
Abstract
Introduction
Overweight and obesity are among the most significant public health challenges of the 21st century, substantially increasing the risk of various chronic diseases (Mohammad Rahimi et al., 2022). By 2035, it is projected that over 50% of the global population will be overweight or obese, with significant implications for healthcare systems worldwide (World Obesity Federation, 2023). Obesity-related chronic conditions are particularly prevalent among women and are strongly associated with the development of metabolic syndrome, which can further result in type 2 diabetes, cardiovascular diseases, and non-alcoholic fatty liver disease (Flegal et al., 2016; Muscogiuri et al., 2024; Vardell, 2020). Since 1975, the global prevalence of overweight has nearly tripled, underscoring the urgent need for comprehensive interventions that not only target weight reduction but also aim to improve physiological and metabolic health markers (Ng et al., 2014; World Health Organization, 2024).
Overweight and obese individuals are at an elevated risk of developing steatosis, which can lead to impaired liver function (Chavarría-Arciniega et al., 2005). Liver enzymes such as alanine aminotransferase (ALT), aspartate aminotransferase (AST), and gamma-glutamyl transferase (GGT) are widely recognized as reliable biomarkers of liver injury, particularly in the context of non-alcoholic fatty liver disease (NAFLD) (Purcell et al., 2013; Whitfield, 2001). These enzymes are critical indicators of hepatocyte damage and are often elevated in NAFLD due to fat accumulation and inflammation in the liver (Younossi et al., 2016). The AST/ALT ratio is also a valuable metric, as a ratio greater than 1 may indicate more advanced liver damage, while alkaline phosphatase (ALP) levels can reflect biliary dysfunction or cholestasis, further complicating NAFLD progression (Angulo, 2002; Sanyal et al., 2021). Previous research has demonstrated significant associations between NAFLD and conditions such as insulin resistance, as well as components of metabolic syndrome, including hypertension, type 2 diabetes, and obesity (Cruz et al., 2015; Mohammad Rahimi & Attarzadeh Hosseini, 2022; Schindhelm et al., 2006).
Evidence supports lifestyle modifications—particularly diet and/or exercise—as effective first-line interventions for reducing both body weight in obese individuals, with multiple studies highlighting their beneficial impact on weight management and metabolic health (Garvey et al., 2016; Swift et al., 2018). Obesity management guidelines currently prioritize the volume of exercise—defined by both the frequency and duration of exercise sessions—over intensity. It is recommended that adults engage in at least 150–300 minutes of moderate-to-vigorous aerobic exercise per week for substantial weight loss, with some guidelines advising up to 300–420 minutes per week for more significant outcomes (Donnelly et al., 2009; Johnson et al., 2023; Liguori & Medicine, 2020; Piercy et al., 2018). Numerous reviews suggest that aerobic exercise is linked to decreases in visceral adipose tissue (Ohkawara et al., 2007; Verheggen et al., 2016). A recent review by Neeland et al. further estimated that a weight loss of approximately 5% achieved through these lifestyle interventions could lead to reductions in visceral adipose tissue of around 15%–25% (Neeland et al., 2019). Furthermore, a systematic review conducted by Smart et al. (2018) found that exercise training, even without accompanying dietary interventions, led to reductions in intrahepatic fat in adults who were overweight or had fatty liver disease (Smart et al., 2018).
In addition to lifestyle modifications such as exercise and dietary interventions, the use of dietary supplements has gained attention as an adjunct strategy for managing weight and improving metabolic health. Among these, Spirulina (Arthrospira platensis), a blue-green alga, has been widely recognized for its nutritional and therapeutic properties. Spirulina is rich in essential nutrients, including proteins, vitamins, minerals, and antioxidants, which may contribute to its potential effects on weight management, liver health, and physical performance (Sokary et al., 2024; Yousefi et al., 2019). Several mechanisms have been proposed to elucidate Spirulina’s role in weight loss. These include reducing macrophage infiltration into visceral adipose tissue, preventing liver fat accumulation, mitigating oxidative stress, enhancing insulin sensitivity, and improving satiety (Dąbrowska et al., 2024). Additionally, Spirulina’s high protein content and bioactive compounds, such as phycocyanin, may enhance cardiorespiratory fitness (CRF) by improving oxygen utilization, reducing exercise-induced oxidative stress, and supporting muscle recovery, potentially leading to improved endurance and aerobic capacity (Delfan et al., 2024). Studies have provided robust evidence for the benefits of Spirulina supplementation on various health outcomes. For example, research by Szulinska et al. (2017) demonstrated that daily supplementation with 2 g of Spirulina significantly improved the ratio of total antioxidant status and insulin sensitivity, with participants also experiencing reductions in body weight, BMI, and waist circumference. Similarly, Hernández-Lepe et al. (2018) observed that a higher dose of Spirulina (4.5 g per day) enhanced the synergistic effects of regular exercise, improving both body composition and cardiorespiratory fitness after a six-week regimen. In another study, it was found that consuming 1 g of Spirulina platensis daily over 12 weeks was effective in regulating weight and reducing appetite (Zeinalian et al., 2017). A recent meta-analysis by Zarezadeh et al. (2021) further confirmed that Spirulina supplementation significantly reduces body weight and waist circumference, supporting its role in obesity management (Zarezadeh et al., 2021).
The existing body of evidence suggests that Spirulina supplementation and aerobic physical exercise may positively influence key risk factors for cardiometabolic diseases, including insulin resistance, oxidative stress, liver function, and cardiorespiratory fitness, potentially aiding in the prevention of these conditions. Nevertheless, given the variability in results across studies, further randomized controlled trials are necessary to establish more conclusive findings regarding the combined impact of aerobic exercise and Spirulina supplementation on improving liver enzyme levels, body composition, and cardiorespiratory fitness in overweight adults. Therefore, this study seeks to address this gap by evaluating the impact of eight weeks of aerobic exercise combined with Spirulina supplementation on liver enzymes, body composition, and cardiorespiratory fitness in overweight and obese women.
Methods
Study Design
In this randomized, double-blind, placebo-controlled trial, 36 overweight and obese women (mean ± standard deviation [SD]; age: 35.2 ± 4.9 years; height: 160.8 ± 6.3 cm, body weight: 78.6 ± 8.4 kg; and BMI: 30.4 ± 2.3 kg/m2) were enrolled (Figure 1). The sample size was determined using G*Power software (version 3.1.9.7), based on a previous study by Hernández-Lepe et al. (2018), which reported a medium effect size (f = 0.25) for body composition changes with Spirulina and exercise. With an alpha of 0.05, power of 0.80, and four groups, a minimum of 36 participants (9 per group) was required to detect significant differences in primary outcomes (liver enzymes, body composition, and cardiorespiratory fitness). They were then randomly assigned to one of four groups: placebo with aerobic exercise (n = 9), spirulina with aerobic exercise (n = 9), spirulina (n = 9), and placebo (n = 9) groups. Flow diagram of how to enter, experimental course, and analysis of participants.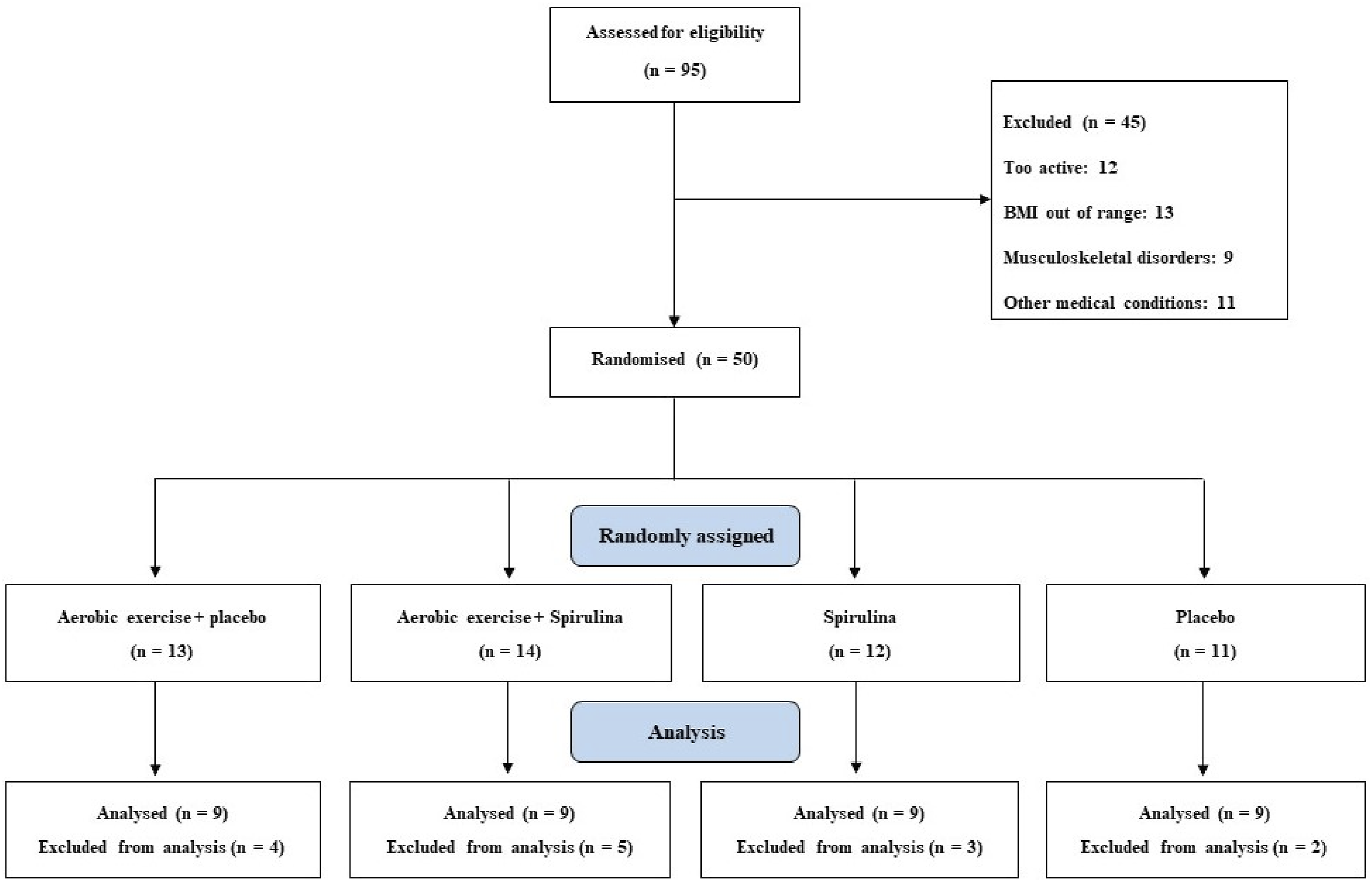
Recruitment took place at local community health centers and gyms in Mashhad, Iran, through flyers, social media announcements, and referrals from healthcare providers. Of 62 women screened between January and February 2024, 50 met the inclusion criteria, and 36 completed the study. Reasons for exclusion included BMI outside the range (n = 8), recent weight loss diets (n = 3), and medical contraindications (n = 1). Of the 50 enrolled, 14 were excluded post-randomization due to non-compliance with exercise sessions (n = 8), withdrawal due to personal reasons (n = 4), or incomplete data (n = 2).
The enrollment and interventions took place in Mashhad, Iran, between 3 March and 14 July 2024. Participants were included if they met the following criteria: BMI ≥ 25 kg/m2 and an age range of 25–40 years. They were excluded if they had a BMI < 25 or >35 kg/m2, were physically active, or had been on weight loss diets within the past three months. Additionally, participants were excluded for having medical conditions that contraindicated physical activity, a history of kidney disease, atherosclerosis, cancer, acute infections, recent surgeries, or for the use of hormonal medications, vitamins, and mineral supplements within the past three months. Pregnancy, lactation, menopause, and adherence to any specific diet were also grounds for exclusion. Participants who missed more than three exercise sessions during the study were removed from the analysis.
The protocol for the current randomized controlled trial was approved by the Ethics Committee of Khayyam University, Mashhad, Iran (Registration number: IR.KHAYYAM.REC.1403.015). Participants were informed about the study’s objectives and were given a 10-day period prior to the trial to confirm their participation. Written informed consent was obtained from all participants.
Randomization was performed using a computer-generated random number sequence (Random Allocation Software, version 1.0), with participants allocated to groups in a 1:1:1:1 ratio by an independent researcher blinded to participant identities. Group assignments were concealed in sealed, opaque envelopes opened only at the time of intervention assignment. The study fowchart is displayed in Figure 1.
Interventions
The aerobic exercise regimen was performed for eight weeks, consisting of three sessions per week, each lasting 40–50 minutes. The 8-week intervention duration was chosen based on previous studies demonstrating significant changes in liver enzymes, body composition, and cardiorespiratory fitness within this timeframe (Hernández-Lepe et al., 2018; Szulinska et al., 2017), balancing efficacy with participant adherence and resource availability. Each session began with a 10-min warm-up that included walking, jogging, stretching, and mobility exercises. The main aerobic activity lasted 30–40 minutes and was conducted in a standing position, with intensity gradually increasing. The sessions started at 60% of the maximum heart rate and progressively increased to 75% by the final sessions. At the end of each session, participants spent 5–10 minutes cooling down. Training intensity was monitored using a Polar heart rate monitor (Izadi Ghahfarokhi et al., 2015; Jurca et al., 2004).
All exercise sessions were carried out at Neshat Sport Gymnasium in downtown Shandiz, Mashhad, Iran, under the supervision of an exercise specialist. Participants who missed more than 20% of the sessions were excluded from the study. Notably, the exercise sessions were conducted in the morning at 10:00 a.m., approximately 3 hours after breakfast, with participants having lunch 1 hour afterward.
In the spirulina with aerobic exercise and spirulina-only groups, participants received a daily dose of Spirulina platensis (Rayhan Naqsh-e-Jahan Company, Iran) in two 500 mg tablets, taken twice per day. The Spirulina used was certified by the manufacturer for purity, with a guaranteed minimum of 60% protein and 1% phycocyanin, consistent with formulations used in prior studies (e.g., Zeinalian et al., 2017). The manufacturer provided a certificate of analysis confirming the absence of heavy metals and microbial contaminants. Conversely, the placebo with aerobic exercise and placebo-only groups were administered two pills daily, each containing one gram of starch, designed to resemble the spirulina tablets in appearance and shape but lacking chlorophyll. To ensure compliance, participants returned unused tablets weekly, and pill counts were recorded by a blinded study coordinator in addition to weekly phone calls. Additionally, they were asked about their adherence to their regular diet. Participants were instructed to avoid taking any mineral or vitamin supplements and to maintain their usual dietary habits throughout the study period (Zeinalian et al., 2017).
Measurement
The study administrator, blinded to the group allocation, assessed body weight, height, and BMI both at baseline and after eight weeks. All measurements were taken in duplicate by trained personnel, with the final value being the average of the two readings. Participants’ height (cm) and body weight (kg) were measured using a digital stadiometer (Seca, Hamburg, Germany) and a digital scale (Beurer PS 07, Ulm, Germany) to the nearest 0.1 cm and 0.1 kg, respectively. BMI was calculated as body weight (kg) divided by height squared (m2). The Inbody 720 Body Composition Analyzer (Biospace, Dogok-dong, South Korea) was applied to evaluate bioimpedance parameters, including body fat mass, percentage body fat, skeletal muscle mass. The Inbody 720 has demonstrated high reliability (ICC > 0.9) and validity (r > 0.8) for body composition measurements compared to dual-energy X-ray absorptiometry (McLester et al., 2020). Waist-to-hip ratio was calculated by measuring waist circumference at the midpoint between the lower rib margin and iliac crest and hip circumference at the widest point over the greater trochanters, using a non-stretchable tape measure to the nearest 0.1 cm, with measurements averaged from two readings.
A 3-day food diary was employed to monitor energy and macronutrient intake at baseline and at the 8-week follow-up to ensure dietary consistency across groups. Data were analyzed using Food Processor SQL 2006 (ESHA Research, Salem, OR, USA) to calculate total energy, carbohydrate, protein, and fat intake. No significant changes in dietary patterns were observed, confirming that outcomes were not confounded by dietary variations. A dietitian provided guidance on the adequacy of the participants’ diets, emphasizing energy-dense foods as well as those with lower nutritional value. Participants were asked to document their food intake for 3 days before the baseline assessment, using food composition analysis software (Food Processor SQL 2006; ESHA Research, Salem, OR, USA), and to repeat the same dietary tracking process prior to the follow-up at eight weeks.
Cardiorespiratory fitness (VO2max) was estimated using a validated algorithm developed by Jackson and colleagues (1990), which incorporates self-reported physical activity (SRPA), BMI, age, and gender. The equation is as follows:

The SRPA questionnaire, adapted from the Physical Activity Rating (PA-R) scale, asked participants to rate their physical activity over the past month on a 0–7 scale, ranging from no regular activity to vigorous activity ≥5 hours/week (Jackson et al., 1990). This non-exercise model was chosen due to resource constraints, as direct VO2max testing (e.g., treadmill or cycle ergometry) was not feasible in this preliminary study. While less precise than direct measures, the model has acceptable validity (r = 0.65–0.78) for population-based studies and was deemed appropriate given the study’s focus on relative changes (Jurca et al., 2005). A systematic review confirmed that this method has the highest scores compared to other non-exercise fitness prediction models (Maranhão Neto et al., 2004).
Twelve-hour fasting blood samples were collected before beginning the study regimen and at the end of 8 weeks of the regimen. Participants were instructed to refrain from physical activity and medication intake during the 24 hours prior to blood sampling. Blood for liver enzyme analysis (ALT, AST, ALP) was drawn between 08:00 and 10:00 a.m. following a 5-min rest in the supine position. Normal reference ranges for liver enzymes were as follows: ALT (7–45 U/L), AST (10–40 U/L), ALP (44–147 U/L). A 20-mL venous blood sample was obtained from the antecubital vein into a tube containing K2EDTA, and the sample was left to clot at room temperature for 15 minutes. Afterward, blood cells were separated by centrifugation at 3000 g for 10 minutes. Liver enzyme concentrations were measured using Pars-Azmun kits (Tehran, Iran) with an enzymatic method, in accordance with the manufacturer’s instructions.
Statistical Analysis
Data analysis was conducted using SPSS software (version 27, SPSS Inc, Chicago, IL, USA). The Shapiro–Wilk test was used to assess the normality of the data distribution. Data are expressed as mean ± SD for normally distributed data and median (interquartile range) for non-normally distributed data. Baseline group comparisons were performed using one-way ANOVA, while the Kruskal–Wallis test was applied for non-normally distributed variables. Within-group changes following the intervention were evaluated using paired sample t-tests, with the Wilcoxon signed-rank test used for non-normally distributed data. Repeated measures ANOVA or Kruskal–Wallis tests were employed to analyze changes between groups at post-intervention. Additionally, the Mann–Whitney test was used to compare each pair of groups for non-normally distributed data. For normally distributed data, if the interaction effect was significant, post hoc pairwise comparisons were conducted using Bonferroni’s test to analyze differences at various time points between each pair of groups. A significance level of p < .05 was considered statistically significant.
Results
Baseline Characteristics (Mean ± SD) of Study Participants (n = 9 per Group), (p > .05).
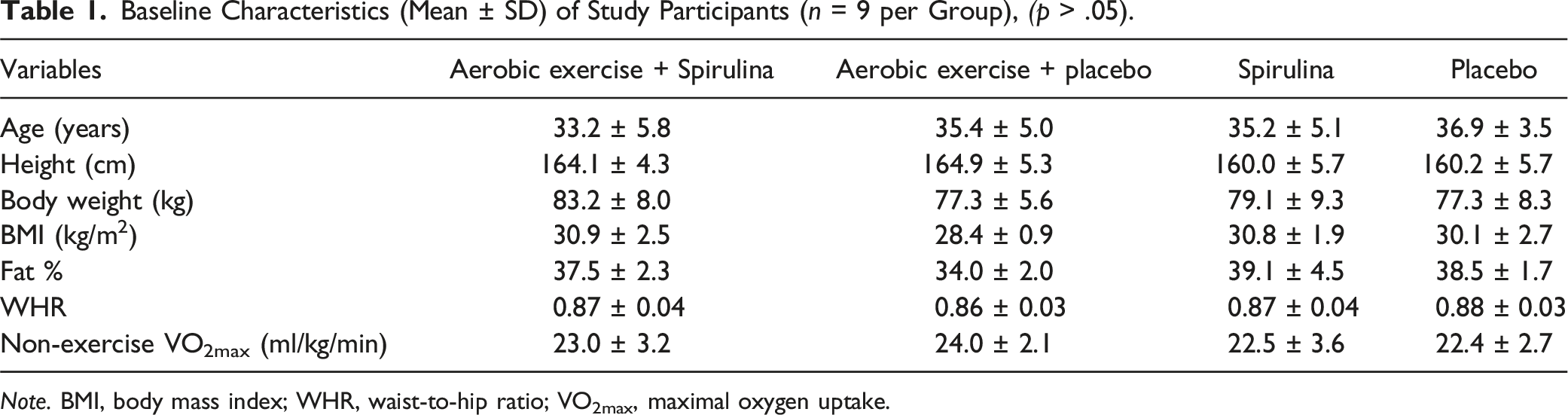
Note. BMI, body mass index; WHR, waist-to-hip ratio; VO2max, maximal oxygen uptake.
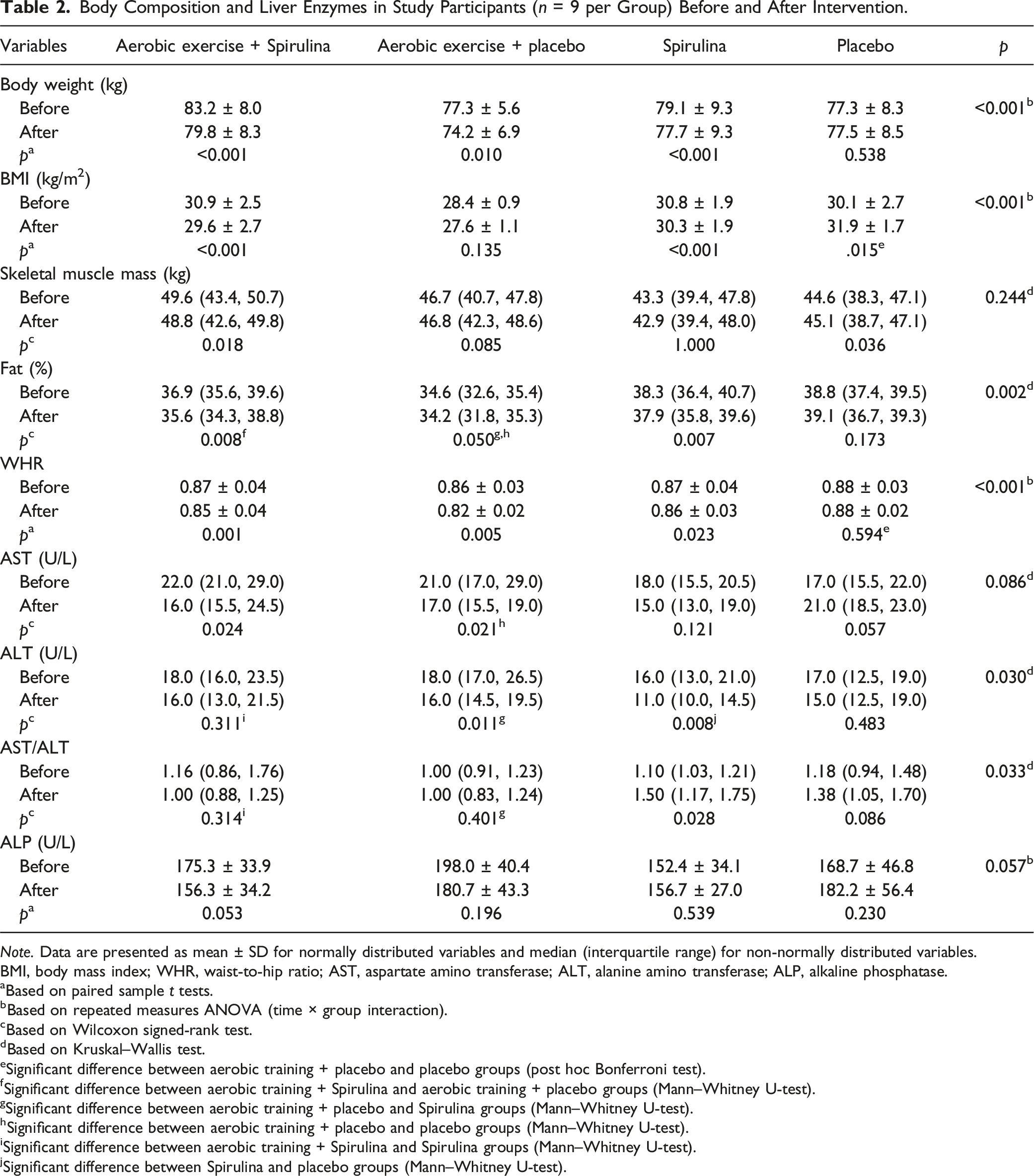
Body Composition and Liver Enzymes in Study Participants (n = 9 per Group) Before and After Intervention.
Note. Data are presented as mean ± SD for normally distributed variables and median (interquartile range) for non-normally distributed variables.
BMI, body mass index; WHR, waist-to-hip ratio; AST, aspartate amino transferase; ALT, alanine amino transferase; ALP, alkaline phosphatase.
aBased on paired sample t tests.
bBased on repeated measures ANOVA (time × group interaction).
cBased on Wilcoxon signed-rank test.
dBased on Kruskal–Wallis test.
eSignificant difference between aerobic training + placebo and placebo groups (post hoc Bonferroni test).
fSignificant difference between aerobic training + Spirulina and aerobic training + placebo groups (Mann–Whitney U-test).
gSignificant difference between aerobic training + placebo and Spirulina groups (Mann–Whitney U-test).
hSignificant difference between aerobic training + placebo and placebo groups (Mann–Whitney U-test).
iSignificant difference between aerobic training + Spirulina and Spirulina groups (Mann–Whitney U-test).
jSignificant difference between Spirulina and placebo groups (Mann–Whitney U-test).
For AST and ALP, no significant differences were observed among the groups. However, within-group analysis for AST revealed significant reductions post-intervention in the aerobic exercise + spirulina group (p = .024) and aerobic exercise + placebo group (p = .021), while no significant changes were detected in the other two groups (p > .05). In contrast, for ALP, no significant within-group changes were observed in any of the groups post-intervention.
There was a significant group × time interaction for body weight, BMI, and WHR (p < .001 for all). Body weight significantly decreased from baseline to post-intervention in the aerobic training + placebo, spirulina + aerobic training, and spirulina-alone groups (p < .001). The greatest reduction in body weight was observed in the aerobic training + spirulina group (p = .010), followed by the aerobic training + placebo group (p < .001). No significant change in body weight was observed in the placebo-alone group (p = .538).
Regarding BMI, significant reductions were observed in the aerobic training + Spirulina group (p < .001) and aerobic training + placebo group (p < .001). In contrast, the placebo-alone group exhibited a significant increase in BMI (p = .015), which was significantly different from the aerobic training + placebo group. No significant change in BMI was detected in the Spirulina-alone group (p = .135).
Furthermore, WHR significantly decreased in the aerobic training + placebo group (p = .001), the spirulina + aerobic training group (p = .005), and spirulina-alone group ( p = .023). No significant change was detected in the placebo-alone (p = .594). Post hoc analysis revealed that BMI and WHR significantly differed between the aerobic training + placebo and placebo groups (Table 2).
In terms of fat percentage, significant reductions were observed in the aerobic training + spirulina group compared with the aerobic training + placebo group, as well as in the aerobic training + placebo group compared with the spirulina group. Additionally, the decrease in fat percentage in the aerobic training + placebo group was significantly greater compared with the placebo-alone group.
Although significant within-group changes in skeletal muscle mass were noted in the aerobic training + placebo group (p = .018) and placebo-alone group (p = .036), no significant changes were observed in the spirulina + aerobic training (p = .085) and spirulina-alone groups (p = 1.000) (Table 2).
The changes in VO2max are illustrated in Figure 2. Within-group analysis revealed significant improvements in VO2max for the aerobic training + placebo, spirulina + aerobic training, and spirulina-alone groups (p < .001 for all), while no significant change was detected in the placebo-alone group (p > .05). Additionally, the group × time interaction analysis was significant (p < .001). However, post hoc analysis revealed no meaningful differences between the groups. Changes (mean ± SD) in non-exercise VO2max before and after intervention. *Significant difference (p < .05) between pre- and post-intervention values.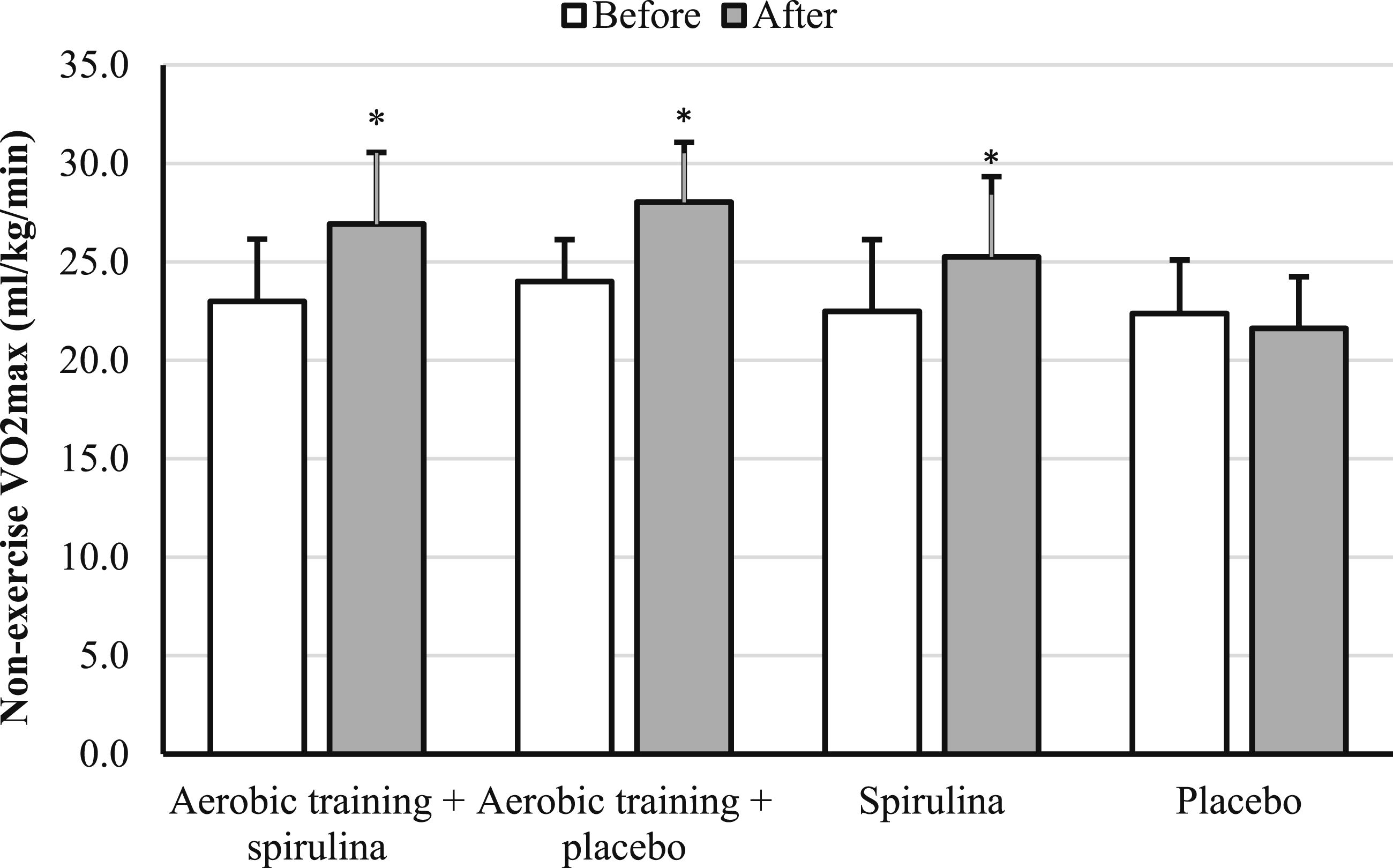
Discussion
The present study evaluated the effects of eight weeks of aerobic exercise combined with spirulina supplementation on liver enzymes, body composition, and cardiorespiratory fitness in overweight and obese adult women. Our findings underscore notable within- and between-group differences in various outcomes, highlighting the potential efficacy of a combined regimen of aerobic exercise and spirulina supplementation in improving specific health markers.
Our findings indicate that serum ALT levels significantly decreased in both the aerobic training + placebo and Spirulina-alone groups, with the Spirulina group demonstrating markedly greater reductions (p < .01). The AST/ALT ratio improved significantly only in the Spirulina group, surpassing the changes observed in both the aerobic training + placebo and aerobic training + Spirulina groups (p = .033). Significant reductions in AST were observed in both the aerobic training + Spirulina (p = .024) and aerobic training + placebo groups (p = .021); however, no significant changes were noted in ALP across or within any groups. Notably, baseline AST (10–40 U/L) and ALT (7–45 U/L) levels were within normal ranges for all groups, and post-intervention changes (e.g., 3–5 U/L reductions in ALT) remained within these ranges. While statistically significant, these small changes may have limited clinical relevance in women with normal liver function, as they do not indicate a shift from pathological to normal states. However, such reductions could reflect early improvements in liver health, potentially beneficial for preventing NAFLD progression in at-risk populations (Younossi et al., 2016). These findings align with prior studies highlighting Spirulina as an effective dietary supplement for lowering liver enzymes in patients with NAFLD. For instance, a six-month intervention with spirulina (6 g/day) resulted in decreased levels of AST, ALT, and glutamyltransferase among adults with NAFLD (Mazokopakis et al., 2014). In women with normal liver function, short-term (8–12 week) Spirulina supplementation (1–2 g/day) has shown modest reductions in ALT and AST (typically 2–4 U/L), often attributed to its antioxidant and anti-inflammatory properties, though clinical significance remains uncertain due to the absence of pathological baseline values (Zeinalian et al., 2017). Spirulina’s hepatoprotective effects are likely mediated by its antioxidant, anti-inflammatory, and lipid-lowering properties (Deng & Chow, 2010). Furthermore, Spirolina’s ability to support the growth of beneficial intestinal microflora and exhibit probiotic-like effects may contribute to its impact on liver function by modulating gut-liver interactions (Prete et al., 2024). However, further research is needed to clarify these mechanisms more definitively.
Exercise training independently demonstrated significant effects on liver enzymes, particularly in reducing AST. These findings are consistent with previous studies indicating that exercise reduces hepatic lipid accumulation, enhances insulin sensitivity, and improves blood lipid profiles. Early research often combined exercise training with dietary changes or weight loss, making it difficult to isolate the independent effects of exercise alone. However, recent high-quality studies have clarified that exercise training can independently affect liver fat content. These studies have also started to explore the underlying mechanisms behind these changes, indicating that exercise alone can positively impact liver function, reducing lipid accumulation and improving metabolic health markers such as insulin sensitivity and blood lipids (Gao et al., 2021; Mohammad Rahimi & Attarzadeh Hosseini, 2022).
Significant improvements in body composition were observed, particularly reductions in body weight, BMI, and WHR, in groups undergoing aerobic training, with or without Spirulina supplementation. The aerobic training + Spirulina group exhibited the greatest reductions in body weight (p < .001), followed by the aerobic training + placebo group (p = .010), consistent with well-established evidence of aerobic exercise’s efficacy in reducing adiposity and improving metabolic health (Swift et al., 2018). The additional benefits observed in the spirulina + aerobic training group may be attributed to Spirulina’s potential to enhance lipid metabolism and antioxidant capacity, as supported by prior research (Calella et al., 2022). Notably, the Spirulina-alone group exhibited a reduction in WHR (p = .023), suggesting modest effects on fat distribution independent of exercise, although the absence of significant BMI changes (p = .135) emphasizes the necessity of combining dietary supplementation with exercise for more pronounced results.
Contrary to expectations, skeletal muscle mass showed significant within-group increases only in the aerobic training + Spirulina (p = .018) and placebo-alone groups (p = .036), with no notable changes in the aerobic training + placebo (p = .085) and Spirulina-alone groups (p = 1.000). This result diverges from earlier studies suggesting Spirulina supplementation may promote muscle protein synthesis and recovery (Hernández-Lepe et al., 2018). Differences in dosage, intervention duration, or participant characteristics may explain this discrepancy. Additionally, the greater reductions in fat percentage in the aerobic training + spirulina group compared to other groups suggest a synergistic mechanism, potentially mediated by enhanced mitochondrial efficiency and oxidative capacity from the combined intervention. Future research is warranted to explore the differential effects of Spirulina on muscle mass and body composition across diverse populations and protocols.
The observed improvements in VO2max the aerobic training + placebo, Spirulina + aerobic training, and Spirulina-alone groups (p < .001) indicate that both exercise and Spirulina supplementation independently contribute to enhanced cardiorespiratory fitness. Aerobic training’s impact on VO2max aligns with extensive evidence of its role in augmenting cardiovascular efficiency, increasing mitochondrial density, and improving oxygen utilization (Chaouachi et al., 2022). Similarly, the Spirulina-alone group’s improvement supports findings that Spirulina enhances aerobic performance by reducing oxidative stress, mitigating inflammation, and improving hemoglobin oxygen-carrying capacity (Han et al., 2021). Despite significant within-group improvements, the lack of meaningful differences between groups in the post hoc analysis suggests that Spirulina and aerobic exercise may exert overlapping rather than additive effects on VO2max. This aligns with prior research indicating that Spirulina’s benefits on endurance may plateau when combined with already effective interventions like aerobic training (Calella et al., 2022). The absence of improvement in the placebo-alone group reinforces the necessity of targeted interventions, such as structured exercise or supplementation, to elicit significant gains in cardiorespiratory fitness. Future studies should investigate optimal dosing, timing, and interaction effects of Spirulina and exercise to maximize benefits on VO2max.
Strengths and Limitations
This study possesses several notable strengths. First, the randomized, double-blind, placebo-controlled design enhances the validity and reliability of the findings by minimizing biases related to group allocation and participant or investigator expectations. Second, the inclusion of multiple intervention arms, including combinations of aerobic exercise and Spirulina supplementation, allows for a nuanced understanding of their independent and combined effects on liver enzymes, body composition, and cardiorespiratory fitness. Third, the rigorous methodological approach, including standardized measurement protocols, supervised exercise sessions, and compliance monitoring for supplementation, ensures the consistency and robustness of data collection. Additionally, the study’s focus on overweight and obese women, a population with a high prevalence of metabolic disorders, provides valuable insights into targeted interventions for improving metabolic health, even in those with normal baseline liver function (Younossi et al., 2016). Finally, the use of validated tools for assessing body composition and VO2max contributes to the reliability and reproducibility of the results.
Despite its strengths, this study is not without limitations. The relatively small sample size (n = 36) limits the generalizability of the findings and may reduce the power to detect smaller effect sizes, particularly for outcomes with modest changes like liver enzymes in participants with normal baseline values. The short duration of the intervention (eight weeks) restricts conclusions about the long-term effects of aerobic exercise and Spirulina supplementation. The short intervention period may also have contributed to the minimal changes observed in some outcomes, such as ALP and skeletal muscle mass, which may require longer durations to manifest significant effects (Yousefi et al., 2019). Moreover, while the study employed rigorous blinding and placebo controls, potential unreported dietary or lifestyle variations among participants might have influenced the outcomes. The reliance on self-reported dietary adherence and physical activity data could introduce recall or reporting bias. Additionally, the estimation of VO2max using a non-exercise prediction model, though validated, may lack the precision of direct cardiopulmonary exercise testing, potentially underestimating or overestimating fitness changes (Jurca et al., 2005). Future studies with larger sample sizes, extended follow-up periods, and direct physiological measurements are needed to confirm and expand upon these findings.
Conclusion
This study provides valuable insights into the combined and independent effects of aerobic exercise and Spirulina supplementation on liver enzymes, body composition, and VO2max in overweight and obese women. The findings suggest that while Spirulina supplementation and aerobic exercise elicit statistically significant improvements in specific health markers, such as ALT and fat distribution, the clinical relevance of small changes in normal-range liver enzymes remains limited. Nevertheless, these changes may contribute to early prevention of metabolic disorders in at-risk populations. Aerobic exercise remains a cornerstone for improving overall metabolic health and cardiorespiratory fitness. Further research is essential to elucidate the underlying mechanisms, optimize intervention strategies, and assess long-term outcomes in diverse populations.
Footnotes
Acknowledgments
We would like to express our sincere gratitude to all the patients who participated in this study. Their cooperation and contributions were essential to the success of this research.
Author Contributions
Haniyeh Akbarzadeh Khadri contributed to conception and design drafted manuscript gave final approval agrees to be accountable for all aspects of work ensuring integrity and accuracy Rokhsare Fazolahzade Mousavi contributed to conception and design critically revised manuscript gave final approval agrees to be accountable for all aspects of work ensuring integrity and accuracy Ladan Hosseini Abrishami contributed to data acquisition, analysis, and interpretation drafted manuscript gave final approval agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.