
Abstract
Previous studies have concluded that exercise training is beneficial to patients on hemodialysis (HD). Results, however, have shown that differences in the type, intensity, and frequency of physical exercise lead to variability in its effects on physical functional performance and depression. Further research is thus warranted. Our aim was to evaluate the effects of aerobic exercise on physical functional performance and depression during HD. Using a pretest–posttest control group design, we recruited HD patients and nonrandomly assigned them to an exercise group (n = 13) that completed a 12-week aerobic exercise program during HD or a control group (n = 11) that did no exercise during HD. The primary outcome measures were physical functional performance, as evaluated by the 6-min walk test and the sit-to-stand test, and depression, as evaluated by the Beck Depression Inventory II. The secondary outcome measures were albumin and triglyceride levels and hematocrit. Results revealed significant between-group differences in physical functional performance and depression but not in albumin level, hematocrit, or triglyceride level. Findings suggest that exercise may play a critical role in physical functional performance and may decrease depression. Exercise should be encouraged and performed during HD in HD centers.
Keywords
According to the U.S. Renal Data System (2012), the incidence of end-stage renal disease (ESRD) continues to increase each year. Taiwan has more than 60,125 patients with ESRD and the highest prevalence of ESRD in the world. Hemodialysis (HD) is the principal form of renal replacement therapy for ESRD, and approximately 91% of ESRD patients receive maintenance HD (Taiwan Society of Nephrology, 2013). HD is typically prescribed to be performed 3 times per week, 3–6 hr per session, for the rest of a patient’s life or until successful kidney transplant has been performed (Cheema & Singh, 2005).
Muscle wasting, decreased visceral protein stores, and reduced physical functioning attributable to uremic myopathy and neuropathy have a significant impact on hospitalization and mortality rates among long-term HD patients (Kosmadakis et al., 2010). Muscle weakness and lack of energy are among the most common complaints of these patients (Storer, 2009). Causes of muscle weakness can include loss of muscle mass (atrophy) and reduced storage of protein in the body, which significantly affect mortality and hospitalization rates (Beddhu, Pappas, Ramkumar, & Samore, 2003). HD patients also have a high incidence of cardiovascular disease, and cardiovascular disease and related factors are the main cause of morbidity and mortality in these patients (Sarnak & Levey, 1999). Approximately two thirds of all patients with ESRD suffer from dyslipidemia (Liu & Rosner, 2006), a common risk factor for cardiovascular disease (Junyent et al., 2010), and it is the cause of death in nearly 50% of HD patients (Al Wakeel et al., 2002). In one study, 84.5% of HD patients had abnormal levels of triglycerides, and 82–92% had lower than normal HDL cholesterol levels prior to the initiation of exercise therapy (Gordon, McGrowder, Pena, Cabrera, & Lawrence-Wright, 2012). Management of dyslipidemia would reduce the incidence of cardiovascular disease and mortality in HD patients.
The most commonly observed psychological problem in HD patients is depression, with reported incidence ranging from 27.9% to 40.2% (Keskin & Engin, 2011; Ugurlu, Bastug, Cevirme, & Uysal, 2012). Depression is, however, underrecognized and undertreated in this patient population, which markedly increases the mortality rate (Hedayati et al., 2008). Hospitalization and mortality rates within the first year of HD for patients with depression were more than twice than those of patients without depression. In a previous study, researchers found a significant positive correlation between depression and death in patients receiving chronic HD therapy (Troidle et al., 2003).
A sedentary lifestyle is common in HD patients because their physical capabilities and levels of physical fitness and function are markedly reduced due to chronic renal failure. More than half of HD patients are considered mildly disabled based on tests of physical functional performance (Jhu, Kuo, & Tseng, 2011). Inactivity in HD patients has been associated with increased obesity and mortality (Kosmadakis et al., 2010). Exercise programs among HD patients have shown promise both for reducing depression and increasing physical functional performance (Eriksson & Gard, 2011). Dialysis exercise programs have resulted in a significant increase in aerobic capacity and peak oxygen uptake and reduced cardiovascular risk (Heiwe & Jacobson, 2011) and depression (Ouzouni, Kouidi, Sioulis, Grekas, & Deligiannis, 2009). In one previous study, investigators found that a brief period of exercise could affect aerobic capacity in patients receiving maintenance HD; however, aerobic capacity had little relationship to physical symptoms or depression after a 1-month follow-up (Carmack et al., 1995). The authors concluded that insufficient training duration and the limited number of interventions might account for the lack of effect on physical and psychological variables. In contrast, several studies have revealed a relationship between the two types of variables. A 10-month intradialytic exercise training program (60–90 min per session) improved functional capacity and depression in HD patients (Ouzouni et al., 2009). A 24-week intradialytic resistance training program (25 min per session) resulted in improved physical function, physical performance, and exercise capacity among HD patients (Segura-Ortí, Kouidi, & Lisón, 2009). A 12-week aerobic exercise training program during HD not only increased physical function but also contributed to controlling blood pressure and anemia (Reboredo et al., 2010). An 8-week aerobic exercise and resistance training program during HD affected serum creatinine level but not weight or hemoglobin level (Afshar, Sheggarfy, Shavandi, & Sanavi, 2010). A 12-month run-in control period with a 6-month exercise program for HD patients demonstrated that physical exercise could safely increase physical performance but had no effect on laboratory variables, including hemoglobin, albumin, triglycerides, cholesterol, calcium, and phosphate (Bulckaen et al., 2011). A 2-month aerobic exercise program (15 min per day, 3 times a week) significantly improved serum phosphate and potassium levels, but not serum calcium and hemoglobin levels, among HD patients (Makhlough, llali, Mohseni, & Shahmohammadi, 2012). Finally, seven of the eight studies examined in a systematic review revealed positive effects of exercise on depression, but the authors concluded that more highly controlled studies on the effect of physical exercise on depression, focusing on the type, intensity, and frequency of exercise are still needed (Eriksson & Gard, 2011).
The wide variation in type, intensity, and frequency of exercise explored in these previous studies led to differences in the findings on the effects of exercise on biochemical indicators and depression. Further study to determine the most effective exercise program for these patients is, therefore, warranted. In this study, we aimed to evaluate the effects of an aerobic exercise program on physical functional performance and depression in patients undergoing HD.
Method
Research Design and Sample
We used a quasi-experimental pretest and posttest, control group design (Figure 1). ESRD outpatients were recruited from an HD center in an 872-bed northern regional hospital in Taiwan. Inclusion criteria were being greater than 20 years of age, having received maintenance HD for more than 6 months, undergoing dialysis treatment 3 times per week, and having arteriovenous grafts or native fistulas in the upper extremity. Exclusion criteria were severe muscle weakness or skeletal deformity, malignant arrhythmia, unstable angina, hospitalization during the study, and uncontrolled blood pressure. Participants were nonrandomly assigned to one of the two groups based on the days they came for HD. Patients who came for HD on Mondays, Wednesdays, and Fridays were assigned to the experimental group and received the 12-week aerobic exercise program. Patients who came for HD on Tuesdays, Thursdays, and Saturdays were assigned to the control group and received routine dialysis care only.
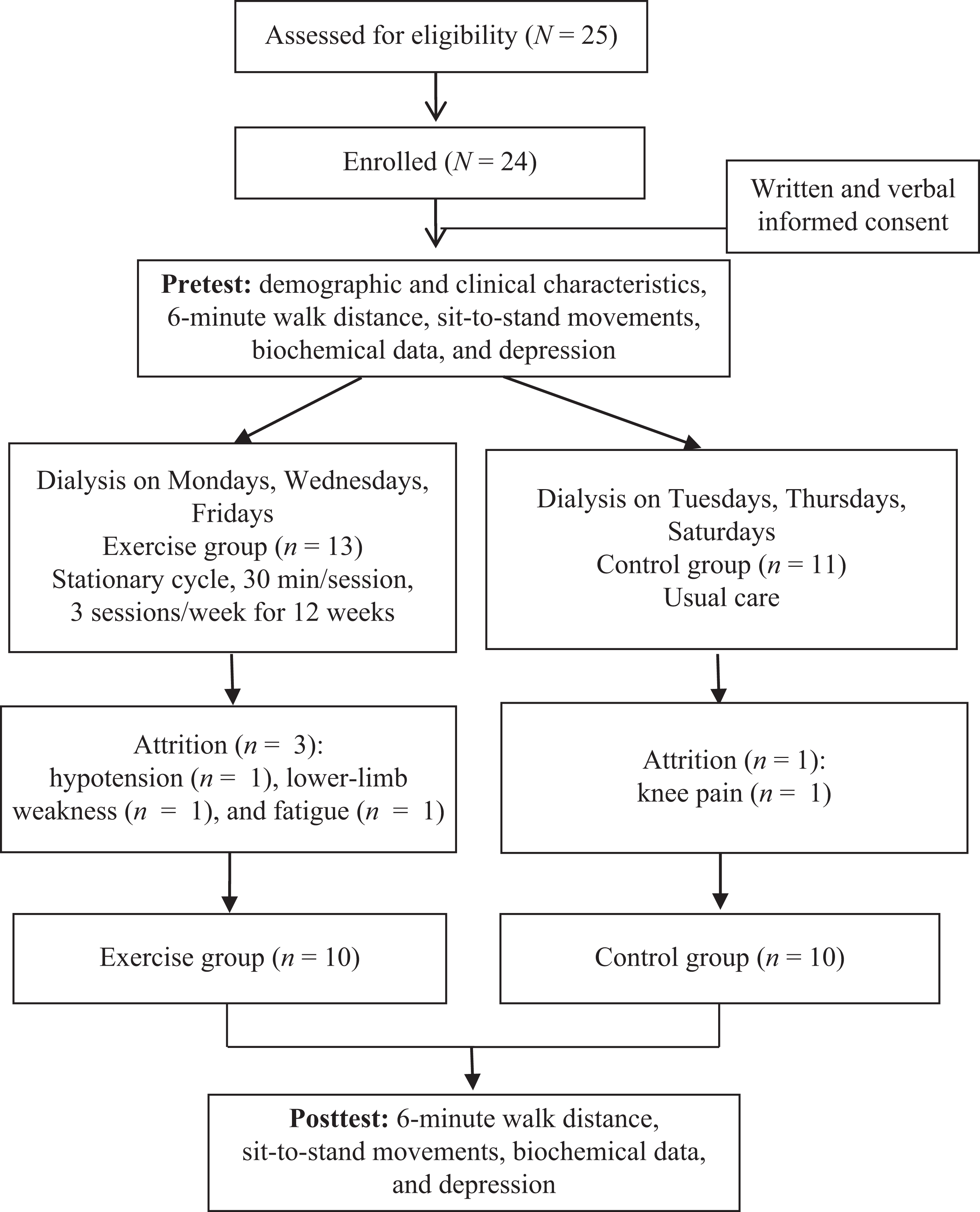
Study design and participant flowchart.
Aerobic Exercise Program
Participants completed the 30-min aerobic exercise sessions during the first 2 hr of each dialysis session, 3 times per week for 12 weeks, using a horizontal electromagnetic cycle ergometer (Medical Exercise Peddler 3000, Medi-Bike, Taiwan). Each exercise session consisted of three phases: warm up, conditioning, and cool down. Before the start of each exercise session, we placed a blood pressure cuff and heart rate and SpO2 monitors on participants and left them on throughout the session. HD physicians also assessed the participant’s clinical condition at this time (i.e., shortness of breath, cardiovascular symptoms, blood pressure, and heart rate). Once the session began, the research assistant measured the participant’s blood pressure, heart rate (Criticare, Systems Inc., Waukesha, WI) and SpO2 (Dash 2000, GE Healthcare, Wisconsin, U.S.A.) electronically every 5–10 min for safety. Participants were excluded from the exercise session if their systolic blood pressure was higher than 180 mmHg, diastolic blood pressure was higher than 95 mmHg, heartbeat was below 60 beats/min, or SpO2 was less than 88%.
The warm-up phase consisted of 5 min of stretching of the lower limbs and low-load aerobic exercise at an intensity of 8–9 of 20 on the Borg Rate of Perceived Exertion (RPE) scale. The conditioning phase included 20 min of aerobic exercise. Intensity was prescribed on the basis of perceived exertion, exercise heart rate, and blood pressure. The exercise participants were requested to exercise at an RPE between 11 (fairly light) and 13 (somewhat hard; Borg, 1970), and intensity was monitored every 5 min. Participants were encouraged to increase the rate of rotation if the Borg scale value was less than 11 and decrease the rate of rotation if the value was greater than 13. During the cooldown period, participants performed light exercise with no load at an intensity of 8–9 on the RPE scale.
The criteria considered for interrupting the aerobic exercise session included intense physical exhaustion, chest pain, dyspnea, dizziness, significant changes in heart rate or blood pressure, or fatigue of the lower limbs. Participants were included in the analyses if they completed at least 10 of the 12 sessions out of any consecutive 4-week period during the 12-week aerobic exercise program.
Outcome Measures
Demographic and clinical characteristics
We collected age, gender, marital status, education level, symptoms of HD, and reasons for not exercising from participants. From the medical record, we collected cause of kidney failure and HD duration.
Physical functional performance
The 6-min walk test (6MWT) is frequently used to measure physical function in HD patients (Reboredo et al., 2010). In this study, participants performed the 6MWT along a 20-m long and 2-m wide walkway in a quiet hospital corridor. We placed markers every 5 m along the length of the corridor. Participants were instructed to walk as far as they could in 6 min. They were allowed to stop and rest if needed but were instructed to resume walking when they felt able to do so. Reasons for immediately stopping a 6MWT included chest pain, dyspnea, leg cramp, or pale appearance. In HD patients, the 6MWT value has been reported to be highly positively correlated with VO2 peak during the cardiopulmonary test (Reboredo et al., 2007).
We used the sit-to-stand test (STS-60) as an indirect measure of lower limb muscle strength and endurance (McIntyre et al., 2006). The STS-60 test measures the number of times a participant can get up from a chair and sit down again during a 60-s period. The STS-60 is a feasible way to measure changes in physical function resulting from exercise (Segura-Ortí et al., 2009).
Depression
We used a Chinese version of the Beck Depression Inventory II (C-BDI-II; Beck, Steer, & Brown, 1996/2000) to measure severity of depression. The C-BDI-II is a 21-item self-administered instrument. Respondents rate each item on a 4-point scale ranging from 0 to 3. The severity of depression is determined by summing the ratings: Total score ranges from 0 to 63, with scores of 0–13 indicating minimal depression, 14–19 indicating mild depression, 20–28 indicating moderate depression, and 29–63 indicating severe or major depression (Lu, Che, Chang, & Shen, 2002). Cronbach’s α, a measure of internal consistency reliability, was .91 for the BDI-II (Beck, Steer, Ball, & Ranieri, 1996) and .93 in this study.
Biochemical data
Albumin level (normal > 4.0 g/dl), hematocrit (male: 36–50%; female: 34–47%), and triglyceride level (normal < 200 mg/dl) were measured before the start of and after the completion of the entire aerobic exercise program. We obtained 1 cc of blood for the hematocrit test and 3–4 cc for the biochemical test as patients underwent HD therapy. Blood samples were processed immediately and analyzed by using an XE-5000 automated hematology analyzer (Sysmex UK and SIEMENS) at the central laboratory of the study hospital (B17D0B043).
Procedure
The institutional review board of the study granted hospital approval for the conduct of this study (CTH-100-3-5-44). We obtained written informed consent from all participants after they received a full explanation of the study. Participants were allowed to withdraw themselves from the study at any time without affecting their care. All data collected remained confidential throughout the study and were used in the analyses. The nurse researcher (SL) on the research team administered the aerobic exercise program to all participants after receiving training on the protocol by another member (YM) of the research team. All participants started their individual exercise programs at the beginning of the month. The nurse researcher collected the outcome measures before the start of and after the end of the 12-week exercise program. Measures were completed at the HD clinic before the start of HD treatment.
Data Analysis
IBM SPSS 20.0 for Windows was used to analyze data. Demographic data and medical history data were analyzed using descriptive statistics. The χ2 test, Fisher’s exact test, and Mann–Whitney U test were used to verify homogeneity between groups. The between-group differences in the effects of exercise were analyzed using paired and independent t-tests.
Results
Demographic and Clinical Characteristics
Of the 25 patients who were eligible to participate, 24 signed the informed consent form and were included in the study. Of these, four dropped out for the following reasons: knee pain (n = 1), hypotension (n = 1), lower limb weakness (n = 1), and fatigue (n = 1). In all, 20 participants (83.33% of the initial number; 9 female and 11 male; mean age, 38.8 ± 8.8 years [range 21–52 years]) completed the study, with 10 adhering to and completing the aerobic exercise program and 10 completing the study in the control group. Table 1 presents participants’ demographic and clinical characteristics. All characteristics (p > .05) except age (p = .002, exercise group significantly older) were similar between groups.
Demographic and Clinical Characteristics of Hemodialysis Patients Who Completed the Study, by Study Group.
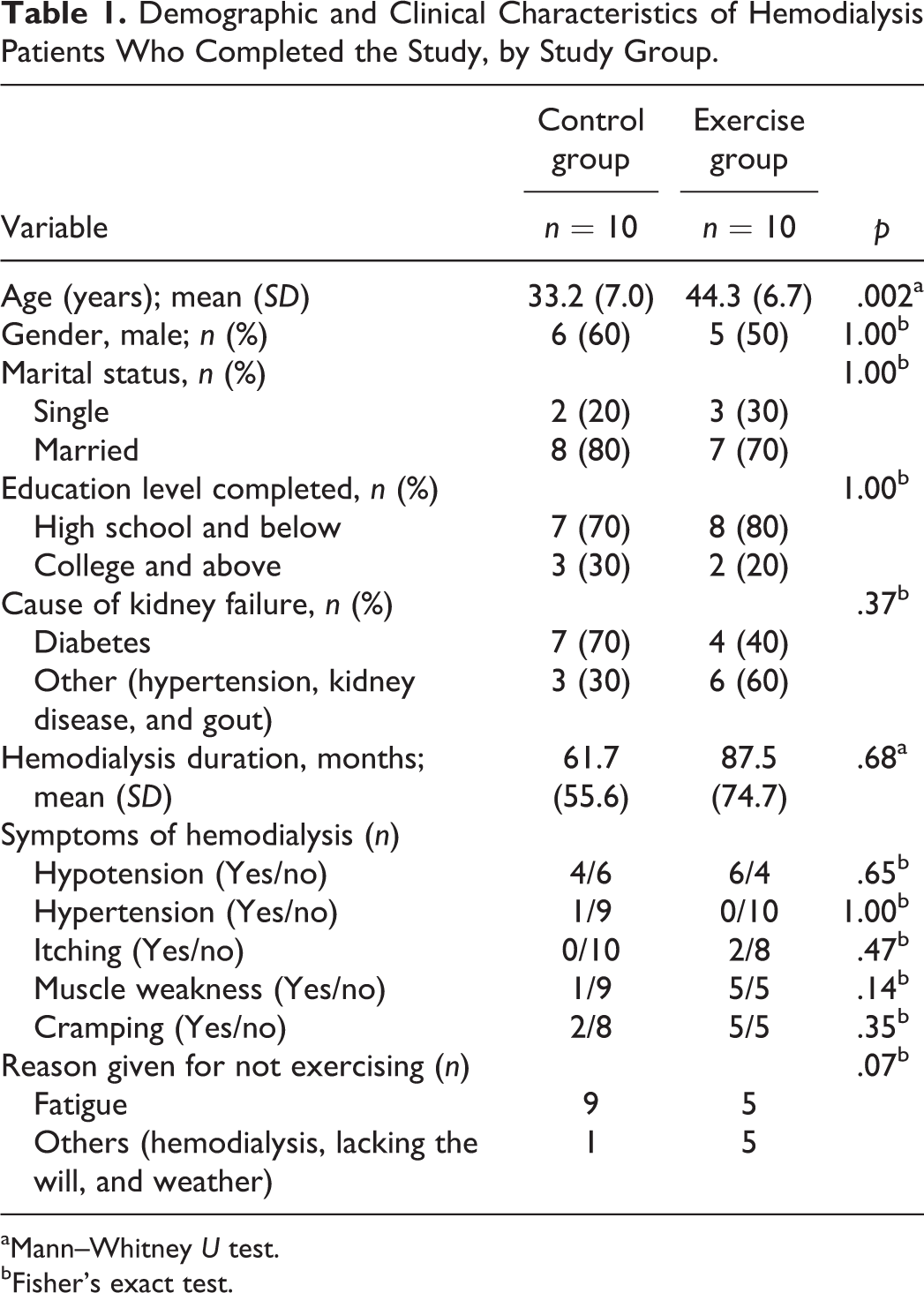
aMann–Whitney U test. bFisher’s exact test.
Physical Functional Performance
As shown in Table 2, there were no between-group differences in the pretest 6MWT (t = −1.98, p = .06) or STS-60 (t = −0.47, p = .64). We did, however, observe significant between-group differences in the pre–post changes for both the 6MWT (t = 4.20, p = .002) and the STS-60 (t = 3.37, p = .007). Analysis revealed a significant positive correlation between the 6MWT distance and number of STS-60 repetitions during pretest (r = –.710; p < .001) and posttest (r = –.789; p < .001).
Outcome Assessment at Baseline and After 12 Weeks of Exercise Training.
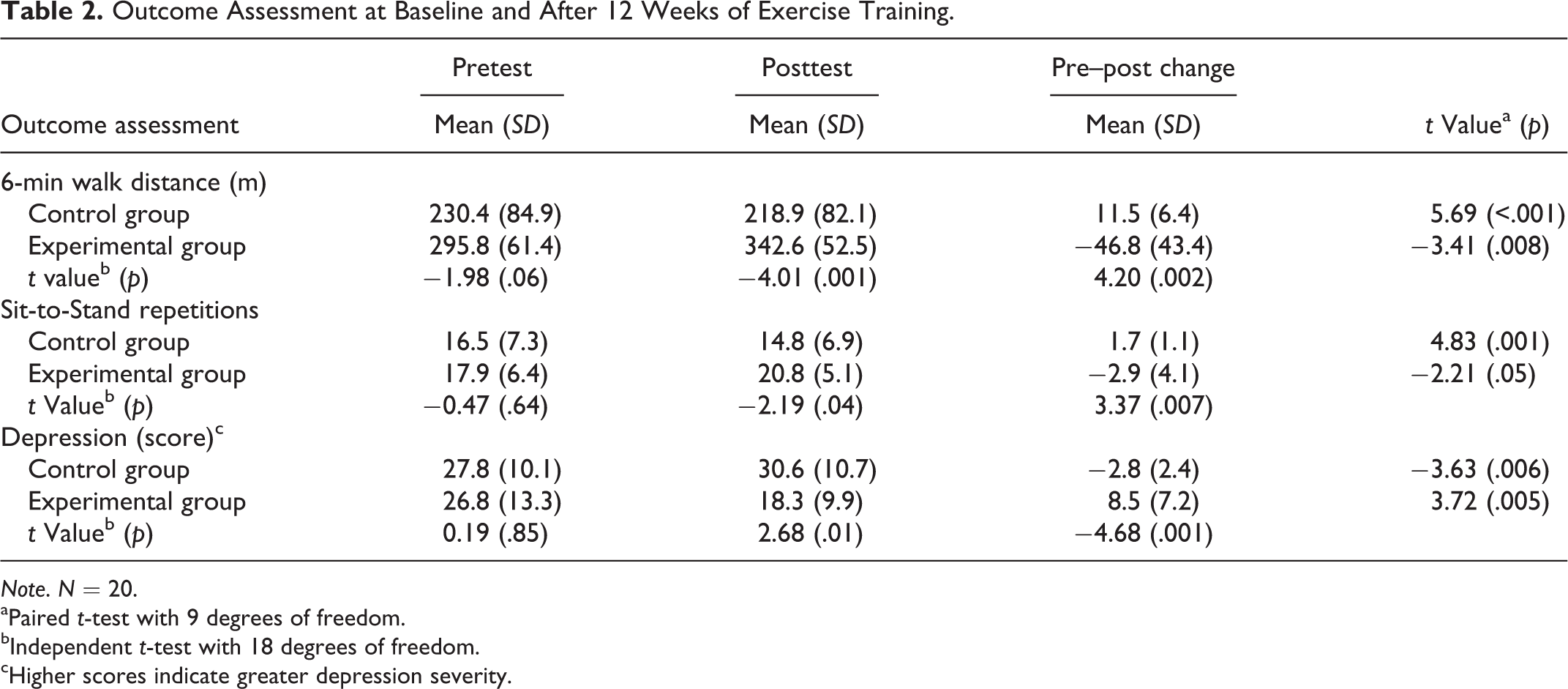
Note. N = 20. aPaired t-test with 9 degrees of freedom. bIndependent t-test with 18 degrees of freedom. cHigher scores indicate greater depression severity.
Depression
Before the exercise program began, BDI-II scores indicated normal or minimal depression in three patients (15%), mild depression in one patient (5%), moderate depression in seven patients (35%), and major depression in nine patients (45%). Table 2 shows that the mean pretest depression scores for both the control and exercise groups indicated moderate depression, with no between-group difference in depression score (t = 0.19; p = .85). After the exercise program ended, mean depression scores indicated major depression in the control group and mild depression in the experimental group, and the between-group difference in pre–post change in depression scores was significant (t = −4.68; p = .001).
Biochemical Data
The mean albumin level, hematocrit, and triglyceride level were, respectively, 3.45 ± 0.50 g/dl, 30.48 ± 2.17%, and 149.70 ± 83.14 mg/dl for the control group and 3.45 ± 0.28 g/dl, 31.54 ± 3.02%, and 161.40 ± 133.25 mg/dl for the exercise group before the start of the exercise program; and 3.46 ± 0.48 g/dl, 29.90 ± 3.61%, and 154.50 ± 80.51 mg/dl for the control group and 3.52 ± 0.28 g/dl, 32.70 ± 3.67%, and 161.30 ± 86.11 mg/dl for the exercise group after the program ended. There were no significant between-group differences at pretest in albumin level (p = .68), hematocrit (p = .53), or triglyceride level (p = .97) between the two groups using the Mann–Whitney U test nor were there significant between-group differences in the pre–post changes for the albumin level (p = .44), hematocrit (p = .48), or triglyceride level (p = .85)
Discussion
In this study, we determined that the 12-week aerobic exercise program improved physical functional performance and reduced depression in HD patients during the short-term intervention. First, the aerobic exercise program significantly increased 6MWT distance by 46.8 m; in contrast, the distance significantly decreased for the control group by 11.5 m. This finding is consistent with those of other studies that have revealed that a 3-month aerobic exercise program improved 6MWT distance by up to 46.2–48.0 m (Reboredo et al., 2010; Segura-Ortí et al., 2009). In a separate study, a 6-month walking program resulted in an increase in 6MWT distance of up to 43.0 m (Malagoni et al., 2008). From these findings, we can conclude that aerobic functional performance among HD patients. Similarly, the exercise program in this study increased the mean number of sit-to-stand repetitions by 2.9, as compared to the control group, in which the number of repetitions decreased by 1.7. Our finding supports that of a prior study in which an individualized rehabilitation program of exercise with RPE intensity of 13–15 significantly increased sit-to-stand repetitions by 5.14 among patients with chronic kidney disease (Greenwood et al., 2012). The RPE intensity used by Greenwood et al. was the same as the intensity we used in this study. The STS-60 test is an indicator of physical function that refers to muscle strength, performance, and endurance. Thus, as intensity increases, the physical functional performance improves.
Second, our 12-week aerobic exercise program significantly reduced depression scores by 31.7%, whereas these scores significantly increased by 10% in the control group. This result is similar to the 30.5–39.4% decrease in depression that researchers have noted after testing other exercise training programs in similar populations (Greenwood et al., 2012; Ouzouni, et al. 2009). In contrast, Carmack et al. (1995) observed no decrease in depression scores after a 10-week exercise training program in HD patients; however, the drop-out rate of this study was high (i.e., 56.3%), which may be a factor in the differences between the results.
Finally, the 12-week aerobic exercise program in this study did not significantly improve serum albumin level, hematocrit, or triglyceride level. This result is consistent with findings from other studies that assessed the effects of an 8-week intradialytic exercise program (Afshar et al., 2010; Makhlough et al., 2012). In contrast, Gordon, McGrowder, Pena, Cabrera, and Lawrence-Wright (2012) found that a 4-month Hatha yoga training program significantly reduced the triglyceride level among ESRD patients receiving HD. Though the length and type of exercise are known to affect outcomes, the authors did not clearly state the frequency and intensity of exercise in their report, so it is difficult to compare the interventions between studies. Reboredo et al. (2010) investigated the effects of a 12-week program of intradialytic aerobic exercise with three sessions per week lasting 30 min each (Borg scale RPE of 12–13), using a one-group pretest design. The authors found that levels of triglycerides and low-density lipoprotein cholesterol increased markedly but stayed within the normal ranges, a finding that they attributed to increased appetite after exercise. Many additional factors can contribute to a lack of effectiveness of exercise in terms of improving these biochemical markers, including gender, nutritional status, uncontrolled secondary hyperparathyroidism, dialysis membrane bioincompatibility, and drug consumption (Afshar et al., 2010). Future studies should control for these factors.
Despite the well-established health benefits of exercise, HD patients rarely or reluctantly exercise on nondialysis days (Jang & Kim, 2009). A structured environment and strict patient monitoring are key components to improving compliance with an exercise program. The most effective time to schedule an exercise intervention, therefore, is during HD, primarily due to a higher level of compliance (Kouidi, 2004) and a greater ability to control risk (Daul, Schafers, Daul, & Philipp, 2004). The drop-out rate of this study was 16.7% due to hypotension, knee pain, lower limb weakness, and fatigue caused by dialysis. None of these complaints were related to the aerobic exercise program and no other exercise-related adverse events occurred during the study. Health care workers were present at all times during HD, and patient safety was strictly monitored. We also monitored the incidence of hypotension caused by dehydration. These factors motivated the patients to comply with and complete the exercise program.
Limitations and Recommendations for Future Research
This study has some limitations. First, we did not randomly assign participants to groups, which may have led to selection bias. Although the participants were not informed of their study group in order to avoid bias, because all participants stayed in the same unit during HD, patient-to-patient interaction could not be completely avoided. Second, the HD patients in this study do not represent all HD patients in Taiwan; thus, the results cannot be generalized. Third, the sample size in this study was small. Fourth, we did not provide any comparable attention for the control group. Fifth, the standard deviations for duration of HD were very large, which may have affected the outcomes of physical functional performance and depression. Finally, the improvements in physical functional performance and depression were measured as a short-term rather than a long-term effect. The long-term effects of the program remain unknown. Broader studies with larger sample sizes, in various medical settings, and different load (including no load) exercise programs and examining the longitudinal effects of this intervention are recommended. In addition, in order to increase the motivation of patients to exercise, researchers should consider active participation of family members.
Though the exercise group was significantly older than the control group in this study, we do not consider age to have been a likely confounding factor. According to Bennett et al. (2010), age is no barrier to exercise on HD. The dialysis medical staff often views HD patients as being too old to exercise (Painter, Carlson, Carey, Myll, & Paul, 2004). However, Bennett and colleagues found a common theme in their review that, though age is a determinant for physical performance, elderly HD patients respond well to some form of physical activity or exercise and there is some evidence that older patients respond better to exercise programs than younger.
Conclusion
Very few HD centers in Taiwan provide exercise programs to improve patients’ physical functional performance and psychological health. This study established that a pragmatically constructed, intradialytic program of aerobic exercise can substantially improve both physical function and psychological well-being for a wide range of HD patients. Therefore, HD patients should be encouraged to exercise during HD treatment, and exercise programs should be implemented in HD centers.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was sponsored by the Cardinal Tien Hospital (CTH-101-1-2A13) and Teh-Tzer Study Group for Human Medical Research Foundation (B1001055).