
Abstract
Purpose:
Fracture of a three-piece polyimide–elastimide intraocular lens at the optic–haptic junction following blunt trauma is a possible complication after cataract surgery. We report a case of an isolated posterior chamber intraocular lens fracture caused by direct ocular blunt trauma.
Case:
A 51-year-old patient underwent blunt orbital trauma caused by a raw chicken egg that was thrown at him, as he was walking. The posterior chamber intraocular lens was found in the anterior chamber, with a broken optic–haptic junction. The intraocular lens was exchanged, followed by iris fixation and pupilloplasty, with satisfactory postoperative anatomical and optical outcomes.
Discussion:
The three-piece polyimide–elastimide intraocular lens was fractured at the optic–haptic junction. Although the fractured intraocular lens surface had a regular appearance, it has been previously reported that the polyimide haptic’s durability is probably inferior to that of polymethylmethacrylate. Therefore, it is highly susceptible to shear stress induced by a blunt trauma.
Conclusion:
To our knowledge, this is an uncommon report of an implanted posterior chamber polyimide–elastimide intraocular lens fracture following blunt orbital trauma. Intraocular lens exchange and fixation had successful optical and anatomical results.
Keywords
Introduction
Modern foldable silicone plate-haptic and polyimide–elastimide intraocular lenses (IOLs) appear to be more prone to damage during folding, loading, and implantation than other IOLs. 1 In contrary to polyimide, single-piece polymethylmethacrylate (PMMA) IOLs can withstand high levels of stress. Still, excessive pressure on the optic–haptic junction can cause a fracture, since it is the weakest point of the IOL.1–3 Most previously reported cases of posterior chamber fracture of IOLs involved lenses made of PMMA, 4 which is still the standard material for IOLs, against which newer materials are compared. 2
Here, we report an unusual case of fracture of posterior chamber polyimide–elastimide IOL at the haptic–optic junction following blunt orbital trauma.
Case description
A 51-year-old man with past medical history of hypothyroidism, hyperlipidemia, and hyperuricemia was referred to our clinic. His past ophthalmic history was significant for several idiopathic anterior uveitic exacerbations in his right eye during adolescence. These were treated conservatively with short-term, local courses of steroids, and an uneventful cataract surgery at the age of 25 years. A three-piece (3P) polyimide–elastimide IOL was implanted in the bag (elastimide; STAAR, Monrovia, CA, USA).
The patient was seen in the emergency department, 6 weeks earlier, due to blunt orbital trauma to his right eye caused when a raw chicken egg was thrown at him from a passing car several meters away as he was walking. He was initially diagnosed with superior and medial orbital wall fractures (seen on computed tomography). Additional findings were significant for a dislocated posterior chamber intraocular lens (PCIOL) which was observed in the anterior chamber, a break at the optic–haptic junction, irregular pupil, and a significant vitreous hemorrhage. He was treated conservatively with topical dexamethasone (Sterodex; dexamethasone sodium phosphate 0.1%; Fischer Pharmaceutical Laboratories Ltd, Tel Aviv, Israel) and ciprofloxacin (Ciloxan; Alcon Laboratories, Fort Worth, TX, USA). On presentation to our clinic, best-corrected visual acuity (BCVA) of the right eye was 20/100. Slit-lamp examination revealed an anteriorly dislocated three-piece polyimide–elastimide IOL located in the anterior chamber. The inferior haptic seemed to be broken. Its free part was attached to the pupil with vitreous strands bulging below the optic. The iris was irregular and recessed nasally. The pupil was unreactive, fixed, and dilated. Posterior synechia were also significant (Figure 1). Macular edema confirmed by optical coherence tomography (OCT) was observed (Figure 2), with intra-retinal and minimal central sub-retinal fluid exudation. Central macular thickness measured 430 µm. Slit-lamp examination and OCT imaging of the left eye were within normal limits with a BCVA of 20/20.
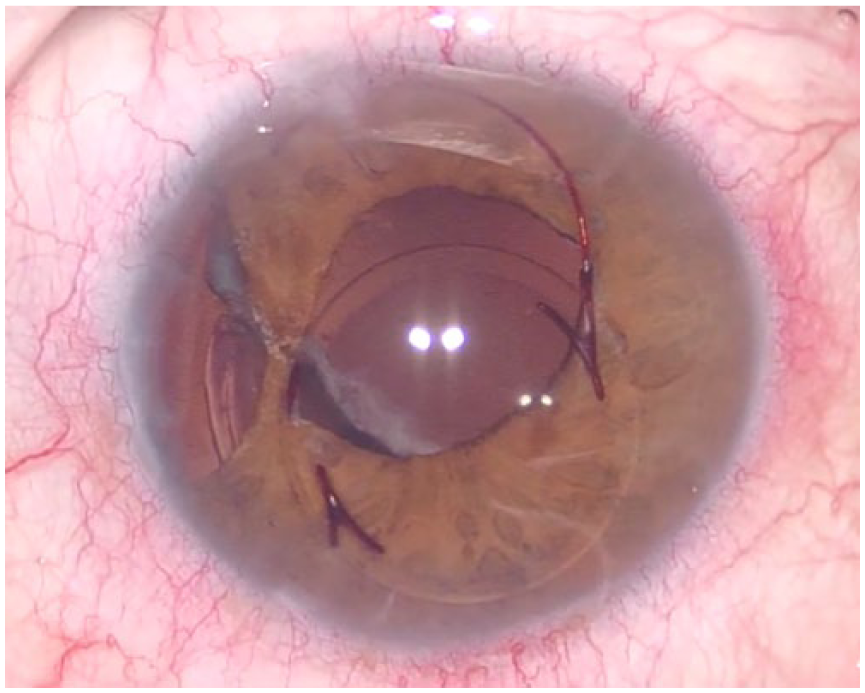
Right eye (RE) preoperative dislocated and broken IOL.
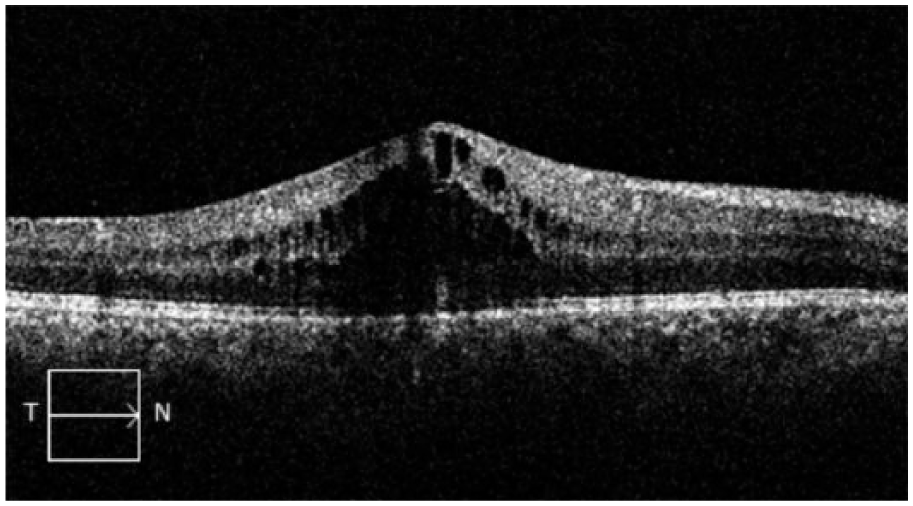
RE preoperative OCT showing macular edema.
The endothelial cell density (ECD) count of the right cornea showed a mean of 1300 cells/mm2 as compared to 2210 cells/mm2 in his left eye.
The patient underwent immediate surgery in which the broken three-piece polyimide–elastimide IOL was cutoff and explanted. This was followed by anterior vitrectomy, after which a single-piece hydrophilic +17.5 PCIOL (Medicontur, Zsámbék, Hungary) was implanted into the ciliary sulcus. Modified McCannel’s technique sutures were used to fixate each of the haptics to the iris. Finally, pupilloplasty and iridoplasty were performed, followed by intravitreal injection of triamcinolone 0.05 mL (Triesence; Alcon Laboratories). The orbital fractures and vitreous hemorrhage were managed conservatively. No further treatment was needed.
On his follow-up visit, 3 weeks postoperatively, the anterior segment was quiet, with a well-centered and stable fixated PCIOL (Figure 3). BCVA was 20/25, and no macular edema was shown on the OCT (Figure 4).
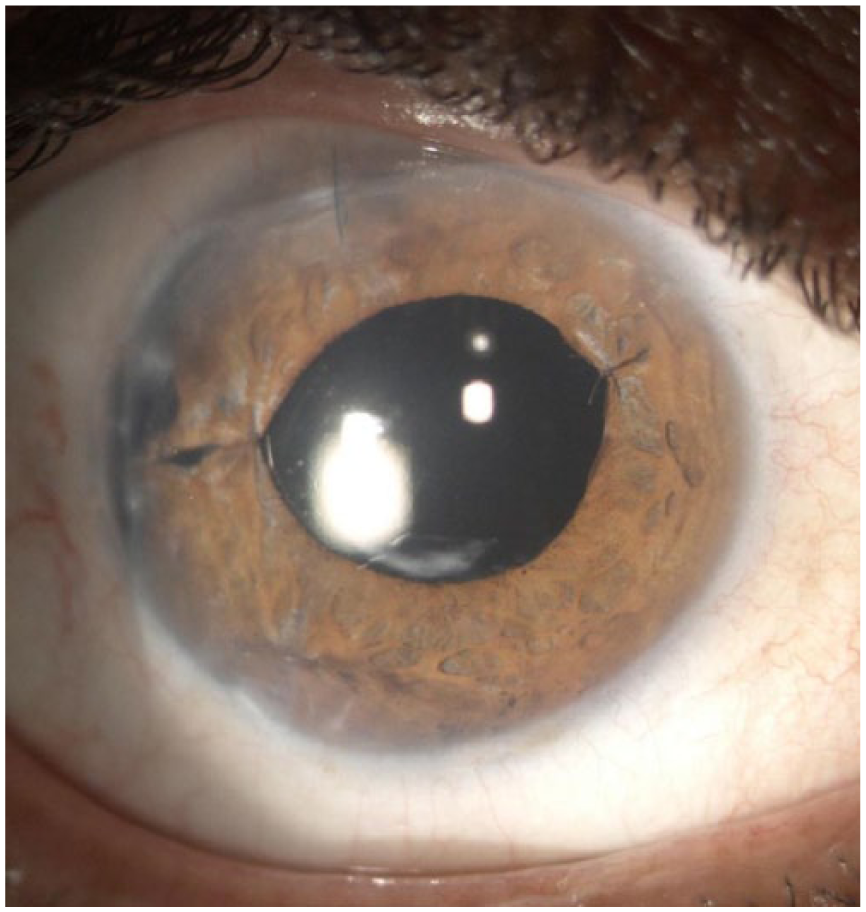
RE postoperative iris fixated with Medicontur PCIOL.
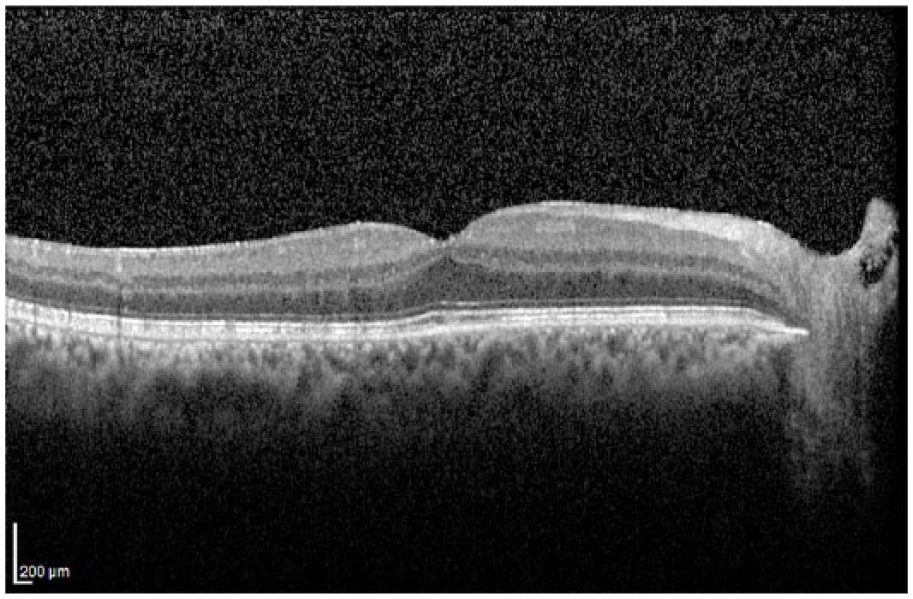
RE postoperative OCT showing the resolution of macular edema.
Discussion
PMMA and polyimide IOLs (located either in the anterior or posterior chamber) were previously reported for possible spontaneous fracture at the optic–haptic junction (which are known for their low optic–haptic junction elasticity).3–9 Natural biodegradation is a known drawback of the three-piece combined polyimide–elastimide IOLs, which is usually observed several years after implantation. Yet, to our knowledge, fracture of a three-piece polyimide–elastimide posterior chamber IOL, following an isolated, blunt orbital trauma, is seldom reported. 9 Das et al. 10 described a possible mechanism of fracture of the optic–haptic junction following blunt trauma. Similar to our case, a possible mechanism is high energy absorbed by the PCIOL, forcing the optic through the pupil, creating high stress against the delayed haptic, which remains behind the iris (found in the bag) secondary to high-force blunt trauma. Interestingly, as in our case, other ocular structures were not damaged 8 and this was a fairly isolated finding.
After removal of the broken polyimide–elastimide IOL, various options for secondary implanted lens were considered. As the patient’s eye had a history of recurrent anterior uveitis and a possibly susceptible blood ocular barrier, a guiding principle was to use a lens material with good biocompatibility for implantation within the ciliary sulcus, which is suitable for iris fixation and will be less likely to provoke an inflammatory reaction. For that purpose, a hydrophilic Medicontur PCIOL was chosen, preferably fixated to the iris, so centration and stability is Longley maintained.
In conclusion, the more susceptible polyimide–elastimide IOLs have less flexible haptics, increased brittleness, and susceptibility to biodegradation. As previously reported by Das et al., 10 blunt trauma, via full kinetic energy absorbance, might result in dislocation and fracture of the IOL, as in our case. Explantation of the broken IOL followed by an implantation and iris fixation of a Medicontur IOL resulted in good anatomical and optical outcomes.
Footnotes
Acknowledgements
A.F. and T.S. contributed equally to this paper.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.