–48,50,51 To improve grief outcomes for these families, more targeted research is warranted to better understand the diverse impacts of unexpected bereavement on different family members, to increase societal awareness, and to develop interventions to support all family members in their bereavement. 36
Strengths and limitations
Strengths of this review include the systematic approach following an a priori registered protocol and inclusion of diverse literature, with most included articles appraised to be of high quality. Limitations included the small number of articles exclusively reporting unexpected deaths and the potential for selection bias within the included studies, which may reflect only the experiences of bereaved people who volunteer to participate in research. Of the articles included, less than 30% were published in the last five years, indicating a paucity of current research in this area. In addition, we acknowledge that five articles by A.E.B. were included. Potential conflict of interest was managed by A.E.B. not being involved in the process of screening or selection of articles for review, contributing only to the synthesis and discussion of findings. Finally, only studies published in English were included, potentially limiting the diversity of this review. Only two non-English publications were found in our initial search, suggesting this is a wider limitation of the evidence available.
Conclusion
This review highlighted complex differences between bereavement for families of children who died from unexpected causes in the PICU setting and families who experienced expected child death supported by specialist palliative care services. The intensity and traumatic nature of unexpected bereavement and time constraints within the PICU affected the way families experienced care, emphasizing a need for additional support and bereavement care extending beyond the PICU. Family bereavement needs are focused on themes of connection, communication, awareness, and support, demonstrating the value of high-quality end-of-life care as well as ongoing follow-up from PICU clinicians to provide bereavement care that transitions from intensive early contact and hospital-to-home support to a gradual disengagement. Additional targeted research is needed to increase understanding of the needs of unexpectedly bereaved relatives beyond the perspective of those willing to participate in research, to separate the specific needs of families following unexpected child death in the PICU setting from the palliative care context, and to inform development of innovative, evidence-based interventions that could enhance bereavement outcomes, not only for parents, but also grandparents, siblings and the whole family.
Authors’ Contributions
A.J.: Conceptualization, data curation, formal analysis, funding acquisition, investigation, methodology, project administration, resources, visualization, and writing—original draft. K.D.: Methodology, supervision, data curation, formal analysis, validation, visualization, and writing—review and editing. A.E.B.: Methodology, supervision, validation, visualization, and writing—review and editing. S.E.: Supervision, validation, and writing—review and editing. K.S.G.: Supervision, validation, and writing—review and editing. F.J.G.: Methodology, supervision, validation, visualization, and writing—review and editing.
Ethical Considerations
Ethical approval was not required as this is a literature review. However, ethical principles were followed, including transparent documentation of the protocol with a priori registration to the Open Science Framework (DOI: https://doi.org/10.17605/OSF.IO/VF4UQ), systematic documentation of the search strategy, inclusion and exclusion criteria, and data extraction methods.
Supplemental Material
sj-tif-1-plm-10.1177_10966218261460500 — Supplemental material for Bereavement Care after the Unexpected Death of a Child in a Pediatric Intensive Care Unit: A Systematic Integrative Review
Supplemental material, sj-tif-1-plm-10.1177_10966218261460500 for Bereavement Care after the Unexpected Death of a Child in a Pediatric Intensive Care Unit: A Systematic Integrative Review by Arielle Jolly, Kylie Davies, Ashleigh E. Butler, Simon Erickson, Kristen S. Gibbons, and Fenella J. Gill
Supplemental Material
sj-docx-2-plm-10.1177_10966218261460500 — Supplemental material for Bereavement Care after the Unexpected Death of a Child in a Pediatric Intensive Care Unit: A Systematic Integrative Review
Supplemental material, sj-docx-2-plm-10.1177_10966218261460500 for Bereavement Care after the Unexpected Death of a Child in a Pediatric Intensive Care Unit: A Systematic Integrative Review by Arielle Jolly, Kylie Davies, Ashleigh E. Butler, Simon Erickson, Kristen S. Gibbons, and Fenella J. Gill
Supplemental Material
sj-docx-3-plm-10.1177_10966218261460500 — Supplemental material for Bereavement Care after the Unexpected Death of a Child in a Pediatric Intensive Care Unit: A Systematic Integrative Review
Supplemental material, sj-docx-3-plm-10.1177_10966218261460500 for Bereavement Care after the Unexpected Death of a Child in a Pediatric Intensive Care Unit: A Systematic Integrative Review by Arielle Jolly, Kylie Davies, Ashleigh E. Butler, Simon Erickson, Kristen S. Gibbons, and Fenella J. Gill
Footnotes
Acknowledgments
The authors would like to acknowledge the contribution of V. Varis, Health Sciences Faculty Librarian at Curtin University, for consultation on the search strategy utilized in this review.
Author Disclosure Statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this article.
Funding Information
This study was supported financially by grant funding from the Perth Children’s Hospital Foundation (PCHF10159), Stan Perron Charitable Foundation (00058ProgPart) and the Future’s Health and Research Innovation Fund (MRAS22-23/4). A.J.’s work on this study was supported via a Nursing Research Fellowship from the Child and Adolescent Health Service and the Telethon Trust. F.J.G.’s research program is supported by the Stan Perron Charitable Foundation. K.S.G. is supported by a National Health and Medical Research Council Emerging Leader Fellowship. A.E.B. is an Australian Research Council Discovery Early Career Researcher Award recipient for research into “Supporting the inclusion of siblings when a family is in crisis” (DE230101123). The funders had no part in the study design, conduct, or data analysis and did not have any authority over these activities.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.