
Abstract
Hair cortisol concentrations (HCC) are an innovative way to measure chronic stress relying on a small sample of hair. To date, there are no studies that have studied HCC as a biomarker of chronic stress in individuals with dementia. Given the vulnerability to chronic stress in people with dementia, using HCC as an objective measure of physiological stress in those with dementia has potential to enhance our understanding of this population. The goal of this exploratory, multidisciplinary, pilot study was to establish feasibility of HCC testing in people with dementia as a biomarker of chronic stress. HCC was examined over a 6-month period to assess physiological stress response during a transition to memory care. Newly admitted memory care residents (n = 13, mean age = 82) were followed over 6 months. Residents’ hair samples and health information were collected at 3-month intervals. HCC levels significantly changed during the transition to memory care, which may reflect chronic physiological stress. Participants with frequent behavioral and psychological symptoms of dementia (BPSD) had significantly lower HCC at baseline and exhibited a blunted cortisol reactivity at follow-up. Based on detected changes in HCC, participants likely experienced stress reactions during the transition to memory care, providing preliminary evidence that HCC may be a useful, non-invasive measure of physiological stress in this population. This approach may also be applied to understanding the significance of person-centered care environments on minimizing chronic stress for people with dementia.
Keywords
Individuals with dementia often feel prolonged and persistent feelings of stress due to the unpredictable changes and losses associated with the disease (Bjørkløf et al., 2019; Kinnaird, 2018; Sharp, 2019). Stressors associated with the experience of living with dementia (e.g., behavior problems, memory loss, perceived dependency, and role and intrapsychic strains) could lead to negative outcomes such as depression, anxiety, and poor quality of life (Dawson et al., 2012). Thus, the adaptive capacity to adjust to stress, and accept the inevitable changes caused by the disease, are key to health, well-being, and quality of life for those living with dementia (Bjørkløf et al., 2019; Sharp, 2019). To date, however, the mechanism of the stress process for individuals with dementia is not yet fully understood.
Stress Processes and Dementia
People with dementia tend to be hyper-responsive to stress because they are likely to misinterpret environmental stimuli as threatening and have a lower threshold for enduring stress (Hall, 1987; Justice, 2018; Smith et al., 2004). Given that the hippocampus is highly susceptible to chronic stress (Conrad, 2008; Kim et al., 2015), and the impaired hippocampus function caused by dementia pathology increases the sensitivity to chronic stress in people with dementia, this likely further aggravates the hippocampal damage and functional disabilities in those with dementia (Alberini, 2009; Rothman & Mattson, 2010; Srivareerat et al., 2009). Moreover, because the hippocampus is involved in the regulation of the physiological stress response (Jankord & Herman, 2008), the hippocampal damage in people with dementia could also lead to hypothalamic-pituitary-adrenal (HPA) axis dysfunction (Rasmuson et al., 2001). Dysregulation of stress hormones (e.g., cortisol) caused by the HPA axis dysfunction can also further impair hippocampal function and HPA axis regulation, which in turn further accelerates dementia pathology and neurodegeneration (Green et al., 2006; Lee et al., 2009). In short, due to the pathology and nature of the disease process, combined with increased vulnerability to stress induced by adjusting to the disease, people with dementia tend to show elevated stress responses which may give rise to long-term activation of the stress response system and cortisol imbalance. This, in turn, may introduce diverse health problems in people with dementia.
It is well established that cortisol levels serve as an indicator of stress that a person perceives (Guilliams & Edwards, 2010). That is, because cortisol reflects adaptation of the HPA axis to stressors, levels of cortisol are indicative of the intensity of HPA axis activity in response to stress. While small increases in cortisol can help the body cope with stress, long-term HPA axis activation caused by repeated and prolonged exposure to stress results in elevated basal and stress-induced cortisol levels that have been linked to elevated risk for a number of health problems: heart disease, behavioral and mood disorders, weight gain, and memory and concentration impairment (Guilliams & Edwards, 2010). Heightened cortisol levels associated with chronic stress also suppress immune function, resulting in an increased risk of infectious diseases, cardiovascular diseases, and diabetes (Sapolsky et al., 2000). Furthermore, long-term activation of the stress response system can bring about HPA axis dysfunction and lead to potential endocrine disorders (e.g., hypercortisolism and hypocortisolism) and/or sleep disorders (e.g., diurnal dysrhythmia) (Guilliams & Edwards, 2010).
The associations between cortisol imbalance, health, and well-being in people with dementia has been reported extensively (Csernansky et al., 2006; Futch et al., 2017; Huang et al., 2009; Kovach et al., 2011; Woods & Dimond, 2002; Woods et al., 2011). Overall, researchers found that elevated circulating cortisol (i.e., physiological stress) leads to increased deposits of ß-amyloid plaques and neurofibrillary tangles in the brain that exacerbate cognitive deficits and accelerate the progression of dementia (Csernansky et al., 2006; Futch et al., 2017; Green et al., 2006; Huang et al., 2009). Additionally, abnormal cortisol profile is associated with greater behavioral and psychological symptoms of dementia (BPSD) (Woods et al., 2011). Despite the importance of chronic stress in understanding health and well-being for people with dementia, few studies have focused on these connections, and little is known about ways to objectively measure chronic stress in this unique and vulnerable population. Some researchers have assessed physiological stress in people with dementia by using traditional cortisol tests that measure the amount of cortisol in the blood, urine, or saliva (Csernansky et al., 2006; Kovach et al., 2011; Pu et al., 2020; Woods & Dimond, 2002; Woods et al., 2008, 2011). These cortisol sampling methods, however, are often challenging and inappropriate for measuring physiological stress in people with dementia because of difficulties in collecting adequate cortisol samples from this population (Pu et al., 2020). Most of all, the HPA axis response to chronic stress cannot be measured by these traditional cortisol sampling approaches because they focus more on “a day in the life” rather than a longer-term timeframe of the impact of stress. Accordingly, an alternative method reflecting longitudinal activation of the HPA axis should be used to capture ongoing, chronic stress in people with dementia.
Hair Cortisol as a Biomarker of Chronic Stress
Hair Cortisol Concentrations (HCC) are a novel method that measures long-term HPA axis activation to determine chronic stress levels. It is different from conventional cortisol tests that only focus on short-term/transient cortisol changes in response to acute stress; HCC represent retrospective accumulations of cortisol indicative of longer-term stress responses integrated into HPA axis activity over the preceding months (Russell et al., 2012). Many diverse, disciplinary research fields have already used HCC to measure physiological chronic stress and have demonstrated the validity and reliability of hair cortisol as a biomarker of chronic stress across age groups (Romero-Gonzalez et al., 2018; Lanfear et al., 2020). Furthermore, studies have focused on applications of HCC as an objective measure for diagnosis, prognosis, and management of clinical conditions (e.g., psychiatric disorders, adrenal disorders, cardiovascular diseases, severe stress, and chronic pain) (Greff et al., 2019). However, there is no study to date on HCC associated with chronic stress in older adults with dementia even though HCC might be particularly advantageous when attempting to understand the inner experiences of individuals with dementia, especially for those in the later stages of the disease process when they are not able to articulate their thoughts/experiences.
Not only could HCC reflect the extent to which people with dementia are under stress, but it may have significant potential in furthering understanding of health and well-being in dementia. For example, while no studies to date have specifically explored HCC in relation to well-being in people with dementia, HCC are associated with key determinants of health and well-being in the general older adult population (Wright et al., 2015). Elevated HCC are linked to depressive symptoms and poor cognitive performance (Abell et al., 2016; Feeney et al., 2020), whereas lower HCC are linked to greater conscientiousness and social connectedness in healthy older adults (Lee et al., 2021; Steptoe et al., 2017). Although results concerning correlations of HCC with mental health in older adults are inconsistent, these findings suggest that HCC might add insight into understanding quality of life in people with dementia. Therefore, in the current study, we aimed to investigate the association between HCC and chronic stress as well as explore the feasibility of HCC as a significant biomarker of chronic stress in people with dementia.
Research Questions
In this exploratory, multidisciplinary pilot study, we focused primarily on the following research question: (1) Is it feasible to use HCC as a biomarker of stress in people with dementia and (2) does HCC reflect their chronic stress? To address these questions, we first developed a protocol for safely acquiring hair samples from participants with moderate to late-stage dementia as they moved into a memory care community. Secondly, we analyzed HCC over multiple time points to detect potential changes in HCC indicative of chronic stress. Because it has been established in prior research that transitions to long-term care settings can be stressful for people with dementia (Ryman et al., 2019), we hypothesized that this timeframe would provide a unique opportunity to explore potential variability in HCC levels reflective of chronic stress-induced activation of the HPA axis. Additionally, we examined patterns of HPA axis reactivity, as well as factors associated with HPA stress reactivity, to help contextualize the HCC results.
Methods
Study Site and Participants
We first established a collaborative research partnership between a community-based memory care community and research university; researchers initially met with leadership and administration from a regional senior living organization to collaboratively identify the memory care study site, develop a recruitment plan, and create a data collection protocol. A newly developed, built, and opened memory care community served as the study site and data collection took place over a period of 6 months. The advantage of recruiting participants and beginning data collection upon relocation to a brand-new facility meant that all participants experienced the transition to memory care within a similar time frame. Eligibility criteria for participants included individuals who were: (1) diagnosed with dementia; (2) aged 60 or more; and (3) expected to move into the long-term memory care program (i.e., newly admitted residents). Recruitment materials (e.g., recruitment flyers, introduction letter, informed consent, HIPPA authorization form, and the assent script) were provided to the admission staff and community relations coordinators. They distributed the recruitment materials to family members of potential new residents via email and during the memory care admission process. All newly admitted residents who met eligibility criteria were invited to participate. Admission staff informed the surrogate decision makers (i.e., legal guardians) for potential participants of the study and referred them to the research team for additional information. Those who consented for their wards to participate in the study signed an informed consent and HIPPA authorization forms. In addition, we also sought verbal assent from the participants before conducting hair sampling or data collection. The response rate was close to half (43%; 13 out of 30) of those approached about the study, agreeing to participate. 13 participants began the study, but 3 participants eventually dropped out at the 24-week follow-up due to transfer to a higher level of care in an intensive care unit. At the time of the 6-month follow-up, 10 participants remained in the sample.
Study Design
We relied on a longitudinal design that employed repeated measurements. Data were collected at 3-month intervals over a 6-month timeframe, which included the following: baseline, 12 weeks, and 24 weeks after the baseline assessment. At these timepoints, we collected participants’ hair samples as well as health records and nursing staff notes. Because hair samples at the time of each data collection reflected cortisol secretion in the prior 3 months, the 3 hair samplings allowed for the examination of changes in participants’ HCC levels between pre-transition and post-transition to memory care (e.g., 3 months prior to baseline, baseline, 3 months post-baseline). This study was approved by the Washington State University Institutional Review Board (the approval number: 16643-001).
Measures
Demographics and Health Characteristics
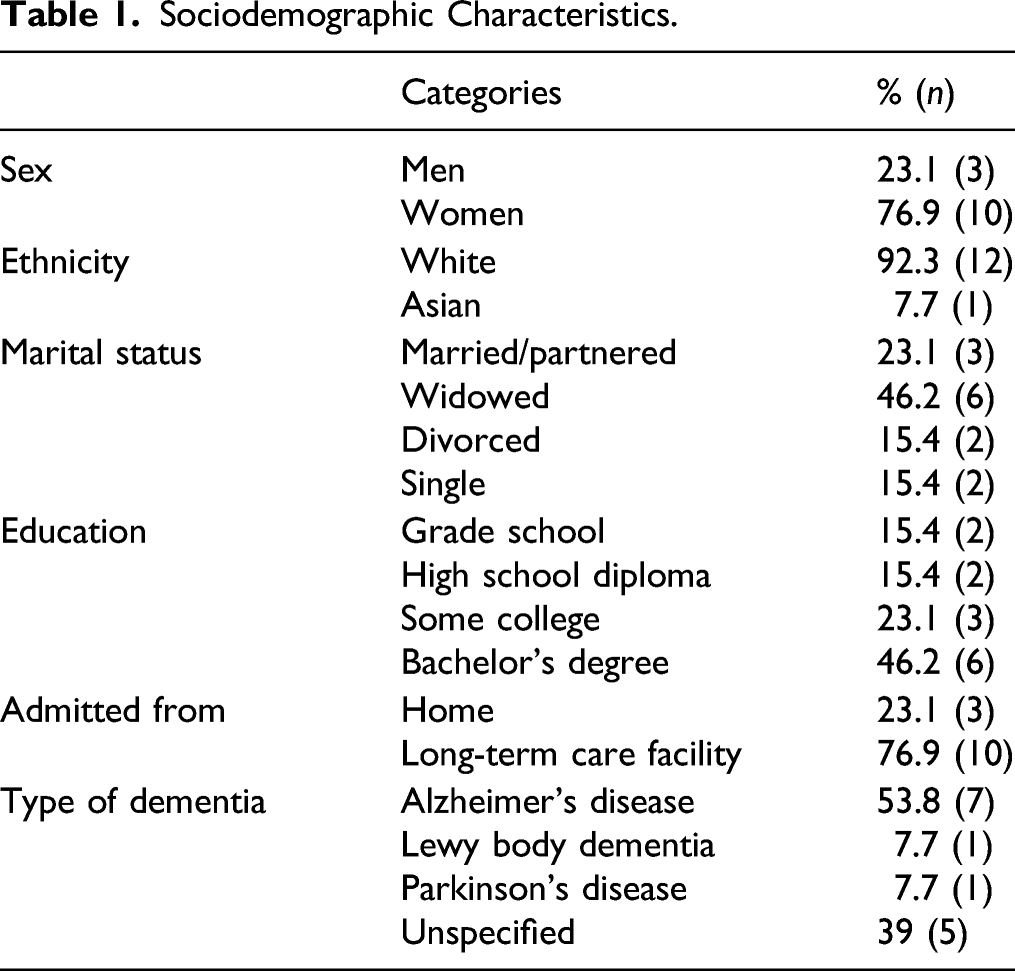
Sociodemographic and health information for each participant was collected from their resident charts. Because the presence of medical conditions have been shown to correlate with human hair cortisol (e.g., adrenocortical conditions, post-traumatic stress disorder (PTSD), cardiovascular disease, diabetes, hypertension, body mass index (BMI), chronic pain, depression, and anxiety) (Wosu et al., 2013), we examined participants’ charts in order to assess their overall health status and functional abilities, the number of active diagnoses, current medications, fall and injury reports, health change reports, and hospital visits over all 3 data collection time points.
Functional Ability
A 12-item resident assessment instrument developed by the participating memory care facility was used as a tool to evaluate the functional capabilities of participants. The nursing staff performed the assessment for all residents on admission, with subsequent monthly assessments, or at any time when residents experienced significant changes in health or functional status. The 12 items consisted of communication, ambulation, ADL, elimination, nurse intervention, cognitive ability, eating, fragility, behavioral-physical/verbal ability, medication services, treatment, and safety supervision. Response categories captured different levels of residents’ functional impairment in each domain. In addition, nursing staff rated residents’ current level of functional abilities on a given numeric scale, with the lower scores representing independent function and the higher scores representing severe impairments. The total score was calculated by summing scores of 12 items, which could range from 3 to 45.
Cognitive Functioning
Participants’ cognitive impairment was assessed via a cognitive ability item in the resident assessment instrument. This item measured the severity of impairment in memory, thinking, and reasoning skills. Nursing staff rated participants’ cognitive functions on a 6-point scale. Response categories ranged from 1 (alert but forgetful, confused or disoriented at times) to 6 (no longer responds to name, does not make/maintain eye contact, loses the ability to communicate). Higher scores indicated greater cognitive impairments.
Behavioral and Psychological Symptoms of Dementia (BPSD)
Participants’ BPSD were measured with the behavior-physical/verbal item in the resident assessment instrument. The behavior-physical/verbal item assessed participant levels of behavioral disturbance. Nursing staff rated the occurrence of physically or verbally aggressive behaviors over the past month on a 4-point scale ranging from 0 (no BPSD, always compliant) to 4 (physically or verbally abusive/aggressive more than 1 time a day). Higher scores indicated more frequent/severe disruptive behaviors.
Psychotropic Medications
Because the use of psychotropic medications is thought of as a proxy measure for levels of psychological symptoms or mood in persons with dementia (Konovalov et al., 2008), psychotropic medications administered to participants were used as a measure of psychological well-being in dementia. Information about psychotropic medications was obtained via a review of physician’s orders, medication orders, and medication dispensing records included in residents’ charts. Specifically, the type, number, frequency, and dosage of psychotropic medications administered to participants was examined at all timepoints.
Hair Cortisol
Hair samples were collected in the memory care facility’s hair salon at baseline, 12 weeks, and 24 weeks after the transition into memory care. The professional salon staff hired by the facility assisted in cutting the samples while participants received services at the salon. The research team trained the salon staff to be well-acquainted with the hair collection protocol prior to hair samplings and monitored all hair sampling procedures during participants’ haircut services. Verbal assent was confirmed by a researcher before continuing with the hair sampling; a researcher collected and stored the samples for lab analysis. The familiarity of the salon and sitting in a salon chair helped to facilitate the hair sampling process for participants. A minimum of 9 mg of the most proximal 3 cm hair segment were cut from the posterior vertex of participants (the back of the head where the scalp transitions from horizontal to vertical). Each sample would represent the total retrospective HPA axis activity over the preceding 3 months based on an average hair growth rate of 1 cm/month (Greff et al., 2019). The average weight of hair samples collected was 22.4 mg (range: 9.4–55.8 mg, median: 22.5 mg).
Hair cortisol concentrations was extracted following protocol described in Russell and colleagues (2012), and cortisol was quantified using an enzyme-linked immunosorbent assay (ELISA, Cayman Scientific, Ann Arbor, MI, USA). Briefly, to extract cortisol, hair samples were washed with isopropanol, dried under nitrogen stream, minced and then incubated for 18 hours in methanol. Methanol was evaporated under nitrogen in a 40°C water bath, and the sample was resuspended with ELISA buffer (provided by manufacturer). Samples were assayed in duplicate following manufacturer’s instructions. Intra-assay coefficient of variation (CV) and inter-assay CV were acceptable: 7.36% (range: 0.41–15.45) and 9.90%, respectively.
Data Analysis Plan
Statistical assumptions were tested as preliminary analyses and descriptive analyses were used to report means, medians, and standard deviations of all study variables. A log transformation was applied to HCC values to correct skewness. First, intra-individual changes in HCC over the 6-month period were examined by using a mixed-effect model. A 2-level growth model was conducted. At level 1, the HCC growth curve over the course of 6 months was explored to identify the effect of the transition to memory care on the long-term cortisol output. At level 2, the influence of individual factors on the HCC trajectories was examined. We adjusted our estimates for the presence of covariates that might affect baseline HCC levels and the HCC trajectories over the course of 6 months. This included controlling for the following variables in analyses: information related to age, gender, clinical conditions associated with HCC (e.g., adrenocortical conditions, cardiovascular disease, diabetes, BMI, and depression), levels of BPSD, functional abilities, the number of active diagnoses, current medication use (psychotropic drug use, dementia medication use), fall and injury reports, health change reports, and hospital visits. SPSS-25 was used to analyze the data.
Results
The data screening process included missing value analysis and the examination of outliers and normality. The statistical assumptions were all met. For the 3 participants who dropped out at the 24-week follow-up, their HCC values and relevant health information at the 24-week follow-up were missing. Missing values were evaluated using the expectation-maximization (EM) procedure to test whether missing values were completely random or whether there were patterns in the missing data. According to Little’s missing-completely-at-random test, no pattern existed in the missing values (χ2 (47) = 33.28, p = .94). Missing values were imputed using multiple imputations, and complete data were used for further analyses.
Sociodemographic Characteristics.
Psychotropic Medications Use at Baseline, 12 weeks, and 24 weeks.
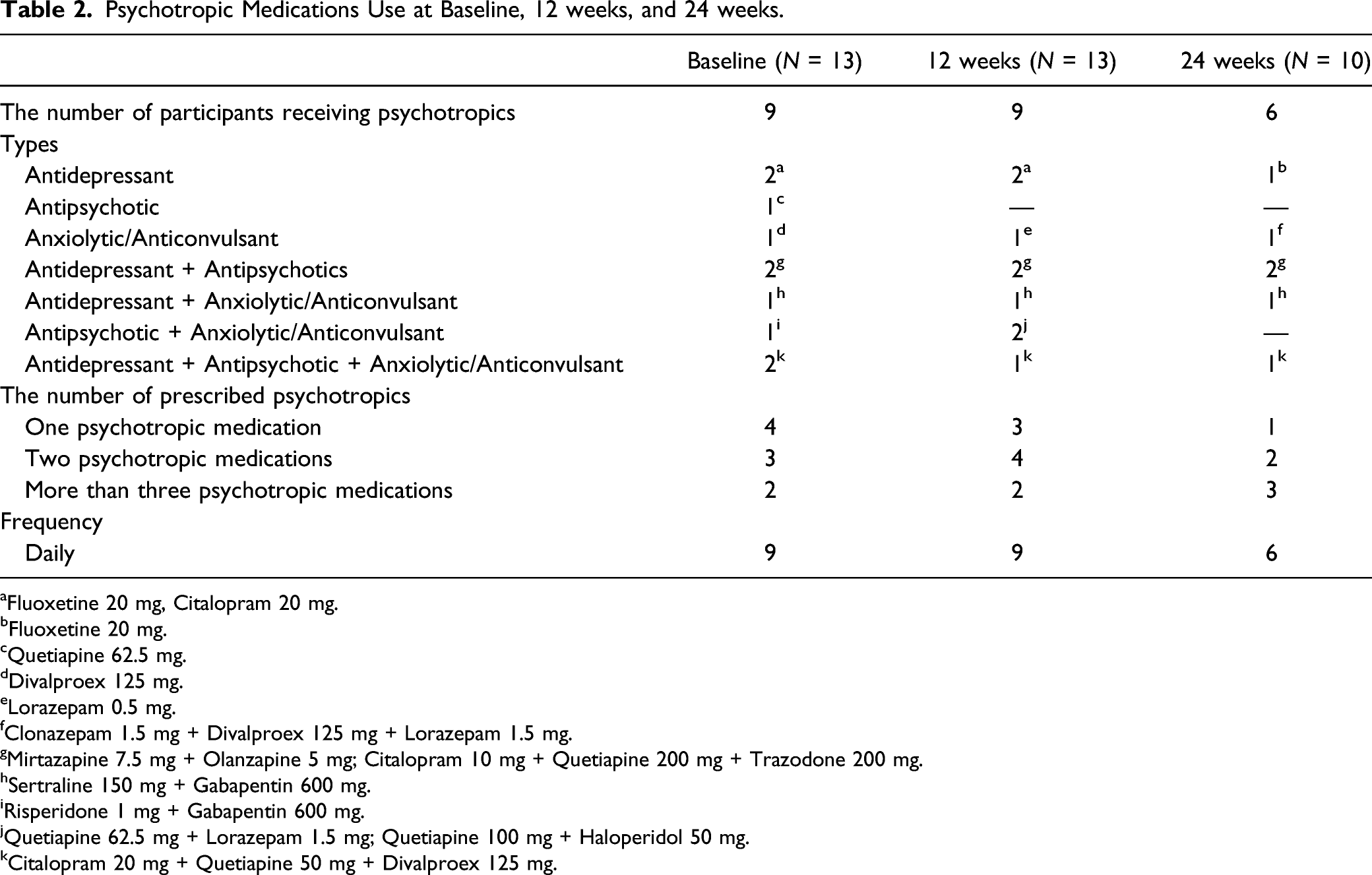
aFluoxetine 20 mg, Citalopram 20 mg.
bFluoxetine 20 mg.
cQuetiapine 62.5 mg.
dDivalproex 125 mg.
eLorazepam 0.5 mg.
fClonazepam 1.5 mg + Divalproex 125 mg + Lorazepam 1.5 mg.
gMirtazapine 7.5 mg + Olanzapine 5 mg; Citalopram 10 mg + Quetiapine 200 mg + Trazodone 200 mg.
hSertraline 150 mg + Gabapentin 600 mg.
iRisperidone 1 mg + Gabapentin 600 mg.
jQuetiapine 62.5 mg + Lorazepam 1.5 mg; Quetiapine 100 mg + Haloperidol 50 mg.
kCitalopram 20 mg + Quetiapine 50 mg + Divalproex 125 mg.
BPSD and Cognitive Impairment at Baseline, 12 weeks, and 24 weeks.
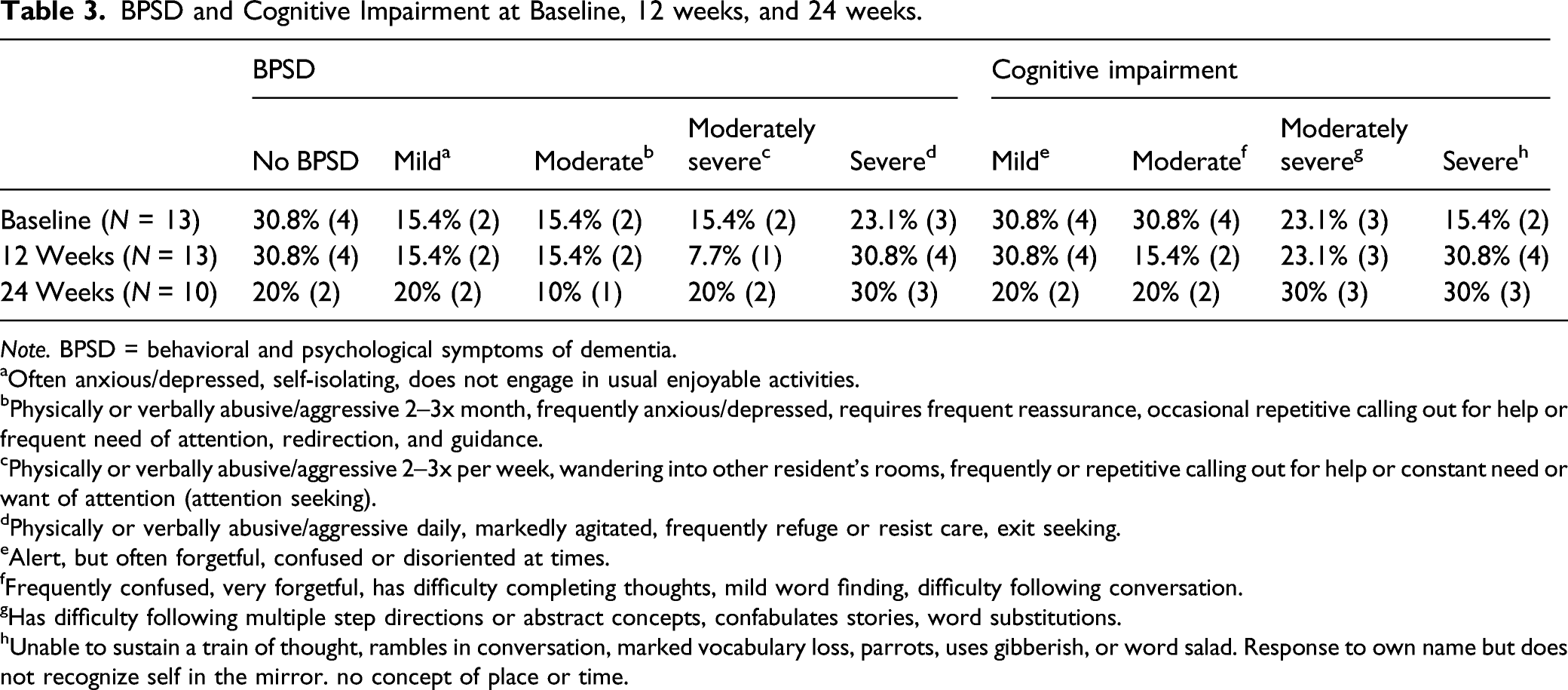
Note. BPSD = behavioral and psychological symptoms of dementia.
aOften anxious/depressed, self-isolating, does not engage in usual enjoyable activities.
bPhysically or verbally abusive/aggressive 2–3x month, frequently anxious/depressed, requires frequent reassurance, occasional repetitive calling out for help or frequent need of attention, redirection, and guidance.
cPhysically or verbally abusive/aggressive 2–3x per week, wandering into other resident’s rooms, frequently or repetitive calling out for help or constant need or want of attention (attention seeking).
dPhysically or verbally abusive/aggressive daily, markedly agitated, frequently refuge or resist care, exit seeking.
eAlert, but often forgetful, confused or disoriented at times.
fFrequently confused, very forgetful, has difficulty completing thoughts, mild word finding, difficulty following conversation.
gHas difficulty following multiple step directions or abstract concepts, confabulates stories, word substitutions.
hUnable to sustain a train of thought, rambles in conversation, marked vocabulary loss, parrots, uses gibberish, or word salad. Response to own name but does not recognize self in the mirror. no concept of place or time.
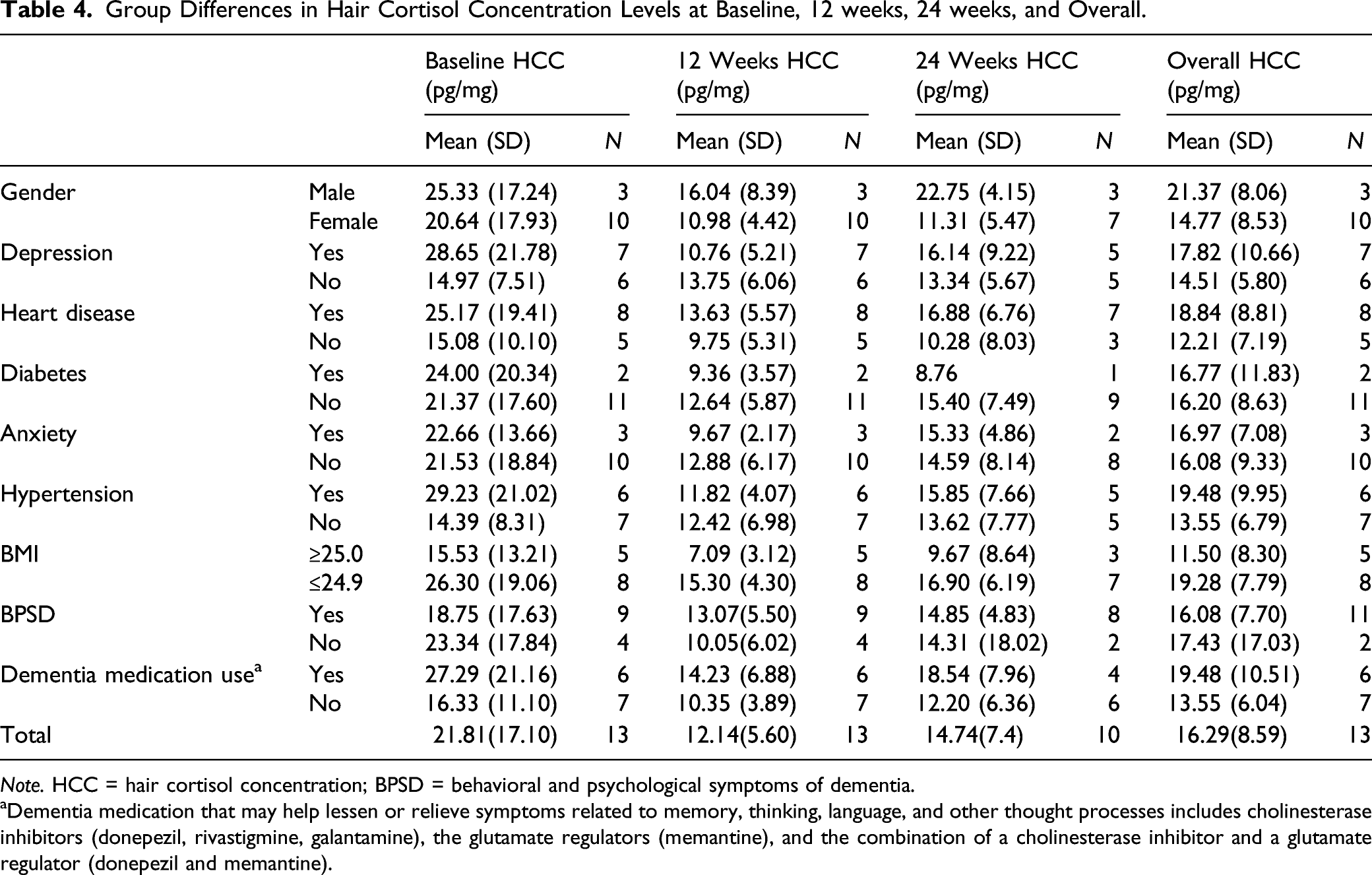
The overall mean of HCC levels over a 6-month period was 16.29 pg/mg (SD = 8.60, range = 5.25–30.32) and the median HCC was 13.35 pg/mg. More specifically, the mean of HCC changed over time: at baseline it was 21.81 pg/mg (SD = 17.10), and then 12.14 pg/mg (SD = 5.60) at the 12-week follow-up, and finally, 14.74 pg/mg (SD = 7.37) at the 24-week follow-up. See Figure 1 for the mean HCC levels at baseline, 12-week, and 24-week follow-up and Table 4 for group differences in HCC levels over the course of 6 months period. Hair Cortisol Concentrations Changes during the Transition to Memory Care. Group Differences in Hair Cortisol Concentration Levels at Baseline, 12 weeks, 24 weeks, and Overall. Note. HCC = hair cortisol concentration; BPSD = behavioral and psychological symptoms of dementia. aDementia medication that may help lessen or relieve symptoms related to memory, thinking, language, and other thought processes includes cholinesterase inhibitors (donepezil, rivastigmine, galantamine), the glutamate regulators (memantine), and the combination of a cholinesterase inhibitor and a glutamate regulator (donepezil and memantine).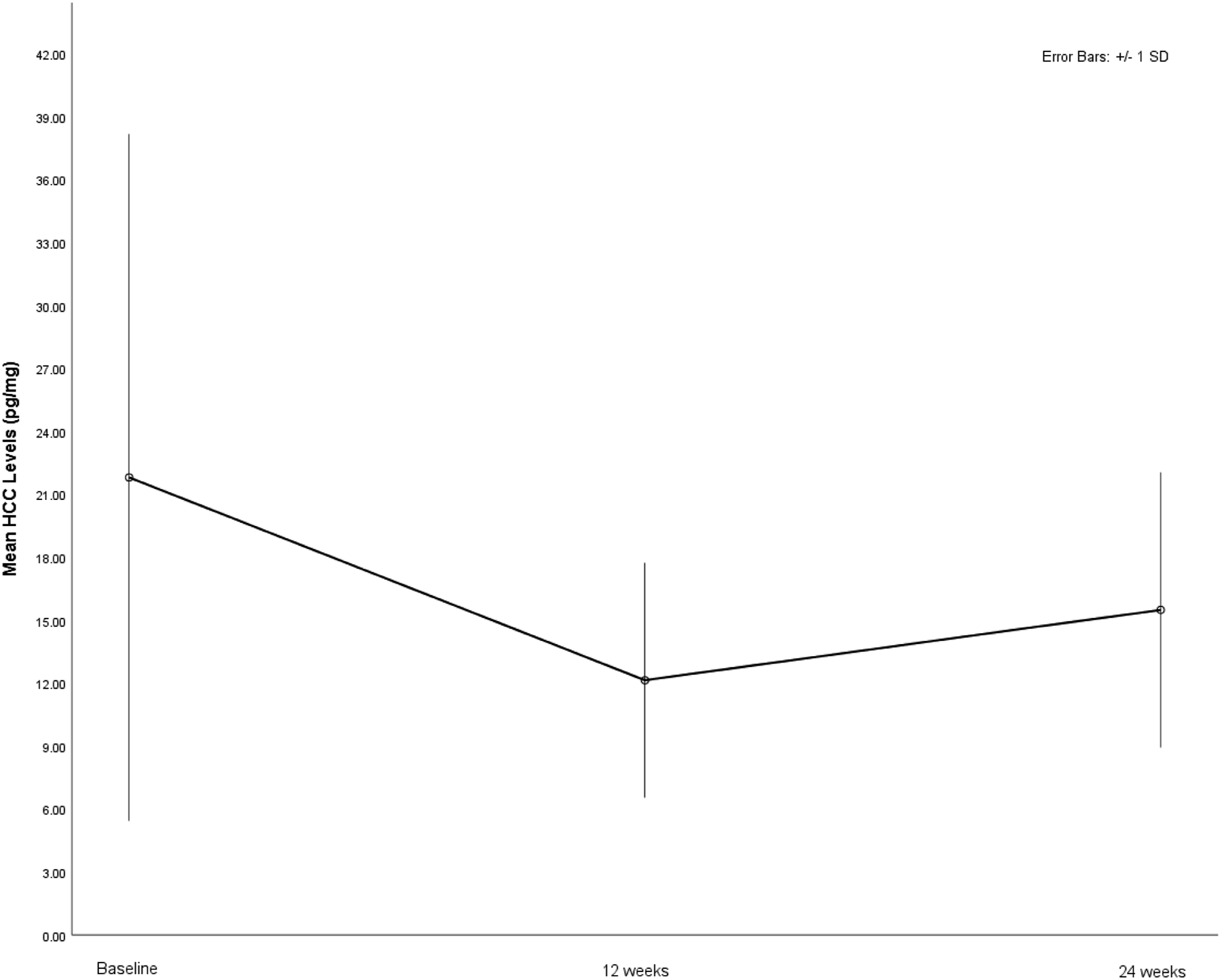
Changes in HCC Levels Over Time
A multilevel model was used to identify changes in HCC levels in response to transition to memory care. Four models, ranging from the simple (a null model) to complex (a 2-level model with fixed and random effects), were performed to find a good model that fit the data. In the initial multilevel model, the majority of factors associated with participants’ health status and functional ability (e.g., number of active diagnoses, fall and injury reports, health change reports, and hospital visits, levels of functional impairment, use of dementia medication) were not significantly associated with baseline HCC levels and the HCC trajectories over time (p > .05). To derive a parsimonious model, we retained variables previously established to be associated with baseline HCC (Feller et al., 2014), including age, gender, the presence of cardiovascular disease, diabetes, depression, BMI, frequency of BPSD, and number of received psychotropic medications).
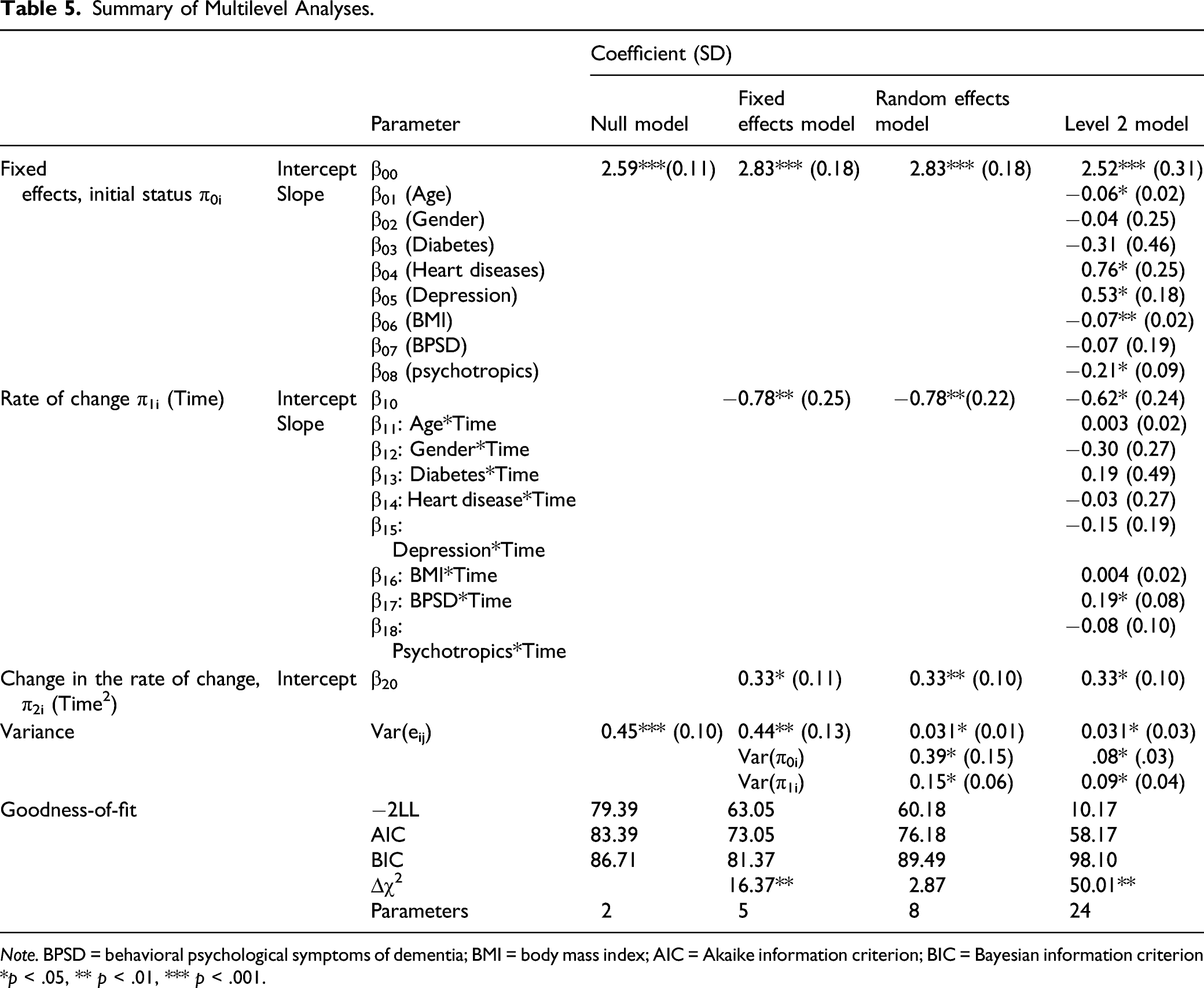
The multilevel model showed significant intra-individual changes in HCC levels over time (β10 = −.62, p < .05) and a significant curvilinear shape of HCC growth trends (β20 = .33, p < .01). This indicated that participants’ HCC levels decreased right after the transition and then increased after the 12-week follow-up (i.e., a U-shared curve). See Figure 2 for individual HCC changes during transition to memory care. Of note, there were significant individual differences in the baseline HCC and the rate of HCC change over time. Specifically, we found that there were significant effects of age (β01 = −.06, p < .05), heart disease (β04 = .76, p < .05), depression (β05 = .53, p < .05), BMI (β06 = −.07, p < .01), and the number of psychotropic medications administered to participants (β08 = −.21, p < .05) on the baseline HCC level. That is, heart disease and depression contributed to higher baseline HCC values while advanced age, being overweight, and greater psychotropic medication use were associated with lower baseline HCC levels. These between-individual predictors accounted for 79.5% of the between-individual variance in the baseline HCC levels. Next, the effects of between-individual predictors on the rate of HCC growth were examined by using cross-level interaction terms. Frequent BPSD were associated with a flat HCC growth during the relocation transition (β12 = .19, p < .05). Overall, 40% of the between-individual variance in the rate of HCC change was explained by frequency of BPSD. See Table 5 for the summary of the multilevel analyses. Intra-individual Changes in HCC levels during the Transition to Memory Care. Note. HCC = hair cortisol concentrations. Summary of Multilevel Analyses. Note. BPSD = behavioral psychological symptoms of dementia; BMI = body mass index; AIC = Akaike information criterion; BIC = Bayesian information criterion *p < .05, ** p < .01, *** p < .001.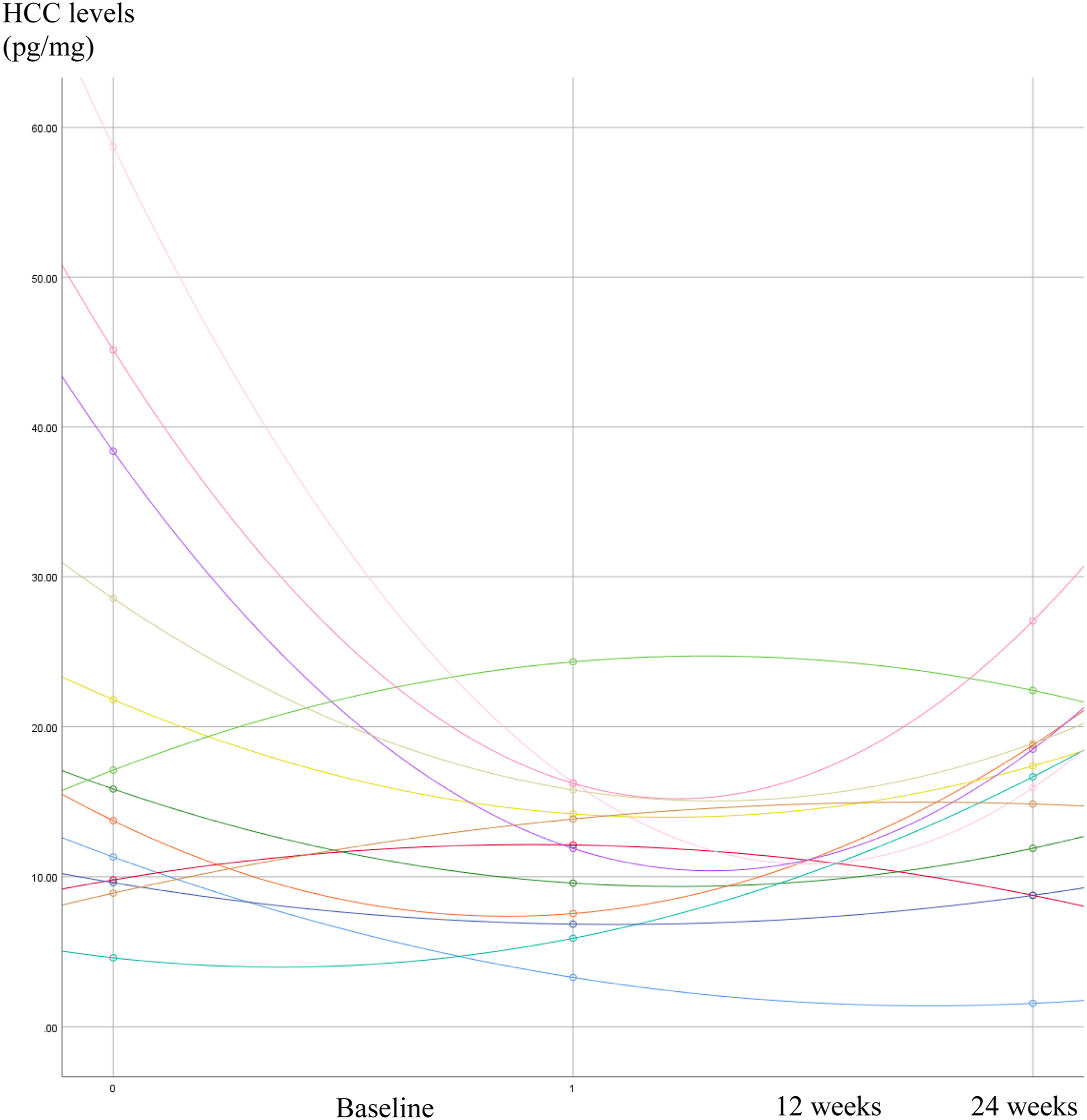
Patterns of HCC Changes During the Transition
Overall, the U-shaped HCC growth trajectory over the course of the 6 months period was identified (β20 = .33, p < .01). HCC declined by 44% between pre-transition and the 12-weeks post-transition, and after the initial transition phase, HCC increased by 21% between 12 weeks and 24 weeks post-transition. It is worth noting that not all participants followed the U-shaped HCC growth pattern. About 70% (n = 9) showed the U-shaped growth curve, while 30% (n = 4) showed an opposite pattern (bell-shaped growth curve) that represents increased HCC levels after the transition and then decreased HCC levels. There were significant differences between the bell-shaped HCC growth group and the U-shaped HCC growth group with regard to baseline HCC levels and the magnitude of HCC alteration during the transition. Specifically, participants with the bell-shaped HCC growth curve exhibited lower baseline HCC (t = 2.45, p < .05) and flatter HCC change trajectory during the transition (t = 2.53, p < .05) compared to the U-shaped HCC growth group. However, there were no significant differences in health conditions and comprehensive HCC levels between these groups.
Discussion
The ability to measure hair cortisol is a novel, non-invasive tool that has only recently emerged, but will become more widespread in research and clinical practices (Greff et al., 2019). To our knowledge, this was the first known study to examine the feasibility of HCC as a biomarker of chronic stress in individuals with dementia, by testing changes in HCC levels during the relocation transition to memory care, wherein persons with dementia are exposed to chronic stress (Ryman et al., 2019). In partnership with leaders and administrators at the memory care clinic, we were able to develop a protocol for feasibly recruiting participants who were receptive to the process and successfully sampled and analyzed HCC in hair from participants with dementia over time. Our results also pave the way for future studies to further establish the connection between HCC as a biomarker of chronic stress in people with dementia.
Collecting hair samples from a vulnerable participant population was achievable. Hair sampling acceptance was high among participants and most participants were cooperative. A high percentage (85%; 11 out of 13) adhered to the protocol of hair collection over the entire course of the study. Although researchers, or even facility clinical staff, could have easily collected hair samples, using the hair salon staff to collect hair during an established in-facility hair cutting appointment enhanced participants’ adherence to and tolerance for the hair sampling and collection protocol. The hair stylists were more familiar to residents than outside researchers and were skilled in cutting hair for people with dementia as well as helping them feel comfortable in the salon. This process also did not over-burden other facility staff or interfere with their clinical care tasks by requiring them to participate in hair sampling data collection. There were some challenges, however, associated with obtaining hair samples from persons living with dementia in general. While most participants eventually provided all their hair samples, on occasion, multiple attempts were needed to obtain hair samples, especially if participants’ health condition, well-being, or general mood at the time of the scheduled salon appointment was not conducive to hair sampling at that time. For example, participants exhibiting severe BPSD at the time of the scheduled appointment were more likely to be reluctant to have their hair sampled and had difficulties in tolerating hair sampling procedures. We adhered to a participant-centered approach, however, and re-scheduled sampling for a later time that was more acceptable to the participants. We recommend a tailored protocol and development of additional strategies for collecting hair samples from people living with dementia to continue fostering future studies using HCC to measure chronic stress in those with dementia.
Effects of Transition to Memory Care on HCC Levels
Given that HCC represent the HPA axis stress response over the preceding months, and because we collected HCC at 3 time points, we were able to observe variation in stress responses during the transition to memory care which causes chronic stress among people with dementia (Ryman et al., 2019). More specifically, we observed a significant decrease in HCC levels between pre- and post-transition to memory care. The sharp drop in HCC at the second time point (representing baseline and time of relocation to a new environment) followed by its gradual return to baseline levels at the third time point, could be interpreted many ways. It may suggest the process of habituation to the new environment (Herman, 2013), or that the patterns of HCC growth trajectory indicated the transition to memory care caused chronic physiological stress. Alternatively, it is plausible that the drop in cortisol during this transition reflected lower activity and engagement while living in a new memory care setting. Due to the exploratory nature of this experiment, we are not able to make conclusive statements that explain the causes of diminished cortisol response to stress during this transition, but we were able to establish feasibility of collecting hair samples in this unique population, conducting HCC testing, and observing variation in stress levels. Ongoing, further research is needed to continue to support the viability of HCC as an objective measure of stress among people with advanced dementia.
In terms of factors associated with HCC levels at baseline and the rate of HCC change during the transition, psychological symptoms affected HPA axis reactivity during the transition. For example, participants with frequent BPSD had lower HCC at baseline and exhibited a blunted cortisol reactivity during the transition (i.e., flattened HCC growth trajectory). These results are consistent with research supporting the association between the severity of BPSD and altered HPA axis stress reactivity (Woods et al., 2011). On the other hand, health characteristics did not appear to be related to HCC levels in this participant sample. More specifically, functional impairment, the number of active diagnoses, hospital visits, fall and injuries reports, and health change reports were not associated with participants’ baseline HCC levels or their HCC trajectories during the transition to memory care. Interestingly, we also found that participants with high BMI showed low basal cortisol, as opposed to findings from previous studies indicating a positive correlation between BMI and HCC in older adults (Feller et al., 2014; Jackson et al., 2017), further highlighting the need for future research to better understand these relationships, especially in people who have dementia.
Long-term stress exposure contributes to prolonged HPA axis activity and elevated HCC levels (Russell et al., 2012). However, HCC levels among participants in this study, significantly decreased after the transition to memory care rather than showing an increased cortisol reactivity during the transition to memory care. This aberrant HPA axis stress reactivity in this study could imply that the process of chronic stress response in people with dementia may work differently. It is possible that their HPA axis function in regulating chronic stress may be altered because of damage to the brain caused by dementia (Woods et al., 2008), potentially leading to a blunted hormonal response to stress and altered stress responses (HCC decline after the transition). According to Miller and colleagues (2007), HPA activity could be either increased or decreased by the exertion of chronic stress, depending on personal traits and external conditions. As such, blunted HPA axis reactivity is another form of response to chronic stress exposure. It is not uncommon for individuals living under ongoing stress to show an altered HPA axis stress reactivity, such as a hypo-reactive HPA axis, and a diminished cortisol response to stress (Heim et al., 2000). In summary, the transition to memory care appeared to elicit cortisol stress responses in participants, which is suggestive that HCC might be a possible objective measure of chronic stress in people with dementia. Furthermore, we identified individual variations in glucocorticoid stress response and heterogeneous forms of cortisol response to chronic stress among participants. However, little is explained for the inconsistent patterns of HCC growth trajectory because of the small sample size, so this finding should be viewed with caution. A larger sample might make it possible to account for heterogenous cortisol stress response in people with dementia by identifying factors (i.e., moderators) that determine the HCC growth trajectory. Future studies should focus on how people with dementia respond to chronic stress and which factors influence their stress processing.
Study Strengths and Limitations
There were several limitations associated with this study. First, as previously noted, the sample size was small relative to the number of explorative variables. Therefore, the results of the analytic modeling may be biased. In addition, participant attrition (23%, n = 3) might affect internal validity and introduce bias into results. In terms of measuring participants’ psycho-emotional functioning, we relied on a single item in the comprehensive resident assessment tool developed and used by the participating facility, which had no prior psychometric evidence. Lastly, because of the small sample size and exploratory nature of this study, caution regarding generalization of our finding to the larger population of people with dementia is needed.
Despite the small scale of this novel study, we were able to generate significant findings. First, we developed a feasible and successful protocol for sampling and analyzing HCC from people with dementia. We also identified the uniqueness of HPA stress reactivity in people with dementia, suggesting that the HPA axis stress reactivity may work differently in this population because of the stressful nature of dementia symptoms and their increased brain stress sensitivity (Smith et al., 2004). It is well documented that the transition to a long-term care facility can cause behavioral, cognitive or psychosocial stress outcomes among people with dementia, but no study has demonstrated physiological chronic stress outcomes associated with care transitions in those with dementia. We observed that transition to a long-term care facility may cause chronic physiological stress by simulating an experimental design that captured data just before the onset of a stressful event (i.e., transition to memory care), collecting data upon admission to memory care, and following participants over a 6-month period. This made it possible to uniquely test the impact of chronic stress on the HPA axis activity in our participants.
Practical Implications
In conclusion, HCC among people with dementia appears to reflect chronic stress, despite impairments in the brain due to disease progression; this supports the potential of HCC as a biomarker of chronic stress in people with dementia, but more research will be needed to establish typical HCC values for this population. Collaborative efforts involving health care providers, family caregivers, and memory care staff are needed to help individuals with dementia to adapt to new environments and minimize stress during care transitions. Because individuals with advanced dementia may not be able to verbalize or communicate their stress, objective measures via HCC could provide valuable information to practitioners. HCC measures may also be applied in research to understand the significance of person-centered care environments in decreasing stress and improving quality of life for people with dementia. Positive care environments that minimize chronic stress for those with dementia are crucial to improving their well-being because prolonged HPA reactivity is linked to adverse health outcomes (Guilliams & Edwards, 2010). Large-scale dementia population studies that include HCC will also help to further validate the usability of HCC in people with dementia as a biomarker of their chronic stress.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.