
Abstract
Keywords
Introduction
Preterm infants have an underdeveloped immune system and an aberrant inflammatory response, placing them at risk for adverse outcomes (Sharma et al., 2012). This vulnerable population exhibits elevated intestinal inflammation that is associated with growth faltering (Thai et al., 2022), necrotizing enterocolitis (NEC; Schurink et al., 2015), and sepsis (Humberg et al., 2020), all of which contribute to an increased risk of infant morbidity and mortality (Humberg et al., 2020). An important factor that may be associated with intestinal inflammation is systemic inflammation, which has been shown to contribute to adverse outcomes in preterm infants (Humberg et al., 2020; Kuban et al., 2017).
Intestinal fatty acid binding protein (I-FABP), expressed in small-intestinal enterocytes, is released into the bloodstream following mucosal injury or increased intestinal permeability and subsequently excreted in urine. Serum I-FABP has been shown to rise in neonates with intestinal ischemic injury and NEC, supporting its role as a biomarker of intestinal wall integrity and inflammation (Chen et al., 2024). More recently, urinary I-FABP has emerged as a convenient, non-invasive measure of compromised gut integrity and intestinal inflammation (Jung et al., 2021; Kokesova et al., 2019; Schurink et al., 2015), and has been investigated as a diagnostic marker for NEC (Coufal et al., 2020). Despite these advances, it remains unclear whether urinary I-FABP can act as a precursor to systemic inflammation in preterm infants.
To improve the prognosis and long-term health of preterm infants, a better understanding of the relationship between intestinal and systemic inflammation is needed. Therefore, we aimed to examine the association between urinary I-FABP and systemic inflammation and to further evaluate whether intestinal inflammation may serve as a precursor to systemic inflammation. We hypothesized that elevations in urinary I-FABP would precede increases in systemic inflammatory markers, and that clarifying this relationship may inform future work aimed at early identification and prevention of systemic inflammation, which has been associated with adverse clinical outcomes in preterm infants.
Methods
Study Population
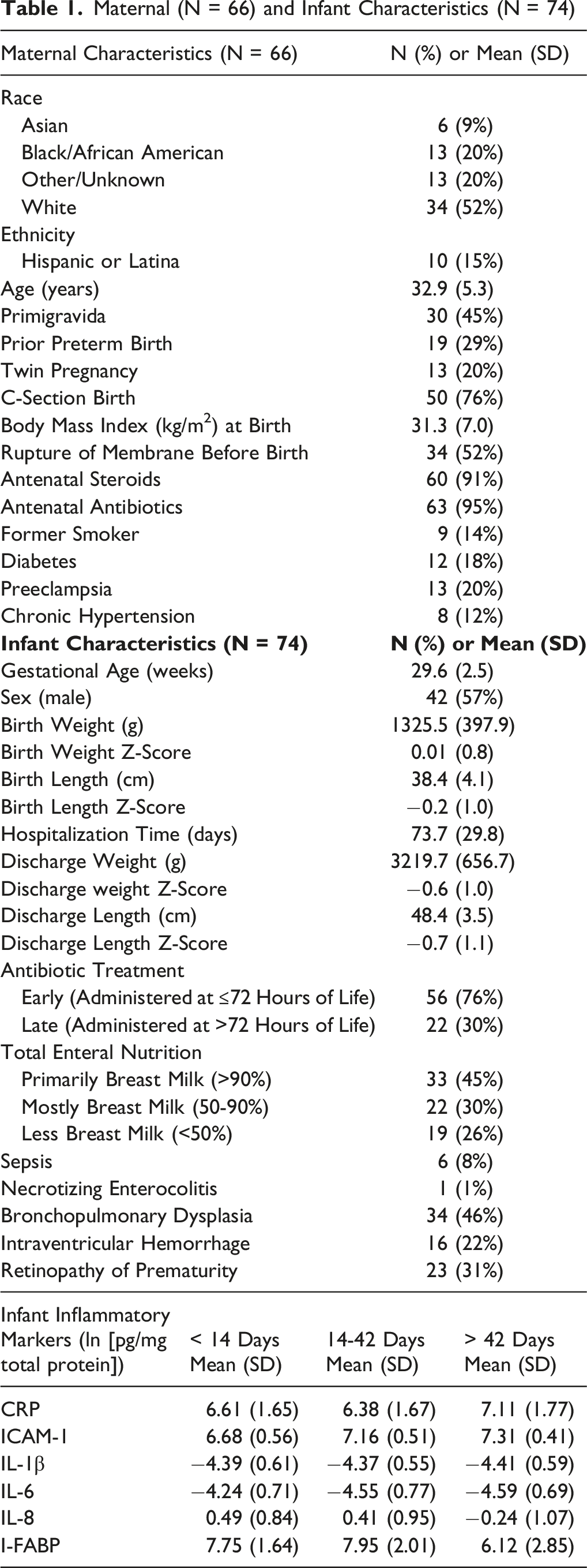
Maternal (N = 66) and Infant Characteristics (N = 74)
Urine Collection and Measurement of Urinary I-FABP, a Marker of Intestinal Inflammation
Urine samples were collected throughout the infants’ NICU hospitalization as previously described (Thai et al., 2022). Briefly, a cotton ball was placed inside the infant’s diaper to collect urine, which was then transferred into a microcentrifuge tube and stored at −80°C within 48 hours of collection until processing. Urinary I-FABP levels were measured using ELISA from diluted urine samples. I-FABP was normalized to total protein content in urine and expressed in pg/mg of total protein. I-FABP was analyzed using the natural logarithm (ln) transformed values.
Urinary I-FABP was evaluated as a biomarker of intestinal epithelial injury. I-FABP serves as an indicator of enterocyte damage and reflects intestinal epithelial damage with potential downstream effects on systemic inflammatory signaling. There are currently no validated reference ranges for I-FABP. Specifically, urinary I-FABP as a diagnostic threshold for intestinal inflammation in preterm infants still lacks validated, evidence-based, gestational-age-specific reference ranges. Reported values vary widely by gestational age, postnatal age, sample matrix (serum, plasma, or urine), and assay methodology. For example, Reisinger et al. observed markedly higher urinary I-FABP levels in extremely preterm infants compared with moderately preterm and term infants, underscoring physiologic variability with maturation (Reisinger et al., 2014). In the absence of a standard cutoff, I-FABP was treated as a continuous, protein-normalized variable and evaluated using cohort-specific temporal trends. This approach is consistent with previous neonatal studies that have used within-cohort comparisons to characterize intestinal inflammation in preterm populations (Coufal et al., 2020; Jung et al., 2021; Reisinger et al., 2014). Samples in our study were collected throughout hospitalization, within 20 weeks postnatal age, with repeated sampling per infant when clinically feasible. Grouped mean (SD) values for I-FABP are reported in Table 1 to provide a simplified summary of biologically relevant hospitalization periods, including the first two weeks of life, a period of early physiologic instability; weeks 2–6, representing a transitional phase; and a later period beyond 6 weeks of hospitalization, reflecting greater physiologic stability. Weekly mean (SD) values for I-FABP over the course of hospitalization are reported in Supplemental Table 1.
Dried Blood Spot Collection and Measurement of Systemic Inflammatory Markers
Blood samples were collected throughout the infants’ NICU hospitalization period. Blood spots were collected for research on filter paper (Whatman 903 Protein Saver Card) alongside clinically indicated blood draws, air-dried overnight at room temperature, sealed in a polyethylene bag with a desiccant packet, and stored at −80°C until processing. We used established methods to elute protein from the dried blood spots (Fichorova et al., 2011). Briefly, filter paper was treated with elution buffer, centrifuged, and filtered to collect eluted proteins. Concentrations of acute-phase proteins (C-Reactive Protein [CRP]), adhesion molecules (Intercellular Adhesion Molecule-1 [ICAM-1]), and cytokines (Interleukin [IL]-1β, IL-6, and IL-8) were measured using the Meso Scale Discovery Multiplex Platform and Sector Imager, adjusted to pg/mg of total protein, and analyzed using the ln-transformed values, as previously described (Fichorova et al., 2011). Samples were collected within 20 weeks postnatal age with repeated sampling per infant when clinically feasible.
Systemic inflammatory markers included CRP, a downstream hepatic acute-phase reactant with delayed kinetics that may limit sensitivity to early inflammatory processes; ICAM-1, an adhesion molecule that facilitates leukocyte adhesion and migration and contributes to both normal immune development and pathologic inflammatory responses; and the proinflammatory cytokines IL-1β, IL-6, and IL-8, which are involved in inflammatory signaling, with IL-6 used as a biomarker of neonatal sepsis and IL-8 functioning as a proinflammatory chemokine.
Similar to I-FABP, there are no standard validated and gestational-age-specific reference values for many systemic inflammatory markers, including ICAM-1, IL-1β, IL-6, and IL-8, to denote inflammation among preterm infants. Although CRP has reported reference intervals for preterm infants during the early neonatal period (Chiesa et al., 2011), its use in clinical practice remains highly variable (Barboza et al., 2024) and it is generally not recommended as a standalone marker for the evaluation of early-onset sepsis (Puopolo et al., 2018). We therefore analyzed all inflammatory markers as continuous variables and interpreted them relative to age-related trends within our cohort, which reflects a representative sample of preterm infants cared for in a tertiary-level NICU. Grouped mean (SD) values for systemic inflammatory markers are reported in Table 1 to provide a simplified summary of biologically relevant hospitilization periods as previously mentioned. Weekly mean (SD) values for systemic inflammatory markers over the course of hospitalization are reported in Supplemental Table 1.
Statistical Analyses
All statistical analyses were conducted using R statistical software (version 4.2.1). We report beta (ß) coefficients, 95% confidence intervals (CI), and p-values for all linear models, with significance set at p < 0.05. Unadjusted linear mixed-effects models with random intercepts for infant ID were used to account for repeated measurements. Additionally, because analyses were conducted using postnatal age in weeks, we stratified infants into three gestational age groups to account for differences in physiological maturity and clinical characteristics. Specifically, infants were stratified according to prior analytical approaches (Thai et al., 2022) and WHO guidelines (de Costa et al., 2021) as extremely preterm (<28 weeks), very preterm (28 to <32 weeks), and moderately preterm (32-34 weeks). Because of the inherent challenges of specimen collection in a vulnerable preterm population, urine and blood samples were not available on a weekly basis for all infants. Furthermore, as universal standards for inflammation are not established among preterm infants, we report the values of all inflammatory markers as mean ± standard deviation (SD) within the first 14 days, 14-42 days, and >42 days of postnatal age (Table 1).
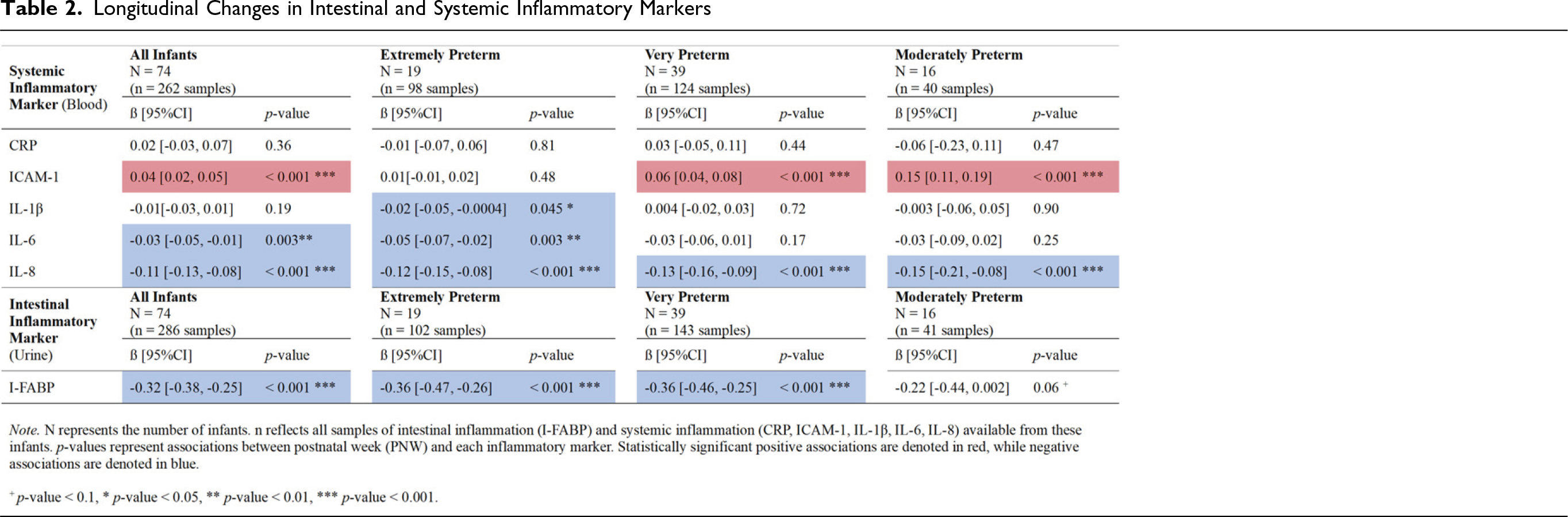
Longitudinal Changes in Intestinal and Systemic Inflammatory Markers
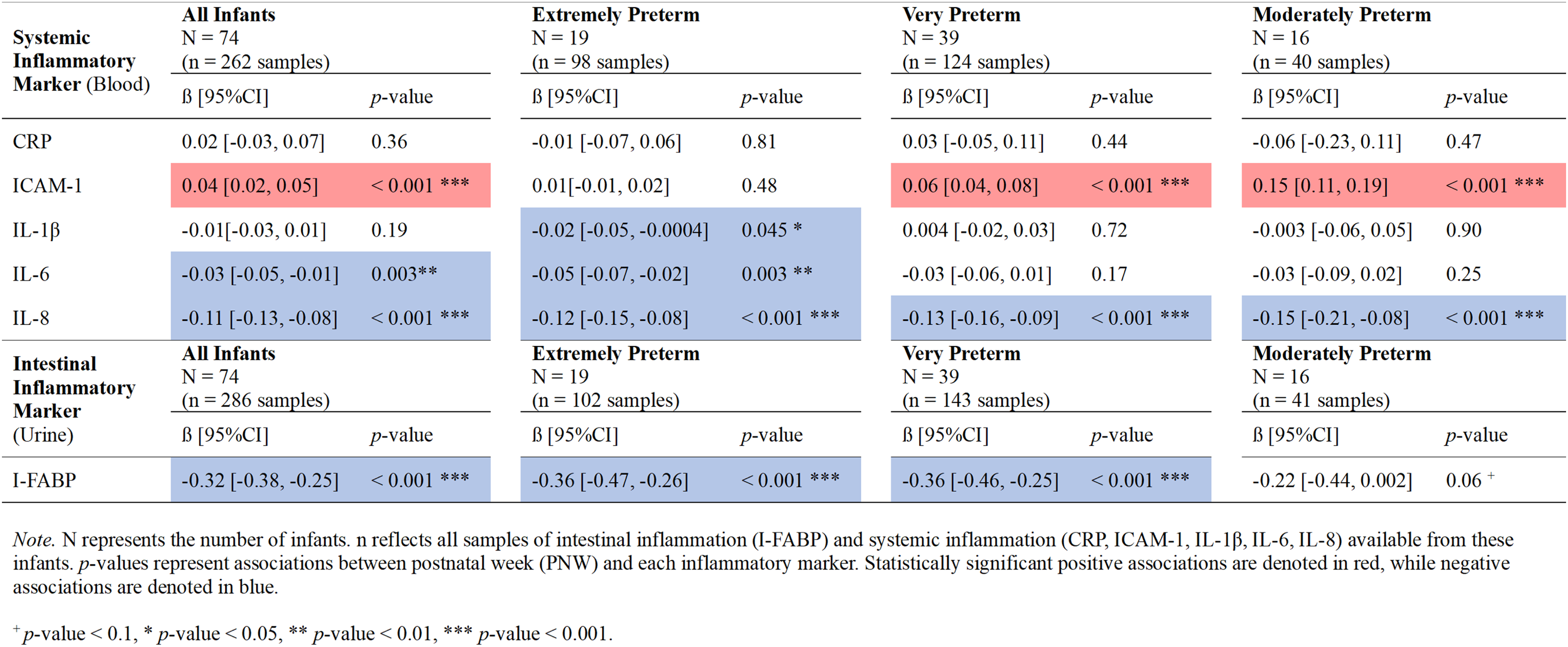
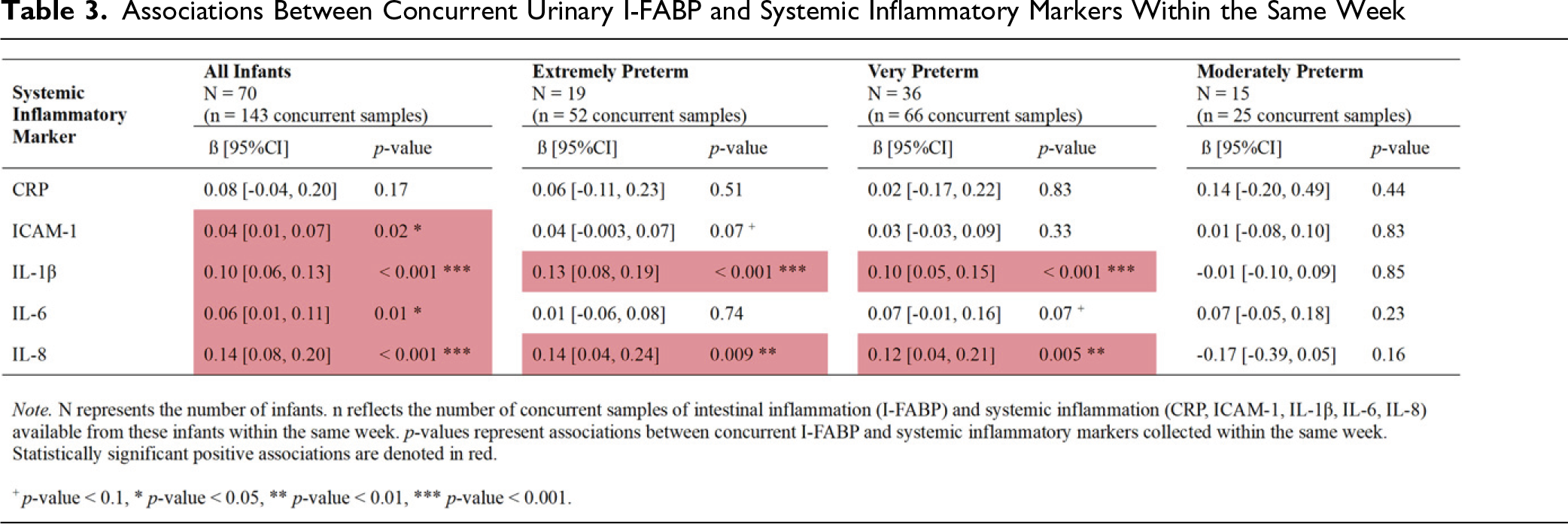
Associations Between Concurrent Urinary I-FABP and Systemic Inflammatory Markers Within the Same Week
Temporal Associations Between Urinary I-FABP and Systemic Inflammatory Markers With I-FABP Preceding Systemic Markers by One Week
For our first analysis evaluating longitudinal changes in inflammatory markers, postnatal week (PNW) was included as a fixed effect in all models. For our second analysis assessing the concurrent relationship between urinary I-FABP and systemic inflammatory markers (CRP, ICAM-1, IL-1β, IL-6, and IL-8), our models included urinary I-FABP and PNW as fixed effects. Analyses were restricted to samples where both urine and blood samples were collected within the same postnatal week. Interaction terms between I-FABP and PNW were tested in all models and were retained only if statistically significant (p < 0.05). For our third analysis investigating temporal associations between urinary I-FABP and systemic inflammatory markers to evaluate the role of intestinal inflammation as a potential precursor to systemic inflammation, we examined urinary I-FABP concentrations measured one, two, and three weeks prior to blood sample collection. Analyses included lagged urinary I-FABP and PNW as fixed effects, and were restricted to infants with available temporal urine and blood samples.
Our primary analyses included the full cohort to provide a comprehensive representation of the NICU population, in which developing comorbidities such as sepsis reflects real-world variability. However, given that a small number of infants in our cohort developed sepsis (n = 6), we performed a secondary analysis excluding these infants to evaluate whether the inclusion of sepsis cases influenced the overall findings. Findings from the non-sepsis analysis, which showed similar trends to the overall sample, are reported in the Supplemental Tables 2–4. The results for the sepsis subgroup are presented descriptively as table footnotes due to the limited sample size which further limits meaningful statistical interpretation of these findings. All analyses were based on available paired urine and blood measurements by postnatal week.
Additionally, we report the weekly inflammatory marker values for the one infant who developed NEC along with the longitudinal trajectories using a simple linear regression model in Supplemental Table 5. We report p-values and confidence intervals for completeness of the regression output, but cannot derive any meaningful statistical conclusions due to the inclusion of only one subject with limited weekly observations.
Due to the exploratory nature of our study, we did not control our models for perinatal and neonatal factors that have been shown to be associated with intestinal and systemic inflammation. Since there are no established normative values for urinary I-FABP and systemic inflammatory markers to indicate a definitive state of inflammation among preterm infants (Stocker & Giannoni, 2024), we thus interpreted intestinal and systemic inflammatory marker values relative to our cohort-specific distributions, while stratifying by infant gestational age, for the purposes of this exploratory study.
Results
Longitudinal Changes in Inflammatory Markers
Longitudinal analyses of all inflammatory marker levels were based on 74 infants with 262 total samples (Table 2). We found a significant decrease over time in levels of I-FABP (ß = −0.32, p < 0.001), IL-6 (ß = −0.03, p = 0.003), and IL-8 (ß = −0.11, p < 0.001), and a significant increase in levels of ICAM-1 (ß = 0.04, p < 0.001). Upon stratifying the temporal effects by gestational age groups, I-FABP showed a similar significant decrease in extremely and very preterm infants (ß = −0.36, p < 0.001; ß = −0.36, p < 0.001, respectively). Similarly, IL-8 significantly decreased over time among extremely, very, and moderately preterm infants (ß = −0.12, p < 0.001; ß = −0.13, p < 0.001; ß = −0.15, p < 0.001 respectively). IL-1β and IL-6 significantly decreased in extremely preterm infants, (ß = −0.02, p = 0.05; ß = −0.05, = 0.003, respectively), while ICAM-1 levels increased among very and moderately preterm infants (ß = 0.06, p < 0.001; ß = 0.15, p < 0.001, respectively). Finally, CRP did not show any significant changes over time in the overall cohort or when stratified by gestational age.
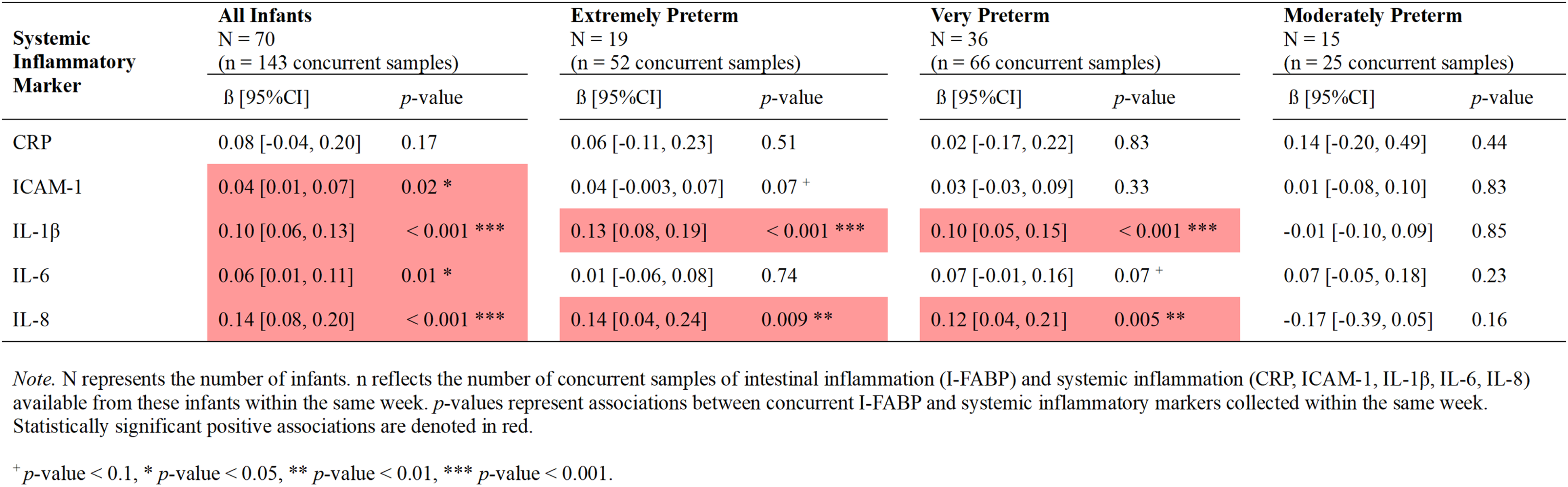
Concurrent Associations Between Inflammatory Markers Within the Same Week
Concurrent associations between urinary I-FABP and systemic inflammatory markers using urine and blood samples collected within the same week are reported in Table 3. Among 70 infants with 143 concurrent samples (n = 286 total samples) included in these analyses, I-FABP was positively associated within the same postnatal week with ICAM-1 (β = 0.04, p = 0.02), IL-1β (β = 0.10, p < 0.001), IL-6 (β = 0.06, p = 0.01), and IL-8 (β = 0.14, p < 0.001). Among extremely and very preterm infants, I-FABP was positively associated within the same postnatal week with IL-1β (β = 0.13, p < 0.001 and β = 0.10, p < 0.001, respectively) and IL-8 (β = 0.14, p = 0.009 and β = 0.12, p = 0.005, respectively). No significant same-week associations were observed for CRP or among moderately preterm infants.
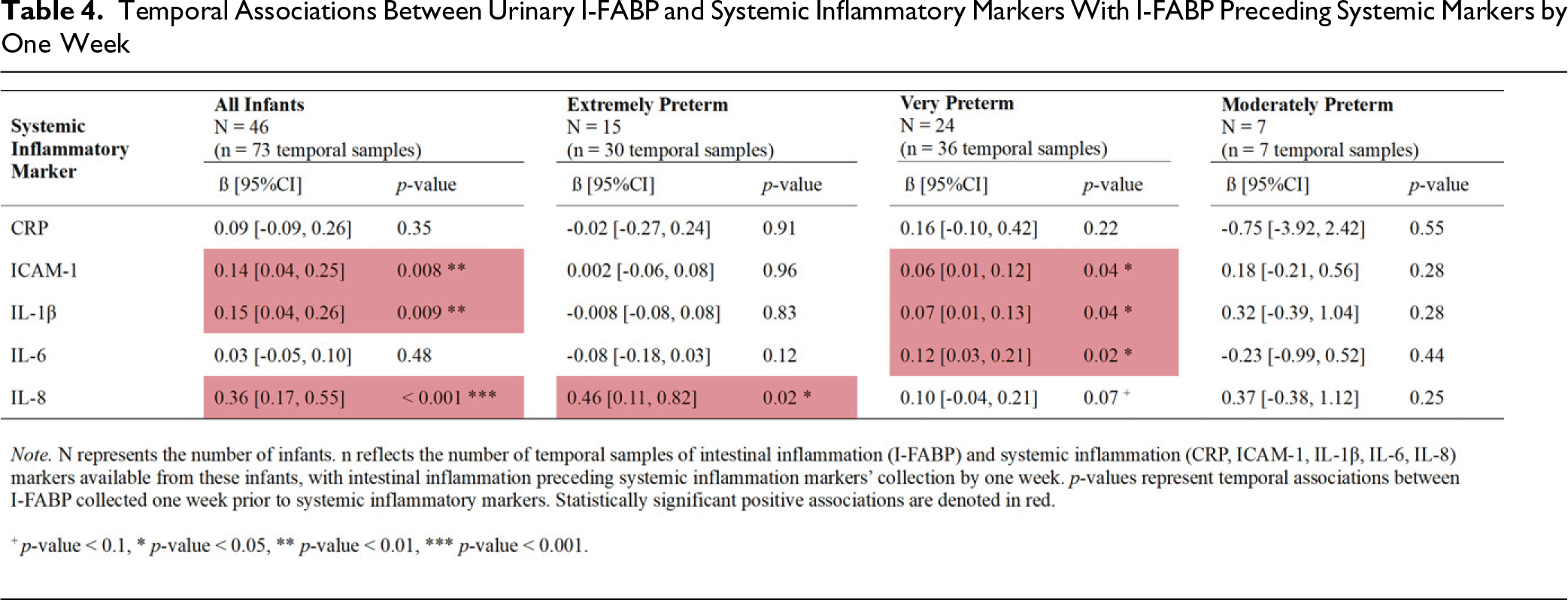
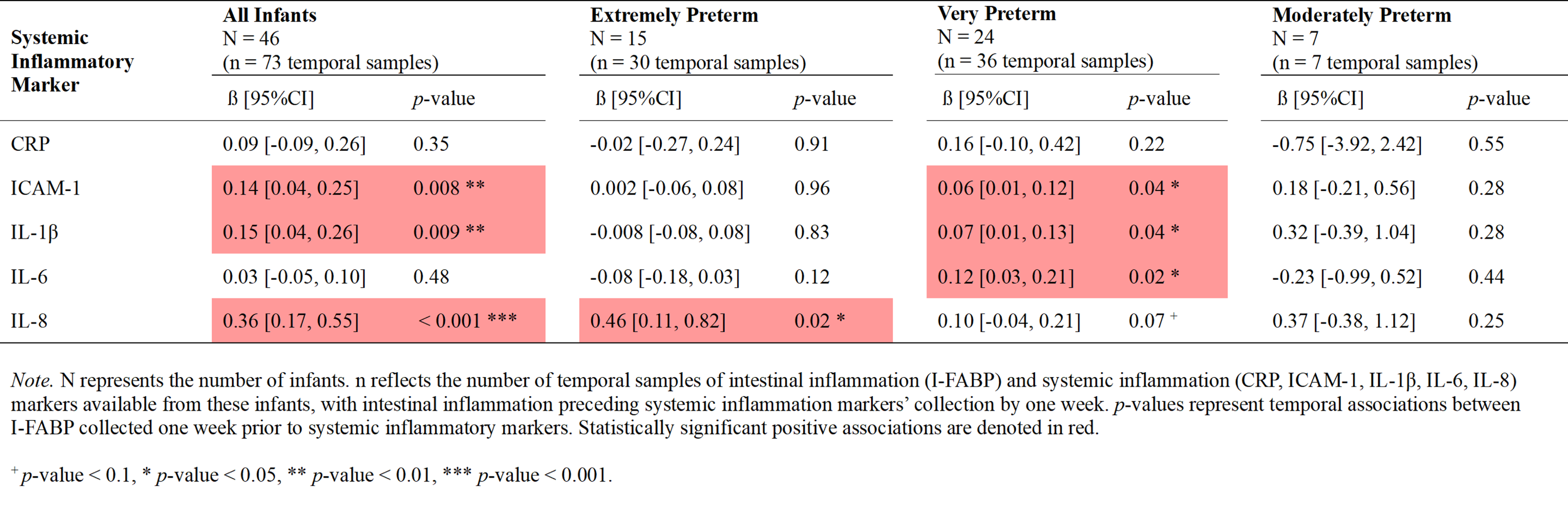
Temporal Associations in Which I-FABP Precedes Systemic Inflammatory Markers
To assess whether changes in intestinal inflammation may precede and act as a precursor to systemic inflammation, we analyzed urinary I-FABP samples collected within one week before blood samples. As summarized in Table 4, these analyses of temporal associations included 46 infants with 73 lagged samples (n = 146 total samples). Among these infants, I-FABP was significantly positively associated with ICAM-1, IL-1β, and IL-8 (ß = 0.14, p = 0.008; ß = 0.15, p = 0.009; ß = 0.36, p < 0.001, respectively). Our age-stratified analyses revealed that among extremely preterm infants, I-FABP was significantly associated only with IL-8 (ß = 0.46, p = 0.02), while no significant associations were found among moderately preterm infants. However, among very preterm infants, I-FABP was significantly associated with ICAM-1, IL-1β, and IL-6 (ß = 0.06, p = 0.04; ß = 0.07, p = 0.04; ß = 0.12, p = 0.02, respectively). No significant temporal associations were observed for CRP or among moderately preterm infants.
We further assessed associations between intestinal and systemic inflammatory markers where urinary I-FABP collection preceded blood collection by two and three weeks to determine whether I-FABP could serve as a precursor to systemic inflammation beyond one week. The two-week interval revealed fewer temporal associations, as I-FABP was significantly associated only with IL-1β and IL-8 (ß = 0.09, p < 0.001; ß = 0.21, p < 0.001). These associations were consistent among extremely (ß = 0.11, p = 0.02; ß = 0.19, p = 0.03, respectively) and very preterm infants (ß = 0.10, p = 0.004; ß = 0.16, p = 0.01, respectively). Finally, no significant associations were detected between urinary I-FABP and systemic inflammatory markers when samples were collected within three weeks apart.
Discussion
This study explored longitudinal changes in inflammatory markers and concurrent and temporal associations between intestinal and systemic inflammation. The results provide new insights into inflammatory processes in preterm infants, indicating time-dependent associations between intestinal and systemic inflammatory markers. Importantly, the findings suggest that intestinal inflammation may have potential predictive value for subsequent systemic inflammatory responses in these infants.
Dynamic Postnatal Changes in Inflammatory Markers
Our analysis demonstrated clear longitudinal changes in inflammatory markers in preterm infants. Specifically, levels of I-FABP, IL-8, and IL-6 decreased significantly over time, whereas ICAM-1 levels increased. I-FABP serves as an indicator of enterocyte damage (Gregory et al., 2014) and, although not inflammation-specific, reflects intestinal epithelial damage with potential downstream effects on systemic inflammatory signaling. In our cohort, we observed a gradual decline in I-FABP levels across all gestational age groups, which is consistent with our prior work demonstrating decreasing I-FABP levels over time (Thai et al., 2022).
Similarly, the decrease in IL-8, a proinflammatory chemokine, was consistent across all gestational age groups, indicating a broad and robust decline over time. Together, the reductions in both I-FABP and IL-8 levels in our cohort likely reflect a physiologic decrease in intestinal epithelial damage or permeability over time as infants mature under standard NICU care. Supporting this interpretation, IL-8 was previously shown to be inversely associated with developmental regulation in the ELGAN study, a large cohort of more than 900 extremely low gestation age neonates followed for 14 days after birth (Leviton et al., 2011).
Levels of IL-6, a proinflammatory cytokine, showed an overall statistically significant decrease over time, particularly among extremely preterm infants. This finding is consistent with previously published ELGAN data showing decreases in key proinflammatory cytokines, including IL-1β, IL-6 and TNFα, with increasing postnatal age, suggesting developmental regulation (Leviton et al., 2011). IL-6 has been used as a biomarker of neonatal sepsis, which involves systemic inflammation in response to infection (Eichberger & Resch, 2022); however, only six infants in our cohort developed sepsis. This low incidence likely contributed to the predominance of a developmental regulation pattern characterized by a decrease in average IL-6 levels over time.
In contrast to proinflammatory cytokines such as IL-8 and IL-6, ICAM-1 is an adhesion molecule expressed across multiple cell types (Bui et al., 2020) and tissues (Chong et al., 2021). Its most well-recognized role is facilitating leukocyte adhesion and migration, thereby contributing to both normal immune development and pathologic inflammatory responses (Haydinger et al., 2023). We observed that overall ICAM-1 levels increased significantly over time, particularly among very and moderately preterm infants. This finding is also in agreement with a previously identified pattern of developmental regulation of ICAM-1 among ELGAN infants, whose levels increased with postnatal age (Leviton et al., 2011). Elevated ICAM-1 levels have also been reported among preterm infants with bronchopulmonary dysplasia (BPD) (Sahni et al., 2020), which may further explain the increase in ICAM-1 levels in our cohort given that nearly half of infants developed BPD. Interestingly, systemic inflammation has been shown to precede and exacerbate BPD (Leroy et al., 2018; Thébaud et al., 2019), suggesting that elevated ICAM-1 levels may therefore reflect ongoing inflammatory signaling and immune cell recruitment prior to the onset of pulmonary injury in our cohort.
Overall, the divergence in longitudinal patterns observed among inflammatory markers supports prior ELGAN findings, demonstrating that while some inflammatory markers may decrease with postnatal maturation, others may increase due to distinct regulatory mechanisms and specific associations with organ development and disease processes in preterm infants.
Concurrent Same-Week Associations Between Intestinal and Systemic Inflammation
The concurrent analysis within the same week revealed significant associations between urinary I-FABP and multiple systemic inflammatory markers, highlighting potential interactions between intestinal and systemic inflammation in preterm infants. In particular, the observed positive associations between I-FABP and systemic inflammatory markers (ICAM-1, IL-1β, IL-6, and IL-8) underscore a potential link between intestinal epithelial injury and/or permeability and systemic inflammatory signaling. In prior neonatal studies, particularly in NEC cohorts, I-FABP levels have been shown to correlate significantly with serum IL-6 (Schurink et al., 2014) and IL-8 (Benkoe et al., 2014) during early disease phases, whereas direct correlation analyses with IL-1β are scarce, likely due to the transient nature of circulating IL-1β (Lopez-Castejon & Brough, 2011). Interestingly, although I-FABP and ICAM-1 exhibited opposing longitudinal trajectories individually, they were positively correlated within the same week, suggesting that these markers co-varied within individual infants. Furthermore, because neither I-FABP nor ICAM-1 is inflammation-specific, their co-variation may reflect early epithelial–immune interactions that precede overt systemic inflammatory responses. This finding aligns with the concept of intestinal inflammation as being closely interconnected with, and potentially preceding, systemic inflammation in preterm infants, a hypothesis that should be further evaluated in a larger cohort. Although IL-6 is a key inducer of CRP synthesis, the lack of same-week association between I-FABP and CRP may reflect CRP’s delayed kinetics as a downstream hepatic acute-phase reactant, limiting its sensitivity to early, localized, or subclinical inflammatory processes in preterm infants (Liu et al., 2025).
I-FABP Levels as a Precursor of Systemic Inflammation
Our temporal analysis provided compelling evidence that intestinal inflammation, as measured by urinary I-FABP levels, may precede the rise in systemic inflammatory markers by one week. Positive associations between I-FABP and systemic inflammatory markers (ICAM-1, IL-1β, and IL-8) measured one week later suggest that intestinal epithelial damage or increased gut permeability might be an early indicator of subsequent systemic inflammatory responses. This temporal relationship was most evident in very preterm infants, where I-FABP was significantly associated with ICAM-1, IL-1β, and IL-6. These findings emphasize the potential role of early intestinal inflammation as a precursor to broader systemic inflammation.
Previous studies have demonstrated increased intestinal inflammation among preterm infants using urinary I-FABP and fecal calprotectin as biomarkers (Rodríguez-Benítez et al., 2021; Thai et al., 2022). However, the characterization of intestinal inflammation in this population and its temporal association with systemic inflammation remain poorly understood. Of note, our results suggest that intervals exceeding one week between urinary I-FABP and systemic inflammatory markers may be too long to detect clinically relevant and meaningful associations, or that clinical interventions may have been initiated in response to underlying intestinal or systemic inflammation (e.g., suspected or confirmed NEC or sepsis).
Interestingly, the association between intestinal inflammation, as measured by fecal calprotectin, and systemic inflammation has been well documented in conditions such as cystic fibrosis, where elevated levels of fecal calprotectin correlate with systemic inflammatory markers (Lee et al., 2012; Tam et al., 2022). This suggests that similar clinical investigations focused on non-invasive markers may be valuable in preterm infants. These findings may be clinically significant because early detection and mitigation of intestinal inflammation may help prevent the subsequent onset of systemic inflammation. Nonetheless, while our analyses suggest temporal associations, causality cannot be inferred due to the observational study design. Additionally, the lack of universally accepted cutoff ranges for systemic inflammatory markers highlights the need for further research to clarify their clinical interpretation and utility in this context.
Strengths and Limitations
There are several strengths to our study. To our knowledge, although intestinal and systemic inflammation have each been studied in preterm infants and other pediatric populations, their temporal relationship remains poorly characterized. Our findings highlight the potential predictive value of non-invasive measurements of intestinal inflammation, such as urinary I-FABP, demonstrating associations with systemic inflammatory markers up to one week before their detection in the blood. These findings suggest that intestinal inflammation preceding the onset of systemic inflammation may present a critical window for intervention, with strategies focused on optimizing gut health and potentially mitigating downstream systemic inflammatory effects. Another strength of our study is the longitudinal assessment of the levels of inflammatory markers over an average hospitalization period of 10 weeks, which strengthens the interpretation of our findings. Finally, the intestinal and systemic inflammatory markers evaluated in our study are well established in the literature, enhancing the clinical relevance, interpretability, and reproducibility of our results.
Despite these strengths, several limitations should be acknowledged. Although our cohort reflects a representative sample of preterm infants cared for in a tertiary-level NICU, the findings may not be generalizable to preterm infants in other clinical settings or broader populations. Additionally, our sample size - particularly for the temporal subgroup analyses - was relatively small, which may further limit the broader applicability of our findings. Due to this modest sample size, our statistical models were not adjusted for any factors known to influence inflammatory marker profiles, including gestational age, infection status, antibiotic exposure, or feeding type. Furthermore, the absence of established cutoff ranges for systemic inflammatory markers limits our ability to definitively classify inflammatory status. As such, our findings should be interpreted as providing insight into temporal associations between intestinal and systemic inflammation, with rising I-FABP levels potentially signaling subsequent worsening of systemic inflammation. Additionally, the observational nature of the study precludes conclusions about causality. Future research should aim to replicate these findings in larger cohorts, incorporate adjustments for relevant clinical variables, and further explore the biological mechanisms underlying the observed temporal changes and their potential utility for early risk identification and intervention.
Clinical Implications
Our findings have important clinical implications, especially when it comes to developing non-invasive methods for early risk assessment and prompt intervention in preterm infants who are at risk of developing worsening inflammatory morbidities. Routine monitoring of urinary I-FABP, a non-invasive marker of intestinal epithelial injury, may help identify infants at increased risk for subsequent systemic inflammation. Early identification, in turn, may guide timely nutritional interventions (e.g., optimization of human milk fortification), microbial strategies (e.g., probiotic supplementation), or other approaches aimed at modulating intestinal and systemic inflammatory responses. Collectively, this non-invasive approach may support earlier risk identification and clinical decision-making while minimizing blood draws and other potential adverse health outcomes in preterm infants.
Additionally, our study underscores the need to establish gestational age-specific reference ranges for both intestinal and systemic inflammatory markers among preterm infants. The differential inflammatory patterns observed across gestational age groups highlight the importance of tailored monitoring and therapeutic strategies that account for developmental differences in immune and intestinal maturation at specific gestational ages. While the establishment of standardized reference ranges for inflammatory markers remains an important goal, defining absolute cutoff values in highly heterogeneous populations such as preterm infants is inherently challenging. In this context, serial increases in markers, such as I-FABP, may potentially serve as early indicators of evolving intestinal and later systemic inflammation, even in the absence of validated cutoff values.
Conclusion
In summary, this study highlights significant longitudinal changes in inflammatory markers and identifies temporal associations between intestinal and systemic inflammation in preterm infants. These findings enhance our understanding of inflammatory processes during early life and suggest that intestinal inflammation may precede and signal subsequent systemic inflammatory responses. Furthermore, this work highlights potential avenues for non-invasive monitoring, earlier identification of infants at risk, and the development of targeted interventions aimed at improving clinical outcomes among this pediatric population.
Future research should prioritize the development of standardized, gestational age–specific reference intervals for both intestinal and systemic inflammatory markers in preterm infants. The current absence of validated cutoff values limits clinicians’ ability to interpret inflammatory markers and accurately identify infants at risk. Establishing these normative ranges will be essential for translating biomarkers such as I-FABP from exploratory research tools into clinically actionable indicators.
Supplemental Material
Supplemental material - Temporal Relationships Between Systemic Inflammatory Markers and Urinary I-FABP in Preterm Infants: Evidence that Intestinal Inflammation Precedes Systemic Inflammation
Supplemental material for Temporal Relationships Between Systemic Inflammatory Markers and Urinary I-FABP in Preterm Infants: Evidence that Intestinal Inflammation Precedes Systemic Inflammation by Noura El Habbal, Evgenia Jen Filatava, Samer Charbaji, Maya Gordon, Raina Fichorova, Katherine E. Gregory in Biological Research For Nursing
Footnotes
Author note
Katherine E. Gregory and Evgenia Jen Filatava: Department of Pediatric Newborn Medicine, Brigham and Women’s Hospital, Harvard Medical School, Boston, MA, USA.
Acknowledgements
The authors wish to acknowledge Tina Steele, RN, BSN, Research Nurse, Brigham and Women’s Hospital, for her generous support of research recruitment activities associated with this project.
Author Contributions
El Habbal, Noura contributed to study design, data analysis and interpretation, drafted the manuscript, critically revised the manuscript, gave final approval, and agrees to be accountable for all aspects of the work ensuring its integrity and accuracy. Filatava, Evgenia Jen contributed to study design, data acquisition and interpretation, critically revised the manuscript, gave final approval, and agrees to be accountable for all aspects of the work ensuring its integrity and accuracy. Charbaji, Samer contributed to data analysis, critically revised the manuscript, gave final approval, and agrees to be accountable for all aspects of the work ensuring its integrity and accuracy. Gordon, Maya contributed to data acquisition, critically revised the manuscript, gave final approval, and agrees to be accountable for all aspects of the work ensuring its integrity and accuracy. Fichorova, Raina contributed to data acquisition, critically revised the manuscript, gave final approval, and agrees to be accountable for all aspects of the work ensuring its integrity and accuracy. Gregory, Katherine E. contributed to study conception and design, data acquisition and interpretation, critically revised the manuscript, gave final approval, and agrees to be accountable for all aspects of the work ensuring its integrity and accuracy.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the NIH grant R21NR017256. All authors have read and approved the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.