
Abstract
Opioid management for symptom relief in serious illness is a core aspect of palliative care (PC) practice, with additional complexities to consider when prescribing in the outpatient setting. Safe and timely access to necessary opioids for patients depends on clinicians writing accurate prescriptions, navigating health care insurance(s), planning for potential medication shortages, and close collaboration with outpatient pharmacies. Access should be supported by, and balanced with, appropriate risk-mitigation strategies, including regular clinical assessments, thoughtful medication selection to minimize adverse effects, and ongoing education for patients and clinicians. This article—written by an interprofessional team of PC-trained physicians, nurse practitioners, pharmacists, clinical practice nurses, and social workers—summarizes ten practical tips for navigating outpatient opioid prescribing.
Introduction
Opioid prescribing is a core clinical practice in palliative care (PC) and essential to the effective management of distressing symptoms in patients with serious illness. Among cancer patients, approximately 55% experience pain and up to 70% report dyspnea.1,2 Pain, refractory dyspnea, and cough are also common in other serious illnesses such as advanced cardiopulmonary diseases such as chronic obstructive pulmonary disease and heart failure.3,4 Grounded in principles established by the World Health Organization analgesic ladder and reinforced by guidelines from the National Comprehensive Cancer Network, the American Society of Clinical Oncology, the American Thoracic Society, and the American Heart Association, the judicious use of opioids remains central to improving comfort, function, and quality of life for patients with serious illness.1–6
While opioids are recommended as part of symptom relief, few guidelines address the practical aspects of navigating the complexity of opioid prescribing for patients with serious illness or those nearing the end of life. This leaves many uncertain about best practices and reluctant to prescribe or titrate opioids, even when clinically indicated. 7 These barriers contribute to delays in symptom management, patient and clinician frustration, and fragmentation of care. 8
Prescribing opioids in the outpatient setting has become increasingly complex due to the interplay of regulatory oversight, supply chain limitations, and insurance restrictions. Although intended to curb opioid prescribing in response to the opioid epidemic, broad policy limits have constrained appropriate access for patients with serious illness. Since 2019, the Drug Enforcement Agency (DEA) has reduced its annual opioid production quotas, and lawsuits against opioid manufacturers and pharmacies have limited opioid manufacturing and dispensing practices.9,10 Prior authorizations (PAs) and coverage exclusions are additional barriers imposed by insurance companies.11,12 Real-time medication shortage information is often not readily available to clinicians to guide decision making. Laws limiting opioid quantity prescribed are variable based on jurisdiction across the United States and are often driven by guidelines for acute or chronic nonmalignant pain rather than pain for patients with serious illness. 13
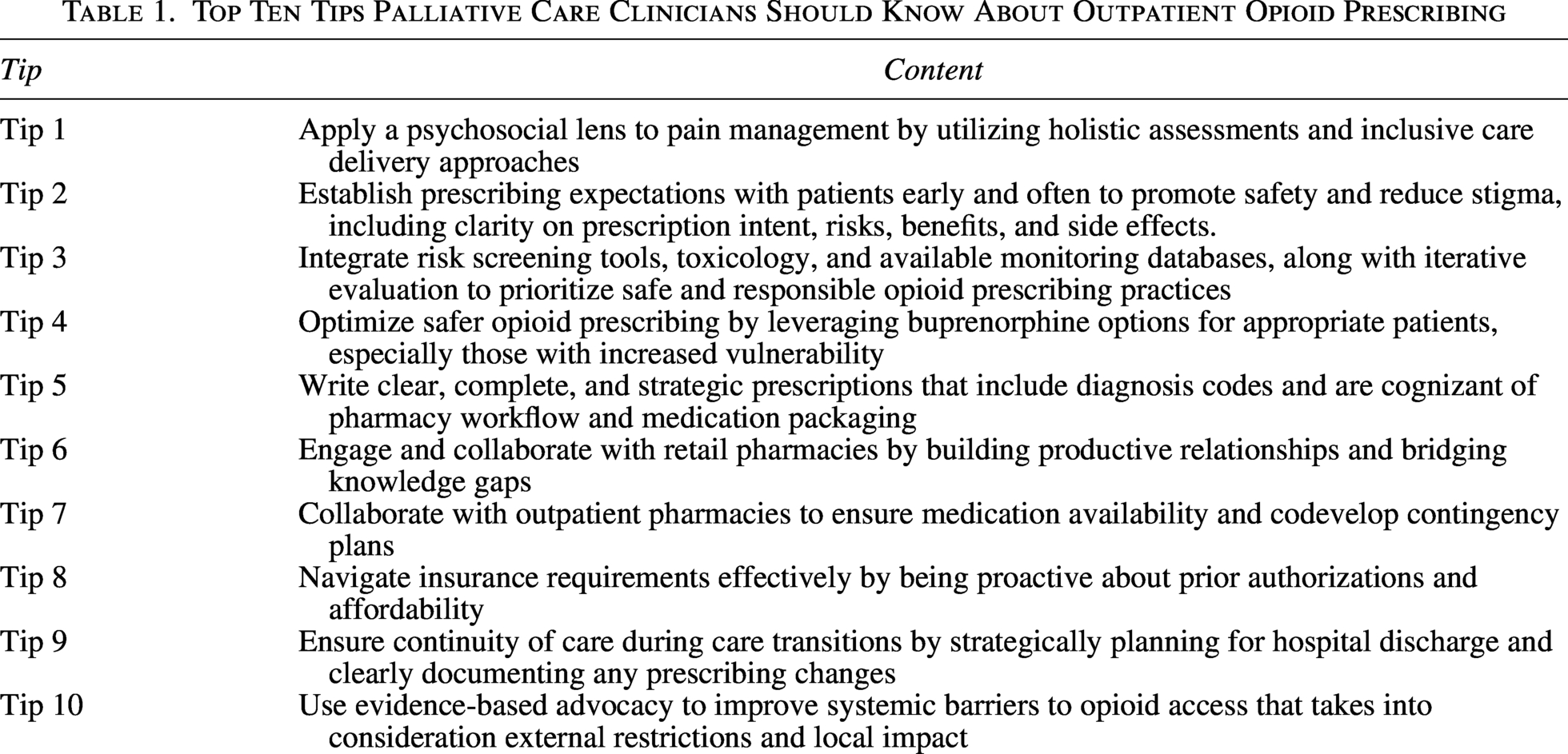
While navigating the regulatory, insurance, and supply constraints, outpatient opioid prescribing for serious illness is best supported by structured risk-mitigation practices and reliable communication between prescribers, patients, and pharmacists to balance opioid safety with access. Interprofessional clinicians ensure safe opioid prescribing for patients in the community through adherence to regular assessments, toxicology screening, use of prescription monitoring programs, and patient education about roles and expectations for opioid-based symptom management.7,8,14–16 Building on these principles, this article summarizes ten key tips to support safe and effective outpatient opioid prescribing for patients with serious illness (Table 1).
Top Ten Tips Palliative Care Clinicians Should Know About Outpatient Opioid Prescribing
Tip 1: Apply a Psychosocial Lens to Pain Management by Utilizing Holistic Assessments and Inclusive Care Delivery Approaches
Pain is almost always multifactorial. Dame Cicely Saunders defined the concept of “total pain” as the suffering that encompasses all of a person’s physical, psychological, social, spiritual, and practical struggles. 17 Interprofessional PC teams should use a biopsychosocial model to guide comprehensive pain management.18,19 Thorough symptom assessment should incorporate spiritual, mental health, trauma history, medical, social determinants of health, cultural, economic, legal, and functional evaluations of patients and their families. Clinical care plans, which may involve opioid prescribing, require thoroughly evaluating all these domains and may ultimately include nonopioid and nonpharmacologic therapies to address total pain.
In addition to these domains, it is important to remember cultural aspects impacting pain experience. Pain has historically been undertreated in marginalized and minoritized populations. 20 To address health disparities and correct these oversights, clinicians should intentionally reduce bias and use culturally responsive practices in pain management. 21
Tip 2: Establish Prescribing Expectations with Patients Early and Often to Promote Safety and Reduce Stigma, Including Clarity on Prescription Intent, Risks, Benefits, and Side Effects
Setting clear expectations at opioid initiation and revisiting them throughout treatment helps build trust, reduce anxiety, and supports adherence and safety. 22 Table 2 outlines standard counseling recommended for all patients when starting or adjusting opioid therapy. This should include clear discussions around treatment goals, side effects, and approaches to regimen adjustment. 23 Common opioid side effects include constipation, sedation, nausea, dependence, tolerance, respiratory depression, and, in rare cases, overdose. Long-term risks in anticipated chronic pain syndromes include hypogonadism, falls, fractures, infections, and the potential for developing an opioid use disorder (OUD). 24 While there is limited evidence of benefit for opioid treatment agreements, it can be helpful to provide practice and patient guidelines on adherence to safe opioid therapy. 25
Universal Counseling and Risk Mitigation Strategies for Safe Opioid Prescribing
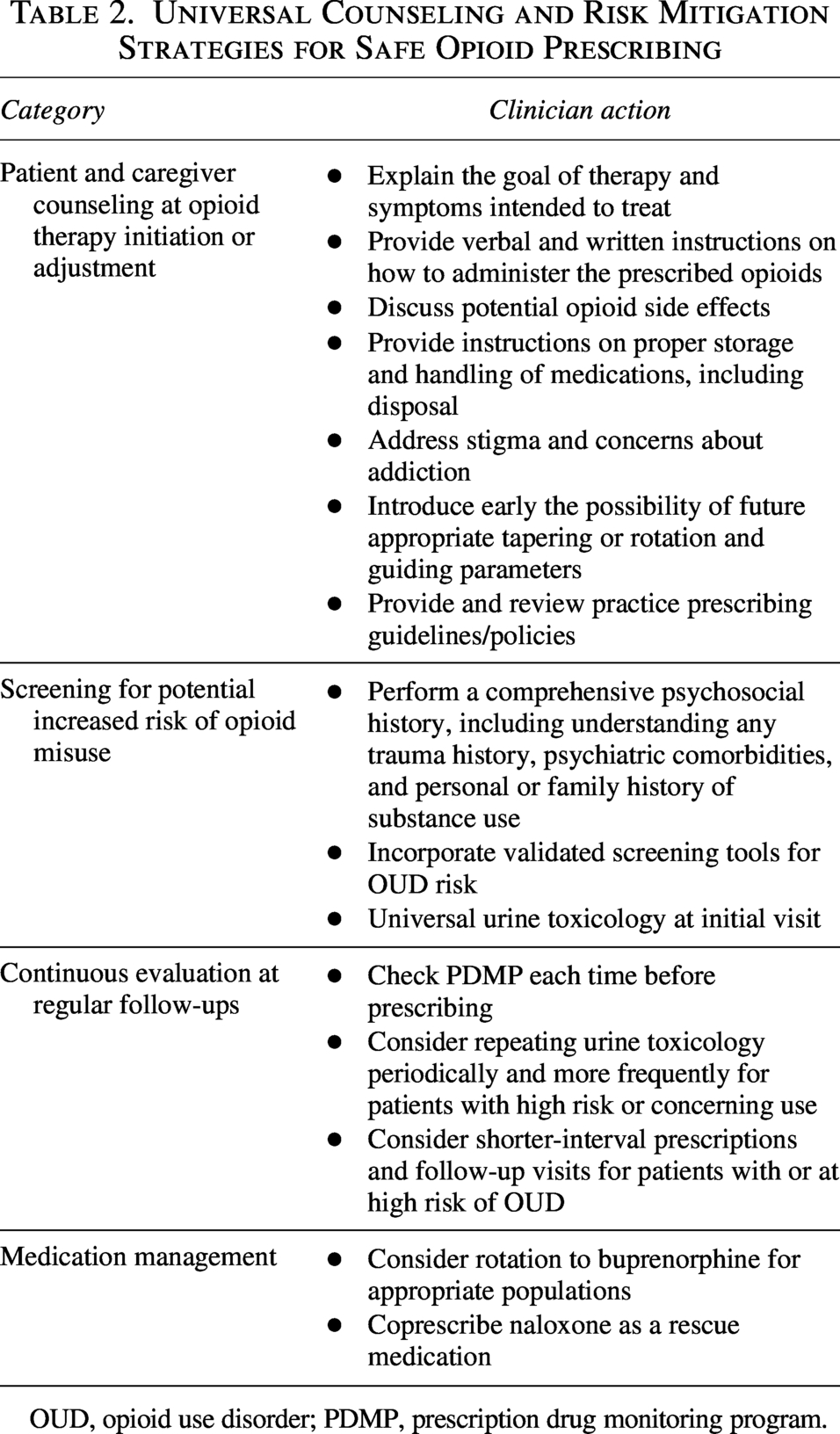
OUD, opioid use disorder; PDMP, prescription drug monitoring program.
To prepare for safer use of opioids at home, patients and caregivers should be instructed on safe storage and handling of medications, especially in households with children or individuals at risk of misuse, and on proper disposal methods (e.g., local take-back programs or DEA-approved disposal sites). We advocate for universal coprescribing of naloxone as a rescue medication to further enhance safety and provide reassurance to both patients and caregivers.
Patients may express concerns about either under- or overutilization of opioids for pain, and clinicians should clarify the appropriate role of opioids with emphasis on safe management and efforts to ensure access to necessary medications. To reduce stigma, we recommend framing education in a way that makes patients feel understood. For example, patients may express worry about “addiction,” now referred to as substance use disorder (SUD) or OUD. We suggest proactively clarifying the distinction between physical dependence (a normal physiological effect of sustained opioid use) and addiction (characterized by specific criteria describing patterns of ongoing opioid use despite harm).
At opioid initiation, clinicians should prepare patients for the possibility of tapering. Framing tapering as an expected component of care is particularly important for patients with cancer pain who are undergoing curative treatment or for those with longer prognoses who may transition to chronic pain management. Opioid tapering should generally proceed gradually and in a patient-centered manner to reduce the risks of abrupt cessation, opioid withdrawal, and severe psychological distress. Strategies include gentle dose reduction, eventual discontinuation, or rotation to safer long-term options (e.g., buprenorphine) when clinically appropriate. Balance empathy with boundaries: if opioids are not effective, prioritize patient safety and taper or discontinue, while maintaining person-centered supportive care.
Tip 3: Integrate Risk Screening Tools, Toxicology, and Available Monitoring Databases, Along with Iterative Evaluation to Prioritize Safe and Responsible Opioid Prescribing Practices
Safer opioid prescribing requires multimodal risk assessment. Clinicians should assess for risk of opioid-related harm—including development of OUD—using chart review and prescription drug monitoring programs (PDMPs). This helps identify prior patterns of substance use, opioid misuse, or prescribing complexity (e.g., multiple prescribers or short-duration prescriptions). Substance use screening tools (e.g., Opioid Risk Tool [ORT], ORT-OUD, Screener and Opioid Assessment for Patients with Pain-Revised) can help identify risk factors for misuse, including personal or family history of SUD and psychiatric comorbidities. 14 However, they are only validated in chronic nonmalignant pain populations, rather than PC settings. It is important to recognize that they serve as screening aids, not definitive predictors, when informing clinical judgment.
Patients with increased risk may still receive opioids and may require closer follow-up and shorter prescription intervals for monitoring (e.g., visits every 2–4 weeks and 7- or 14-day supplies). 1 Although there is no consensus on the optimal frequency of urine toxicology screening in serious illness populations, baseline and periodic (e.g., at least annual) urine toxicology testing are supported, with increased frequency when indicated. 26 Unexpected results should prompt a nonjudgmental and nonpunitive discussion, reassessment of risk, and potential changes to management. 22 Longitudinal outpatient prescribing requires regular continuous evaluation using these tools and universal counseling strategies as outlined in Table 2.1,14
Tip 4: Optimize Safer Opioid Prescribing by Leveraging Buprenorphine Options for Appropriate Patients, Especially Those with Increased Vulnerability
Compared with conventional full agonist opioids, buprenorphine provides effective analgesia with a lower risk of opioid-related adverse effects, such as respiratory depression, constipation, physical dependence, and tolerance. 27 As a partial agonist of the mu (µ)-opioid receptor, agonist of opioid receptor-like 1, and antagonist of the delta (δ)- and kappa (κ)-opioid receptors, it offers a safer profile than full opioid agonists.27,28 Expert consensus identifies several populations who may benefit most, including patients with comorbid OUD or misuse, other SUDs, advanced age, frailty, heightened sensitivity to full agonist opioids, or a prolonged prognosis requiring long-term opioid therapy.7,28,29 In the United States, buprenorphine can be prescribed for pain or OUD without additional DEA training requirements. 30
Access to buprenorphine can be limited by payer and dispensing barriers that often require proactive documentation and coordination. Insurance coverage, including PA, may require supporting materials such as detailed clinical history, treatment goals, and a rationale for buprenorphine over other opioids. Coverage variability and pharmacy unfamiliarity with certain indications, such as coprescribing full agonist opioids during low-dose initiation, can further impede access. Clinicians may need to change between buprenorphine formulations based on insurance coverage, which include transdermal patches and buccal films for lower-dose products and buprenorphine sublingual tablets and naloxone-buprenorphine sublingual tablets or films for higher-dose products.28,31
Tip 5: Write Clear, Complete, and Strategic Prescriptions That Include Diagnosis Codes and Are Cognizant of Pharmacy Workflow and Medication Packaging
Prescribers must understand federal and state regulations. Although federal law permits paper prescriptions for Schedule II medications, many states mandate the use of Electronic Prescribing for Controlled Substances. In some emergencies, oral prescriptions can be provided for a limited quantity. Schedule II medications cannot be refilled, and the dispensing limit is a 30-day supply. Clinicians may prescribe Schedule III–V medications in writing or verbally in some states, with a maximum of five refills (a 6-month supply) and a quantity limit for a 90-day supply on each prescription (although insurance may impose different limitations). Insurers may restrict refills before day 28 of a 30-day prescription, even if the dose is adjusted. Given these restrictions, prescribers should order a 1- to 2-week supply of opioids at initiation or dose change to prevent delays in access if dose titration is expected. PDMP data will reveal critical information, including whether a partial fill was provided.22,32
Including relevant International Classification of Diseases (ICD-10) codes and serious illness indicators improves prescription clarity, reduces verification delays, and may bypass inappropriate quantity limitations.13,32 Knowledge of commonly available formulations supports effective management and helps pharmacies fill prescriptions accurately within regulatory and supply constraints (see Table 3). For example, most pharmacies will not split a box of transdermal patches, that is, they will not dispense less than a 15-day supply (five patches) of fentanyl or a 28-day supply (four patches) of buprenorphine. 33 Ensure prescriptions are double-checked for accuracy in the intended formulation, dose, route, duration, and quantity.
How to Effectively Navigate Pharmacies and Insurances
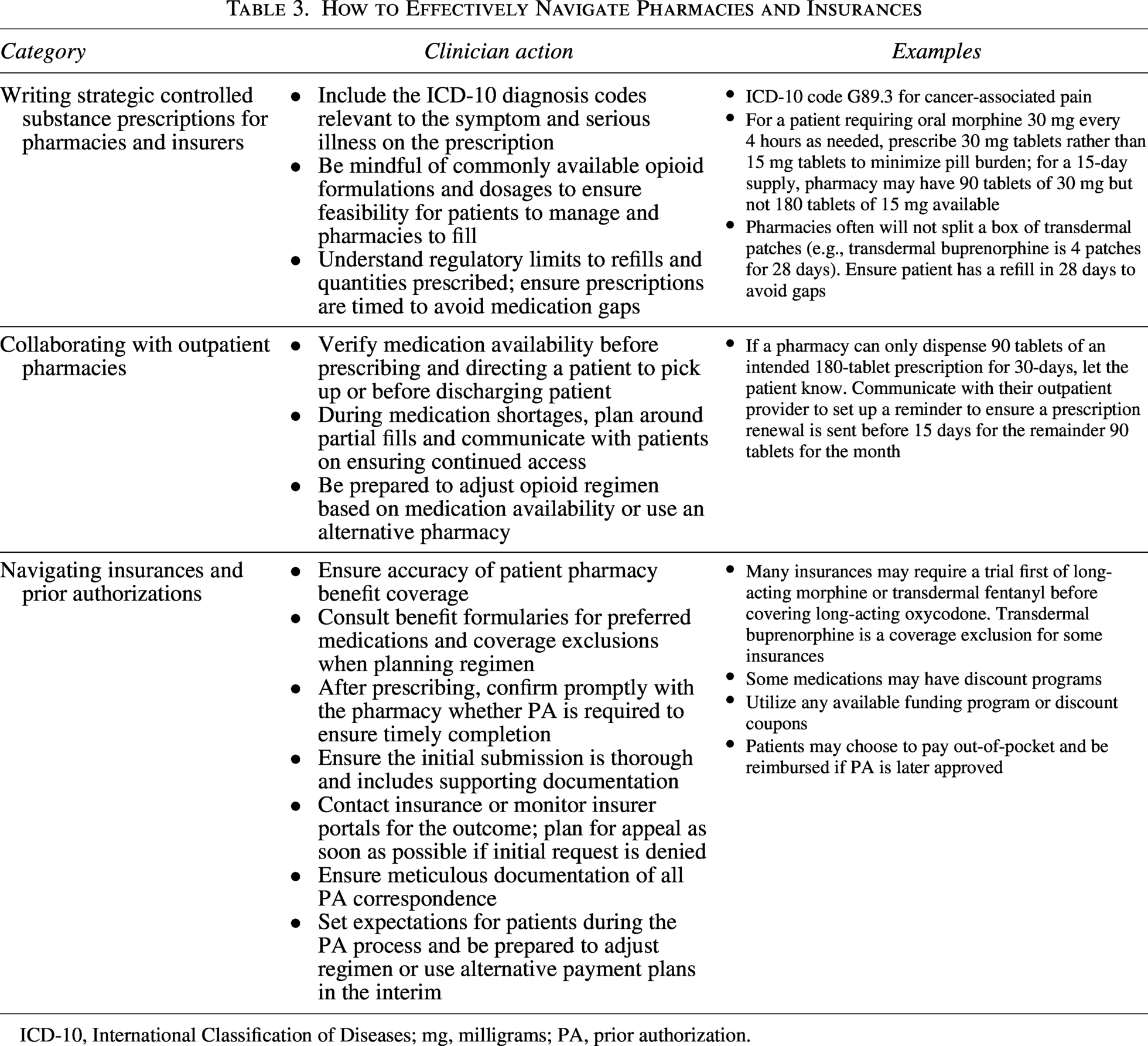
ICD-10, International Classification of Diseases; mg, milligrams; PA, prior authorization.
Tip 6: Engage and Collaborate with Retail Pharmacies by Building Productive Relationships and Bridging Knowledge Gaps
Community pharmacists play a critical role in safe and timely opioid access. Regulatory scrutiny, limited access to clinical information, insurer restrictions, and corporate policies can create dispensing delays. 15 Under the DEA Controlled Substance Act, pharmacists share responsibility with prescribers to ensure opioids are prescribed for legitimate medical indications. 34 Perceived stigma and varied familiarity with opioid prescribing in PC can further barriers in opioid access.35,36 Engaging pharmacists as clinical partners in medical decision making, rather than solely as medication dispensers, supports an informed prescription verification process. This also aligns pharmacist and prescriber collaboration within the “assess” and “plan” domains outlined by the Joint Commission of Pharmacy Practitioners’ “Pharmacists’ Patient Care Process” (PPCP) framework. 37
Strategic relationship-building between prescribers and community pharmacists fosters trust and helps bridge knowledge gaps through various strategies. 38 Proactive, bidirectional communication (e.g., brief follow-up calls, use of electronic health record [EHR] messaging portals) helps clarify prescription intent, especially in complex cases (e.g., high-dose opioids, buprenorphine, methadone). It allows discussion around common pharmacist concerns (e.g., high oral morphine equivalents [OMEs], early refills, and multiple prescribers). Prescribers should include relevant clinical context not otherwise readily accessible on prescriptions (e.g., ICD-10 diagnosis codes or brief notes about serious illness indicators). Shared references can serve as standards, such as OME conversion charts, resources for opioid conversions, and available expert recommendations about opioid prescribing.23,39,40 Collaboration can facilitate the development of new tools such as prescribing aids (e.g., quick reference guides or decision support tools), which may help standardize prescribing practices and help prescribers anticipate pharmacist prescription verification needs.
Tip 7: Collaborate with Outpatient Pharmacies to Ensure Medication Availability and Codevelop Contingency Plans
Addressing the dynamic nature of opioid supplies requires a shared approach that builds on strategic relationships between prescribers and pharmacists. This aligns with the “implement” domain of the PPCP, which focuses on operationalizing the pharmacotherapy plan and ensuring patients can access medications in real time. 37
Establish standardized workflows as follows, both at the point of prescribing and in the pharmacy, to improve efficiency in this process. Prescribers and pharmacists should mutually share preferred contact information for reliable partners to allow real-time communication. Before directing a patient to pick up a prescription, clinical staff should call ahead to verify pharmacy stock to prevent treatment delays and unnecessary travel, especially for patients with mobility or transportation barriers.41,42 Create workflows for which team members (e.g., nurse coordinator or team pharmacist) would call a community pharmacy after prescription is sent and what a checklist of necessary information to provide to the pharmacist may entail (e.g., exact medication and quantity needed, by when, patient insurance).
When opioid medications are unavailable, clinicians should promptly identify therapeutic alternatives (e.g., opioid rotation, switching formulation). An alternate dispensing arrangement may be required during shortages, in which pharmacies may dispense only a partial fill. Patients should be clearly counseled on the quantity dispensed, expected timeline for the remainder of the prescription, and what alternatives exist if delays occur (e.g., opioid rotation, using an alternative pharmacy). 43 Clinic teams can use reminder calls, electronic messages, or EHR-based tracking to coordinate timely opioid prescriptions as additional prescriptions may be needed to complete the fill (see Table 3).
Tip 8: Navigate Insurance Requirements Effectively by Being Proactive About PAs and Affordability
Medication PAs are increasingly burdensome, and requirements vary widely across insurers.44–47 Clinicians should work with available clinical nurse or pharmacist colleagues to strategically navigate each step in PA completion (see Table 3). Electronic Prior Authorization (ePA) tools may assist during clinical encounters by flagging formulary options, but they are not always current or comprehensive. 46
When PA is needed, submissions should include the diagnosis, treatment history, prior therapeutic failures, and a clear justification for medical necessity.44,46 PA templates can be useful, but customization to the patient’s specific clinical context can reduce the likelihood of denial. ePA portals may allow supporting documentation to be uploaded. Consistent follow-up is critical as a lack of response does not equate to approval. Clinicians should monitor insurer portals, identify denial rationale, and prepare appeals to reduce delays. Thorough documentation of all PA correspondence is essential, including submission dates, reference numbers, and appeal details for when escalation becomes necessary.
Patients should be educated about potential delays and interim solutions—including discount programs such as GoodRx® or pharmaceutical company coupons, obtaining a limited supply while awaiting PA approval, or temporary medication alternatives to support symptom control. 44 In some cases, clinicians may also consider prescribing lower-cost opioid formulations such as methadone or morphine when clinically appropriate, particularly for patients paying out of pocket for short-term supplies or those with limited or temporary insurance coverage (e.g., emergency Medicaid).
Tip 9: Ensure Continuity of Care During Care Transitions by Strategically Planning for Hospital Discharge and Clearly Documenting Any Prescribing Changes
Medication errors are common around care transitions such as hospital discharge, where medication doses may be missed or prescriptions inadequately filled. 48 The complexity of outpatient opioid prescribing can further exacerbate this problem, resulting in uncontrolled symptoms and repeat emergency department visits or readmissions. 8 Effective communication between inpatient teams (e.g., hospitalists, inpatient PC consult services) and outpatient teams (e.g., primary care providers, outpatient PC teams, skilled nursing facilities) supports consistent management. Continued education and culture change toward cross-setting collaboration helps inpatient providers who may not be as familiar with outpatient opioid-prescribing plan before discharge. 49
Strategies summarized in Table 3 can be utilized by inpatient teams to ensure patients have access to necessary opioids at the time of hospital discharge. Awareness of local opioid shortages might impact analgesic choice when planning a discharge regimen. Inpatient and outpatient clinicians should collaborate to develop feasible pain regimen adjustments, especially if facing insurance barriers, medication shortages, or a need for formulation change. Discharge prescriptions should be written to last until the next outpatient follow-up—ideally 2–4 weeks—to reduce the risk of treatment interruptions. PC clinicians should work within existing health system policies to ensure compliance with applicable laws and regulations while creating contingency plans in case of opioid shortages. For example, in select circumstances where permitted by state law, inpatient pharmacies may be asked to dispense a short-term supply (e.g., 3 days) of opioids upon hospital discharge to bridge outpatient access gaps. 50
Careful documentation in notes and discharge summaries or direct communications help relay key information for the next clinician managing the opioids who may need to plan for continued medication access. Changes made to a patient’s chronic opioid regimen should be clearly documented and should include details of the current regimen prescribed, prior medications tried, and reasons for discontinuation or adverse effects.
Tip 10: Use Evidence-Based Advocacy to Improve Systemic Barriers to Opioid Access That Takes into Consideration External Restrictions and Local Impact
Systemic factors, such as DEA policies, supply chain disruptions, and insurance limits, can hinder access even as clinicians follow best practices for safe and effective opioid prescribing. These restrictions can disproportionately affect patients in rural, underresourced, or historically marginalized communities and those with high symptom burden. 8 Recognizing these barriers and their underlying causes can empower clinicians to advocate for change, reinforcing their vital role in improving patient care.
PC clinicians can translate frontline experiences into collective advocacy for policy improvements and system-level change by tracking local barriers, documenting real-time shortages, and their adverse outcomes. For example, pharmacy stock limitations and manufacturer discontinuations can lead to abrupt changes in opioid regimens, threatening patient safety. These data and case examples provide information necessary to inform legislation that resonates with policymakers and the public. Pharmacists have also expressed support for mechanisms such as documentation of ICD-10 diagnosis codes that override restrictive insurer limits, underscoring opportunities for interprofessional advocacy.13,32 Partnering with professional societies by contributing data and supporting reforms helps safeguard appropriate access. 51 q1′ Evidence-based advocacy helps shift narratives around opioid access for patients with serious illness from restriction to balance, equity, and stewardship.
Conclusion
Patient-centered, high-quality pain and symptom management using opioids is a core PC skill. Opioid prescribing in the outpatient setting is nuanced and requires skillful maneuvering in multiple domains, including a clear understanding of the systems-based challenges surrounding opioid prescribing and close collaboration across disciplines and care settings. Strong prescriber–pharmacist partnerships enable coordinated strategies to navigate insurance and supply limitations, select appropriate opioid regimens, and provide patient counseling that supports safe and timely access to opioids for all patients living with serious illness for whom an opioid is appropriate.
Footnotes
Author Disclosure Statement
No competing financial interests exist for all other authors.
Funding Information
Lorin Fisher is supported by the National Association of Chain Drug Stores Foundation. Rebecca Rodin is supported by the National Institute on Aging (grant no.: R03 AG082996), the American Cancer Society (grant no.: CSDG-23-1151579-01-HOPS), and the Claude D. Pepper Older Americans Independence Center at Mount Sinai (P30AG028741-07).