
Abstract
Internal Family Systems (IFS) is a psychotherapeutic model that conceptualizes human experience as shaped by different internal “parts” that respond to stress, threat, and vulnerability in patterned ways. In the setting of serious illness, these parts may become increasingly polarized or extreme, contributing to rigidity, ambivalence, emotional narrowing, or disengagement. By integrating IFS principles with serious illness communication, palliative care clinicians can better understand these responses as protective rather than pathological. This article uses a clinical case to illustrate how an IFS-informed approach can help clinicians identify and work with protective and vulnerable parts, including Managers, Firefighters, and Exiles, while supporting access to the Self as a source of calm, curiosity, and clarity. Through techniques such as recognizing and exploring activated parts, relating to protective responses with greater compassion, and tracking multiple parts within a single encounter, clinicians may help reduce inner conflict, soften reactivity, and support more flexible, values-concordant coping in serious illness care.
Keywords
Introduction
Internal Family Systems (IFS) is a psychotherapeutic model that conceptualizes the mind as composed of multiple internal “parts,” each shaped by life experience and organized around distinct emotions, beliefs, and protective functions. 1 Rather than viewing internal conflict or extreme reactions as evidence of pathology, IFS offers a nonpathologizing framework for understanding how different parts of a person attempt to respond to threat, vulnerability, and overwhelm. 1 Although the literature on IFS in serious illness care remains limited, emerging evidence suggests potential benefit across medical contexts.2–4 IFS may be particularly useful in serious illness care, where patients often confront uncertainty, altered identity, threatened autonomy, anticipatory loss, mortality, and profound suffering. 6 5,7,11 In these settings, coping may become narrowed, rigid, or polarized. What appears outwardly as ambivalence, avoidance, urgent symptom focus, or intense control-seeking may be a manifestation of an internal system attempting to protect the person from experiences that feel intolerable.7–9 In this way, IFS aligns with the growing emphasis in palliative care on formulation: the intentional effort to understand why a patient may be coping in a particular way at a particular time, so that communication can be more therapeutically aligned with underlying psychological needs.7,8,10
Using a case-based approach, this article demonstrates how clinicians can adapt IFS principles in serious illness communication (SIC) to address internal tension, protectiveness, and emotional polarization. We illustrate how recognizing and responding to protective and vulnerable parts may help clinicians better accompany patients through distress, reduce shame, and support more flexible, values-concordant coping. This article is the fifth in a nine-paper series on psychotherapeutically informed SIC.9,11
Case Description
Maya is a 51-year-old cisgender female who was recently diagnosed with stage IV pancreatic cancer. She has worked as an intensive care unit nurse for the last 25 years and arrives at the clinic with a list of questions and highlighted journal articles. When the discussion turns to values, she redirects briskly: “Just tell me the regimen, the response rates, and the timeline. I want to start treatment as soon as possible.”
During a hospitalization for uncontrolled pain, Maya repeatedly presses the team for faster imaging, earlier medication adjustments, and clearer timelines. When the team and her wife explore topics of emotional or spiritual distress, her reports of physical pain intensify and become her focus. Later, in a quieter moment, when the team asks about her teenage sons, her eyes briefly fill with tears before she straightens and turns back to the whiteboard schedule. “They’re fine,” she says. “They’re strong.”
Discussion
When the team attempts to explore emotions or the impact on her family, Maya quickly pivots to logistics and care planning. This pattern of rigidity and avoidance seems to suggest the inner conflict of distancing herself from experiencing anticipatory grief and fear. In the hospital, Maya’s distress presents as escalating pain scores that appear to be relieved only by pain medicine. From an IFS lens, Maya appears to protect herself by restricting discussion to the narrow range of topics she can immediately tolerate. Communication strategies informed by IFS principles can help address Maya’s underlying psychological needs, softening internal conflict and promoting flexibility.1,6–8
IFS principles
From an IFS perspective, people have many “parts” within their internal landscape, but are ideally guided by the Self, a central and steady core within each individual.1,13 Under intense stress, however, protective internal parts may become more dominant and assume more extreme roles. Instead of seeing these as flaws, IFS conceptualizes these parts as protective, attempting to manage fear, uncertainty, or prior wounds (see Table 1). The goal of IFS-informed communication is to support the Self, the organizing center characterized by calmness, curiosity, and clarity, in regaining a leadership role. 1
Roles of Protective and Vulnerable Parts in Internal Family Systems
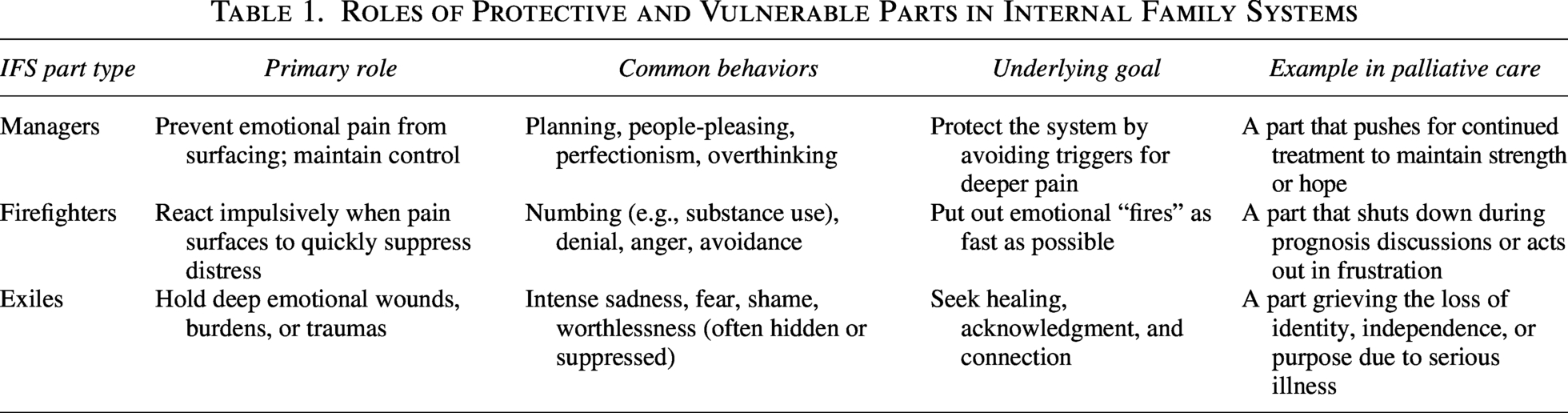
The IFS framework organizes the protective inner parts into three main roles: Exiles, Managers, and Firefighters.
Maya’s case illustrates how these roles may emerge in a single clinical encounter: a highly competent and experienced nurse planning for her care and keeping emotion at a distance; a clear narrowing of attention to symptoms when distressed; and brief moments of raw vulnerability at the mention of her family that get quickly extinguished. Table 2 considers how different parts of Maya become activated at different points of the clinical encounter.
Considering Maya’s Clinical Encounter Through an Internal Family System LensIFS Part How the Part May Manifest in May
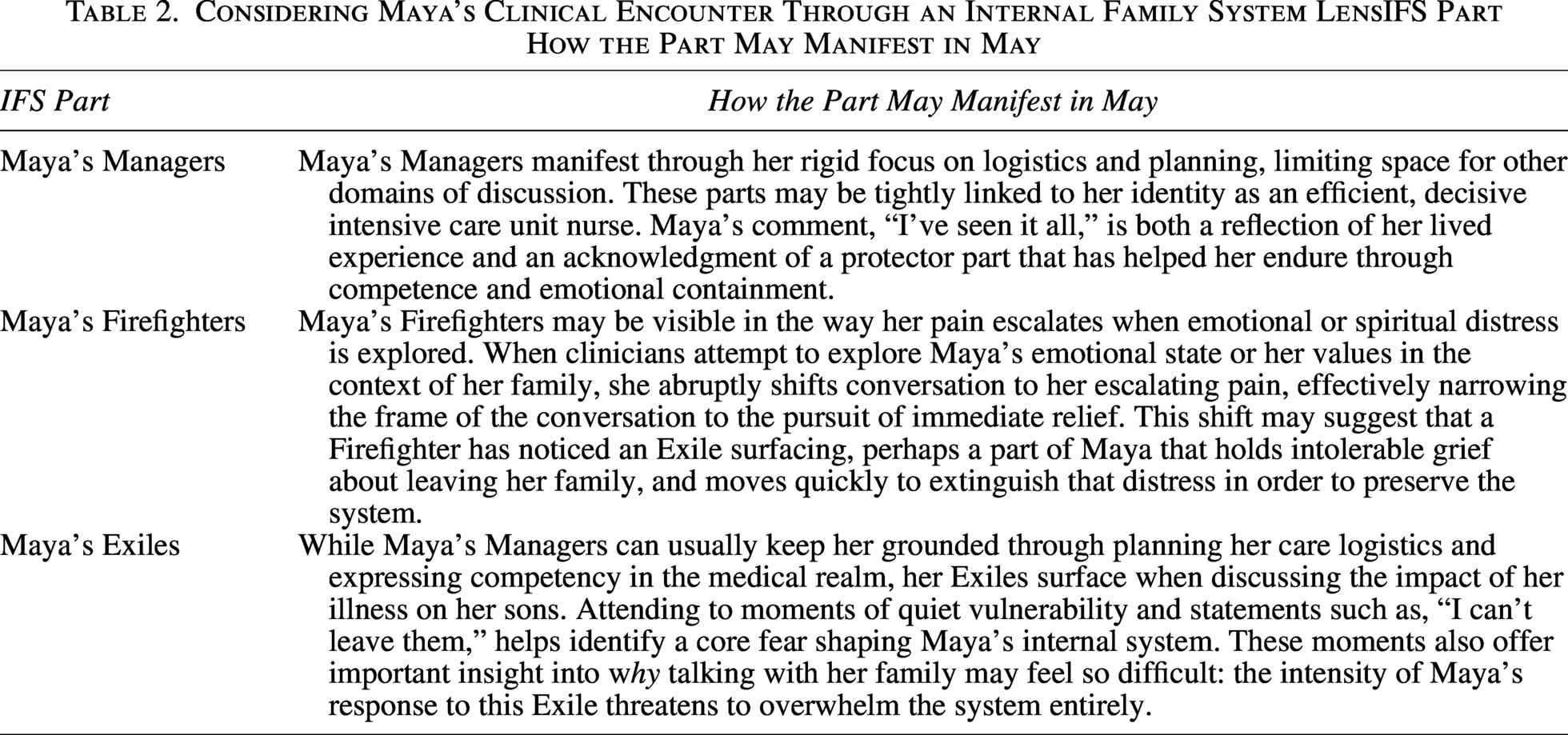
In Maya’s case, the team is not concerned that Maya and her wife do not understand her situation. Rather, the concern is that very important moments, including sitting with uncertainty, prognosis, trade-offs, and anticipatory work with her family, cause a shift in Maya’s ability to meaningfully engage. Over time, this may lead to a delay in value exploration and missed opportunities for connection facilitation with loved ones. As a result, Maya may make treatment decisions more based on fear and avoidance than on her deeper needs and values. An IFS lens offers a non-pathologizing way to understand these inner conflicts as protective responses.6–8,14
IFS principles inform practical communication techniques that can reduce polarization, support clinical pacing, and help patients like Maya access curiosity, compassion, and calmness in making values-based decisions. Recognizing that formal, operationalized IFS is outside the scope of general palliative care practice, below we describe IFS-informed SIC strategies that palliative care clinicians can readily apply in routine care.9,11
SIC techniques aligned with IFS principles
In a patient with intense inner conflict, the goal of IFS-informed SIC is to help the patient develop a more curious and compassionate relationship with activated parts, allowing protective patterns that have become rigid or extreme to soften. In turn, this may help the patient regain greater internal flexibility and authentic choice. When the Self becomes more accessible, it allows patients to respond to stressful situations with greater clarity, flexibility, and choice, while still valuing all internal parts. Clinicians can follow the part that is most activated or accessible, using the techniques below in a safe and paced manner.
1) Recognize and understand the part
Recognizing and understanding the part facilitates the process of differentiation—becoming aware of distinct internal experiences. One can imagine this process like untangling a knot to understand each individual strand as a part of the larger whole. This can allow unblending, or the ability to observe what is happening inside oneself, rather than feeling fully swept up in it. A feeling becomes something one experiences rather than something one is. 1
Recognizing and understanding the part maps to the first three Fs of the 6-F mnemonic presented in Table 3: Find the part, Focus on the part, and Flesh Out the part. The strategies below explore what that might look like in Maya’s case.
The “6 Fs” Framework for Engaging Protective Parts in Internal Family Systems
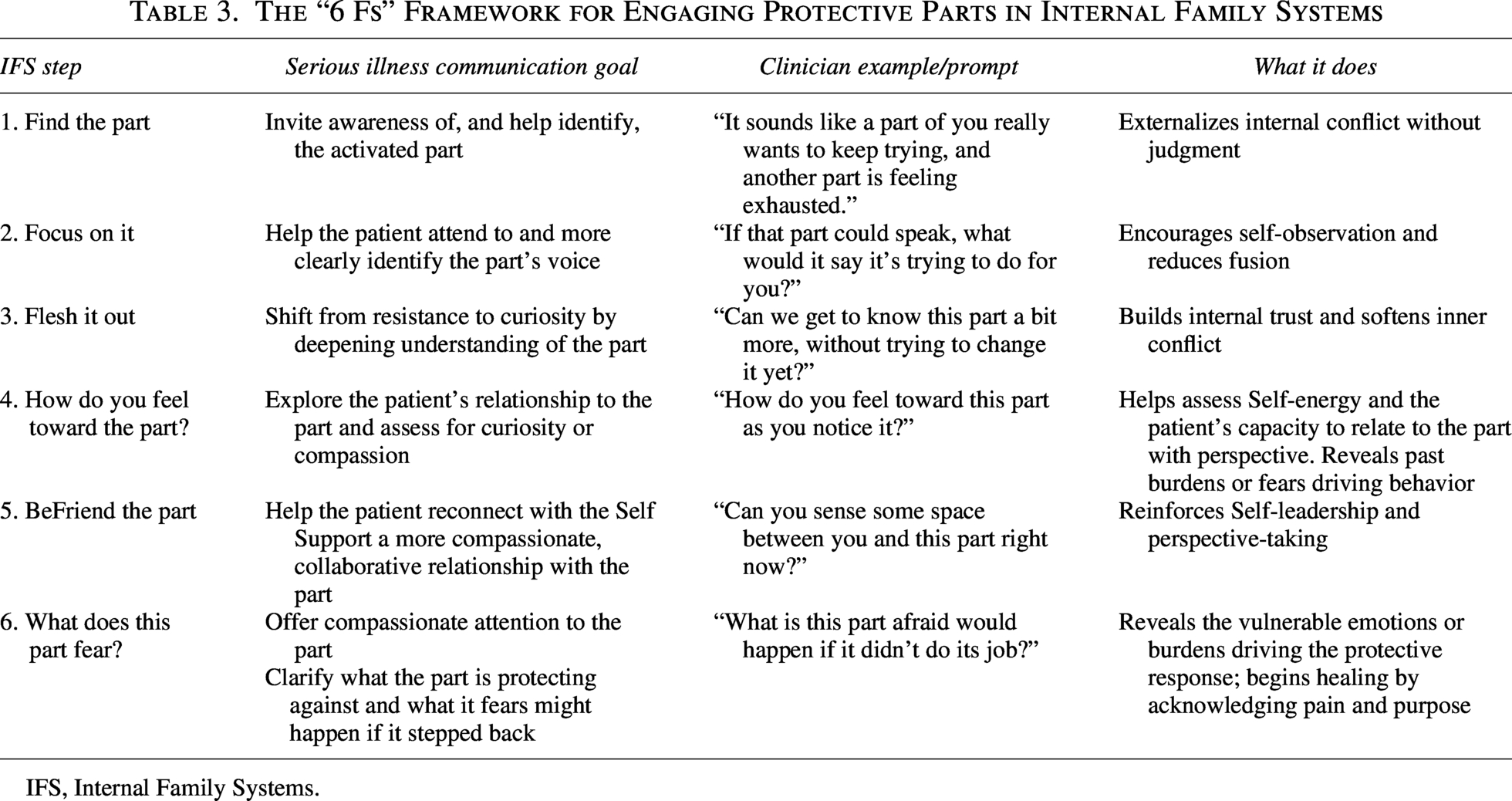
IFS, Internal Family Systems.
As we talk about this, I am noticing a part of you that is working very hard to keep your care moving forward.
Where do you feel the Manager in your body? In your chest? Is there tightness in your jaw?
Would it be alright if we got to know that part a bit better?
What happens if you and I slow down? Does this part get quieter or louder?
This part is helping to protect you. What are its top three jobs right now?
How has this part shown up in the past?
When things get intense, what part kicks in to get you through the moment?
Where do you feel alarm in your body?
Would it be ok if we notice that emergency response? We don’t need to fix or change it.
Can we stay near this part? Let’s take a few steps back and look at it.
Co-regulate: Can we breathe together while we notice it? What would it take for you to feel safe right now?
How quickly does this part arrive? Is it instant, or is there a build-up?
What is it protecting you from feeling in your body? Panic? Grief?
When the room gets quiet, what comes up for you? Where do you feel it in your body?
Under all of the managing and coping, what feels most tender to you in this moment?
Would it be ok if we stay with this feeling through a few breaths?
What would help you feel more supported as we focus on this?
What does this part want you to know the most?
What does it need right now—a witness, permission to grieve, or comfort?
2) Relate to and work with the part
Relating to and working with the part reflects a deepening of the processes of unblending and cultivating self-leadership. Unblending creates space between the patient and their internal experiences; self-leadership uses that space wisely.
The goal is to respond to all parts with compassion; this allows protective parts to soften and increasingly trust the Self to lead. To help patients do this, clinicians can use the second three Fs of the 6-F mnemonic presented in Table 3: how does one Feel Toward the part, BeFriend the part, and what does the part Fear.
The goal is to help Maya work with and relate to the part most activated in the current moment. The strategies below explore what that might look like depending on which of Maya’s parts we are engaging with.
How does she
How do you feel about the part that is managing—gratitude, exhausted, annoyed, proud?
If you could approach it with curiosity, what would you want to learn?
What does this part want me to understand as your clinician?
What would help it trust that you can handle logistics and feelings?
What does the part
What is this part most worried you might feel?
Is this part trying to protect your family as well? What would you want them to know if it were safe?
How does she
Can we offer this part a little compassion for how hard it works to keep you safe?
Can you access any amount of gratitude for this part?
What does this part want me to do differently when it arrives?
What helps to calm down the fastest when this part arrives?
What does the part
What feeling is this part protecting you from? Could we feel that feeling for 10 seconds together?
What might happen if this part weren’t around?
How does she
If you could talk to this part, what would you say?
As we notice this tender place, what do you feel toward it?
How long have you been carrying this?
What does this part want for you?
What does the part
What is this part most afraid of?
What is it hoping for?
3) Track multiple parts
While IFS principles often guide us toward sustaining attention on one part at a time, clinicians may at times intentionally track multiple parts in the room in order to verbalize a patient’s inner conflict. This can be an especially powerful intervention in serious illness care, where ambivalence is often intensified. Verbalizing it in the room helps to externalize inner conflict, reduce shame, and mitigate urgency. This can help patients and clinicians recognize that no one part defines the whole. This differentiation can invite the Self back into leadership and help patients process and respond to serious illness in more values-aligned ways. In addition, it subtly reassures patients that you aren’t asking them to resolve this conflict immediately, but rather inviting them to understand it. 14
For Maya, this may include comments such as:
It sounds like there is a part of you that is determined to stay strong and keep everything together in your care. And perhaps there’s another part of you that feels overwhelmed or scared when thinking about how your cancer might impact your sons. Does that feel like it fits with your experience in any way?
I wonder if, after so many years as a nurse, a part of you copes by planning medical details, researching choices, and keeping control over this familiar realm. Perhaps there’s another part that feels much more scared or vulnerable when considering the uncertainty of your situation or witnessing other patients in similar situations.
I’m noticing how quickly you shift into problem-solving mode when we look toward the future. I wonder if that is driven by a part of you that wants to stay with the practical in order to protect you from overwhelm. I also wonder if maybe another part is quietly hoping for space to acknowledge how painful this all is.
When enacting these IFS-informed communication techniques, clinicians are far more effective when keyed into our own countertransference. Just as patients have protective parts that become activated in times of stress, clinicians may also experience activation of their own protective parts in response to how a patient presents. For example, we may notice Manager responses (e.g., defensiveness or over-explaining our care choices) when confronted with a patient’s anger, Firefighter inclinations (e.g., changing subjects or shortening visits) when faced with a patient’s helplessness, or activation of our own vulnerable Exiles (e.g., our own fears of loss or mortality) in the presence of a patient’s profound existential suffering. We may even notice our own internal conflict, with one part wanting to be fully present with a patient’s distress while another distances emotionally in an effort to remain grounded. Recognizing these internal reactions can help clinicians return to a more grounded stance of therapeutic presence. 15
Conclusion
All people have a unique inner world of protective parts, which work together to manage fear, uncertainty, and old emotional wounds. Under the stress of a serious illness, these parts can become rigid, polarized, and internally conflicted, which can manifest in behaviors of ambivalence, avoidance, urgent symptom focus, or intense control seeking. When caring for a patient showing signs of inner conflict, clinicians can use IFS-informed SIC strategies to discern which parts may be constraining the patient’s ability to live in accordance with deeply held values. In turn, clinicians can help patients relate more compassionately and productively to their internal parts. IFS-informed communication strategies can help soften reactivity and reduce the tension of inner conflict, thereby helping patients access their evolving values and priorities with greater flexibility. 11
Consent to Publish
All cases presented in this series are hypothetical composites developed for illustrative and educational purposes. They do not represent real patients, and therefore, consent to publish was not required.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.