
Abstract
Background:
Hyperphosphatemia in end-stage renal disease patients is prevalent and associated with increasing cardiac mortality. Restricting dietary phosphate intake is a key element in controlling hyperphosphatemia, but most patients fail due to lack of knowledge and sustainability. In this study, we aimed to examine whether incorporating a smartphone application (APP) into a multidisciplinary caring system can decrease the prevalence of hyperphosphatemia in hemodialysis patients.
Methods:
We designed a quasi-experimental study to enroll patients undergoing regular hemodialysis and assigned them to receive APP-assisted caring program (ACP group, n = 30) or standard education caring program (SCP group, n = 30). Both caring programs targeting dietary phosphate control were administered. Patients’ general characteristics, self-care efficacy scales, knowledge test of phosphate control, and results of monthly blood biochemistry were analyzed.
Findings:
Knowledge of diet phosphate control and self-care efficacy were significantly higher in the ACP group. Notably, the knowledge improvement was higher in patients aged over 60 years. Compared to the SCP group, the percentage of patients with successful hyperphosphatemia control was significantly higher in the ACP group (p = 0.0398).
Conclusion:
The APP-assisted caring program benefits patients with regular hemodialysis to achieve better dietary phosphate control without compromising proper protein intake.
Patients with end-stage renal disease (ESRD) are a critical health burden worldwide, particularly in Taiwan (Saran et al., 2019). Hyperphosphatemia is prevalent in patients with ESRD and has been shown to be associated with several critical complications, such as secondary hyperparathyroidism, renal osteodystrophy, and even cardiovascular diseases (Ganesh et al., 2001; Block et al., 1998; Slatopolsky & Delmez, 1994). Even though dialysis in any form removes a substantial amount of phosphate, it is often not sufficient, and protein loss is a concern (Delmez et al., 1982; Gotch et al., 2003; Minutolo et al., 2002). Phosphate binders, both non-calcium and calcium-based, have been shown to achieve an average control rate of 64% to 66% in patients with ESRD (Joy & Finn, 2003; Xu et al., 2013), but the real-world effectiveness of phosphate control with these agents is limited due to poor gastrointestinal tolerance (Fissell et al., 2016). The dietary restriction of phosphate remains a fundamental recommendation in both the Kidney Disease Improving Global Outcomes (KDIGO) and Kidney Disease Outcomes Quality Initiative (K/DOQI) guidelines (Coladonato, 2005; Isakova et al., 2017; Outcomes, 2017). However, information on phosphate content in various kinds of food and associated additives is overwhelming and difficult to deliver timely to patients, making it challenging for patients to successfully restrict phosphate in their diets.
With advances in information technology and the widespread use of smartphones, an increasing number of mobile health applications (APPs) and programs are being developed to promote self-management for chronic diseases. Connelly et al. (2012) developed a personal digital assistant APP with visual interfaces, barcode scanning, and voice recording to assist hemodialysis patients with varying levels of literacy to track their diet and further change their behavior. Ong et al. (2016) designed a smartphone-based self-management system that not only empowered chronic kidney disease patients to engage in self-care, but also resulted in blood pressure reductions, with 80% of the patients self-monitoring their blood pressure regularly. However, it is not easy to find a mobile APP that meets the expectations of both the clinician and the patient. Lambert and colleagues evaluated 21 renal diet-related mobile APPs in Australia and found that over half of them did not contain accurate, evidence-based information (Lambert et al., 2017). The general lack of quality and poor upkeep of these health-related mobile APPs should not be surprising because most of them were free to download and created by individual developers rather than by large health information groups/companies or universities (Singh et al., 2019). Furthermore, several studies have shown that positive and personal feedback are two of the key elements for successful diet control and behavioral change (Khaylis et al., 2010).
In this study, we investigated the effects of an APP-assisted caring program that included APP-assisted timely information and individually tailored feedback on the effects of serum phosphate control in ESRD patients in Taipei, Taiwan.
Materials and Methods
Study Design and Patients
This quasi-experimental study was conducted from June 2018 to August 2018 at Tri-Service General Hospital in Taipei, Taiwan. The study protocol was reviewed and approved by the Institutional Review Board of the Tri-Service General Hospital, and the informed consent was signed by all participants. Patients with a hemodialysis vintage of more than 3 months were screened. Inclusion criteria were as follows: aged between 30 and 70 years with a serum phosphate level ≥ 5.5 mg/dL for 3 consecutive months. Patients who were unable to use smartphones properly or upload dietary records or refused to receive counseling or join the online group discussions were excluded. The patients’ group assignments were based on the participants’ choices. Patients who chose to join the APP-assisted caring program (ACP) group received personal instruction on how to install the mobile APP on their smartphones and how to use them. Patients who chose the standard caring program (SCP) received education in a conventional manner. The SCP was provided by the dialysis charge nurses in person and included the following: the interpretation of monthly biochemistry results (including hemoglobin, electrolytes, phosphate, and albumin levels), dietary counseling, evaluation of oral phosphate-binder compliance and adherence, and patient education fact sheets or folding cards as enhancements. Patients were requested to repeat the essential information and sign their personal education records at the end of each education session. Group education regarding various topics was held quarterly.
All patients’ blood biochemistry results were collected monthly. A questionnaire assessment regarding knowledge of phosphate control and a self-efficacy scale were completed at the end of the study. All personal information was kept strictly confidential and anonymous, with access restricted at all times only to the principal investigator or to the research staff directly involved.
Development of Smartphone Application for Phosphate Control
The ACP was created by a tightly integrated multidisciplinary medical team, with the aim of shortening the knowledge gap between the patients and the overwhelming information on food content. We used the Taiwan Food Nutrition Database, which is owned and maintained by the Food and Drug Administration of the Ministry of Health and Welfare of Taiwan (https://consumer.fda.gov.tw/Food/TFND.aspx?nodeID= 178; Taiwan Food Nutrition Database ), to build the smartphone-based APP. To enhance accessibility, this mobile APP allowed users to search for items or food additives by their formal or common names in Mandarin or by pictures. We also simplified portion size estimation. The results were translated into an easy-to-understand calculation, the health score, based on the phosphate-to-protein ratio (Figure 1). The health score of each patient was recorded in the APP, and a weekly or monthly summary was provided. In addition, the APP also provided users with useful recipes and cooking tips based on his/her record and food search results. Individual participants’ food records were tracked and evaluated by our care team and used to provide tailored feedback and to adjust the dietary plan.
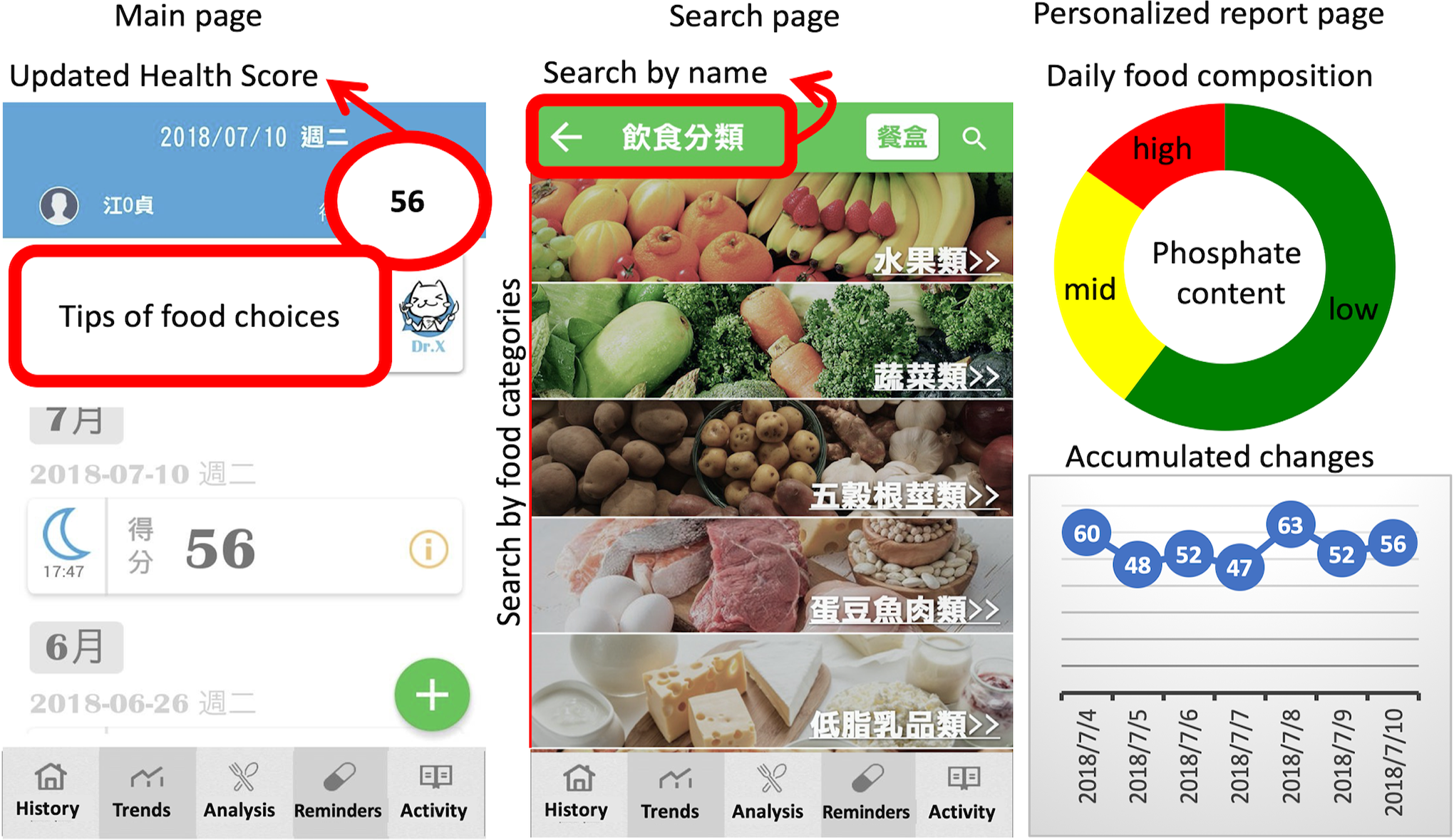
Features of phosphate control smartphone application.
Self-Efficacy and Knowledge Assessment
We evaluated the patients’ self-motivation and awareness of dietary phosphate control using a self-efficacy scale and knowledge tests. The self-efficacy scale was developed based on 3 existing chronic disease self-management scales: the Chinese version of the Diabetes Management Self-Efficacy Scale (C-DMSES; Vivienne Wu et al., 2008), the Chronic Kidney Disease Patient Self-Efficacy Scale (Lin et al., 2012), and the Asthma Patients Self-Efficacy Scale. Briefly, the scale we developed included basic demographic data that influence self-care efficacy, diet control, medicine compliance, problem-solving, and social support. After a multidisciplinary team (including the hemodialysis center chief, nephrologists, nephrology dietitians, senior nurses with expertise in patient education, and medical affairs consultants) reviewed the scale for expert validity assessment, the content validity index was found to be between 0.79 and 1.0, with an average of 0.91. The pretest was carried out on 10 chronic dialysis patients after approval by the Institutional Review Board, and a Cronbach’s α coefficient of 0.89 indicated excellent internal consistency.
Knowledge about dietary phosphate control was assessed by the same research staff using a questionnaire comprised of 3 parts, which involved identifying (1) food containing high-phosphate, (2) side effects of hyperphosphatemia, and (3) the proper use of oral phosphate-binders. Expert validity and face validity were confirmed after it was reviewed by the multidisciplinary team. A Kuder-Richardson Formula 20 (KR20) of 0.85, an average difficulty of 0.67 (0.5–0.98), and a discrimination power of 0.5 (0.3–0.9) indicated this questionnaire had excellent reliability, appropriate difficulty, and good discrimination power.
Statistical Analysis
The sample size for this study was calculated to achieve a 30% improvement compared to the control group. We anticipated a sample size of 58 patients to have an 80% chance of detection, at a significant level of 5% (Enderlein, 1985). Changes in biochemistry values were calculated by subtracting the first month’s value from the final month’s value, then dividing that by the first month’s value, in milligrams per deciliter (mg/dL). From baseline, a change in serum phosphate (or albumin) level of more than the mean plus 1 standard deviation (SD) or less than the mean minus 1 SD was defined as an increase or decrease, respectively. A change from baseline within the mean ± 1 SD was defined as stable. Continuous variables were reported as the mean ± SD and compared using the Student’s t-test (two-tailed). Categorical data were reported as numbers (%) and compared using the χ2 test. The interactions between the knowledge test and categorical variables were analyzed using the regression model and expressed as β values (95% confidence interval [CI]). A p-value < 0.05 was considered statistically significant. All statistical analyses were performed using IBM SPSS Statistics for Windows, Version 22.0 (Armonk, NY, USA).
Results
Patients’ Baseline Characteristics
From June to August 2018, 65 patients with regular hemodialysis were enrolled. Five patients dropped out of the study due to death from an unrelated cause (n = 3), transfer to another hospital (n = 1), and kidney transplantation (n = 1). Sixty patients were assigned to either the ACP (n = 30) or the SCP (n = 30) group. None of the general characteristics were statistically different between the groups, except there were more males and more patients with hemodialysis vintage ≤ 5 years in the ACP group compared to the SCP group (Table 1).
Baseline Characteristics.
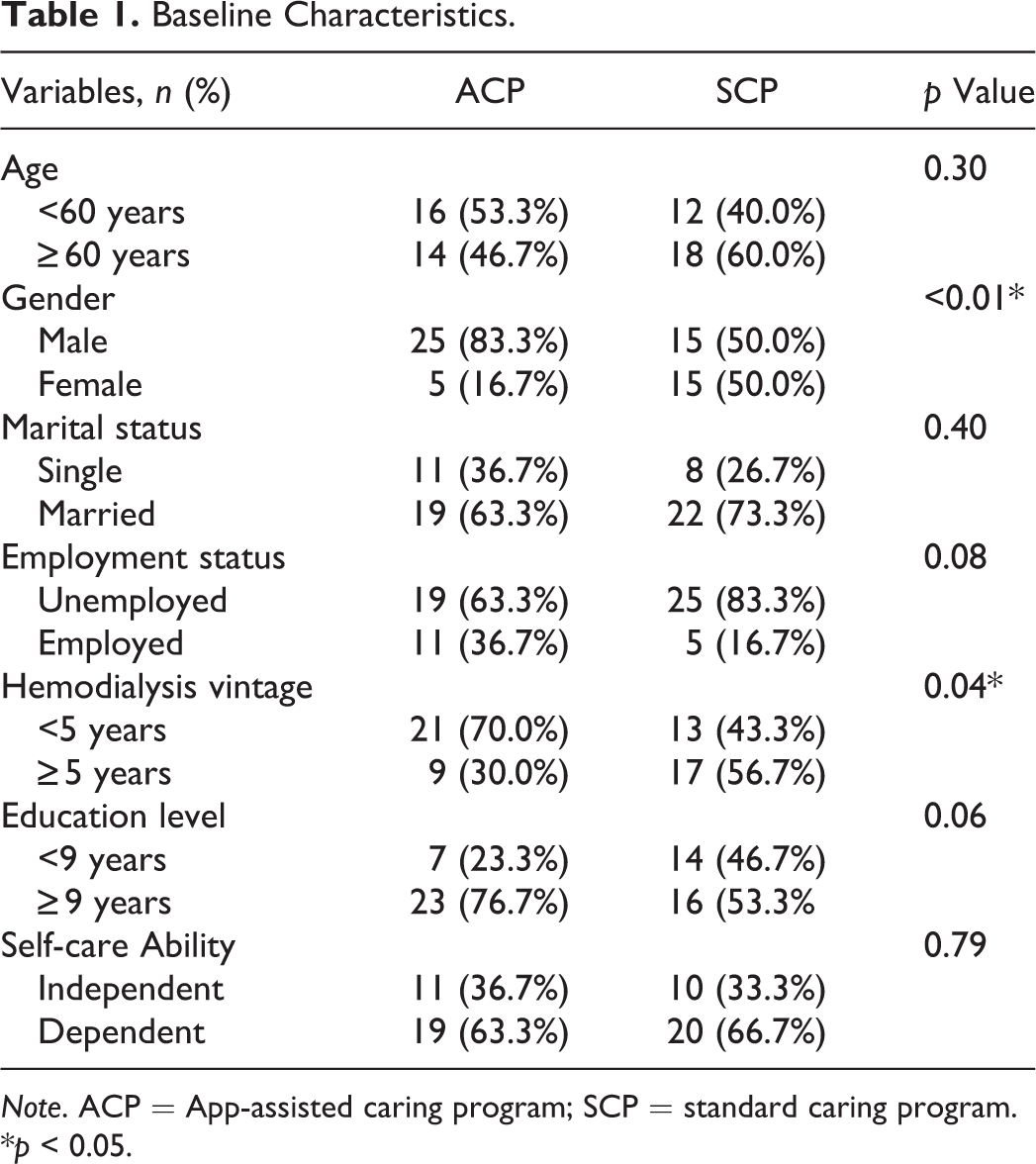
Note. ACP = App-assisted caring program; SCP = standard caring program.
*p < 0.05.
Self-Efficacy and Knowledge Assessments
Patients’ self-care and knowledge of dietary phosphate control were evaluated using the self-efficacy scale and knowledge tests at the end of the study. In both measurements, patients in the ACP group performed significantly better (Table 2). Differences in knowledge and self-efficacy were not significant according to sex or hemodialysis vintage. We further examined the interactions between baseline variables and ACP effectiveness using a linear model. We only found an interaction between age and the ACP intervention. Notably, the β (95% CI) of patients aged over 60 years was 16.39 (7.40–25.37), suggesting that the benefit of ACP was significant for patients aged over 60 years (Table 3).
Serum Phosphate, Albumin, Knowledge Test and Self-Care Efficacy Questionnaire Results Across Intervention Groups.
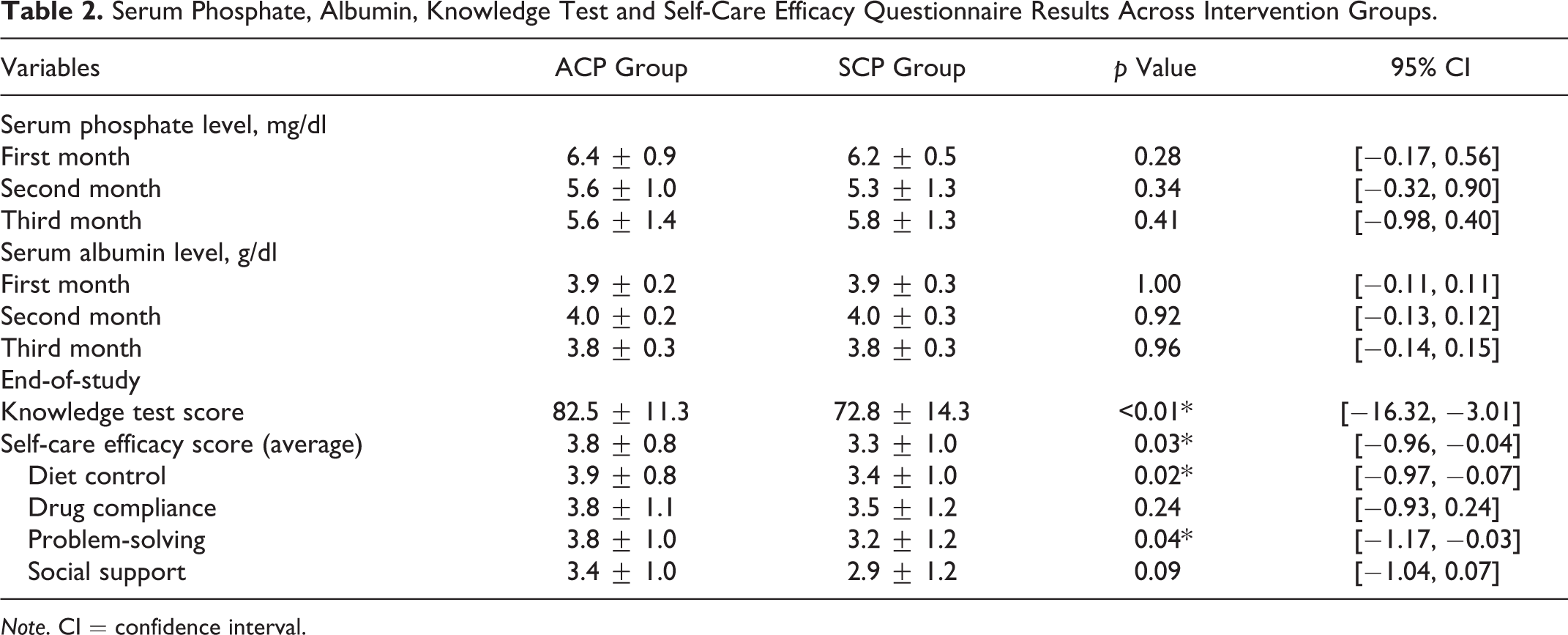
Note. CI = confidence interval.
Interactions Between Knowledge Test and Categorical Variables.
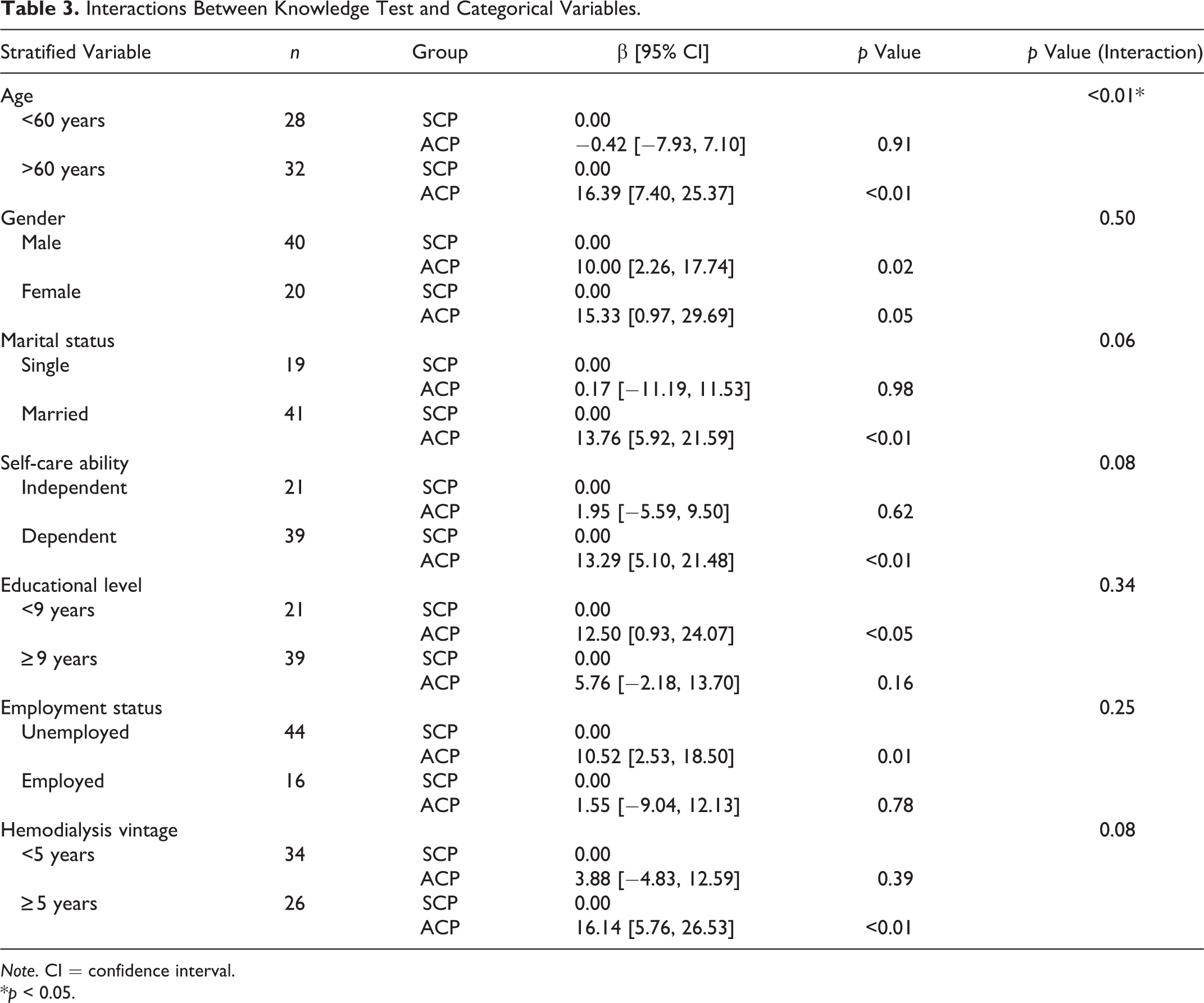
Note. CI = confidence interval.
*p < 0.05.
Changes in Serum Phosphate and Albumin Levels
There was no difference in the monthly blood biochemistry results between the groups (Table 2, Supplemental Table 1). We further examined changes in serum phosphate and albumin before and at the end of the trial. As shown in Figure 2, more patients in the ACP group had a significant decrease in serum phosphate, and more patients in the SCP group had increased serum phosphate levels (p = 0.0398, Figure 2a). Notably, we found no significant changes in serum albumin levels after diet control in either group (Figure 2b). Our data suggest that this mobile ACP significantly reduced serum phosphate levels without decreasing serum albumin levels.
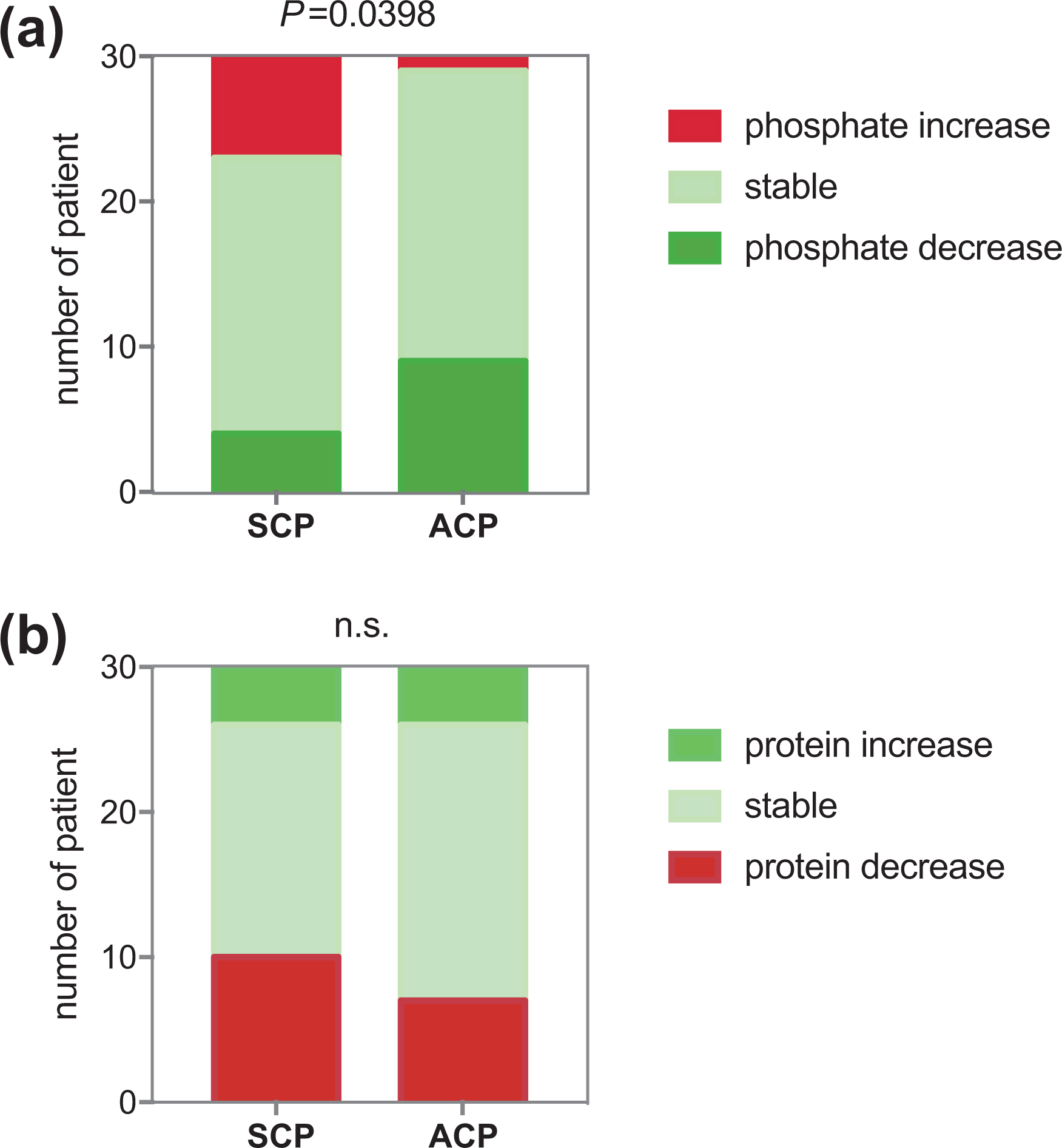
(a) phosphate change. (b) protein change.
Discussion
This study investigated the effects of an ACP for dietary phosphate control in patients with regular hemodialysis and showed that the use of the APP increased patients’ self-care efficacy and knowledge of dietary phosphate control, leading to decreased serum phosphate levels. The benefit of integrating smartphone-based APPs in medical care has previously been examined, but the results have not consistently supported the use of APPs. Singh et al. (2019) suggested that there was a considerable gap between the experiences that patients and medical professionals had with APPs (Topf & Hiremath, 2019). While medical professionals focused on the accuracy of data, patients were more concerned with usability. The results of our study highlighted the importance of considering both usability and data accuracy in developing a patient-friendly health mobile APP. To ensure the accountability of data, we used the Taiwan Food Nutrition Database, which was first established in 1992 and is maintained solely by the Taiwan Food and Drug Administration, Ministry of Health and Welfare. The latest version was updated in 2018. Meanwhile, we made a user-friendly interface and simplified the search results and dietary records into an easy-to-understand scoring system to ensure usability for patients. Furthermore, the dietary information and records generated by the APP were incorporated into a bidirectional communication featuring tailored feedback from medical staff to establish and adjust the participants’ dietary plans.
Timely updates of dietary records have been shown to be an important driving force for motivation and self-management (Arsand et al., 2008; Intille et al., 2003). In our study, we also found that timely updates of the health score did improve patients’ understanding of dietary phosphate content. Furthermore, we noted that the feature allowing participants to share their dietary records with the medical team impacted the success of the dietary control of phosphate. This demonstrates that sharing records with others further enhances patients’ motivation for diet control, which can be explained by “intrinsic motivation,” a concept described in the self-determination theory (Pelletier et al., 2001). On the other hand, the use of the APP further empowered the patients by allowing them to share their secret recipes or ingredients to obtain a better health score and to demonstrate their active problem-solving ability, which could also be an important element leading to the success of our study.
In the interaction analysis, we noted that patients aged over 60 years showed a more positive association with the ACP than patients younger than 60 years old (Table 3). We think this finding validated the usability of the APP that we developed for this study. Furthermore, it highlighted the feasibility of integrating mobile APPs into the personalized care of chronic diseases, even in elderly patients. Interestingly, Wu and Lu (2017) demonstrated that increasing informal medical care improved the health behavior of elderly people. It would be interesting to further investigate whether these mobile device-based APPs are potential methods to provide timely and personal medical attention to elderly patients and improve their health behavior.
However, there were some limitations to the study that might prevent the generalization of this mobile APP. Mainly, the number of patients was small, the duration was only 3 months, and the participants had to possess and be able to operate a smartphone, which eliminated random allocation and generated inevitable selection bias, similar to most previous adherence intervention studies on dialysis patients (Milazi et al., 2017; Murali et al., 2019). Instead of pre-validated self-efficacy scales like Strategies Used by People to Promote Health (SUPPH), a 29-item self-report (Lev & Owen, 1996), our scales and questionnaires were modified from three Chinese self-efficacy scales for other chronic diseases. Even though internal validation was performed, the assessment of patients’ self-care efficacy might not have been comprehensive. There were more men and more patients with hemodialysis vintage < 5 years in the APP group, which suggested a suboptimal allocation of participants; however, this did not affect the results of self-efficacy, knowledge, or biochemistry outcomes. Even though this was a single-center, short-term, non-randomized control trial (due to its nature as a pilot study), it demonstrated the safety and usability of a mobile APP on phosphate control in hemodialysis patients in daily practice and contributed to time-saving for healthcare professionals. A longer randomized control trial is necessary to determine whether the phosphate-lowering effect could be sustained, even leading to better clinical outcomes and lower medical costs. In conclusion, the ACP benefited patients with regular hemodialysis to achieve better dietary phosphate control without compromising proper protein intake.
Supplemental Material
Supplemental Material, sj-pdf-1-brn-10.1177_1099800420975504 - Effects of Individualized Dietary Phosphate Control Program With a Smartphone Application in Hemodialysis Patients in Taiwan
Supplemental Material, sj-pdf-1-brn-10.1177_1099800420975504 for Effects of Individualized Dietary Phosphate Control Program With a Smartphone Application in Hemodialysis Patients in Taiwan by Yung-Chen Chiang, Ya-Ping Chang, Ssu-Chin Lin, Chin Lin, Pi-Hsiu Hsu, Yu-Juei Hsu and Tsung-Jui Wu in Biological Research For Nursing
Footnotes
Author Contributions
Chiang YC and Chang YP, contributed to conception, design and drafted manuscript. Lin SC and Lin C contributed to analysis and interpretation. Hsu PH and Hsu YJ contributed to conception and design. Wu TJ contributed to analysis and interpretation, drafted the manuscript and gave final approval.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Medical Research Council of Tri-Service General Hospital [grant number: TSGH-C107-196].
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.