
Abstract
Purpose:
To describe the case and the follow-up of an inadvertently damaged XEN gel implant during needling procedure.
Methods:
Case report.
Results:
A 60-year-old African American patient underwent an uncomplicated combined phacoemulsification with the insertion of a XEN gel implant. Two months postoperatively, a needling procedure was required. During the needling procedure, a fragment of the XEN gel implant was inadvertently damaged. One month postoperatively, the intraocular pressure was still controlled and the bleb was functioning well.
Conclusion:
This case report reveals a previously unreported complication concerning XEN gel implant. It is important for the surgeon to pay attention during needling procedure, especially if there is a subconjunctival hemorrhage impairing the view, to defer the procedure until good visibility exists.
Introduction
Intraocular pressure (IOP) is the only modifiable factor in the therapy of glaucoma. When medical treatment and laser procedures fail to reduce the IOP or cause ocular surface toxicity, glaucoma surgery is proposed. Trabeculectomy remains the gold standard of surgical glaucoma therapy. 1 Despite the potential reduction of IOP following trabeculectomy with the use of antimetabolites, several vision-threatening complications may still occur, such as hypotony maculopathy, choroidal effusion, suprachoroidal hemorrhage, and bleb-related endophthalmitis.1,2
The XEN gel implant, a hydrophilic, non-inflammatory, subconjunctival gelatin stent (XEN Gel Stent, Allergan, Dublin, USA), provides an ab interno approach to create a permanent channel from the anterior chamber to the subconjunctival space and is designed to avoid early postoperative hypotony.3,4 The flexibility of the implant and its expansion upon hydration allow it to be tissue conforming and thus preventing the risk of extrusion and migration. 5 As with standard filtering surgery, this procedure creates a subconjunctival bleb which is subject to subsequent fibrosis. When this occurs, needling with or without antimetabolites is indicated. 6 This report describes the first case in which part of the XEN gel implant was inadvertently damaged during needling procedure (see video, Supplemental Digital Content 1, which demonstrates the needling procedure post-XEN gel implant).
Case report
A 60-year-old African American patient with primary open-angle glaucoma (POAG) and who underwent argon laser trabeculoplasty (ALT) in 2006 was referred to our glaucoma center for a second opinion. The patient reported having had an old blunt trauma to his left eye. On his first visit, best corrected visual acuity (BCVA) was 1.0 and 0.7 in the right eye (OD) and the left eye (OS), respectively. Gonioscopy showed open angles in both eyes with partial angle recession in the supero-temporal quadrant of the left eye. The rest of the anterior segment examination was unremarkable except for a cataract in the left eye. Posterior segment examination showed an optic nerve sized 2 mm in both eyes, a cup to disk ratio (C/D) of 0.7 in OD and 0.9 in OS. His IOPs were 16 and 14 mmHg in OD and OS, respectively, on four glaucoma medications: brimonidine, brinzolamide, bimatoprost, and timolol. Central corneal thickness, measured by optical coherence tomography (OCT), was 520 µm OU. Recent visual fields revealed early diffuse sensitivity losses with a mean deviation (MD) value of 4.0 dB in OD and partial arcuate defect and paracentral scotoma with an MD value of 7.7 dB in OS. OCT showed significant retinal nerve fiber layer (RNFL) thinning in OS with an average RNFL thickness of 77 µm. Therefore, selective laser trabeculoplasty (SLT) was suggested for the right eye and a combined surgery of phacoemulsification and XEN gel implant for the left eye.
A combined surgery of phacoemulsification and insertion of the XEN gel implant with the use of mitomycin C (MMC) was done in the left eye. The surgery was uneventful. Day 1 post surgery, the left eye showed corneal edema, descemet folds, 1+ cells in the anterior chamber, and a diffuse hyperemic bleb. IOP for the left eye was 12 mmHg. The patient was on a combination of tobramycin and dexamethasone eye drops four times daily.
One week postoperatively, corneal edema was reduced, anterior chamber was deep and quiet and the XEN gel implant was in place with a diffuse and hyperemic bleb in the left eye. IOP was 14 and 10 mmHg in OD and OS, respectively. One month postoperatively, the left eye showed hyperemic flat bleb with the XEN gel implant in place and an IOP of 24 mmHg. Tobramycin and dexamethasone eye drops were stopped to exclude a steroid response. Two weeks later, the patient’s OS IOP was 18 mmHg. Bimatoprost once a day and timolol twice a day were added for the left eye, and the decision of needling procedure for that eye was taken.
After topical anesthesia with cocaine 4% and disinfection using povidone-iodine 5%, the left eye was stabilized in downward position using 5-0 silk stay suture. Upon inspection, the XEN gel implant was visible under the conjunctiva and in the anterior chamber (Figure 1(a)). A 28-gauge needle attached to a syringe filled with 50% balanced salt solution and 50% rapidocaine was advanced gradually to the bleb area on the supero-nasal quadrant subconjunctivally (Figure 1(b)). The subconjunctival scarring was disrupted using sideways sweeping movements back and forth. Perforation of a subconjunctival blood vessel led to a subconjunctival hemorrhage which impaired the clear view of the XEN gel implant through the conjunctiva (Figure 1(c)). At the end of the needling procedure, a fragment of the XEN gel implant extruded to the conjunctival surface (Figure 1(d)). No bleb leak was found. The fragment was removed and measured to be 1.1 mm. A moderate-sized bleb was present at the end of the intervention. Subsequently, 0.2 mL of 0.4 mg/mL MMC was injected subconjunctivally posterior to the site of broken XEN gel implant.
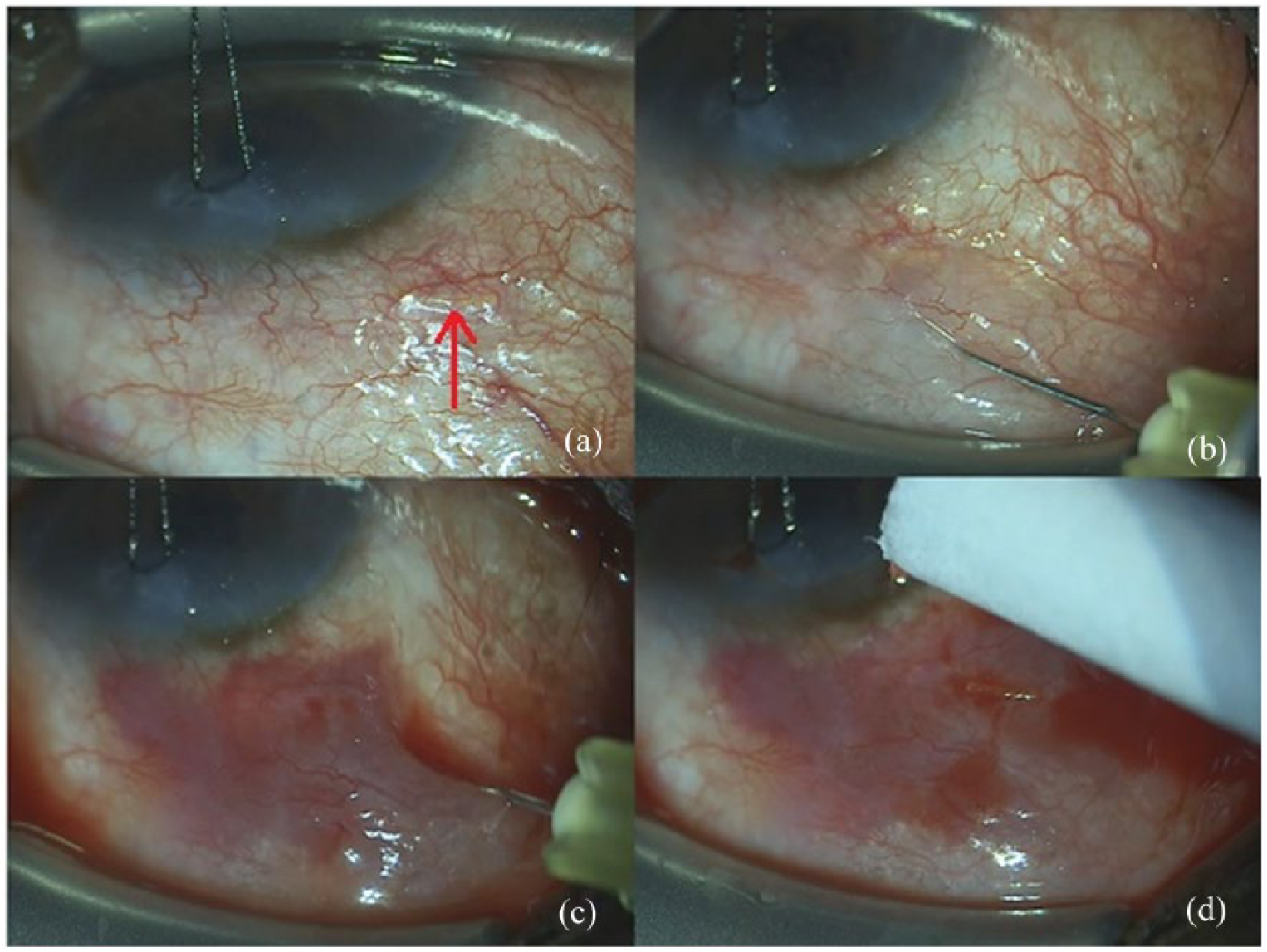
Intraoperative photographs during the needling procedure. These photographs show (a) the XEN gel implant under the conjunctiva at the beginning of the surgery, (b) insertion of the 28-gauge needle in the subconjunctival space on the supero-nasal quadrant, (c) needling procedure with subconjunctival hemorrhage, and (d) cutting and extrusion of the distal part of the XEN implant after needling.
Day 1 postoperatively, the XEN gel implant was visible and unobstructed on gonioscopy in the anterior chamber angle. The bleb was hyperemic associated with a subconjunctival hemorrhage which impaired the visualization of any XEN gel implant segment. IOP was 15 mmHg measured by iCare rebound tonometry as the patient was non-compliant for Goldmann applanation tonometry (GAT).
One week postoperatively, XEN gel implant was not visible under the conjunctiva and the IOP in left eye was 12 mmHg (GAT) with a deep anterior chamber and a shallow bleb. Ultrasound biomicroscopy showed XEN gel implant in the sclera and a shallow bleb (Figure 2(a)). OCT and OCT-angiography of the bleb showed the XEN gel implant in the sclera and anterior chamber with a moderately diffuse bleb around it (Figure 3).
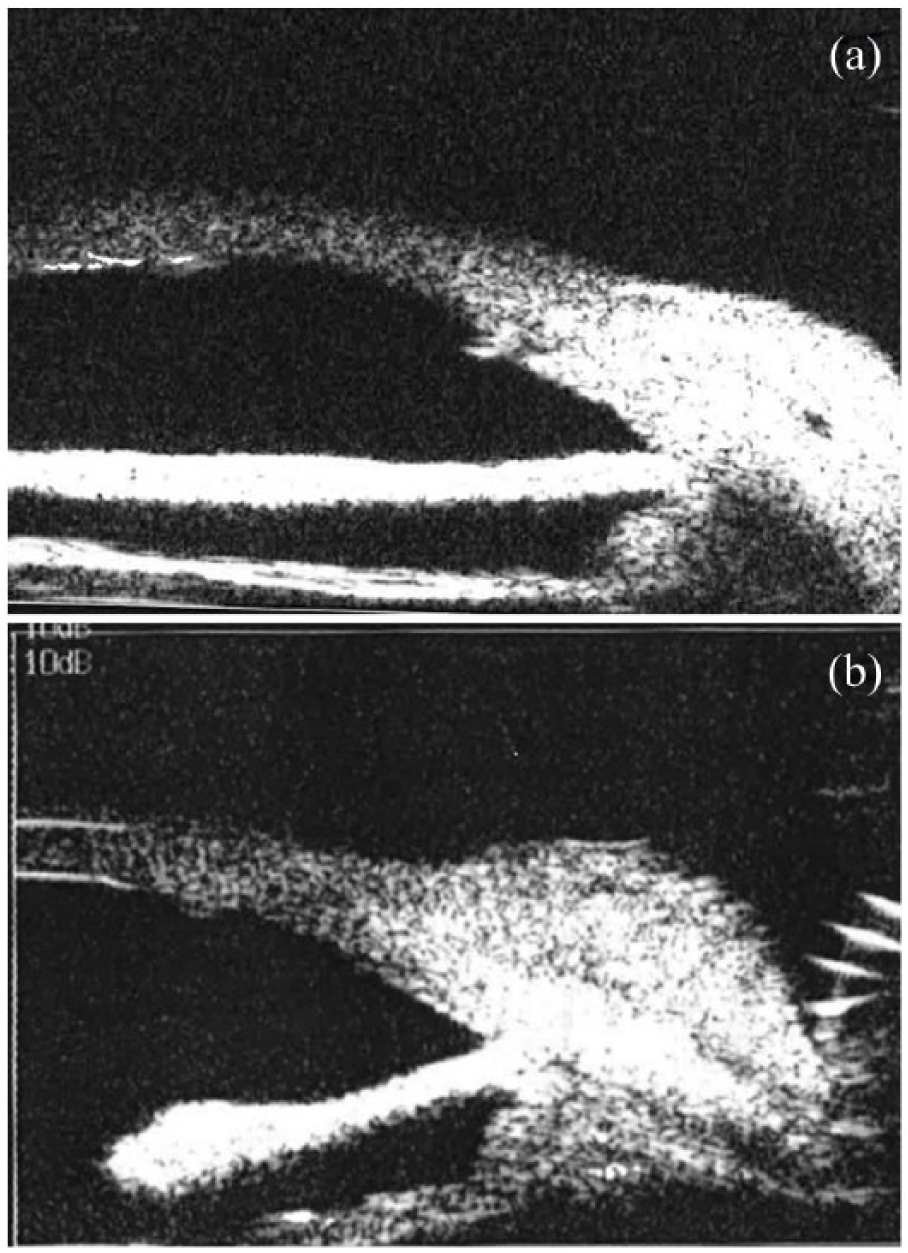
Ultrasonic biomicroscopy. It reveals a patent XEN gel implant in the sclera (a) 1 week postoperatively and (b) formation of bleb at 1-month follow-up.
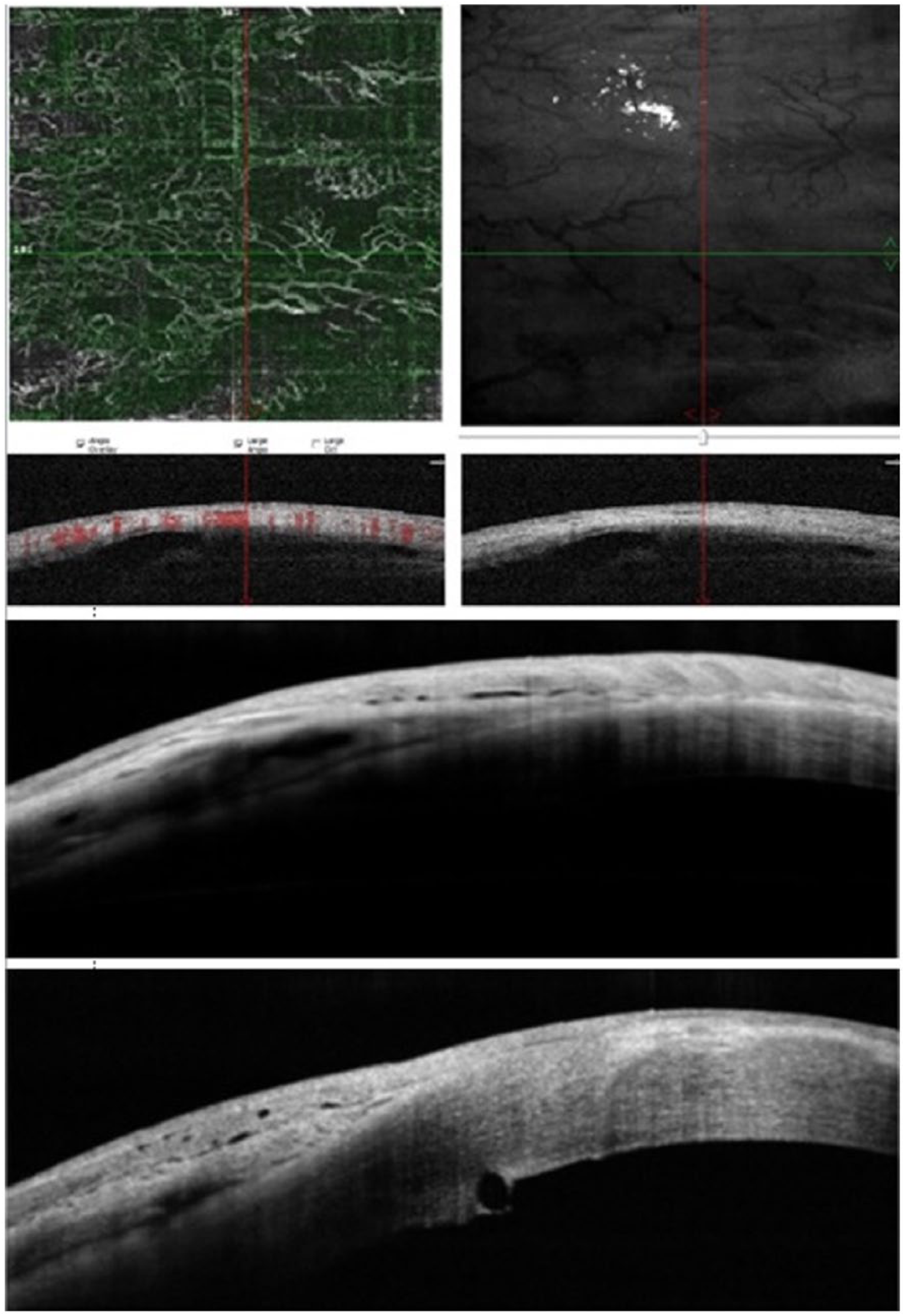
Optical coherence tomography (OCT) and OCT-angiography (OCTA) of the bleb.
One month postoperatively, IOP was 15 and 14 mmHg in OD and OS, respectively. Ultrasound biomicroscopy revealed a formed bleb (Figure 2(b)).
Discussion
To our best knowledge, this report is the first case of XEN gel implant being damaged during a needling procedure. As with other filtering procedures, postoperative needling has been reported to be frequently required after XEN implantation. In a large size study by Schlenker et al., 6 needling was performed on 43.2% and 30.8% of XEN and trabeculectomy eyes, respectively. In our case, the subconjunctival hemorrhage intraoperatively impeded our clear view of the XEN gel implant and hence led to the damage of its distal part. Therefore, needling is potentially more complicated in patients with XEN than from other filtering surgeries because of the possibility of damaging the implant especially if the view was not clear. Since good visualization is more important when doing needling in a XEN case than after trabeculectomy, care should be applied to avoid damaging blood vessels. However, as demonstrated in this case, even when moderate damage occurs to the XEN tip, the surgery can still function.
At present, there are no data that show whether inadvertent cutting of the subconjunctival part of the XEN gel implant would affect its function. In our case, having a low IOP and a well-formed bleb demonstrated by the OCT after the needling procedure confirm the XEN gel implant functioning. Thus, having even a small part of the distal end of the XEN gel implant draining into the subconjunctival space might be sufficient to lower the IOP.
Therefore, besides other postoperative complications like flat anterior chamber, hyphema, transient hypotony, dislocation, repositioning, and exposure of XEN gel implant as well as internal ostium occlusion, this case report reveals a new complication. The surgeon must be aware of the possibility of inadvertent damage to the XEN device when performing needling as its soft tube structure and its subconjunctival position put it at risk for such an adverse outcome.3,7–9
Conclusion
As with any other glaucoma surgery with subconjunctival bleb formation, needling procedure may be needed after XEN implantation. It is important for the surgeon to pay attention during needling procedure, especially if there is a subconjunctival hemorrhage impairing the view, not to damage the subconjunctival XEN gel implant. It is also possible that a shortening of the subconjunctival portion of the XEN device might have an effect of reducing outflow resistance.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental Material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.