
Abstract
Background:
Early integration of specialist palliative care (sPC) improves patient-centered outcomes, but its impact on hospital costs during terminal admissions remains insufficiently studied.
Aim:
To compare total and daily hospital costs associated with early versus late initiation of sPC during the terminal hospital admission of patients who died in hospital.
Design:
Retrospective cohort study using routinely collected administrative and clinical hospital data. Costs were analyzed using generalized linear models adjusted with inverse probability of treatment weighting. Bias-corrected mean ratios with 95% confidence interval (CI) calculated from 2,000 bootstrapped samples were presented.
Setting/Participants:
The study was conducted at a single Swiss tertiary care hospital and included adults aged ≥18 years who died during their terminal hospitalization between 2016 and 2022 and received sPC. Early sPC was defined as initiation within three days of admission. Patients with refusal of data use, external causes of death, perioperative death in otherwise healthy individuals, or incomplete cost data were excluded.
Results:
The cohort comprised 790 patients (397 early sPC; 393 late sPC). Adjusted total hospital costs were substantially lower among patients receiving early sPC (CHF, 22,999; 95% CI: 21,149–25,072) compared with late sPC (CHF, 60,691; 95% CI: 55,186–67,165). Patients receiving early sPC also had lower daily costs. The largest cost differences occurred in pharmacy, laboratory, material, and room categories, whereas staff costs were similar between groups.
Conclusions:
Early initiation of sPC during terminal hospitalizations is associated with markedly lower hospital costs without increased staff expenditures. Additional studies are needed to establish whether this association is causal. Nonetheless, these findings suggest that providing patients with the benefits of sPC earlier during terminal hospitalization may be possible without increasing overall hospital costs and may have important implications for health care resource utilization.
Keywords
Key Statements
What is already known about the topic?
Early specialist palliative care improves patient-centered outcomes, but its effect on hospital costs during end-of-life care has been unclear. Existing cost studies are narrow in scope, often disease-specific, and rely on highly processed administrative data sources such as reimbursement or insurance claims data, rather than real-world hospital cost data. Health systems need broader evidence on whether earlier specialist palliative care reduces resource use.
What this paper adds
Early specialist palliative care during terminal hospitalization is associated with substantially lower hospital costs. Savings stem mainly from reduced pharmacy use and laboratory testing.
Implications for practice, theory, or policy
Practice: Literature has already shown that specialist palliative care improves patient-centered care. Now it is also shown that early inpatient specialist palliative care is associated with substantially lower hospital costs, with no evidence of reduced staff-related costs. Policy: Policies promoting early referral to specialist palliative care may reduce high-costs at the end-of-life. Theory/Research: These findings highlight the importance of studying the timing of specialist palliative care across health systems.
Introduction
Early integration of specialist palliative care (sPC) is increasingly recognized as a cornerstone of high-quality care for patients with advanced, life-limiting disease. Systematic reviews and meta-analyses have demonstrated that early outpatient sPC—typically initiated weeks to months before the terminal phase—improves quality of life, reduces symptom burden, and is associated with a survival benefit in patients with advanced cancer.1,2 Pooled analyses further suggest a survival benefit associated with early outpatient sPC in advanced cancer, with patients randomized to palliative care showing a 25.7% lower rate of mortality compared with controls. 2 Beyond clinical outcomes, growing evidence suggests that early sPC may also optimize health care utilization by reducing unnecessary interventions and hospitalizations.3,4
Although prior studies have reported associations between palliative care involvement and lower end-of-life costs, existing economic evidence remains inconsistent, with some reviews reporting cost savings primarily through reductions in hospitalization and intensive care unit use, while others find no significant effect.5–7 In particular, few studies examine the explicit timing of sPC initiation. In routine clinical practice, however, sPC is frequently initiated only in the last weeks or days of life. 8 Therefore, evaluating the economic impact of earlier sPC initiation, even when initiated close to death, for example during terminal hospitalization, is highly relevant to real-world practice. Moreover, much of the available evidence focuses predominantly on oncologic populations or overall end-of-life trajectories rather than acute inpatient cost patterns.3,9,10 Additionally, many analyses focus on overall health care expenditures, with relatively few examining detailed hospital cost structures or the contribution of specific cost categories.11–13
Consequently, the economic implications of initiating sPC at different time points remain insufficiently understood—particularly in inpatient settings, where health care costs accumulate rapidly.6,14 In this context, terminal hospitalization represents a particularly relevant period, as a substantial proportion of health care expenditures accrue near the end of life. Analyses of end-of-life trajectories consistently identify the final weeks of hospital admission as the period of highest cost intensity, with nearly 40% of all end-of-life health care costs expended in the last month of life.15,16 Cross-national data from nine high-income countries show that hospital care constitutes the largest single cost category in this period. 17 A more comprehensive understanding of inpatient cost patterns within this period is essential for clinicians, administrators, and policymakers seeking to balance quality improvement with financial sustainability.
Switzerland provides a distinctive context for examining sPC. Mandatory basic health insurance covers all medically indicated inpatient and outpatient services, as well as medications, including sPC, thereby minimizing financial barriers to access.18,19 Residents may purchase supplemental insurance for additional amenities such as private hospital accommodation; around 20–30% of the population hold such coverage for hospital care, with a larger proportion insured for other supplementary benefits. 20 In addition, sPC ward infrastructure, such as single or family rooms, is accessible to all patients, independent of insurance status. Hospital care is financed through a combination of insurance payments and public funding, resulting in relatively low levels of patient cost-sharing. 21 In the region surrounding the Swiss capital, Bern, hospital-based sPC is integrated into a broader palliative care network that also provides 24/7 mobile support in home and long-term care settings; dedicated hospice facilities are not yet available. 22
In Switzerland, sPC can be introduced early in the disease trajectory and delivered alongside disease-directed treatments across inpatient and outpatient settings. Despite recommendations for earlier integration of sPC, referral often occurs late in the disease trajectory, frequently near the end of life.23,24 This pattern is not unique to Switzerland: Studies across multiple health systems have documented that palliative care is commonly initiated only in the final weeks of life, even when earlier access is structurally available.25,26 Hospice care, in contrast, typically refers to end-of-life care focused on comfort in the final weeks to months of life and is usually provided outside acute hospitals. Although assisted suicide is not illegal under specific conditions in Switzerland, it remains rare and is generally organized outside hospitals.27,28 Importantly, sPC is conceptually and practically distinct, focusing on symptom control, communication, and goal-concordant care.
The integration of sPC into routine inpatient workflows varies widely: There is substantial variation in referral timing (early vs. late), models of delivery (consultative vs. integrated teams), availability across care settings, and the use of standardized referral criteria. These differences influence how and when patients access sPC and underscore the need to examine not only whether sPC impacts costs, but also when during the hospitalization its initiation yields the greatest economic benefit—a question that has only recently begun to receive systematic empirical attention.6,29
The relevance of this question has increased in light of demographic changes. Populations in high-income countries are aging, and the prevalence of multimorbidity continues to rise, expanding the number of patients who could benefit from structured palliative involvement.30,31 Concurrently, hospitals face intensifying financial pressures as diagnostic technologies, therapeutic options, and staffing demands become more costly.19,32,33 In this context, health systems are increasingly encouraged to adopt value-based care approaches that emphasize the relationship between outcomes and resource use. 34 Understanding the economic consequences of early versus late sPC initiation is therefore integral to informed health policy and hospital management.
We conducted a retrospective observational cohort study at a Swiss university hospital to compare hospital costs of patients receiving early versus late sPC during their terminal hospital admission in which the patient deceased. Focusing on this period allows for a more comparable assessment across patients, as survival time is limited and disease-specific differences are attenuated. We hypothesized that early initiation would be associated with lower total and daily hospital costs, particularly in cost categories linked to costly diagnostic and therapeutic interventions.
Methods
Study design
We retrospectively analyzed administrative and clinical data from the entire last hospital admission of patients who died in the hospital between January 1, 2016, and December 31, 2022. This study was approved by the local ethics committee (BASEC-ID: 2021-00253).
Setting
Our study was conducted at a Swiss university hospital with 846 inpatient beds, treating more than 57,000 inpatients annually across 39 clinical departments.35,36 The hospital’s sPC program includes a ten-bed inpatient unit, as well as both ambulatory and in-house consultation services. Care is delivered through an interdisciplinary team offering physiotherapy, nutritional counseling, social and psychological support, and access to a full range of diagnostic and therapeutic modalities, including advanced imaging, chemotherapy, and radiotherapy. The service is designed to enable concurrent palliative and disease-directed care. 37
Sample selection
We excluded patients who did not consent to the use of their health data for research purposes and those younger than 18 years. We further excluded individuals whose deaths resulted from injury, poisoning, or other external causes—including self-harm, assault, transport-related accidents, or other categories defined by the International Classification of Diseases, Tenth Revision. Patients who died from medical or surgical complications while otherwise healthy were also excluded. In addition, we removed ambulatory patients with fewer than one overnight stay at the university hospital and those with missing cost data. These databases capture resource use at a granular level, including medications (down to individual pills), laboratory tests, therapeutic procedures, and staff services.
Definition of sPC exposure
We included only sPC consultations delivered during the index hospitalization, as our analysis was restricted to inpatient hospital data. sPC provided in outpatient or community settings before or after hospitalization was not captured in our dataset and therefore could not be considered in the analysis. Patients were classified as having received sPC if they met at least one of the following criteria: (1) admission to the inpatient sPC ward; (2) at least one formal consultation by the sPC team; or (3) documented sPC recommendations to the treating team.
Definition of early and late sPC
Patients were categorized as early sPC if the first sPC consultation occurred within three days of their terminal hospital admission and as late sPC if it occurred later. The three-day cut-off was based on existing literature38,39 and expert consensus. It reflects the typical period during which treatment goals and care intensity are determined in acute hospital settings. Earlier involvement allows the sPC team to participate in these decisions, whereas later involvement often occurs after treatment escalation has already occurred.
Cost data and categories
We adopted the provider perspective, considering real costs incurred. Costs were presented in Swiss Francs (CHF). Overhead costs were included and proportionally allocated. Costs were grouped into seven predefined categories:
Catering costs: Food and beverages provided to patients during hospitalization. Laboratory costs: Charges for internal and external laboratory testing and analyses. Materials costs: Consumable medical supplies, including cannulas, bandages, tubes, pumps, and implants. Patient management costs: Administrative services such as patient registration, medical controlling, bed management, and archiving of medical records. Pharmacy costs: All medications and related pharmaceutical products, including oral drugs, transfusions, and other therapeutic supplies. Room costs: Calculated based on standardized room-size pricing, including surcharges for private rooms and amenities such as telephony. Staff cost subcategories:
Nursing costs: Services provided by nursing staff, medical technical assistants, and pharmaceutical technical assistants, measured using TACS® nursing minutes—a Swiss system capturing direct and indirect nursing care time.40,41 Physician costs: Services provided by physicians across disciplines and levels of seniority, measured through effort points (Taxpunkte) assigned to each service.
42
Social counseling costs: Psychological and social support services, also quantified using fixed effort points. Therapy costs: Services delivered by physiotherapists, occupational therapists, and music therapists, measured through assigned effort points.
Swiss hospitals use a sophisticated cost allocation system that allows fine-grained attribution of resource use, which strengthens the accuracy of cost comparisons. This detailed accounting also supports policymakers seeking insights into which cost categories are most sensitive to sPC interventions.
Statistical analysis
Patient characteristics were summarized using medians (quartiles) for continuous variables and frequencies (%) for categorical variables. Comparisons between early and late cohorts were conducted using the Mann–Whitney–Wilcoxon or chi-squared tests. To account for skewed cost distributions, we applied bootstrap resampling (2000 iterations) to calculate bias-corrected mean ratios with 95% confidence intervals (CIs). P values were derived from bias-corrected point estimates using bootstrap standard errors and a normal approximation. We used a generalized linear model with a gamma distribution and log-link using inverse probability weighting to adjust for patient characteristics differences and including death year as proxy for inflation index. Propensity scores were derived from a logistic regression model including age, sex, marital status, nationality, insurance class, type of illness, and stay before admission to hospital. Inverse probability weights were evaluated by assessing covariate balance using a Love plot. Analyses were conducted using Stata 18 (StataCorp, College Station, TX).
Results
Study population
Between 2016 and 2022, a total of 10,558 patients died in the hospital. Of these, 790 patients met the eligibility criteria for inclusion in the study. We present a detailed flowchart of the study population in Figure 1.
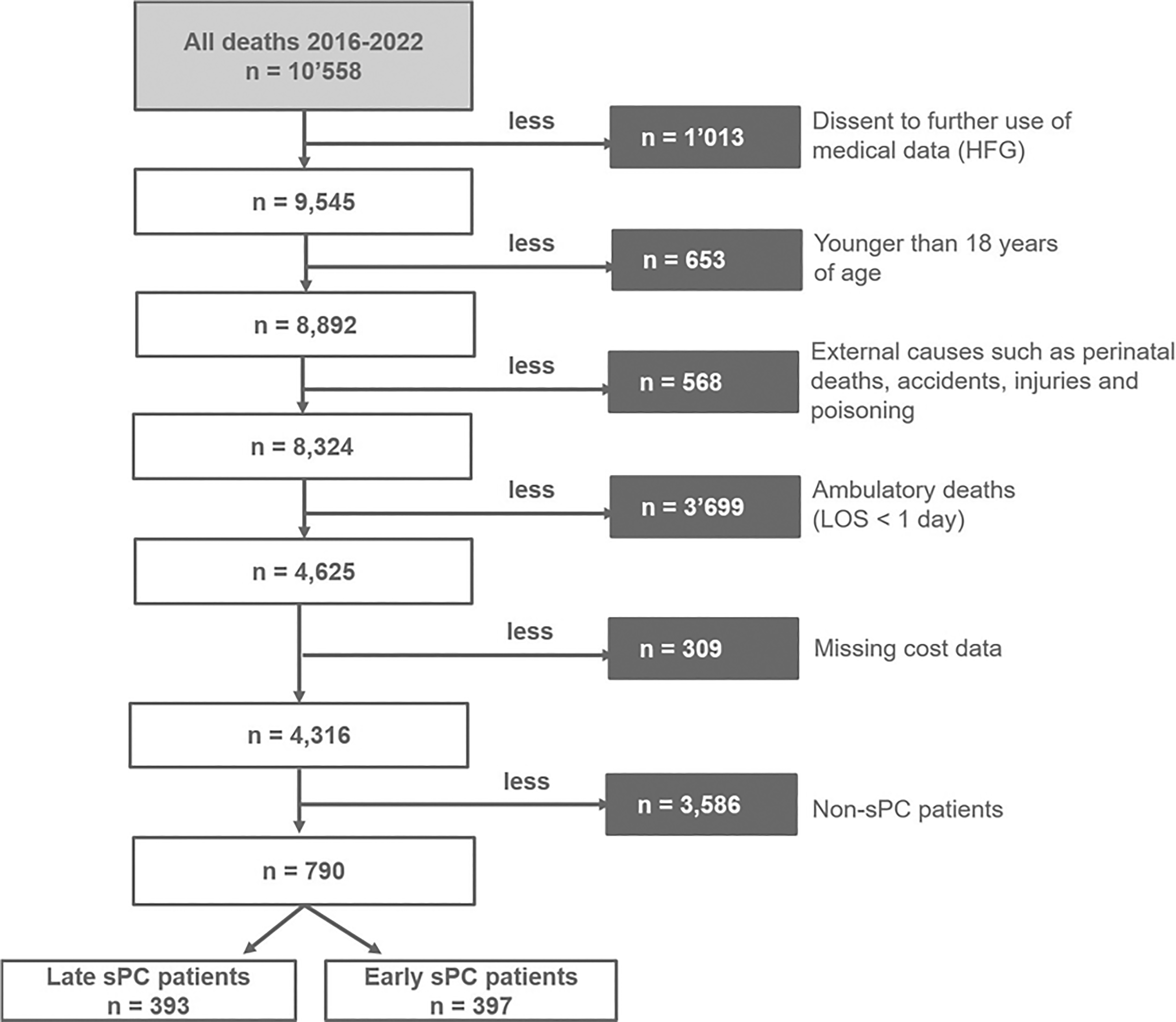
Inclusion flowchart for study population.
We included 397 early and 393 late sPC patients. Table 1 shows that the median age was 69 years (early sPC: 67; late sPC: 71; p < 0.001). The majority were men (early sPC: 62%; late sPC: 61%; p = 0.85), married (early sPC: 60%; late sPC: 60%; p = 0.34), of Swiss nationality (early sPC: 86%; late sPC: 88%; p = 0.43), and publicly insured (early sPC: 80%; late sPC: 77%; p = 0.45). Median hospital length of stay was shorter for early sPC patients compared with late sPC patients (8 vs. 16 days; p < 0.001). The median case-mix index was higher for late sPC patients compared with early sPC patients (2.5 vs. 1.4; p < 0.001). The majority of patients in both groups entered the hospital from home (63%).
Baseline Characteristics of Early and Late Specialist Palliative Care Patients Who Died Between January 1, 2016 Until December 31, 2022 in the University Hospital
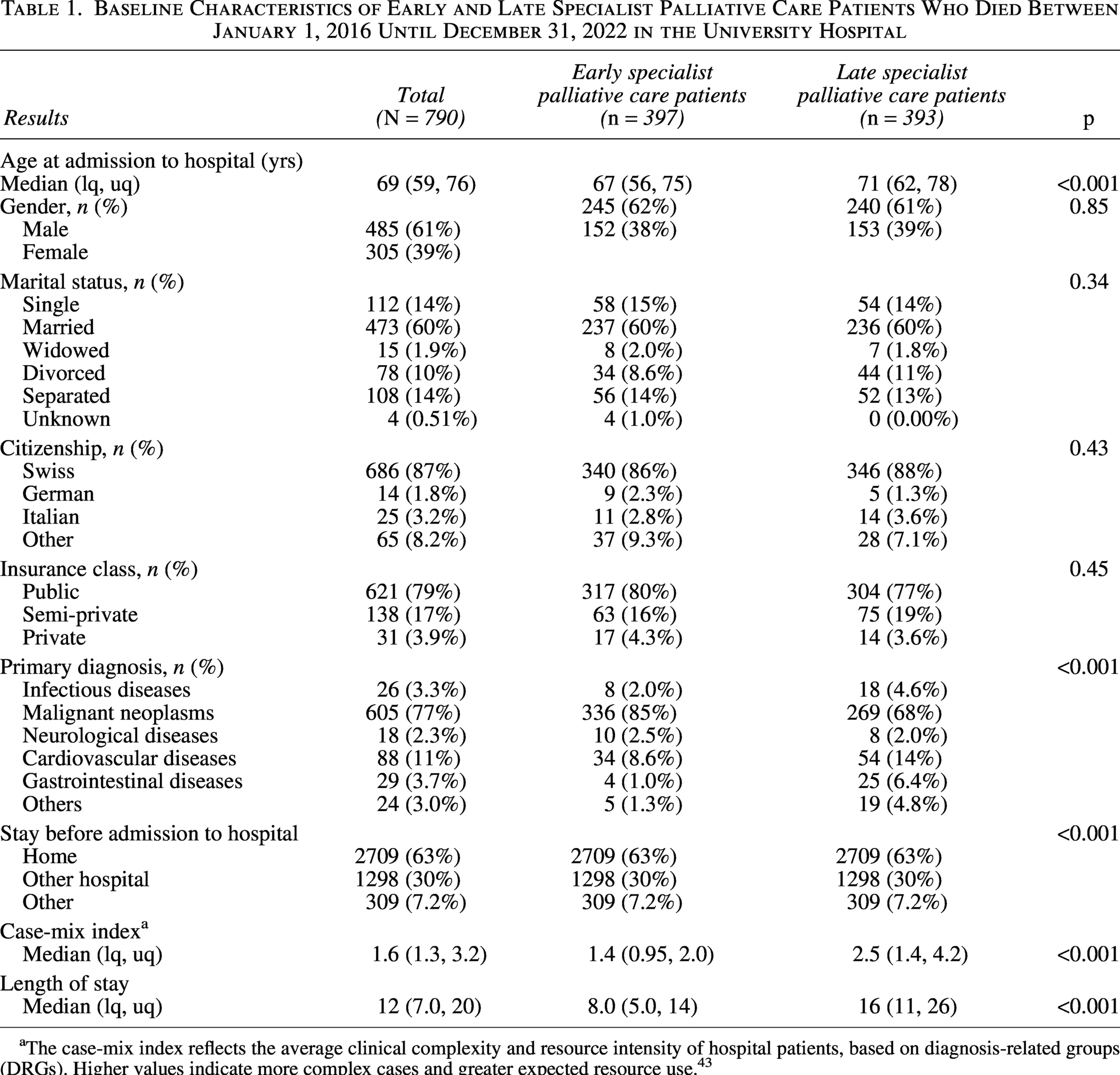
The case-mix index reflects the average clinical complexity and resource intensity of hospital patients, based on diagnosis-related groups (DRGs). Higher values indicate more complex cases and greater expected resource use. 43
Overall, 77% of patients in the cohort had a malignant neoplasm as their primary diagnosis. Diagnostic distribution differed between groups: in the early sPC group, 85% of patients had a malignant neoplasm compared with 68% in the late sPC group. Cardiovascular diseases were more frequent in the late sPC group (14%) than in the early sPC group (8.6%). The remaining patients had other nonmalignant primary diagnoses.
Cost analyses
Adjusting cost for difference in patient characteristics was performed with inverse probability of treatment weighting, which substantially improved covariate balance between groups. Supplementary Figure SA1 shows all standardized mean differences below 0.1, indicating adequate balance.
Overall hospital costs per stay
Table 2 shows that adjusted total hospital costs per stay were notable lower for patients receiving early sPC (CHF, 23,062; 95% CI: 21,305–25,141) compared with late sPC (CHF, 60,531; 95% CI: 55,156–66,909), mean ratio 0.38 (95% CI: 0.34–0.43; p < 0.001). Across all cost categories, expenditures were higher in the late sPC cohort. The largest relative differences were observed in laboratory, pharmacy, and physician costs, which were two-fold, six-fold, and two-fold higher, respectively, than in the early sPC group.
Comparison of Adjusted Overall Potential Mean Hospital Costs Per Stay of Early and Late Specialist Palliative Care Patients Using Generalized Linear Model with Inverse Probability of Treatment Weighting a
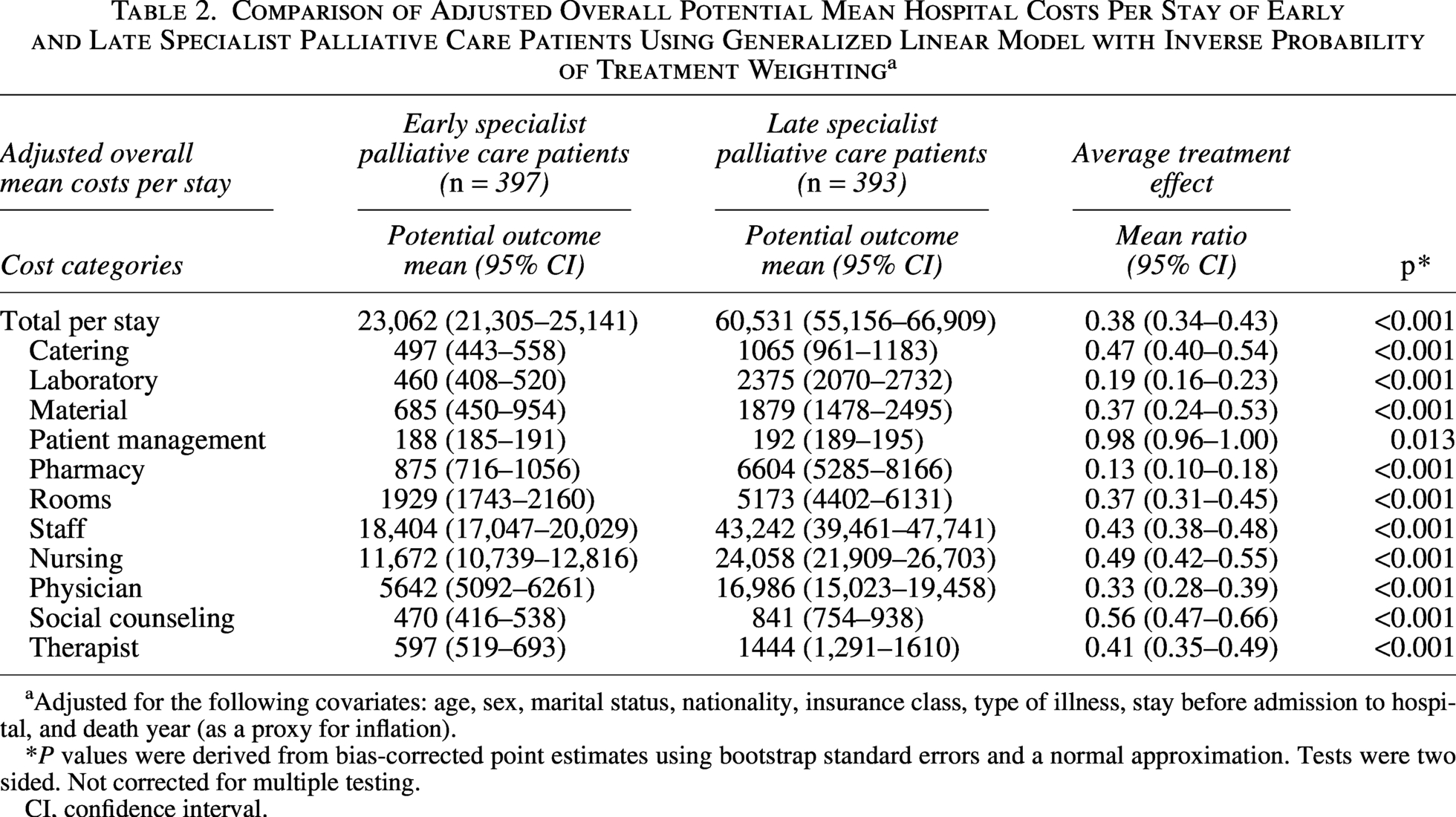
Adjusted for the following covariates: age, sex, marital status, nationality, insurance class, type of illness, stay before admission to hospital, and death year (as a proxy for inflation).
*P values were derived from bias-corrected point estimates using bootstrap standard errors and a normal approximation. Tests were two sided. Not corrected for multiple testing.
CI, confidence interval.
Daily hospital costs
Average daily costs are represented in Table 3. They remained lower in the early sPC group (CHF, 2651; 95% CI: 2470–2856) versus late sPC group (CHF, 2962; 95% CI: 2811–3134), mean ratio 0.90 (95% CI: 0.82–0.97; p = 0.010). Pharmacy costs accounted for the most striking relative difference in daily expenditures (−65%), with CHF 107 per patient per day in the early sPC group versus CHF 302 in the late sPC group (p > 0.001). Additional relative savings were observed in catering (−11%), laboratory (−58%), room (−30%), and material costs (−15%). In contrast, daily expenditures patient management costs (+250%) were higher in the early sPC compared to the late sPC group. Staff costs per day were similar (mean ratio 0.98).
Adjusted Potential Mean of Hospital Costs per Day of Early and Late Specialist Palliative Care Patients Using Generalized Linear Model with Inverse Probability of Treatment Weighting a
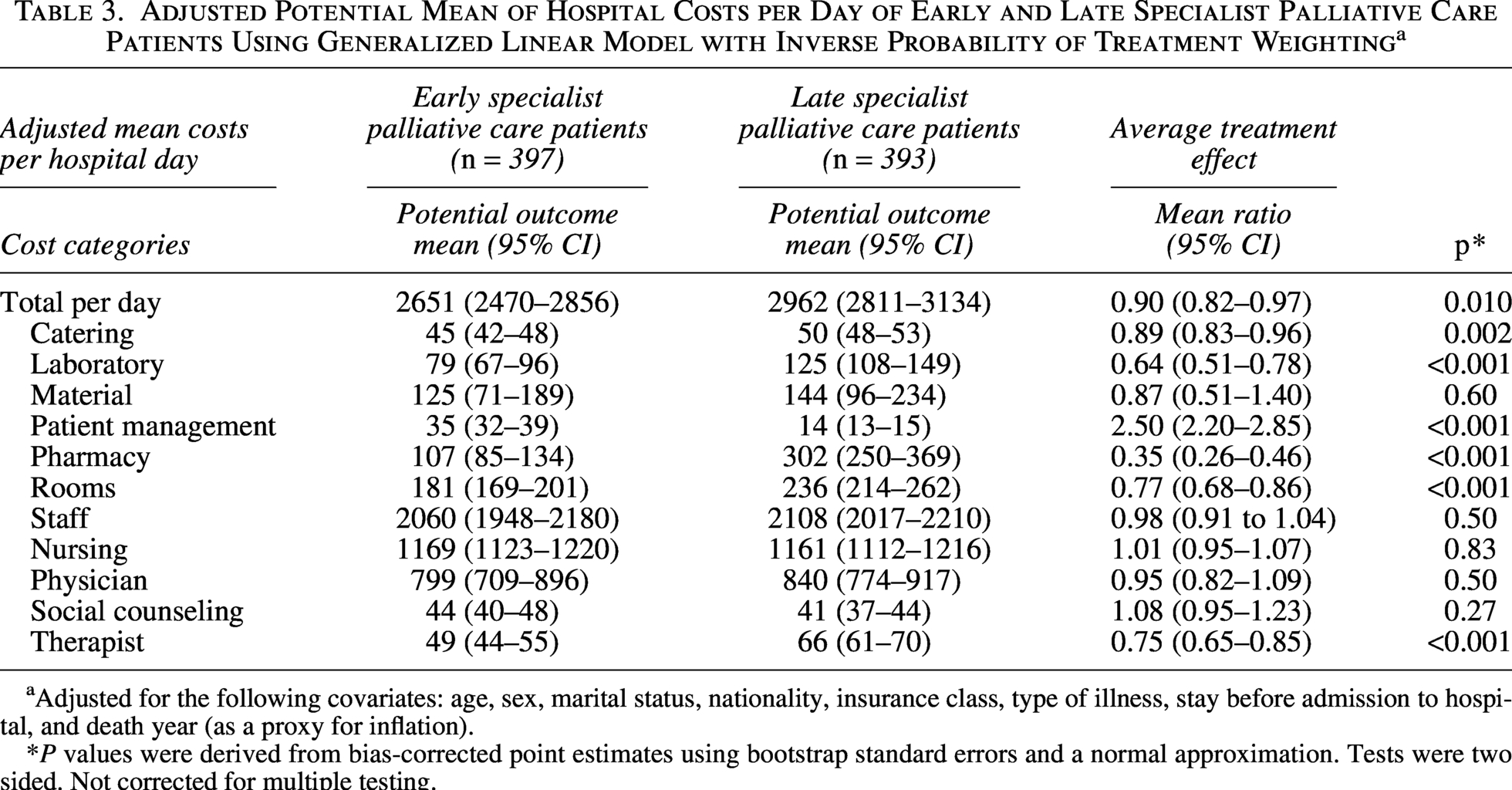
Adjusted for the following covariates: age, sex, marital status, nationality, insurance class, type of illness, stay before admission to hospital, and death year (as a proxy for inflation).
*P values were derived from bias-corrected point estimates using bootstrap standard errors and a normal approximation. Tests were two sided. Not corrected for multiple testing.
Discussion
Principal findings
This study provides evidence that early initiation of sPC during terminal hospitalization is associated with substantially lower overall and daily hospital costs compared with later referral. The largest relative cost differences per stay were observed in pharmacy, laboratory, and physician costs. These patterns suggest that late sPC is accompanied by substantially greater use of pharmacological interventions and diagnostic investigations—resource categories commonly associated with high-intensity, disease-directed care. When costs were examined on a per-day basis, total daily costs remained notably lower in the early sPC group, indicating that the cost difference reflects not only the shorter length of stay (LOS) in the early sPC group (median 8 vs. 16 days) but also a genuinely lower daily resource intensity. The most pronounced daily cost difference was observed in pharmacy expenditures, where early sPC patients incurred roughly one-third of the costs of late sPC patients.
Importantly, daily total staff costs were statistically similar between the two groups (mean ratio 0.98; p = 0.50). This finding suggests that cost reductions associated with early sPC are not driven by a reduction in direct patient contact or staffing intensity, but rather by a reduction in resource-intensive diagnostic and pharmaceutical interventions. In other words, early sPC appears to shift the composition of care away from high-cost technical interventions without diminishing the human care component, which is consistent with the goals of palliative care philosophy.
Comparison with literature
Our results support systematic reviews highlighting cost reductions when sPC is introduced in a timely manner across different health care settings.19,43 The pronounced decrease in pharmacy spending in our data, mirrors with a case–control study from the United States showing lower total hospital cost for patient admission to the palliative care unit, especially due to lower chemotherapy use and fewer aggressive interventions. 44 The direction and magnitude of our findings also align with two landmark US studies. May et al. conducted a prospective cohort study in 969 advanced cancer patients across five hospitals and found that consultation within two days of admission reduced total direct costs by 24% compared with no consultation, while consultation within six days still yielded a 14% reduction—demonstrating a clear dose–response relationship between earlier timing and greater savings. 6 Similarly, Zaborowski et al. reported that early palliative care consultations in a US academic center shortened LOS by ∼2.7 days and reduced overall hospital costs by more than USD 3000 per patient, reinforcing our observation that LOS reduction is a central mechanism of total cost savings. 29 Nevertheless, length of stay explains only part of this mechanism, as pharmacy use and diagnostic practices also contribute.
Not all studies, however, have found comparable cost reductions. Smith et al. noted in a systematic literature review that the evidence base on palliative care cost-effectiveness remains heterogeneous, with effect sizes varying substantially across settings, populations, and analytic approaches 11 This variability may partly be attributable to differences in patient populations, disease trajectories, timing of palliative care referral, and the organization of health care systems. Zhang et al.’s recent meta-analysis of 23 observational studies likewise reported considerable variability and attributed attenuated effects in some studies to reliance on insurance claims data rather than granular provider-level cost accounting. 7 Studies restricted to nonterminal admissions or lacking adjustment for disease severity and case-mix have produced smaller or no effects. Our study addresses several of these limitations by applying provider-perspective cost data captured at the level of individual medications, laboratory tests, and nursing minutes, and by adjusting for case-mix heterogeneity between groups through inverse probability of treatment weighting—factors that likely contribute to the comparatively large cost differences observed here.
Limitations
An important consideration in interpreting our findings is the contribution of LOS to the observed cost differences. The substantially greater differences in total hospital costs compared with daily costs suggest that shorter terminal hospitalizations in the early sPC group are a key mechanism underlying the overall savings. A limitation of the study is that the classification of late sPC inherently requires survival beyond the third hospital day, introducing the potential for time-dependent and immortal time bias. Patients must survive long enough or have a more favorable estimated prognosis to receive a later consultation, which may partly contribute to longer LOS and higher cumulative costs in this group.
In addition, the late sPC group likely represents a heterogeneous population. Differences in case-mix may further contribute to longer LOS: Patients in the late sPC group had a higher case-mix index, reflecting greater clinical complexity and resource intensity. By contrast, early sPC was more common among patients with advanced oncologic disease, whereas late sPC consultations were relatively more frequent among patients with cardiological conditions, who may follow different and less predictable disease trajectories. The relatively modest differences in daily costs indicate that the economic impact of early sPC is driven more by longer hospital stays than by large per-day cost reductions. These considerations are important for a nuanced interpretation of our findings within the context of end-of-life care.
Some additional aspects should be considered when interpreting these findings. The retrospective, single-center design may limit generalizability, and residual confounding cannot be excluded despite rigorous statistical adjustment. In particular, general administrative data do not capture all relevant patient-level factors such as documented advance care planning, patient preferences, or functional status at admission, which likely influence both the timing of sPC referral and the intensity of subsequent care. Furthermore, the absolute cost estimates reflect Swiss hospital tariffs; direct comparisons with other health systems should account for differences in their own case-mix compositions and palliative care infrastructure.18,19 Nonetheless, the large sample, comprehensive cost data, and consistent findings across multiple analytic approaches enhance the validity of the results. Moreover, our analysis was limited to inpatient sPC consultations and did not capture sPC provided in outpatient or community settings; therefore, we cannot account for prior or subsequent sPC involvement that may have influenced hospitalization outcomes.
Conclusion
Initiating sPC within the first three days of terminal hospitalization showed substantial reductions in total and daily costs through decreased resource use related to laboratory testing, pharmacological interventions, and material and room charges. Beyond economic consideration, intergrating sPC is already the preferred model of concurrent care for many inpatients nearing the end of life. Earlier referral therefore need not be justified on economic grounds alone. As pressures on hospital budgets intensify, embedding sPC early into acute care delivery may represent a high-value and economically sustainable strategy. Future research should examine whether alternative timing thresholds beyond the three-day cut-off, stratified by diagnostic group and illness trajectory, can further define the optimal window for sPC initiation and clarify the extent to which the observed cost differences reflect a causal relationship.
Authors’ Contributions
M.H.: Conceptualization, formal analysis, methodology, funding acquisition, writing—original draft, and writing—review and editing. M.S.: Conceptualization, formal analysis, and methodology. O.S.: Methodology, statistical analysis, and writing—review and editing. S.E.: Conceptualization and writing—review and editing. M.M.: Conceptualization, formal analysis, methodology, funding acquisition, writing—original draft, and writing—review and editing. All authors approved the final article and agree to be accountable for the work.
Research Ethics
Ethical approval for this study was obtained from the Ethics Committee of the Canton of Bern (BASEC-ID: 2021-00253).
Data Management and Sharing
Due to institutional policies and strategic restrictions by the university hospital’s finance department, raw cost data cannot be shared. Other data are available upon reasonable request.
AI Use Disclosure
This article benefited from the use of OpenAI’s, GPT-5 and Claude Sonnet 4.6 (Anthropic, 2025) for language refinement. The AI tools were used only to improve readability and efficiency; all interpretations, data analyses, and conclusions are the sole responsibility of the authors. The authors have verified the accuracy and integrity of all AI-assisted content.
Footnotes
Author Disclosure Statement
The authors declare no competing interests.
Funding Information
This work was supported by the Swiss National Science Foundation (10531G_212822). The grant provider had no influence on designing the study; collecting, analyzing, and interpreting data; writing the report; and deciding to submit the article for publication.
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.