
Abstract
Introduction:
Clinical reasoning is essential for hospice and palliative medicine (HPM) fellows, yet structured assessment tools are lacking. The Assessment of Reasoning Tool (ART) has shown positive results for early learners but has not been applied to advanced learners.
Methods:
We conducted an 18-month mixed-methods study at a single academic center. Seven fellows and seven faculty participated. Faculty used the ART every day during clinical teaching rounds on a fellow’s inpatient rotation. Pre- and post-intervention surveys assessed the ART via 4-point Likert scale and free-response questions.
Results:
Fellows reported increased feedback on clinical reasoning (2.33 vs. 3.25; p = 0.05) and reflection on cognitive bias (2.67 vs. 2.81; p = 0.02), and no difference in satisfaction with feedback, comfort with clinical reasoning terminology, and time spent on feedback. Faculty reported no difference across all areas. Both groups cited time constraints and a need for clearer guidance on effective use as barriers to using the ART. Qualitative themes highlighted the ART as a diagnostic versus management reasoning tool, limited application to non-symptom-based case scenarios, and persistent faculty discomfort despite training.
Conclusion:
This study suggests the ART is feasible for HPM fellowship training and may enhance certain aspects of clinical reasoning assessment for fellows, particularly during early fellowship. However, its broader utility is limited by the absence of faculty-perceived benefit, persistent faculty discomfort with implementation, and the tool’s emphasis on diagnostic rather than management reasoning. Further research on effective faculty development and assessment tools tailored to management reasoning would help define the optimal role of the ART in HPM training.
Keywords
Introduction
Clinical reasoning is an essential skill in medical education 1 and is defined as the cognitive process of evaluating and managing a patient’s medical problems. 2 Within graduate medical education, there is increasing recognition of the need to explicitly teach and assess clinical reasoning.1,3,4 Clinical reasoning includes diagnostic reasoning, the process of identifying what disease a patient has 5 ; and management reasoning, the process of making decisions about patient management, including choices about tests, treatment, allocation of resources, and follow-up. 6 Prior work suggests that diagnostic reasoning is focused earlier in medical training while management reasoning becomes increasingly prominent as trainees progress. 7
In hospice and palliative medicine (HPM), clinical reasoning is especially important due to the potential uncertainties that arise in diagnosis, prognosis, and treatment pathways for patients with serious illness and the goal to align our support and treatments with patients’ values and priorities. However, there is a dearth of structured approaches to assess clinical reasoning skills for HPM trainees.4,8
Workplace-based assessments (WBAs) are assessment tools for advanced trainees that facilitate feedback at the “does” level based on the extended Miller’s pyramid.9,10 Current WBAs specific to HPM focus more on whether specific content is collected,8,11,12 whereas assessing clinical reasoning requires understanding the learner’s cognitive process. While recent literature emphasizes the need for more robust assessment strategies in HPM fellowship training, 4 clinical reasoning assessment remains underrepresented.
The Assessment of Reasoning Tool (ART), developed in 2018, is a WBA focusing on diagnostic reasoning. It assesses five domains: hypothesis-driven data gathering, constructing a problem representation, forming a differential diagnosis, developing a plan with prioritization, and reflecting on cognitive biases. 13 The ART has demonstrated efficacy and feasibility in assessing clinical reasoning and facilitating structured faculty feedback for pediatric interns. 5 To the best of our knowledge, the ART has not been applied to more advanced medical learners such as HPM fellows. Of note, assessment tools for management reasoning are in development,6,14 but none have been validated to date.
This study evaluates the feasibility of implementing the ART in HPM fellowship training and explores its impact on clinical reasoning assessment using a mixed-methods approach.
Methods
Study design, setting, and participants
We conducted a mixed-methods study at a single academic quaternary medical center with an ACGME-accredited HPM fellowship. The fellowship has three to four HPM fellows annually with nine supervising faculty members (including two of the study authors). The study was conducted over 18 months to evaluate two fellow cohorts. Quantitative and qualitative data were collected from HPM fellows and their supervising HPM faculty via pre- and post-intervention surveys. Primary outcomes were effectiveness and satisfaction with ART compared to traditional clinical teaching rounds. Secondary outcomes included ease of use and challenges with implementation.
Survey design
We created anonymous online surveys with quantitative and open-ended questions distributed via Qualtrics. The survey underwent iterative review by the study authors and a content expert. We also conducted cognitive interviewing and pilot testing with an HPM fellow–faculty pair to strengthen evidence for validity. 15 The survey evaluated six aspects of clinical reasoning via 4-point Likert scale items (1 = least favorable, 4 = most favorable); domains are detailed in Table 1. The post-intervention survey also inquired about the number of uses needed for an HPM fellow or faculty member to develop comfort with the ART, how much time was added to clinical teaching rounds by using the ART, and barriers to use.
Summary of Pre- Versus Post-ART Survey Responses from HPM Fellows and Faculty
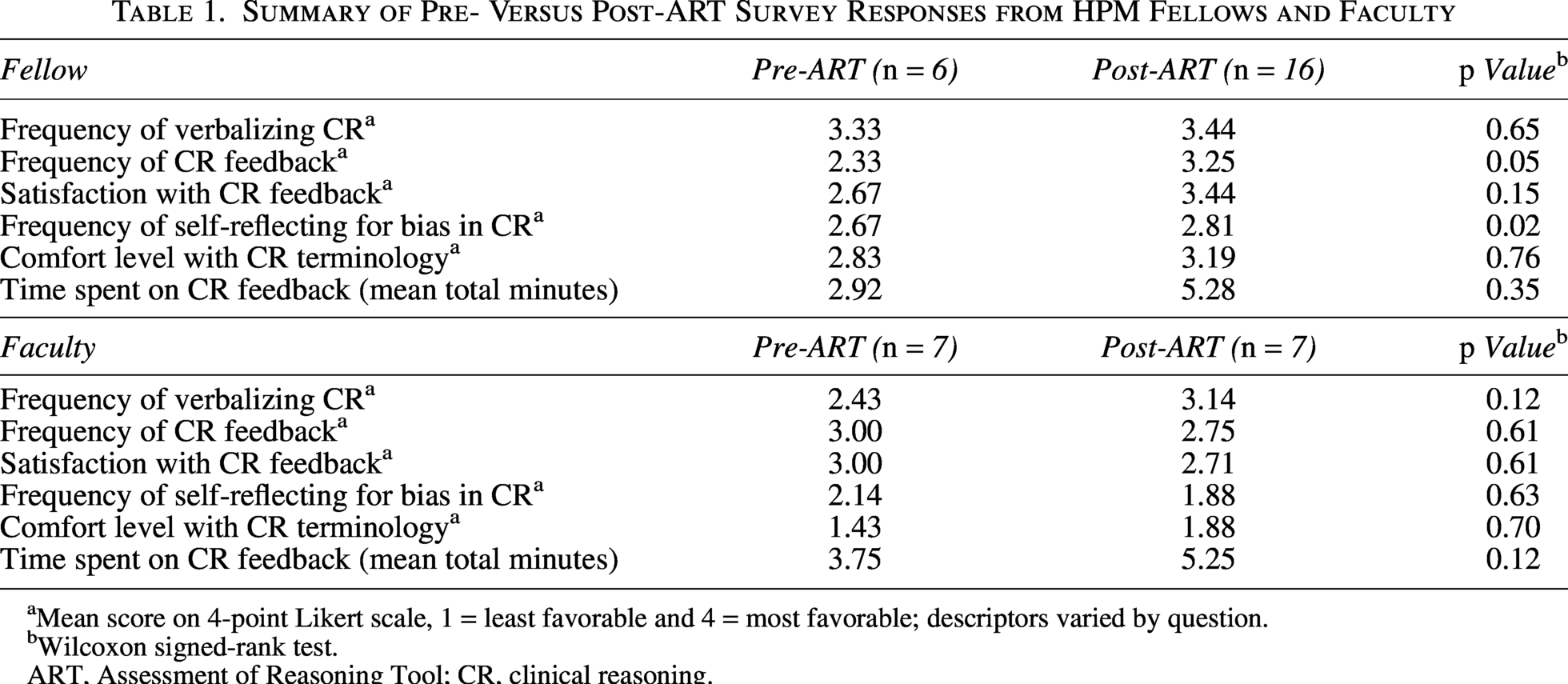
Mean score on 4-point Likert scale, 1 = least favorable and 4 = most favorable; descriptors varied by question.
Wilcoxon signed-rank test.
ART, Assessment of Reasoning Tool; CR, clinical reasoning.
Faculty development
Six HPM faculty (excluding two study authors) attended a one-hour faculty development session that included a review of clinical reasoning terminology, introduction to the ART, and practice with case scenarios to develop a shared mental model. No introductory sessions were conducted for the fellows.
Implementing the ART
The ART and pre-intervention surveys were emailed to both the fellow and faculty on Day 1 of the fellow’s hospital consultation service rotation (two to four weeks long), with instructions to complete the surveys prior to clinical teaching rounds. Afterward, faculty were asked to use the ART daily during the fellow’s first new patient presentation. Use of the ART was limited to case scenarios involving uncontrolled symptoms based on pilot feedback. New case scenarios were selected because they most consistently require diagnostic reasoning. Post-intervention surveys were distributed to fellows and faculty at the end of each week.
Data collection and analysis
Pre-intervention surveys were collected once prior to ART use, while post-intervention surveys were collected weekly. Because of the small sample size, repeated weekly responses from the same participant were included in both descriptive and inferential analyses. Quantitative data were summarized by participant (fellow vs. faculty) and intervention (pre- vs. post-) before statistical analyses (Wilcoxon rank-sum test). Qualitative data were analyzed using inductive thematic analysis by one study author (A.C.). Paired pre- and post-intervention responses were only used for ad hoc descriptive analysis of perceived time added by using the ART.
Results
Participants and survey responses
Seven HPM fellows and seven HPM faculty participated in the study. Six fellows (86%) completed the pre-intervention survey, and all seven fellows completed the post-intervention survey, with a total of 16 responses (three fellows completed the survey at multiple time points). All seven faculty members completed the pre-intervention survey, and five completed the post-intervention survey, with a total of eight responses (three faculty members completed the survey at multiple time points).
Pre-intervention versus post-intervention
Fellows reported significant increases in the frequency of feedback on clinical reasoning (2.33 vs. 3.25; p = 0.05) and self-reflection for cognitive bias (2.67 vs. 2.81; p = 0.02). They reported no difference in frequency of verbalizing clinical reasoning, satisfaction with clinical reasoning feedback, comfort level with clinical reasoning terminology, and time spent on clinical reasoning feedback. In contrast to fellows, faculty did not report any significant changes between pre- and post-intervention survey responses (Table 1). Overall, fellows somewhat agreed (12 responses [75%]) or strongly agreed (four responses [25%]) that the ART was perceived as effective in assessing clinical reasoning, whereas faculty responses ranged from somewhat disagree (four responses [50%]) to somewhat agree (three responses [38%]).
Post-intervention surveys also showed that all fellows (100%) felt comfortable with the ART within the first week of use, while 50% of faculty responses showed they never became comfortable with the ART. In terms of perceived time added by the ART to the case presentation/teaching during rounds, 50% of fellow responses reported no added time, while faculty responses showed up to 10 minutes were added (Fig. 1). The most frequently cited barriers to ART use were lack of time (eight fellows [50%] and six faculty [75%]) and clearer guidance on how to use the ART (five fellows [31%] and two faculty [25%]).
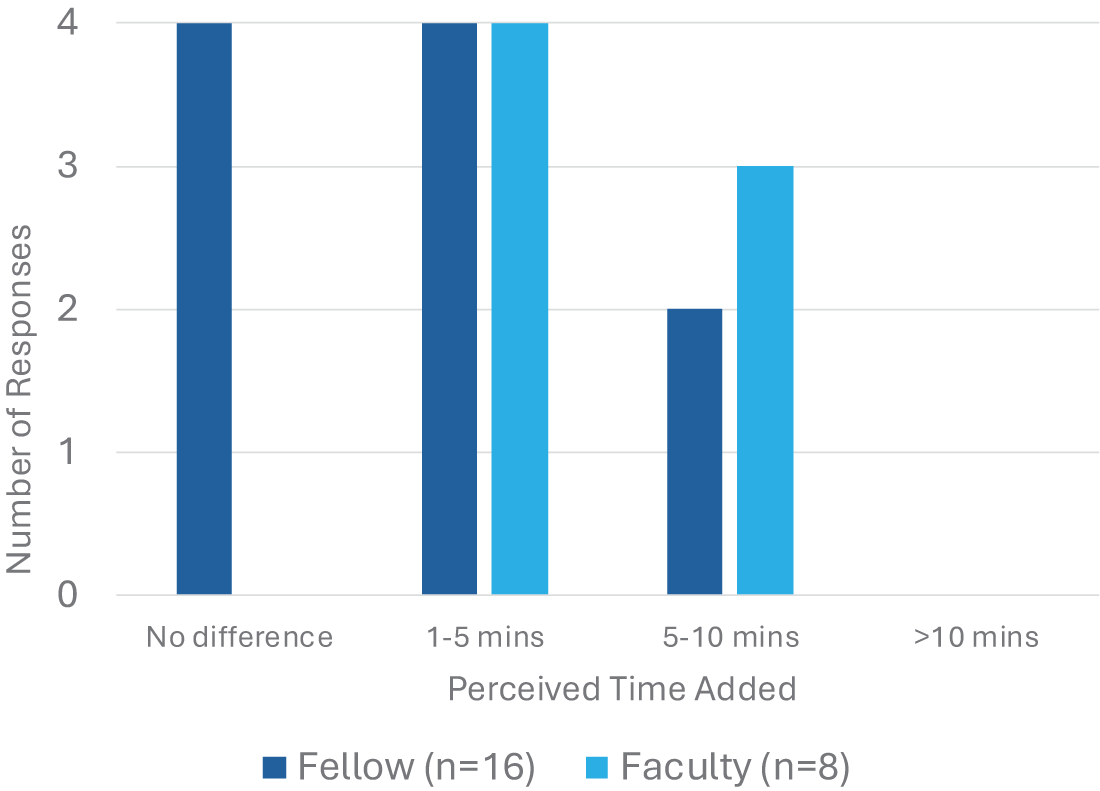
Perceived time added to clinical teaching rounds by using the ART. ART, Assessment of Reasoning Tool.
Qualitative results
Qualitative post-intervention surveys (four fellow and six faculty responses) revealed three themes: focus on diagnostic reasoning when most HPM case scenarios emphasize management reasoning; limited applicability beyond symptom-focused case scenarios such as clarifying goals of care; and a need for clearer guidance on how to use the ART effectively. Table 2 shows representative quotes for each theme.
Themes and Representative Quotes from Qualitative Analysis
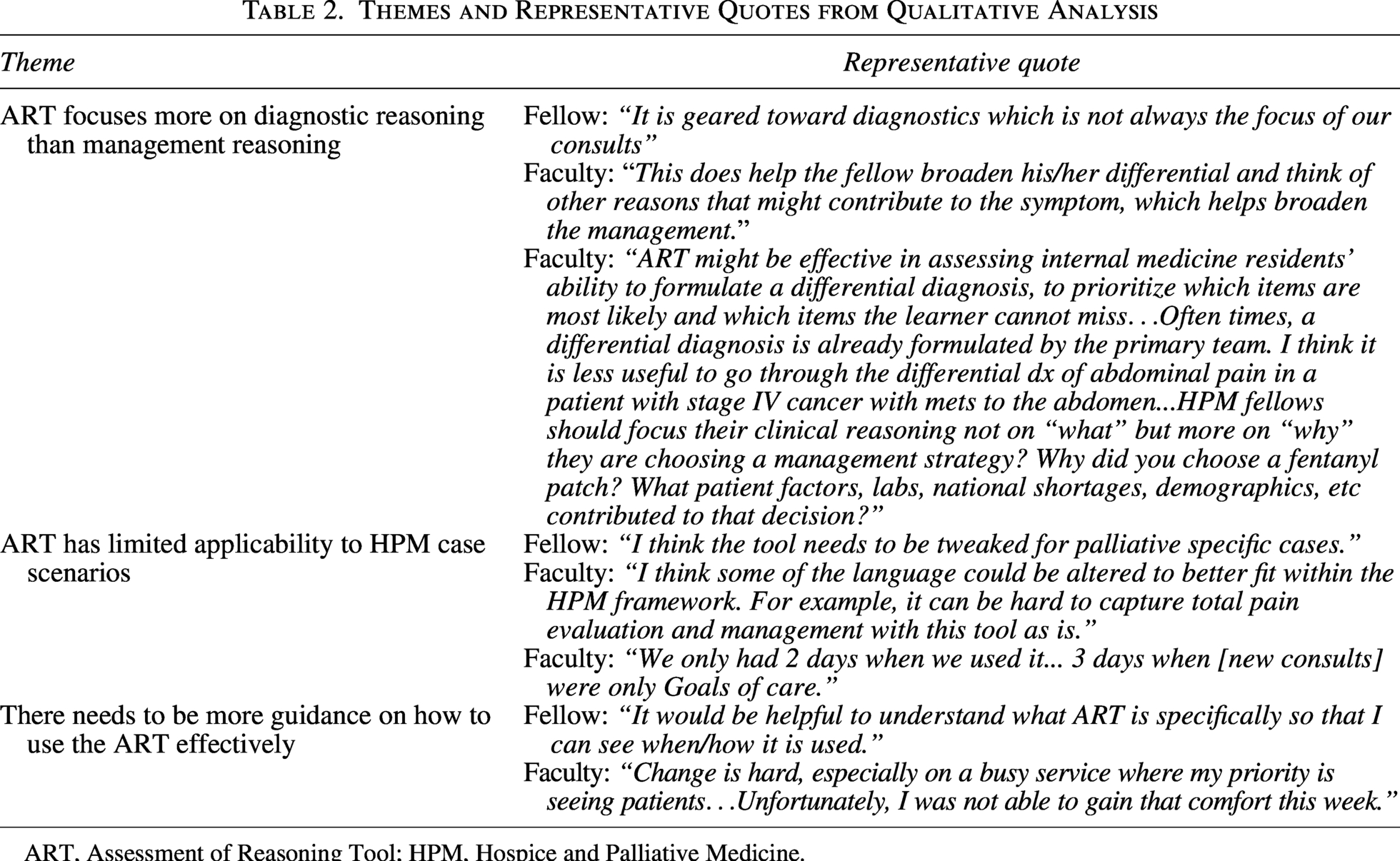
ART, Assessment of Reasoning Tool; HPM, Hospice and Palliative Medicine.
Discussion
We found that the implementation of the ART, a published tool for assessing diagnostic reasoning, in HPM fellowship training was feasible. Fellows perceived improvements in certain aspects of clinical reasoning feedback and reflection. However, faculty did not report similar benefits, and several limitations constrain the tool’s applicability for HPM faculty and fellows.
The improvement in the frequency of feedback on clinical reasoning and self-reflection for cognitive bias among fellows suggests the ART provides an opportunity for fellows to receive feedback and reflect in the diagnostic reasoning domain. The HPM fellows may have been more engaged knowing that they were being assessed at the “does” level of the extended Miller’s pyramid, where competence transitions to entrustment for independent practice.10,16,17 Moreover, structured WBAs such as the ART help establish shared mental models between learners and faculty, which in turn promotes meaningful feedback. 18
In contrast, faculty did not perceive a meaningful improvement in assessing HPM fellows’ clinical reasoning with the ART. We noted that the type of clinical reasoning being assessed may not have aligned optimally with the learner stage of a fellow. The ART focuses on diagnostic reasoning. 5 However, much of the clinical reasoning for HPM clinicians and thus HPM fellows often centers more on management reasoning. 6 Several qualitative comments echoed this distinction, pointing out that HPM training often occurs in the context of developing a plan rather than establishing a diagnosis. Nonetheless, one faculty commented on the benefit of developing a broader differential diagnosis, which remains a valuable skill, particularly for early fellows.
A second explanation for the faculty perception is the limited application of the ART across all HPM case scenarios. Based on feedback from the pilot study, faculty were guided to use the ART for cases of uncontrolled symptoms. Faculty provided qualitative comments regarding this limitation, reflecting their broader clinical experience and consideration of how the ART might not be applicable to non-symptom-based HPM case scenarios.
A third explanation is that social desirability bias may have inflated the fellow ratings, considering the small sample size. This is less likely, as our findings reflect prior work showing that trainees report greater confidence in their program’s ability to assess clinical reasoning than the faculty express. 4 Actively engaging fellows during faculty development could further improve the quality of the shared mental model and potentially increase the perceived impact of the ART by faculty.
A fourth explanation is that faculty may have experienced ceiling effects in self-assessed outcomes given their established baseline assessment practices. This is supported by the pilot survey data, which showed that most faculty rated existing clinical reasoning assessment tools (e.g., chart stimulated recall, postencounter note, script concordance tests) as somewhat or very effective. Considering the additional resources associated with learning a new WBA, the benefit of the ART may not have been perceived as significant compared to prior assessment tools.
While both fellows and faculty perceived no to minimal added time to clinical teaching rounds, “lack of time” remained the most frequently cited barrier to using the ART. This paradox may reflect the cognitive load associated with using assessment tools. 19 Ad hoc analysis of paired observation data showed repeated ART use did not lessen the perceived time added. Moreover, despite a dedicated faculty development session, qualitative data from faculty revealed a lack of comfort and uncertainty about the ART—consistent with literature showing that one-time faculty development sessions have limited impact. 20 The fact that 85% of faculty shared a lack of comfort with WBAs during the pre-intervention survey highlights the ongoing challenge of effective faculty development in the era of competency-based medical education. 21 The request for clearer guidance from both fellows and faculty reinforces this idea and aligns with prior research that faculty often experience discomfort and low confidence when implementing new WBAs without calibration. 22 It is important to recognize that faculty are the key to any assessment tool’s effectiveness. 16 Achieving consistent assessment of clinical reasoning—both diagnostic and management—will require ongoing faculty development and broader cultural shifts within HPM.
Limitations of this study include the single-site design and small sample size. Repeated weekly responses from the same participants were included in inferential analyses, which may have introduced non-independence that could have inflated the statistical significance. Completed ART forms were not collected or analyzed. This may have clarified the scope of HPM case scenarios appropriate for the ART.
In conclusion, implementation of the ART in HPM fellowship training is feasible, and fellows perceived improvements in feedback and reflection on their clinical reasoning. However, the absence of faculty-perceived benefit, persistent discomfort despite dedicated faculty development, and the tool’s focus on diagnostic reasoning raise important questions regarding its application to HPM with a cost–benefit tradeoff. In its current form, the ART may be better suited as an early-fellowship adjunct rather than a standard assessment tool in HPM fellowship training. Further research, particularly on faculty development and assessment tools for management reasoning, would help define the optimal role for the ART.
Footnotes
Acknowledgments
The authors would like to thank Dr. Jennifer Kapo for serving as content expert; Julie Palmer-Hoffman, APRN, for serving as cognitive interviewer; Dr. Dmitry Kozhevnikov and Dr. Caitlin Bennet for participating in the pilot study; and Cole Cassady, MS4, for statistical analysis.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.