
Abstract
Introduction
The post-anesthesia care unit (PACU) is where surgical patients under general anesthesia receive monitoring and care immediately after surgery and is an intermediate transitional unit to provide care for patients (Truong et al., 2004; Waddle et al., 1998). Postoperative patients were admitted to the PACU and closely cared for by the anesthetic nurse and anesthesiologist until they recovered from the anesthesia effects, and then safely transferred to the ward by the anesthetic nurse (Lee et al., 2014).
Unplanned transfer of patients from the PACU to the ICU after surgery is one of the common critical events in the PACU (Bothner et al., 1999; Bruins et al., 2017). It is well-known that there is a shortage of ICU beds worldwide (Bing-Hua, 2014; Chomton et al., 2021; Coppadoro et al., 2021). Patients without plans to transfer to the ICU before surgery, and their transport time is often delayed compared with those who have reserved ICU beds (Shank et al., 2020). Limited ICU resources and delays in transfers are associated with increased hospitalization costs and morbidity, which can negatively affect their treatment and prognosis (Hourmant et al., 2021).
The risk of complications in cerebral surgery is high, and patients are prone to unpredictable changes after surgery (Franko et al., 2018; Zhou et al., 2018). In previous clinical practice, patients were usually admitted to the ICU for 12–24 hours of observation and treatment after cerebral surgery; most of them were transferred to the general ward the next day (de Almeida et al., 2018; Ehlers et al., 2020; Ziai et al., 2003). With the recent advancement in medicine and surgery, many studies have shown that patients do not need to be routinely transferred to the ICU after cerebral surgery; patients should be strictly evaluated and then judged whether they need to be transferred to the ICU for treatment and care, even for emergency cerebral surgery (Bonow et al., 2019; Henker et al., 2017; Laan et al., 2020; Lonjaret et al., 2017; Taylor et al., 1995; Volovici et al., 2019). Identifying postoperative patients requiring ICU admission is a challenging but necessary daily task. In the clinical setting, some patients undergoing cerebral surgery require unplanned ICU transfer despite thorough evaluation (Bui et al., 2011; Laan et al., 2020). Therefore, it is vital to improve the positive rate of identification, especially for those patients assessed as transferred to the ward but transferred to the ICU after surgery.
The identification of risk factors is critical to improving preoperative assessment. Therefore, this study aimed to examine preoperative, surgical, and PACU data for potential risk factors for unplanned ICU transfer, which has implications for improving the management and postoperative resource allocation of those vulnerable patients.
Materials and Methods
Design
This was an observational, retrospective, case-control study in which each case was matched with 2 controls. Unplanned transfer to the ICU was defined as no plan to transfer the patient to the ICU before starting anesthesia (i.e., the decision to transfer to ICU was made during or after surgery).
Setting
The study was conducted at the Affiliated Hospital of Jining Medical University, a Shandong Provincial Regional Medical Center with 82 clinical departments, 9 intensive care units, and 3028 beds. We retrospectively reviewed data of patients admitted to PACU after cerebral surgery. Those scheduled to be transferred to the ICU were excluded. Because for patients with scheduled postoperative intensive care admission, the general practice is to transfer them directly from the operating room to the ICU. The study followed the guidelines of the Declaration of Helsinki. The Ethics committee/IRB of Affiliated hospital of Jining Medical University gave ethical approval for this work (approval number: 2021-07-C009). A written informed consent was obtained from all patients upon transfer to the Affiliated Hospital of Jining Medical University.
Cases
Electronic records were used to selected patients ≥18 years of age who had undergone cerebral surgery from January 1, 2016, to December 31, 2020, and who had an unplanned transfer to ICU after cerebral surgery. The researchers reviewed the completeness and accuracy of each case.
Controls
For each patient with an unplanned transfer to ICU after cerebral surgery, 2 controls of the same type of surgery were randomly selected from the electronic medical records. Patients in the control group were matched (2:1) for sex, age (±5 years), and operation date (±48 hours). Researchers reviewed the data from patients in the control group to ensure the integrity of the included patients’ medical records.
Data Collection
All data extraction and data input were completed by members of the research team who have been trained in scientific research. The following demographic and current diseases data were collected: age, sex, smoking history, drinking history, and the presence of lung disease, hypertension, diabetes, hyperlipidemia, and/or cardiovascular disease. Patients who had quit smoking and drinking were still categorized into the smoking and drinking groups, respectively. Data on laboratory indicators, such as platelet volume, hemoglobin, total protein, albumin, uric acid, and blood glucose levels, were also collected. Laboratory indicators were measured on an empty stomach the day before the operation.
Surgical and anesthetic data, including the type of surgery, operation duration, blood loss volume, fluid replacement volume, urine volume, blood transfusion volume, heart rate, percentage of oxygen saturation (SpO2), removal of tracheal intubation, reintubation, and PACU duration, were collected. Volume of blood loss, of fluid replacement, and of urine were obtained over the entire operation period; heart rate and blood oxygen were obtained immediately after leaving the operating room.
Statistical Analysis
Statistical analysis was performed using Stata version 14.0 (StataCorp, College Station, TX, USA). Categorical data are described in terms of frequencies and percentages. The normality of continuous data was evaluated using the Kolmogorov–Smirnoff test. Normally distributed data are described in terms of means ± standard deviation, and non-normally distributed data in terms of medians and interquartile ranges. The T-test, Mann-Whitney test and the Chi-squared test were used to compare the characteristics between the case and the control groups. Logistic regression analysis was used to identify independent risk factors for unplanned ICU transfer of cerebral surgery patients. Statistical significance was set atp < .05.
Results
Patient Characteristics
From January 2016 to December 2020, 11,807 patients received recovery care after cerebral surgery in the PACU, of which 81 patients had unplanned ICU transfer (incidence of unplanned ICU transfer, 0.686%). Among unplanned ICU transfer patients, 3 patients under the age of 18 years and 2 patients who lacked relevant data were excluded. Finally, 228 patients were enrolled in this study: 76 in the case group and 152 in the control group (Figure 1). Study flow diagram.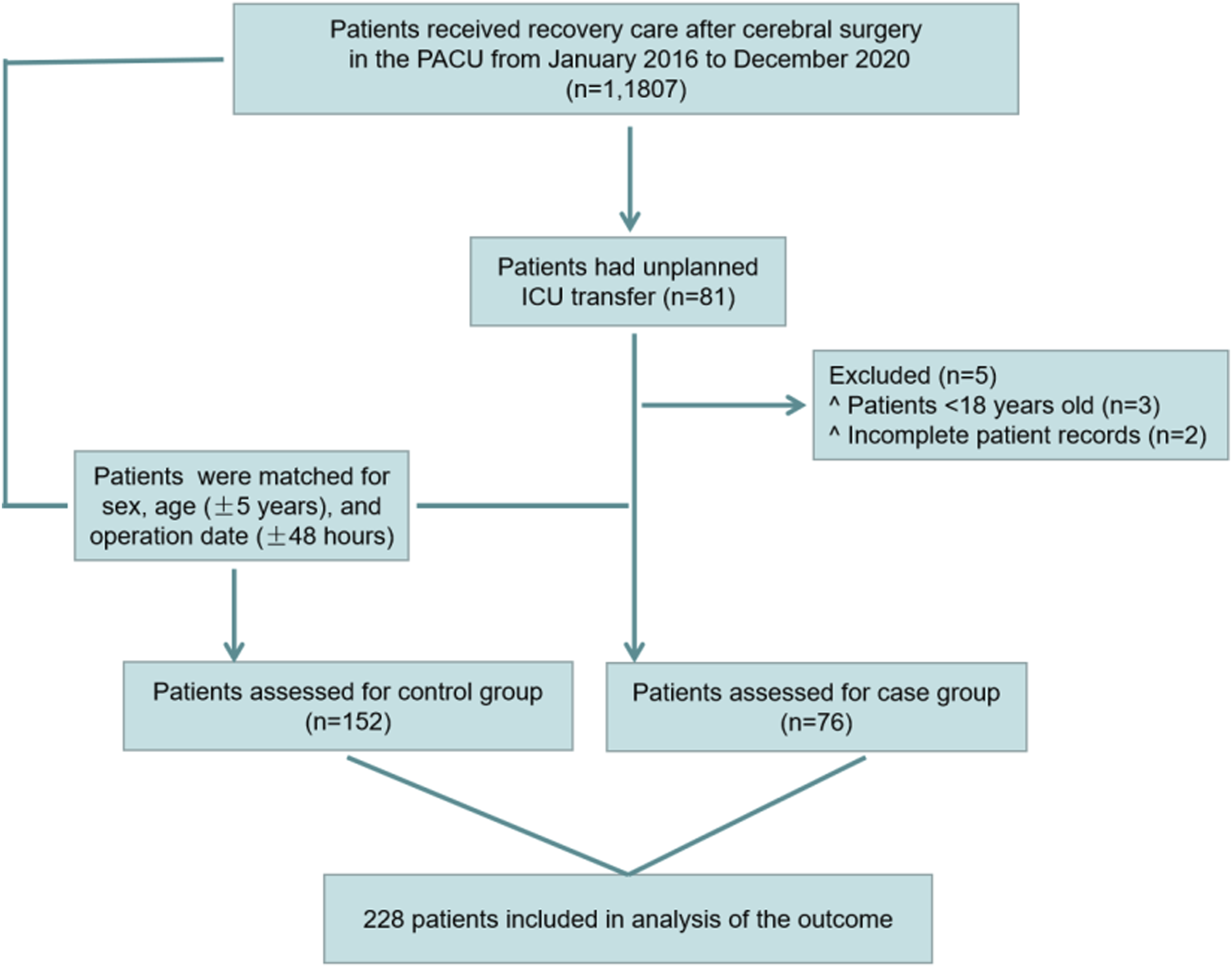
Patient Characteristics.
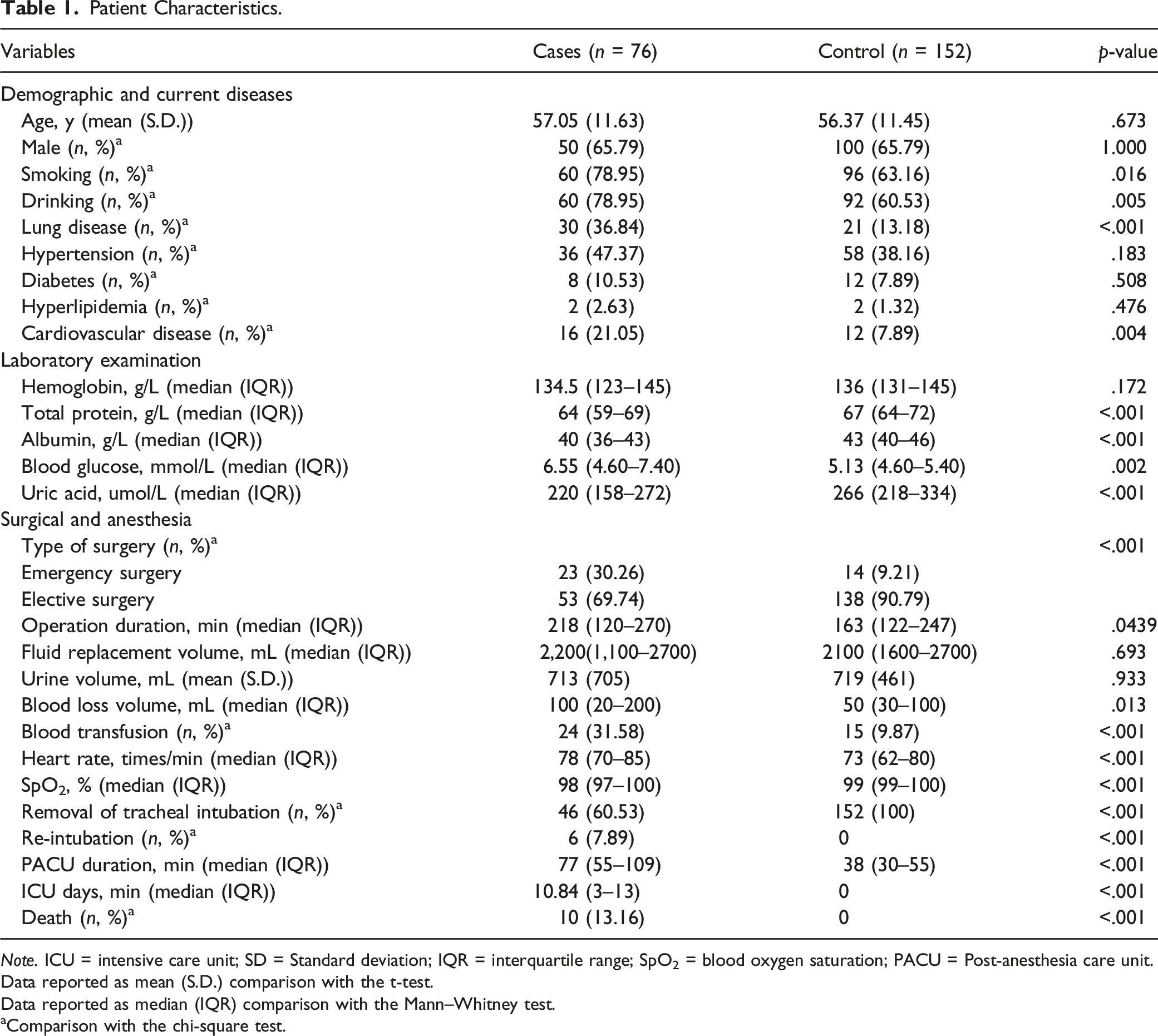
Note. ICU = intensive care unit; SD = Standard deviation; IQR = interquartile range; SpO2 = blood oxygen saturation; PACU = Post-anesthesia care unit.
Data reported as mean (S.D.) comparison with the t-test.
Data reported as median (IQR) comparison with the Mann–Whitney test.
aComparison with the chi-square test.
Compared with routine postoperative care, patients who with unplanned ICU transfer were more likely to have a history of smoking and alcohol use; a higher combined rate of pulmonary and cardiovascular disease; lower levels of total protein, albumin, and uric acid; and higher blood glucose levels. They were more likely to undergo emergency surgery, had longer procedures, lost more blood, and receive blood transfusions. They had higher mean heart rates, lower oxygen saturation levels, the possibility of removal of endotracheal tube was lower with higher risk of reintubation, and longer stay in PACU.
Risk Factors for Unplanned ICU Transfer
Univariate Analysis of Unplanned ICU Transfer.
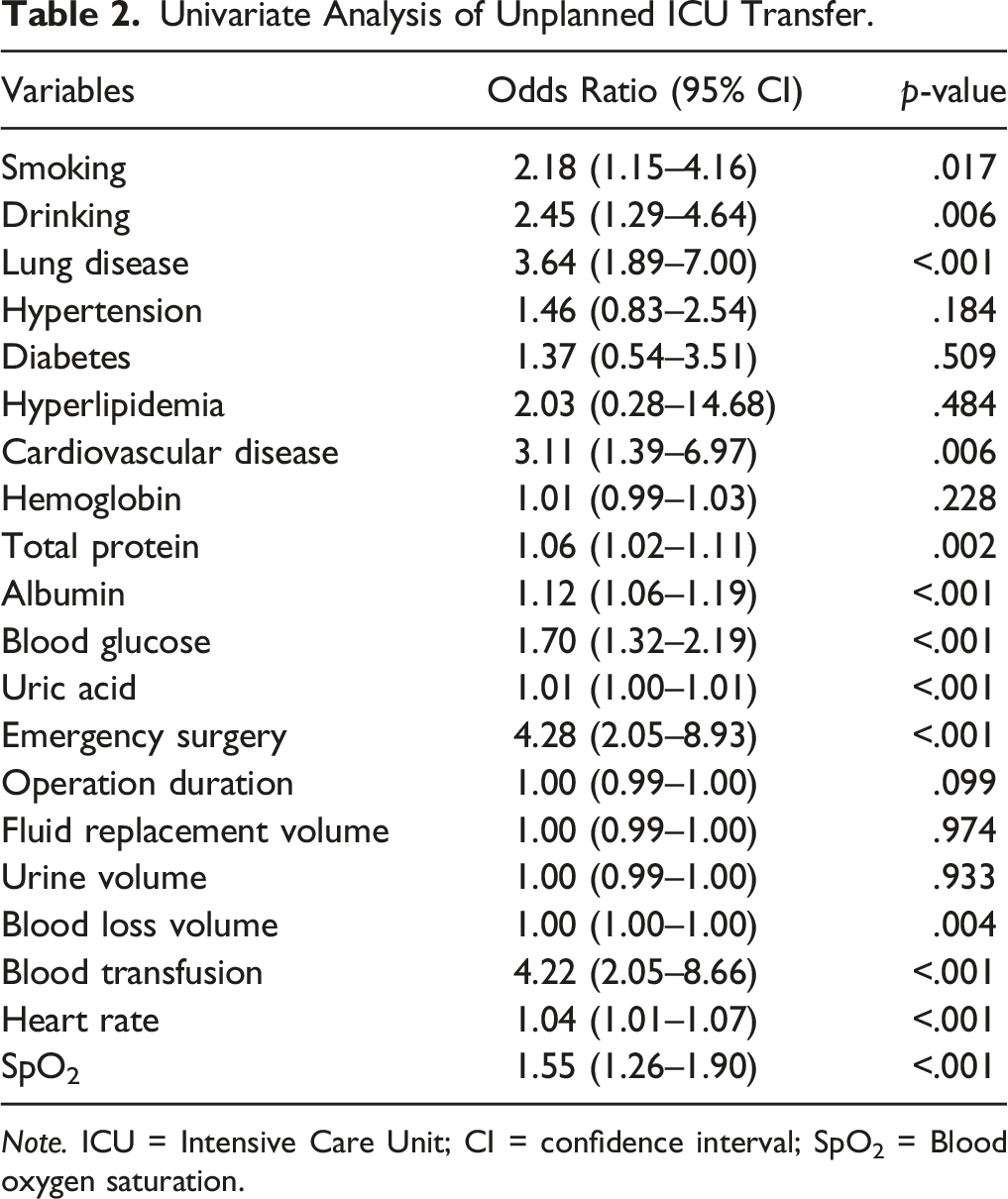
Note. ICU = Intensive Care Unit; CI = confidence interval; SpO2 = Blood oxygen saturation.
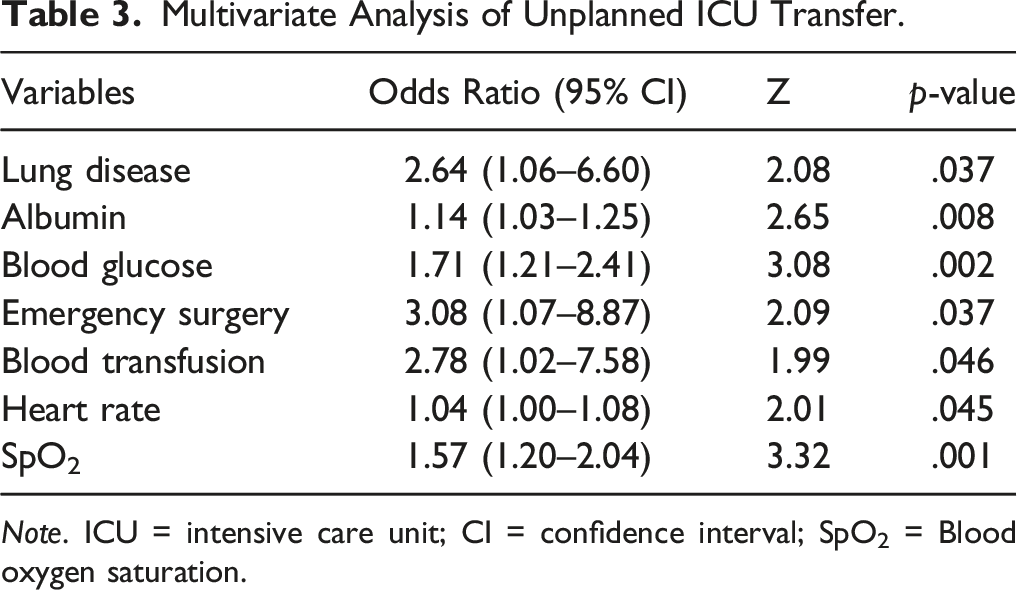
All variables at p < .1 in univariate analysis were further evaluated by multivariate logistic regression to assess independent risk factors for unplanned ICU transfer. Of the initial 20 variables, 7 remained in the final multivariate model. For example, lung disease: Odds Ratio [OR] = 2.64, 95% Confidence Interval [CI] = 1.06 - 6.60; albumin: Odds Ratio [OR] = 1.14, 95% CI = 1.03 - 1.25; emergency surgery: Odds Ratio [OR] = 3.08, 95% Confidence Interval [CI] = 1.07 - 8.87; blood transfusion: Odds Ratio [OR] = 2.78, 95% Confidence Interval [CI] = 1.02 - 7.58 (Figure 2) (Table 3). Forest plot for multivariate analysis of unplanned ICU transfers. Multivariate Analysis of Unplanned ICU Transfer. Note. ICU = intensive care unit; CI = confidence interval; SpO2 = Blood oxygen saturation.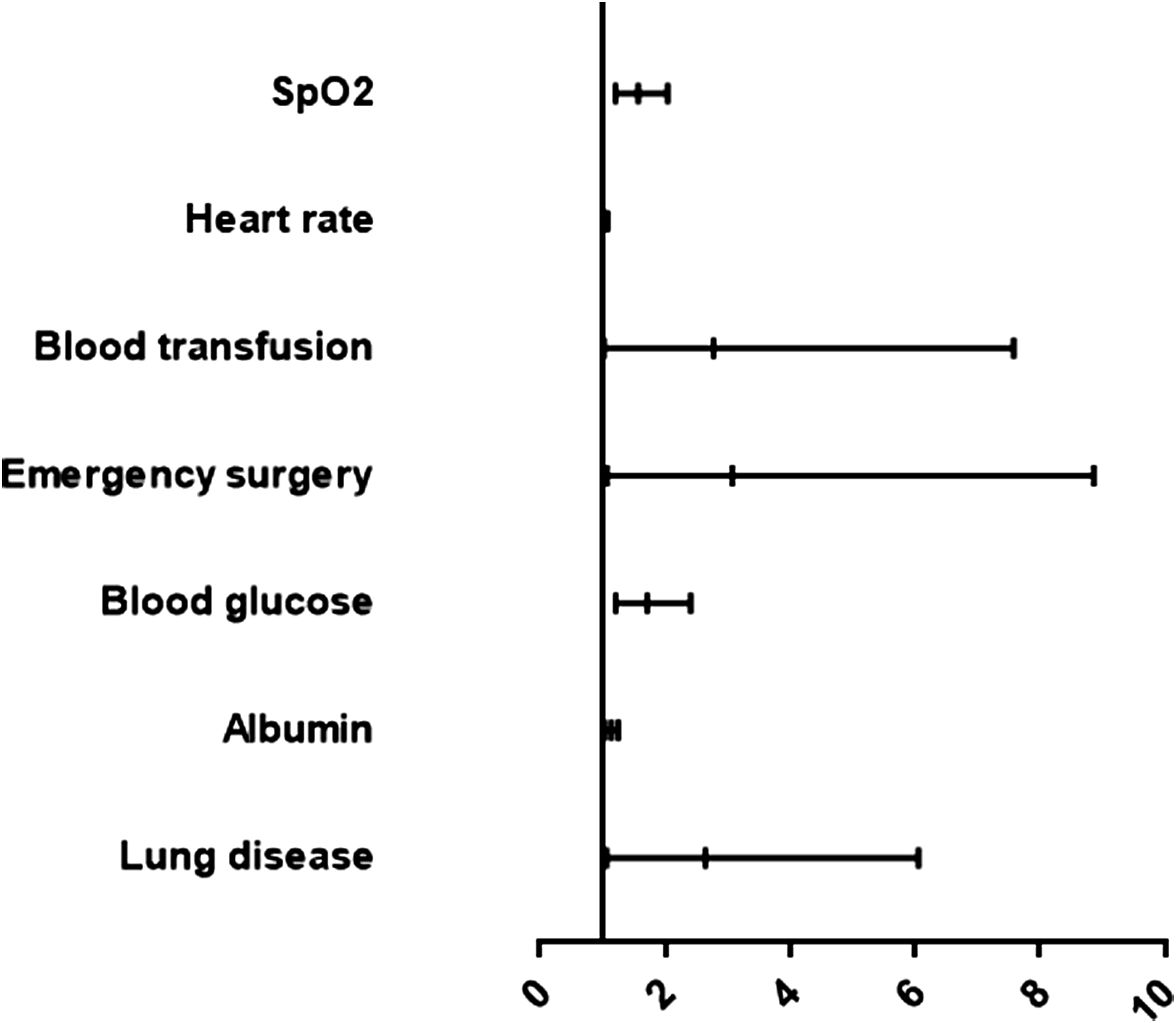
Discussion
This retrospective study aimed to explore the incidence and influencing factors of unplanned ICU transfer from PACU in patients undergoing cerebral surgery. Our study found that the independent risk factors for unplanned transfer from PACU to ICU in patients after brain surgery were the presence of lung disease, low albumin value, high blood sugar value, emergency surgery type, blood transfusion during operation, high heart rate value, and low blood oxygen saturation value. To the best of our knowledge, this is the first study to investigate the risk factors for unplanned ICU transfer from the PACU in patients undergoing cerebral surgery. This present study serves a reference for our next step in developing an electronic medical record system-based, large data-based intraoperative prediction model for unplanned ICU transfer of surgical patients.
We investigated 11,807 patients admitted to the PACU after cerebral surgery and found that 81 had unplanned ICU transfers, with an incidence rate of 0.686%. A study by Hines et al. involved 18,437 patients in the PACU recorded a total of 186 unplanned ICU admissions (1.01%) (Hines et al., 1992), and a study by Kluger et al. investigated 49,532 patients who were admitted to the PACU for observation and found that 184 had unplanned ICU transfers (0.4%) (Kluger & Bullock, 2002). Overall, the incidence of unplanned ICU transfer in PACU patients ranged from 0.4 to 1.01%. This is similar to the previously reported incidence of unplanned postoperative ICU transfer in adults (0.1–0.9%) (Da et al., 2013; Meziane et al., 2017; Petersen et al., 2017).
Our study showed that 76 patients with unplanned ICU transfer from the PACU had an average ICU length of stay of 10.84 days and an in-hospital mortality rate of 13.16%. A study by Mou et al. found that 40 patients who were unplanned transferred to the ICU by postoperative intermediate care units had an average ICU length of stay of 2.5 days and an in-hospital mortality rate of 12.5% (Fujii et al., 2016). Wanderer et al. reported that the average length of ICU stay was 5 days, and the in-hospital mortality rate was 5.6% in 4847 patients who were unplanned transferred to the ICU from the PACU (Wanderer et al., 2013). In contrast, the mean ICU length of stay for patients who were unplanned to be transferred to the ICU in our hospital was slightly higher than that in the other 2 studies, and the in-hospital mortality rate was similar to that in a certain study. This may be related to the different types of procedures that patients experience.
Some patients developed unplanned ICU transfers due to severe cerebral edema, bleeding, and malignant arrhythmias, and others developed unexplained cognitive dysfunction such as delirium, intense agitation, or somnolence. Six of the patients who developed unplanned ICU transfers required emergency intubation (7.89%), corresponding to 0.05% of all patients during the study period. Rose et al. found that of 21,457 patients under general anesthesia, 0.1% (n = 22) required emergency reintubation in the PACU (Rose, 1996). Bruins et al. reported that the emergency intubation rate in the PACU of their hospital was also 0.05% (25 out of 49,532 procedures) (Bruins et al., 2017). Peskett et al. found that patients required reintubation was 13 (0.08%) (11 out of 266 procedures) postoperatively (Peskett, 1999). In summary, the reintubation rate in PACU centers is approximately between 0.05 and 0.08.
Clinical and Research Implications
Unplanned postoperative ICU transfer is worse than planned postoperative ICU transfer for both patients and medical staff. Spontaneous ICU transfer after surgery challenges medical staff to adjust the allocation of ICU resources and psychologically burdens patients and their families. Furthermore, unplanned transfer to ICU usually lead to longer hospital stay, higher medical bills, and worse outcomes (Gold et al., 2015; Liu et al., 2012). Spontaneous ICU transfer also decrease the trust of patients and their families in medical staff (Jennerich et al., 2020).
Exploring the risk factors of unplanned transfer to ICU is of great significance to improve the awareness of both medical staff and patients and help them take preventive measures for potential risk factors. In the future, we hope to preoperatively stratify patients based on these factors to predict which patients will need a higher level of postoperative care. By preventing or predicting the need for unplanned transfer to ICU after surgery, we can better allocate ICU resources, reduce the morbidity and mortality of vulnerable patients, and ultimately improve the overall safety of cerebral procedures.
Strengths and Limitations
The study had limitations. First, this study was retrospective in nature; hence, all data collected were from cases and medical records. Second, the complete outcome of the patients was unclear, and further longitudinal studies may be needed. Third, was a single-centered study, and that the results may have been affected by regional characteristics, hospital policies, and types of surgical procedures provided by the hospital. Finally, this study aimed to explore risk factors; thus, the results might have been affected by the included variables.
Conclusion
The study identified independent risk factors for unplanned transfer from PACU to ICU after cerebral surgery by screening demographic data, laboratory tests, surgical and anesthesia-related information of patients undergoing cerebral surgery. Combining the results of the study with clinical practice in PACU can identify the possibility of unplanned ICU transfer from cerebral surgery patients who do not have an ICU appointment, providing guidance for accurately identifying the patient’s level of care.
Footnotes
Author Contributions
Qinqin,Cao contributed to conception and design contributed to acquisition, analysis, and interpretation drafted manuscript critically revised manuscript gave final approval agrees to be accountable for all aspects of work ensuring integrity and accuracy. Chengjuan, Fan contributed to conception contributed to acquisition and analysis drafted manuscript gave final approval agrees to be accountable for all aspects of work ensuring integrity and accuracy. Wei, Li contributed to acquisition drafted manuscript gave final approval agrees to be accountable for all aspects of work ensuring integrity and accuracy. Shuling, Bai contributed to analysis critically revised manuscript gave final approval agrees to be accountable for all aspects of work ensuring integrity and accuracy. Hemin, Dong contributed to acquisition critically revised manuscript gave final approval agrees to be accountable for all aspects of work ensuring integrity and accuracy. Haihong, Meng contributed to design contributed to analysis and interpretation drafted manuscript critically revised manuscript gave final approval agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was supported by the Jining Key Research and Development Program (Social People’s Livelihood) project (study code: 2020 YXNS003) hosted by the head nurse Haihong Meng and the “Miao Pu” program of the Affiliated Hospital of Jining Medical University (study code: MP-MS-2022-005) hosted by Hemin Dong.