
Abstract
Purpose:
To review the published scientific literature concerning clinical and material degradations of intraocular lenses after implantation in cataract surgery.
Methods:
A search was undertaken using the following databases: CENTRAL (including Cochrane Eyes and Vision Trials Register; The Cochrane Library: Issue 2 of 12 February 2019), Ovid MEDLINE (R) without Revisions (1996 to February week 2, 2019), Ovid MEDLINE (R) (1946 to February week 2, 2019), Ovid MEDLINE (R) Daily Update 19 February 2019, MEDLINE and MEDLINE non-indexed items, Embase (1980–2019, week 7), Embase (1974–2019, 19 February), Ovid MEDLINE (R) and Epub Ahead of Print, in-Process & Other Non-Indexed Citations and Daily (1946 to 19 February 2019), Web of Science (all years), the metaRegister of Controlled Trials (mRCT) (www.controlled-trials.com), ClinicalTrials.gov (www.clinicaltrial.gov) and the WHO International Clinical Trials Registry Platform (www.who.int/ictrp/search/en). Only published articles in English were selected. Search terms/keywords included ‘IOL’ or ‘intraocular lens’, combined with ‘opacification’, degradation, glistenings, nanoglistenings, whitening, transmittance, light scatter, discolouration/discoloration, performance, quality, material, biocompatibility, calcification, explantation and ultraviolet/UV radiation. Relevant in-article references not returned in our searches were also considered.
Results:
After review of the available articles, the authors included 122 publications in this review, based on the quality of their methodology and their originality. The studies included in this review were randomized controlled trials, cohort studies, case-controlled studies, case series, case reports, laboratory studies and review papers. Differing material degradations of intraocular lenses have been described and their associated pathophysiology studied. Reported anomalies include photochemical alterations, water vacuoles, internal and surface calcific deposits, surface coatings and discolouration. The nature of such changes has been shown to depend on the type of intraocular lenses material used and/or manufacturing processes and storage conditions employed. Changes in the intraocular lens can also be influenced by surgical technique, coexisting ocular pathologies and topical and systemic medications. The clinical significance of these degradations is variable, with some resulting in significant visual disturbance and the need for intraocular lens explantation and others producing only minimal visual impairments. Failure to recognize the precise nature of the problem may lead to unnecessary laser capsulotomy procedures.
Conclusion:
Clinical degradations of intraocular lenses are uncommon but have been reported following the implantation of intraocular lenses made of differing biomaterials. Their correct identification and thorough investigation to determine the underlying cause is necessary for optimal patient management and the prevention of such problems. Choosing a lens made of a particular material may be important in patients with certain ocular conditions.
Introduction
Cataract surgery is the commonest surgical intervention in the developed world, with more than a million such surgeries being conducted annually in the United States, 350,000 in the United Kingdom and 20 million worldwide. 1 With modern surgical techniques, visual and refractive outcomes are excellent with almost 95% of eyes achieving 0.3LogMar corrected acuity or better. 2 As such, not only is it the most common surgical intervention but also one of the most successful, with increasingly high outcome expectations. 3
Among the many innovations that have contributed to the superior outcomes of modern cataract surgery, the development of the intraocular lens (IOL) implant is of paramount importance. The concept of replacing the cataractous lens in cataract surgery with a prosthetic implant to improve unaided visual acuity (VA) and reduce dependence on spectacles, was first proposed by Sir Harold Ridley who implanted the IOL on 8 February 1950 at our unit, St Thomas’ Hospital, in London. 4 These initial lenses were manufactured by Rayner Ltd. (Worthing, UK) and made of Perspex CQ polymethylmethacrylate (PMMA). This material was apparently chosen as Sir Harold had noted that it was inert after seeing Royal Air Force personnel with pieces of intraocular Perspex from shattered canopies in World War II. 4
Any IOL, implanted during cataract surgery needs to meet certain basic criteria, such as being biocompatible, causing no inflammation or tissue reaction either in the short (months), medium (years) or long term (decades), have excellent optical properties to restore vision and maintain its clarity and shape. While clinical and material degradations of IOLs are uncommon, they have been reported and may cause significant visual impairment, necessitating lens explantation. Several types of degradations including photochemical material alterations, surface precipitations, depositions with the IOL material itself, water vacuolation (glistenings), surface coatings and discolouration have been described. Investigation of these changes shows them to be typically related to the type of IOL material used and/or the manufacturing process to create such implants. Such conditions need to be recognized not only to avoid unnecessary laser capsulotomies, which may make any subsequent lens explantation problematic, but also to limit the future occurrence of such problems. The purpose of this review is to describe the clinically apparent material degradations that can occur in IOLs, how and why they have occurred and their typical clinical consequences and management.
Degradation/opacification/discolourations within the IOL
Photochemical material degradations of PMMA IOLs
The first IOLs were manufactured from PMMA. 4 This material appeared to be biocompatible and has been successfully used in cataract surgery for almost seven decades. Indeed, while in modern small-incision cataract surgery, rigid PMMA IOLs have been superseded by foldable silicone and acrylic polymers, they are still implanted as sulcus lenses and often routinely in the developing world, where phacoemulsification small-incision surgery may not be available.
In 2002, Apple et al. 5 reported 25 cases in 18 patients of late-postoperative degeneration (typically over 10 years) of 3-piece posterior chamber PMMA IOLs of which 10 were explanted due to visual loss. They documented spherical, white-brown crystalline opacifications within the optic of the IOL, composed of compressed, degenerated PMMA surrounded by an outer clearer area, which they described as ‘snowflake-like’. This condition occurred in lenses from more than one manufacturer, but in some cases was restricted to certain lot numbers. Since this time, other investigators have documented similar cases.6–11 They also typically occurred several years after implantation, are present in the central and mid-peripheral zones of the optic with a clear zone around the optic edge, which is the portion covered by iris. The anomalies are usually focal with intervening areas of clarity, but occasionally can coalesce to form a confluent area of opacification. These opacities are not on the surface but within the anterior third of the substance of the optic and on X-ray spectroscopy the lesions are made of non-organic material.5–7 They do not disappear when the lens is explanted and dried, which distinguishes them from glistenings (described later), which are typically small water filled vacuoles. However, while these snowflake lesions are described as ‘dry’, water does collect within the affected area upon hydration, presumably from associated surface cracks and this can worsen the opacification. 7
Based on the findings described above, it has been postulated that the changes may be due to chronic light exposure causing material degradation of the PMMA. The exact nature of this material photochemical degradation is unknown and requires further investigation, but Werner 6 have suggested that possible causes might have been insufficient post-annealing of the cured PMMA polymer, excessive thermal energy during curing causing voids in the polymer matrix, non-homogeneous distribution of the ultraviolet chromospheres and/or possible poor filtration of pre-cured monomeric components. It is unlikely that this degeneration will represent a significant problem in the future, as the majority of these lenses were implanted in the 1980s to early 1990s, so the majority of patients are now deceased. In addition, manufacturing processes have changed over the past three decades and modern PMMA lenses are mostly produced by lathing, which eliminates the possible causative steps postulated above.
Glistenings
Glistenings are small water-filled vacuoles within the IOL material (Figure 1). They are reported to be between 1 and 30 µm in size and are thought to occur when water permeates micro-channels within the IOL material and forms small inclusions.12–14 Due to the difference between the refractive index of the glistenings and the IOL material, they act as refractile particles that glisten on slit lamp examination. The first reports of glistenings date to 1984 and were described by Dr Norman Ballin 15 in a ‘Surgidev Leiske’ IOL with a hydrophobic poly (methyl methacrylate) optic. He later acknowledged credit for the actual initial observations of glistenings to Dr John Pearce, who had observed them several years earlier (J. Pearce, MD, ‘Glistenings Observed in Injection-moulded Optics’ (letter) Ocular Surgery News, 15 October 1985). 15
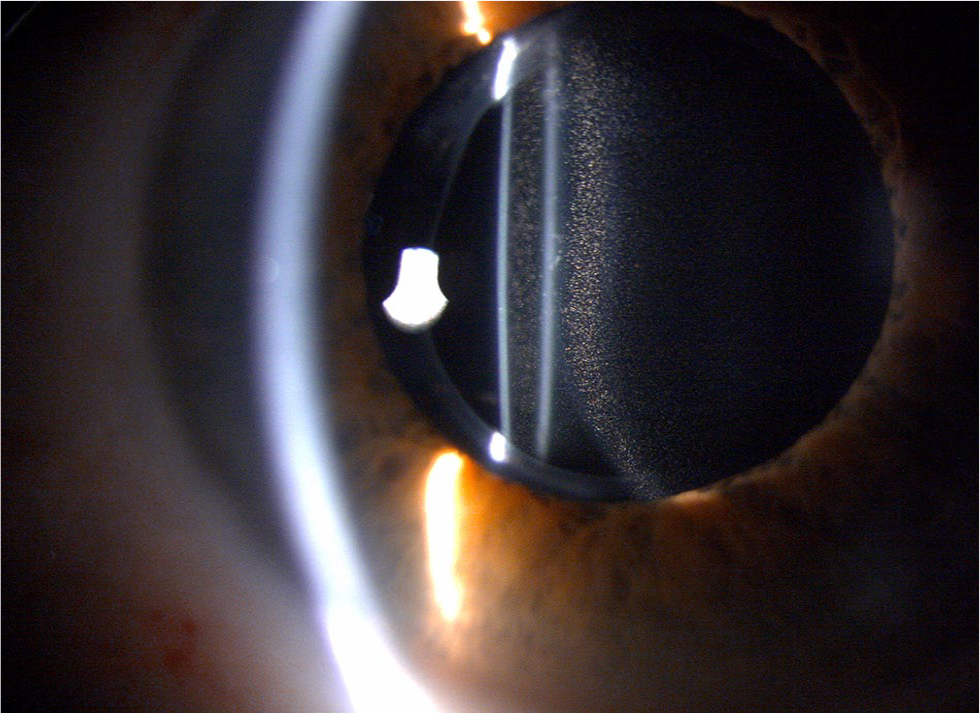
Slit-lamp photograph of glistenings within an AcrySof IOL appearing as multiple small refractile bodies within the bulk of intraocular lens optic.
While most reports of glistenings have been in hydrophobic acrylic lens materials,16–19 they have also been reported in PMMA17,20 silicone17,21 and hydrophilic acrylic IOLs. 22 Tognetto et al., 16 while investigating glistenings prospectively in a series of foldable IOLs, found them to be present in silicone (CeeOn Edge 911A, Pharmacia & Upjohn, Bridgewater, NJ, USA and SI40NB; Allergan, Irvine, CA, USA), hydrophilic acrylic (ACR6D, Corneal®, Corneal Laboratories, Pringy, France, Hydroview H60M, Bausch and Lomb Surgical, Rochester, NY, USA and Stabibag, IOLTECH laboratories, Carl Zeiss Meditec Inc., Germany) and hydrophobic acrylic (AcrySof, Alcon Laboratories Inc., Fort Worth, TX, USA and Sensar, AMO, Santa Ana, CA, USA) IOLs. However, the hydrophobic acrylic ‘AcrySof’ group had a higher percentage and a greater density of glistenings than the other IOLs studied. 16 Similarly, Rønbeck et al. 17 followed patients implanted with three different IOL materials for 12 years and found glistenings in all three IOLs, but they were more prevalent in the hydrophilic acrylic lenses (AcrySof MA60BM) than in the silicone (SI40NB, AMO) or heparin-surface-modified PMMA IOLs (8090C, Pharmacia & Upjohn).
The incidence of glistenings varies between published studies. In AcrySof IOLs, Davison 23 reported an 11% incidence of glistenings in the AcrySof SA30AL and 0% in the AcrySof SA60AT model (Alcon Laboratories) albeit at only 3 months, while Waite et al. 24 reported a 100% incidence in AcrySof SA60AT and SN60AT models and Leydolt et al. 25 a 97% incidence in AcrySof SN60WF IOLs at 3 years. Kahraman et al. 26 found that the presence of glistenings increased from 66% at 1 year to 86% at 3 years and was 100% at 5 years post-implantation of the AcrySof SA60AT IOL. This was similar to Tognetto et al., 16 who documented an increase in the incidence of glistenings in AcrySof IOLs with time, while interestingly, they seemed to stabilize after 6 months in IOLs composed of other materials.
This increase in glistening with time in AcrySof IOLs has been reported in several studies.27–30 Dhaliwal et al. 27 identified that in a series of AcrySof IOLs, glistenings developed within weeks after implantation, but in some patients the number of glistenings reduced with time. Christiansen et al. 13 found no statistically significant increase in glistenings over a 4-year follow-up period, although there was a positive trend. Colin et al. 28 in a retrospective study of AcrySof SN60AT, SN60WF and SA60AT IOLs found stabilization of glistenings over time, with over 2 years’ follow-up in many eyes. More recently, Johansson 29 found that glistenings developed in AcrySof SN60WF IOLs, with an increase between 2 and 3 years after implantation, with as part of this randomized, controlled study, only a small number of glistenings seen in hydrophobic acrylic ZCB00 IOLs (AMO, Santa Ana, CA, USA) with no increase in their number in these lenses with follow-up. Similarly, Moreno-Montañés 30 reported that frequency and intensity of glistenings in AcrySof MA30BA IOLs increased with time up to 30 months after surgery and Behndig and Mönestam, 31 with Scheimpflug photography, documented an increase in glistenings number with time with a mean follow-up time of 105 ± 33 months (range, 21–137 months).
Two main theories concerning the development of glistenings in IOLs have been proposed, 32 namely water absorption due to environmental temperature change 12 and osmolarity change under isothermal conditions. 33 The first theory is based on the observation that the water absorption rate of polymers changes according to temperature. This theory proposes that glistenings are a result of IOL material water absorption due to environmental temperature changes. 12 The second theory proposes that a change in the osmolarity of the external environment within the eye can lead to an influx of water into the IOL material under isothermal conditions. 33 It is of note that the IOL material water content varies in differing materials. Hydrophobic acrylic polymers generally have low water content (less than 0.5%), 34 as do silicone IOL materials (less than 0.4%)34,35 and PMMA IOLs (0.4%–0.8%), 34 while hydrophilic acrylic materials have higher water contents (up to 38% in some materials). 34 However, the water content can vary in different environmental and aqueous solutions and how this may or may not relate to glistenings formation is unknown.
AcrySof is composed of a cross-linked polymer network that can absorb significant amounts of water, which can be increased with temperature changes. Dhaliwal et al. 27 showed that glistenings were related to hydration of the acrylic material and that they could be reversed by drying the IOL for 48 h. Kato et al. 12 reported that even small changes in temperature (e.g. 37°C–34°C) were enough to initiate glistenings formation and proposed that this occurrence may involve spinodal decomposition of the swollen polymer network, initiating the formation of microvacuoles consisting of water and loosely packed network chains. Kato et al. 12 showed that water content of the IOL material increases upon heating and that glistenings formation occurs upon their cooling, and the latter is also dependent on the rate of temperature change.
While changes in temperature,12,27 equilibrium water content, 36 osmotic changes, 33 environmental factors30,36 and equilibrium water content 14 are important in the development of glistenings in IOLs, other factors are also relevant. Control of the polymerization process, to make it as uniform as possible, appears to play a role, 32 with surface scattering and glistenings formation found to be more significant with IOLs manufactured by cast moulding than by lathe cutting. 32 In order to reduce the occurrence of glistenings in AcrySof IOLs, Alcon Laboratories Inc. altered the manufacturing process in the early 2010s, implementing tight environmental and process controls in the formulation, cast moulding and curing operations.37,38 Subsequently, Miyata et al. 37 found that surface light scattering due sub-surface nanoglistenings was significantly reduced and Thomes and Callaghan 38 found that the percentage of IOLs with glistenings, induced in the laboratory, with a density of >100/mm2 was 99% in the 2003 AcrySof IOL models and only 4.8% in AcrySof IOLs manufactured in 2012.
Breakdown of the blood aqueous barrier (BAB) and intraocular inflammatory factors may also be associated with the development of glistenings. Dick et al. 39 found that with AcrySof IOLs the incubation of these lenses in fluid containing serum increased vacuolation. They proposed that lipids within the serum can reach the cavitations in the acrylic material and become visible, as the space between the cross-linked molecule chains in the AcrySof polymer enhances the deposition of such hydrophobic substances. It is of note that an association between glistenings and diabetes mellitus, where there is often a breakdown of the BAB, has been documented.32,39 Werner 32 reported an incidence of glistenings in a group of diabetic patients of 76% compared with 47% in non-diabetic patients. Indeed, they found that 21% of their so-called higher grade glistenings were in those patients with diabetes compared with 5.5% in non-diabetics. 32 Interestingly, Colin at al. 28 documented an association between the incidence of glistenings and glaucoma, which it has been postulated may be due to preservatives in topical anti-glaucoma medicines that can lead to the breakdown of the BAB. In addition, uveitis 40 and postoperative inflammation, 30 which both result in BAB breakdown, have been linked to glistenings formation. Indeed, complex/prolonged surgery, which typically results in a higher degree of inflammation and BAB breakdown, has been found to be associated to glistenings occurrence. 30
Other suggested factors that might be associated with the development of glistenings include the ‘tightness’ of the capsular bag 41 and the presence and degree of anterior capsular opacification (ACO). 29 This was postulated, as in a few randomized, controlled studies the ZCB00 IOL (AMO, Santa Ana, CA, USA), which is made of a hydrophobic acrylic polymer, appeared to have much less propensity to glistenings development than similar Alcon AcrySof IOLs, also manufactured from an acrylic polymer. As the ZCB00 IOL has an elevated anterior rim, which lifts the anterior capsule from the anterior optic surface, appearing to result in less anterior capsular fibrosis than that seen with the AcrySof lenses that are biconvex, it was then suggested that the occurrence of ACO and capsular bag ‘tightness’ might be important in glistenings creation.26,29
Finally, a positive correlation between higher IOL power and the presence of glistenings has been established,30,42 although this relationship appears intuitive as higher powered IOL are thicker with a larger volume of material, and therefore may have a greater chance of developing degradations.
Clinical studies investigating the association between glistenings and visual performance have produced conflicting results. While most have demonstrated no significant effect of glistenings on vision,22,24,28,42–45 a few have found that high numbers of such vacuoles within IOLs impair visual performance,13,14 especially high spatial frequency contrast sensitivity.27,46–48 Waite et al. 24 in a longitudinal study of up to 3 years in AcrySof IOLs, found no correlation with corrected distance visual acuity (CDVA) and glare testing and glistening size or density, although they felt that the effects of glistenings on high spatial resolution contrast acuity required further investigation. Mönestam and Behndig, 42 in a series of 103 patients with 10-year follow-up, documented no significant impact between glistenings grade and vision, including low-contrast VA at 10% and 2.5%. Colin et al. 28 in a series of 157 of 260 eyes with glistenings and up to 7 years’ follow-up in some eyes, found no association between glistenings and VA. The same research group in a further study of yellow-tinted AcrySof IOL in 111 eyes of 74 patients, 43 reported that although there was a trend towards decreased visual acuities at higher glistening grades, there were no significant differences in CDVA between their glistening severity groups. Chang et al. 44 in 80 patients in a randomized, controlled trial at 5–7 years after surgery stated that glistenings were not correlated with CDVA and confirmed this in a follow-up study of the patients at 9 years. 22
However, Christiansen et al. 13 in 42 eyes implanted with AcrySof IOLs found that Snellen acuity in eyes with severe glistening grades was statistically less than those with mild glistenings. Xi et al. 46 in 120 eyes implanted with AcrySof IOLs at 2 years following surgery found that while there was no statistical correlation between glistening grades and unaided distance visual acuity (UDVA), CDVA and contrast sensitivity, sub-analysis did show more eyes with severe glistening grades had reduced contrast sensitivity at high spatial frequency. Henriksen et al., 14 in 79 eyes with glistenings in AcrySof IOLs, showed a correlation between glistening size and density and distance acuity and contrast acuity with glare. Gunenc et al. 47 in 34 eyes with glistenings in a series of 94 eyes found no statistically significant difference in VA and contrast sensitivity at low or medium spatial frequencies between eyes with glistenings and those without, although they did document a difference at high spatial frequency. Schweitzer et al. 48 in 67 pseudophakic eyes in 47 patients with coexisting glaucoma not only showed that a higher number of topical glaucoma medication were associated with a higher glistening severity grade (probably due to breakdown of the BAB as discussed above), but that higher grades of glistenings density had lower mean contrast sensitivity values at high spatial frequencies, although there was no difference in CDVA.
It seems therefore that in most eyes, glistenings are likely to have little effect on visual performance, except in some eyes with very high densities of glistenings, when high spatial contrast acuity is preferentially affected. It is of note, however, that most of these studies have used subjective glistening grading systems with the methods for using these scales often unclear13,14,27,43,47 While the number of glistenings is likely to be important, size and distribution might also be expected to affect vision. Most reported glistenings grading systems have a 3- to 4-point ordinal scale, which might lack sensitivity depending on the grade boundaries and implementation. In addition, and importantly, published studies typically rely on subjective counting and grading of glistenings ‘per field’ of slit lamp13,49 or ‘in the slit lamp’28,43 without defining the regions of the IOL being studied or the illumination parameters used when viewing the glistenings. Clearly, such lack of standardization will introduce variability in glistenings assessment that could provide a partial explanation for the differences in the results of studies described above using subjective assessment. In addition, a further important variable will be differences in the visual tests employed in these studies and their sensitivities and the existence in some eyes of visually significant comorbidities. To address such issues, in a recent study Stanojcic et al. 45 using a defined, reproducible, standardized 8-point ordinal scale of glistenings density and an array of computerized visual function tests, including contrast sensitivity and forward scatter, investigated the visual effects of glistenings in vivo in 34 eyes implanted with AcrySof IOLs (SA60AT) in patients with no other ocular or neurological morbidities. They found no association between glistening grades and visual function. 45
Additional evidence that supports the results of studies that demonstrate glistenings have little effect on vision comes from explantation rates. In 2013, 67 cases of IOL glistenings associated with visual impairment were reported to the Canadian government, one of which was said to have been explanted. 50 Similarly, Raven et al. 51 reported a case in which an AcrySof IOL required explantation due to intractable symptoms in bright light and when driving at night. Dogru et al. 52 also reported such a case, although it is of note that this patient developed glistenings several months after neodymium: YAG laser capsulotomy and this may have contributed to development of glistenings by disrupting the IOL material integrity. Similarly, Werner et al. 53 reported a case of explanted 3-piece AcrySof IOL because of glistenings that impaired fundus visualization. Because of coexistent retinal disease, the effects of glistenings on visual function could not in this case be ascertained. It appears therefore that glistenings can, albeit very rarely, cause clinically significant changes in vision. Hopefully, however, with the improvement in AcrySof IOL manufacture, introduced in the early 2010s and the development of newer ‘glistenings free’ hydrophobic acrylic polymers, such problems may be negated.
Postoperative degradation/opacification of silicone IOLs
Werner et al. 54 reported on six cases of 3-piece silicone IOLs (SI-40NB, Allergan, Westport, Ireland), which required explantation due to early (hours after surgery) opacification and associated visual loss. The lenses had been implanted in four different locations in Brazil and France, with the Brazilian lenses stored at the same location. The lenses underwent microscopy (including electron microscopy in one case) as well as gas chromatography–mass spectrometry (GC–MS) analysis and/or extraction by isopropyl alcohol or acetonitrile. All lenses had white optic opacification in the hydrated state, becoming transparent on drying. Unusual exogenous chemical compounds were identified, including terpenes and ketones, which are typically found in industrial cleaning agents and fumigants. It was postulated by the authors (although no clear history of chemical contamination could be identified) that spraying of the storage area with cleaning compounds and insecticides caused chemical contamination of the IOLs rendering the silicone material more hydrophilic so the influx of water into the IOL material was rapidly possible after implantation. 54 It is of note that many IOLs are enclosed in semi-permeable packages to allow sterilization by ethylene oxide gas, while at the same time being impermeable to infective microorganisms and contaminants. It is therefore feasible that during cleaning or disinfection of storage rooms, aerosolized solutions might introduce chemicals through the package and onto the IOLs.
Elgohary et al. 55 reported two similar cases of silicone (multifocal) IOLs, with opacification occurring within weeks of surgery. No obvious cause was apparent, and they suggested that possible causes might be the presence of low-molecular weight silicone fractions that were not cross-linked during the curing process, large polymer impurities due to inadequate filtering leading to IOL hydration and interaction between silicone and intraoperative or postoperative medications. Tanaka et al. 56 also reported a similar case of a silicone SI40NB (Allergan, Westport, Ireland) IOL which opacified with a brown haze within 24 h of implantation, requiring explantation. Microscopic examination of the extracted IOL showed numerous spheroid structures, which the authors proposed may be due to water incorporation into the silicone IOL material.
Milauskas 57 in 1991 reported 15 cases of brownish discolouration of two silicone IOLs, manufactured by IOLAB Corp, Claremont, CA, USA, and STAAR Surgical Co., Monrovia, CA, USA, which was documented 15–60 months after implantation. VA was 20/30 or better in all cases and no lenses were explanted. Two similar cases in the same lens type were reported by Koch and Heit 58 in 1992. No cause for this problem was identified, but it could be postulated that it may be due to ingress of water/water vapour into the lens due to anomalies in the manufacturing process. It is of note that the effects on visual performance appeared to be minimal and there have been no further reports in the literature possibly due to improvements in manufacturing techniques.
In 2007, Werner et al. 59 reported 12 cases of late (4 weeks to 2 years) opacification of silicone lenses in the United States. The opacification was generally less than they had observed in their series of early onset (weeks) opacification of silicone IOLs. 54 They undertook GC–MS analysis as in their previous study and found benzophenone in 7 of the 12 IOLs, which may or may not have been implicated. Improvements in the manufacturing process since this problem was documented seem to have prevented the problem from recurring.
Jones and Irwin 60 in 2002 reported a case of ‘rose-colour’ discolouration of a silicone IOL (model SI-30NB; Allergan Inc., Irvine, CA, USA). This patient had undergone bilateral cataract surgery several years earlier. This patient had been on Rifabutin therapy for mycobacterial infection for over 10 months, which was discontinued after the IOL discolouration was documented. Corrected VA was 20/20 and there were no perceived VA or colour discrimination problems by the patient, so the IOLs were not explanted. In a laboratory investigation, 60 the authors immersed IOLs from four different manufacturers representing three materials for 1 week in a concentrated Rifabutin solution. All lenses remained clear except for the silicone lenses which were discoloured rose, with the discolouration fully penetrating the lens.
In 2007, Stevens et al. 61 reported discolouration of a silicone IOL (SI40NB; AMO, Irvine, CA, USA) in a patient who presented immediately postoperatively with corneal oedema and a blue IOL. A ‘blue dye’ had been used to enhance visualization during capsulorhexis. It was determined that methylene blue had been used instead of trypan blue in this case staining the IOL. The IOL was explanted and the corneal oedema resolved within 1 month. Microscopic analysis of the explanted IOL revealed that its surface and internal substance had been permanently stained blue. In a separate experiment, the authors immersed IOLs of differing materials (silicone, hydrophobic acrylic, hydrophilic acrylic and PMMA) in methylene blue at varying concentrations. All IOLs, except the PMMA lenses were permanently stained, with the hydrophilic acrylic lenses stained most intensely. 61 Methylene blue is not appropriate for intraocular usage, with Trypan blue being the appropriate dye for anterior capsule staining.
Katai et al. 62 in 1999 reported a case of ‘brown’ discolouration of silicone IOLs (STAAR Surgical Co., Monrovia, CA, USA) in both eyes of the same patient. This patient had been treated with Amiodarone for 3 years. It was proposed that Amiodarone can cross BAB under certain conditions, and possibly after vitrectomy, which this patient also underwent in their left eye, and which resulted in unilateral worsening of discolouration. Contrast sensitivity and blue colour sensitivity were found to be impaired in this patient’s right eye. The authors proposed that minute particles including water vapour that could not be removed by filtering may have also caused this brown discolouration.
Sathyan et al. 63 reported a non-progressive green discolouration in a silicone IOL (Allergan SI-40NB, USA). This was documented 6 months after surgery in two patients. Contrast sensitivity without glare was slightly reduced but not the VA and the patients were asymptomatic. No cause for discolouration has been elucidated. In 2008, Venkatesh et al. 64 reported a similar case of green IOL discolouration. There were no visual complaints and the patient had a best-corrected VA of 20/20 with normal colour vision and contrast sensitivity. The explantation was required and no cause is yet established.
Opacification/discolourations of hydrophilic acrylic IOLs
Werner et al. 65 in 2002 reported a blue discolouration of a hydrogel IOL, ‘Acqua’ IOL (Mediphacos, Belo Horizonte, MG, Brazil). This patient underwent cataract surgery using Trypan blue 0.1% to stain anterior capsule and presented at 7 days with ‘dark and double’ vision, with CDVA of 20/60. After explantation 2 months later, CDVA improved to 20/25. Microscopic analysis showed dark blue staining, denser in the optic, especially in its periphery, with the blue discoloration remaining even after 24 h of immersion in balanced salt solution. Trypan blue should probably be avoided in cases where a high water content IOL, such as hydrophilic acrylic IOLs, is to be implanted and/or complete anterior chamber irrigation undertaken before lens implantation.
Ghosh and Goodal 66 in 2004 reported five cases with ‘total IOL’ opacification a single-piece acrylic hydrophilic IOL (Aqua-Sense, Ophthalmic Innovations Inc., Ontario, CA, USA). In two cases, opacification was mistaken for posterior capsule opacification (PCO) and in one case for a non-resolving diabetic vitreous haemorrhage. The patients in five of these cases had significant visual deterioration due to total opacification of the IOL more than a year after surgery and explantation was performed in most cases. After consultation with the manufacturer, it was suspected that opacification was due to an interaction between the silicone sleeve, used to hold the IOL in the vial, and the acrylic material of the IOL, which may have created negative charge resulting in opacification. These IOLs have been withdrawn.
Opacification/discolourations of hydrophobic acrylic IOLs
Manuchehri et al. 40 described ‘brown deposits’ in IOLs in a series of pseudophakic, uveitis patients (54 patients; 71 eyes). These were said to be distinct from glistenings and difficult to image. The implantation of AcrySof MA60BM hydrophobic acrylic IOLs was strongly associated with these deposits. This lens is known to be associated with glistenings formation. One can therefore speculate that these deposits might have been a variation of glistenings. Albeit, rather than water vacuoles, the vacuoles within these IOLs may have contained different organic/inorganic material in association with the uveitis documented in these cases and perhaps topical medications used to treat this condition.
More recently, a series of 14 brown discoloured AAB00, ZCB00 and ZMBOO IOLs (AMO, USA) was recently reported by Wong et al. 67 The browning of the IOLs was noted as early as day 1 postop and as late as 327 days. No patients had loss of lines of CDVA. However, desaturated Lanthony D15 Hue test was abnormal in 8 of 16 eyes. The authors were not able to find a clinical cause for the discolouration but suspected it was due to impurities in the IOL that occurred during the manufacturing process. No patient required IOL exchange.
Twenty years after his first report of brown discolouration in silicone IOLs, Milauskas 68 in 2012, reported brown discolouration of two AcrySof (no specific IOL model provided but author suggested a blue-light filtering IOL) hydrophobic acrylic IOLs and a yellow hydrophobic acrylic PY-60AD IOL (Hoya Surgical Optics GmbH, Singapore). The implantation of these IOLs was between 6 months and 8 years. In some of these IOLs, glistenings coexisted with discolouration, and the author noted that discolouration occurred around glistenings. He also concluded that both Alcon and Hoya IOLs used the same blue-filtering agent, and that glistenings may play a role in discolouration of IOLs. Assessment of visual function was difficult due to multiple patient comorbidities.
Surface depositions/degradations/coatings of IOLs
Calcification
The deposition of calcium within tissues, may be either physiological or pathological, and can also occur on any bioprosthetic or biomaterial implant in the human body such as heart valves, blood pumps, intrauterine contraceptive devices, contact lenses, scleral buckles and IOLs. 69 Neuhann et al. 69 have proposed three possible routes for IOL calcification: primary calcification, which is related to the IOL itself (e.g. the polymer, manufacturing or packaging process), secondary, which is not only dependent on the IOL but also associated with pre-existing disease that may involve breakdown of BAB and, finally, false positive calcification or pseudo-calcification that occurs due to misdiagnosis of tissue artefacts or incorrect use of special stains.
The pathogenesis of IOL calcification is not fully understood. 70 Two possible mechanisms have been proposed for calcification of biomaterials: intrinsic (material-dependent) and extrinsic (host- and cell-dependent). 69 Extrinsic calcification may be due to foreign body reaction to the biomaterial and it has been suggested that blood cells, devitalized cells, bacterial, inflammatory cells or lipids may provide an initial nidus for calcification. 69
IOL calcification has most commonly been associated with surface deposition on hydrophilic acrylic IOLs,69,70 but also has been reported in silicone IOLs in the presence of asteroid hyalosis.71,72 Wackernagel et al. 71 and Foot et al. 72 in the early 2000s reported opacification of plate haptic IOLs occurring a few years after cataract surgery in the presence of unilateral asteroid hyalosis. These lenses were explanted, and white deposits were documented on the posterior lens surface only. Light microscopy, scanning electron microscopy and dispersive X-ray spectrometry showed the deposits consisted of calcium and phosphate, presumably hydroxyapatite. It was hypothesized that this deposited material might be derived from the asteroid bodies within the vitreous themselves or due to the process that is responsible for this condition. Werner et al. 73 described a similar case in one eye implanted with a 3-piece silicone IOL SI30NB (AMO, Irvine, CA, USA) in a patient with bilateral asteroid hyalosis. The IOL was explanted, while the other eye in which an acrylic IOL was implanted did not develop opacities with 6 years of follow-up. More recently, Stringham et al. 74 (16 eyes) and Espandar et al. 75 (3 eyes) have also described cases with posterior surface calcification on silicone IOLs in the presence of asteroid hyalosis. In the last report, laser capsulotomy was documented to make IOL explantation/exchange problematic. 73 While such cases are rare considering the vast numbers of silicone IOLs that have been implanted, the use of such lenses in the presence of pre-existing asteroid hyalosis needs to be carefully considered and the selection of an IOL with another material may be prudent.
As discussed above, IOL surface calcification has most commonly been on hydrophilic acrylic IOLs.70,71 Apple et al. 76 and Werner et al. 77 in 2000 were the first to describe calcification in foldable hydrogel ‘Hydroview’ IOLs (Bausch and Lomb Surgical, Rochester, NY, USA). Surface staining of explanted IOLs with Alizarin red, suggested that the deposits on the lens surface, both anterior and posterior, were composed of calcium and phosphates. According to this group at this time in 2000, there had been 76 cases in 9 centres worldwide with the same anomaly and in 17 of these cases the IOLs were explanted.
There have since been multiple reports in several different hydrophilic acrylic IOL models from different manufacturers both in the United States and Europe.6,69,78–82 Within the United States during the early 2000s, four major designs of IOLs seem to have had problems with deposits on the optic surface made up largely of calcium and phosphate: ‘Hydroview’ (Bausch & Lomb Surgical, NY, USA), ‘Memory Lens’ (Ciba Vision Duluth, GA, USA), ‘SC60B-OUV’ (Medical Developmental Research, Clearwater, FL, USA) and ‘Aqua-Sense’ IOLs (Ophthalmic Innovations International, Claremont, CA, USA).6,69,78–82 Time to explantation of these IOLs was approximately 2 years with microscopic analysis, as well as X-ray spectroscopy of explanted IOLs confirming the presence of calcium and phosphate within the deposits on the IOL hydrophilic acrylic surfaces.77–82
The precise pathophysiology of the factors involved in the calcification of these IOLs is yet undetermined. Dorey et al. 80 using energy dispersion X-ray spectrometry showed that many of the deposits were composed of calcium and phosphate in an electron-dense periphery with silicone in the electron-lucent centre. They proposed that the silicone gasket in the ‘Surefold’ packaging system, manufactured specifically for the ‘Hydroview’ IOL, might be responsible, contaminating the lens with silicone particles on the IOL surface, which then act as a nidus for calcium deposition. 80 It was of note that the IOLs in packaging prior to introduction of the silicone gasket did not appear to opacify and that the manufacturer (Bausch and Lomb) changed packaging to one sealed with a gasket made from a perfluoroelastomer rather than silicone to negate this problem. Guan et al. 83 and Wu et al. 84 examined the role of silicone compounds in the calcification of hydrophilic acrylic IOLs, examining their interaction with long saturated fatty acids. They showed that IOL surfaces treated with fatty acids, such as behenic acid, present in aqueous humour, calcify in vitro. They suggested that hydrophobic cyclic silicones adsorbed on the IOL surfaces can interact with hydrophobic hydrocarbon chains of the fatty acids to create a layer of amphiphiles which may act as sites of calcification. 83 Werner et al. 82 also demonstrated the presence of silicone compounds on the ‘Memory Lens’ IOL and on and within SC60B-OUV and Aqua-Sense IOLs, suggesting their importance in the development of calcification of these hydrophilic acrylic lenses as well. Ophthalmic Innovations International (‘Aqua-Sense’ IOL) subsequently excluded siloxane silicone elastomers from their IOL packaging components to address possible contamination problems. In addition to manufacturers removing silicone compounds from their acrylic hydrophilic IOL packaging, Ciba Vision changed its polishing process of its ‘Memory Lens’ IOL with which it correlated the opacification problem. 78 Hunter et al. 85 reported a single case of calcification in a ‘Memory Lens’ IOL manufactured after this time, although this was attributed an intrinsic defect in the optic itself and not the mechanism described above.
Gartaganis et al. 86 examined explanted opacified hydrophilic acrylic IOLs, from the four types described above, chemically analysed aqueous humour from eyes in which the IOLs had been explanted and conducted in vitro experiments. They concluded that the opacification is due to the deposition of calcium phosphate crystallites, with hydroxyapatite predominating and the surface hydroxyl groups of the polyacrylic material polymer facilitating surface nucleation and calcific crystalline growth. 86 They also suggested that the calcium and phosphate may be derived from residual cataractous material and surgical technique such as cortical clean-up may be of importance, explaining the occurrence of unilateral cases in patients implanted with the same lens type in both eyes.
Since these initial case series and studies and despite changes in manufacturing and packaging, there have been multiple reports of calcification of other hydrophilic acrylic IOLs in the past decade, both in cataract surgery and other surgical situations. Werner et al. 87 published in 2015 a series of seven hydrophilic acrylic IOLs, six designs from five manufacturers that required explantation due to granular calcific surface deposits within the margins of the capsulorhexis or the pupil on the anterior IOL surface/sub-surface that caused decreased VA. These deposits had developed in these eyes after the patients underwent Descemet’s stripping endothelial keratoplasty (DSEK) (Figure 2). The authors proposed three possible causes for this calcification including: direct contact between the intra-cameral air and hydrophilic acrylic IOLs material, intra-cameral metabolic changes because of the presence of exogenous substances injected during surgery and exacerbated inflammatory reaction with breakdown of the BAB due to the surgical procedure itself. 87 They suggested that surgeons should be aware of this phenomenon following DSEK and Descemet’s stripping automated endothelial keratoplasty (DSAEK) procedures in pseudophakic patients with hydrophilic acrylic IOLs and counsel patients accordingly. 87 Similarly, Giers et al. 88 reported the occurrence of opacification of 13 hydrophilic IOLs, months to years after DSAEK and Descemet’s membrane endothelial keratoplasty (DMEK), identifying a thin layer of calcium-phosphate deposition just beneath the central, anterior IOL surface. These lenses typically required explantation. 88 Such reports suggest that surgeons might be advised to avoid using hydrophilic acrylic IOLs in patients who are likely to require corneal endothelial lamellar surgery, such as in eyes with Fuchs endothelial and other corneal endothelial dystrophies.
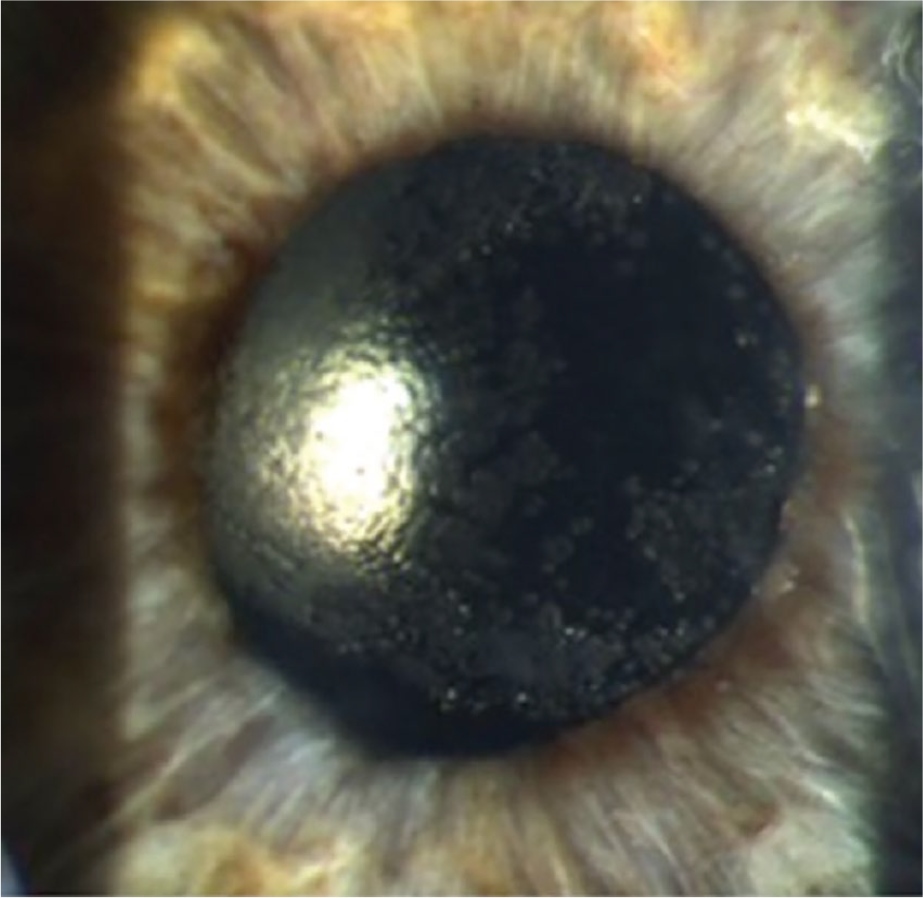
A hydrophilic acrylic IOL opacified following DSEK (courtesy of Mr M Nanavaty, Sussex Eye Hospital, Brighton, UK).
In addition to the injection of air/gas into the anterior chamber during DMEK/DSAEK procedure, similar changes have been reported after pars plana vitrectomy (PPV) and intravitreal gas injection. Recently, Marcovich et al. 89 reported 11 cases of hydrophilic IOL opacification, 1 month to 6 years after PPV with gas injection, with calcium and phosphate deposition on the anterior, central IOL surface in explanted IOLs. 89 They suggested that a hydrophobic IOL may be preferred when a simultaneous phacoemulsification and vitrectomy with intravitreal gas is being considered. It is of note, however, that there have been recent case reports of calcification of hydrophobic acrylic IOLs (AcrySof SA60AT) associated with intravitreal gas injection and retained perfluorocarbon liquid following vitreoretinal surgery, so that this problem is not entirely related to hydrophilic acrylic polymers. 90
Aside from air/gas injections, recombinant tissue plasminogen activator (rtPA) has also been recently reported to cause IOL opacification secondary to calcification in hydrophilic acrylic IOLs (Rayner C-Flex 570C and Rayner Superflex 620H; Rayner, Worthing, UK). Fung et al. 91 in a case series of seven eyes of seven patients reported IOL anterior surface/sub-surface opacification, which stained positive for calcium salts, within 12 months of the use of rtPA to treat inflammatory membranes that formed after cataract surgery. They proposed that the rtPA may have released sequestered calcium from the fibrinous inflammatory membranes and introduced phosphate ions contained in its buffer solution, potentiating calcium deposition. 91
Other reports of IOL calcification include those by Tandogan et al., 92 who documented in 2015 a series of explanted opacified ‘Euromaxx ALI313Y’ and ‘ALI313’ IOLs (ARGONOPTICS, Germany) hydrophilic acrylic IOLs. X-ray spectroscopy revealed fine granular surface deposits made of calcium and phosphate. These IOLs were explanted due to reduced VA, the reasons for the calcification in these eyes was not elucidated. Similarly, Zuberbuhler and Carifi 93 in 2012 reported a series of five patients with glittering deposits on the surface of hydrophilic acrylic IOLs (3C-flex 970C IOLs, Rayner, Worthing, UK) and two with Akreos AO (Bausch and Lomb Surgical, Rochester, USA). Disposable forceps were found to be the cause of these during injector loading process. None of the patients experienced visual symptoms. The IOLs did not undergo staining to see if these deposits were calcific. 93
In addition, there have been a number of recent reports concerning calcification in hybrid hydrophilic acrylic IOLs with hydrophobic surfaces manufactured by Oculentis GmbH (Berlin, Germany;94,95 Figure 3(a) and (b)). Gartaganis et al. 94 reported six cases with the Lentis LS-502-1 IOL, two of which had undergone vitreoretinal procedures. Analysis confirmed the presence of sub-surface formation of calcium phosphate crystalline deposits. Gurabardhi et al. 95 in 2018 reported the largest series so far (71 eyes, 63 patients) of these calcified acrylic hydrophilic IOLs with hydrophobic surfaces (LS-502-1, LS-402-1Y, LS 312-1Y, LS-313-1Y, L-402 and L-312). Light microscopy revealed numerous granules within opacified areas (optic and/or haptic) close to the surface or on the surface of the IOLs, which were positive for alizarin red 1% suggesting calcium deposition. The lenses were implanted between 2009 and 2012 and explantation was performed 4 years ± 1.2 (SD) after initial phacoemulsification. Ocular and systemic comorbidities were found without statistical correlation, with the most frequent being diabetes, uveitis and glaucoma. A definitive cause was not identified, but it was suggested by the authors that a manufacturing issue might be the reason. 95 This has been supported by a voluntary recall of lenses, implemented by Oculentis first in December 2014, who stated at that time that ‘analysis suggests a possible interaction between phosphate crystals originating from the hydration process of the IOL material and the fluctuating, batch related presence of silicone residues on some IOLs’. According to the relevant literature, ‘such residues may potentially change the IOL surface properties, making it under certain medical conditions more prone to deposition of calcium phosphate from the aqueous humour in predisposed patients. These deposits may compromise the optical transparency of the IOL, potentially leading to a reduction in the patient’s visual acuity’. In September 2017, Oculentis issued a further ‘Field Safety Notice’, applying to all Lentis foldable IOLs with model numbers starting with L-, LU- and LS- and having an expiry date between January 2017 and May 2020. Within this notice, they reported that they have identified the source of calcific opacification as phosphate-containing cleaning agent used in their production process, which they apparently changed in June 2015.
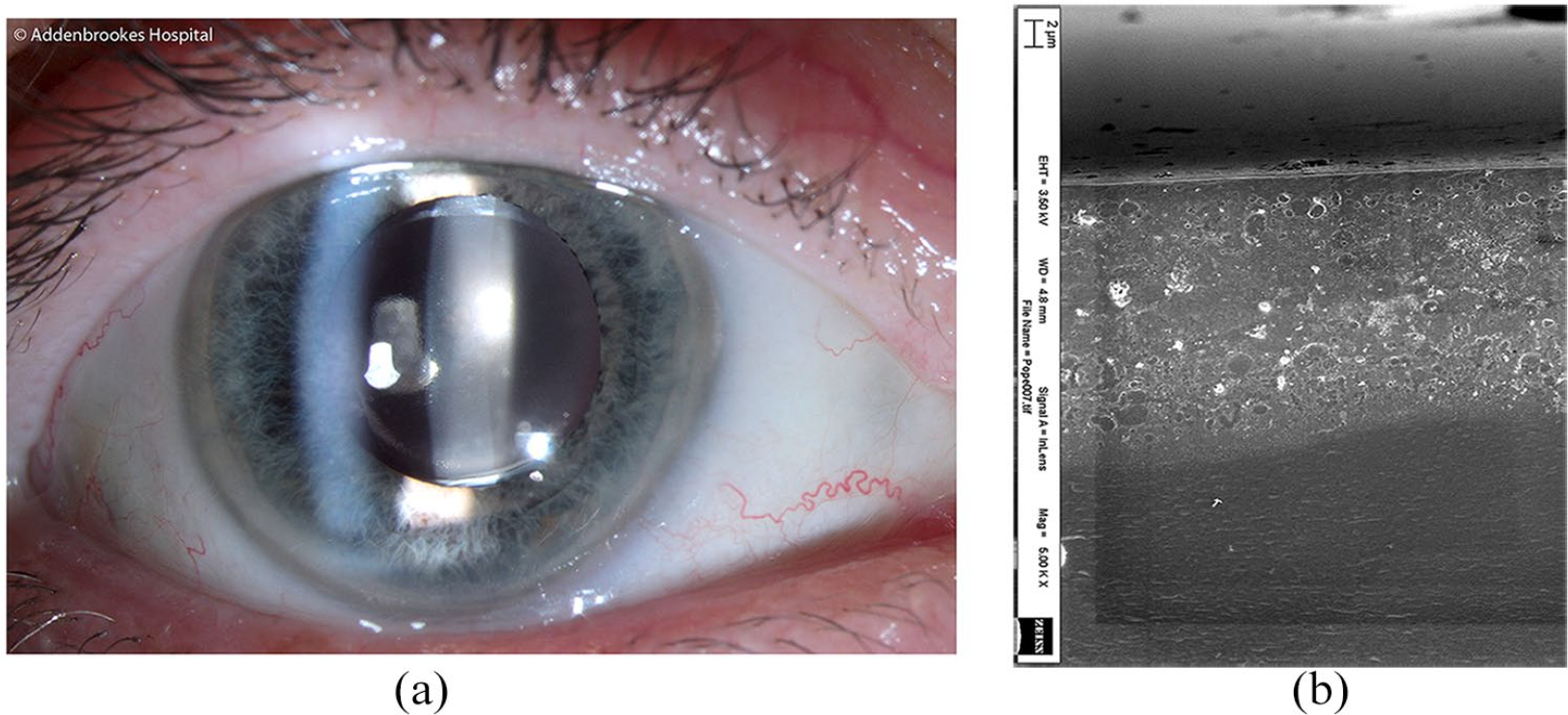
(a) Slit lamp image of a calcified Lentis (Oculentis, GmbH, Berlin, Germany) intraocular lens (Courtesy of Mr M Rajan, Addenbrookes Hospital, Cambridge, UK). (b) Electron microscopy (5000× magnification) of a cross section of a calcified LentisM30 (Oculentis, GmbH, Berlin, Germany) intraocular lens showing calcium deposits extending 20 μm from the lens surface (Courtesy of Mr J Stevens, Moorfields Eye Hospital, London, UK).
Such cases clearly highlight the need for vigilance on behalf of both surgeons and manufacturers alike to be aware of such problems, strongly consider analysis of any explanted IOL in a specialist centre to provide a definitive diagnosis, as well as feedback to the manufacturer and regulatory medical device agency. This requirement for increased post-market surveillance of medical devices is stated in the latest Medical Devices Regulation, issued by the European Union in April 2017 (Regulation (EU) 2017/745 of The European Parliament and of The Council of 5 April 2017 on Medical Devices. Available at: https://eur-lex.europa.eu/legal-content/EN/TXT/PDF/?uriZCELEX:32017R0745&fromZEN).
Sub-surface whitening/nanoglistenings
Surface light scattering was first reported in hydrophobic acrylic IOLs by Nishihara et al. 96 in 2003. They described ‘surface whitening’ of 40 patients implanted with AcrySof hydrophobic acrylic IOLs (Alcon Laboratories). They could only examine five eyes in four patients in vivo with a slit lamp and could therefore not elucidate the cause, as the lenses in these eyes were not explanted. They felt the problem was on the surface/sub-surface and was not due to glistenings (discussed above) as these are normally within the substance of the IOL, not on its surface. The authors postulated that the structure of the IOL polymer might have changed over time with reorganization of the surface or near the surface to produce such changes.
Further reports of such phenomena in AcrySof IOLs have attempted to elucidate the nature of these problems.97,98 Matsushima et al. 97 examined four explanted IOLs (due to dislocation) and found that light transmission in the visible range was only 4% less than that of unused IOLs, that X-ray analysis showed no calcium phosphate deposits, Fourier-transform infrared spectrophotometry showed no evidence of hydrolysis and that the opacification disappeared after drying of the IOLs but reappeared with immersion in physiologic saline. They postulated that it was likely that the ‘whitening’ of the hydrophobic acrylic IOLs was due to trace water molecules infiltrating sub-surface of the lens optic and that within the three-dimensional (3D) network of the acrylic lens polymer, water molecules were able to form aggregates of sufficient size to scatter visible light, causing opacification or so-called ‘whitening’ 97 (Figure 4).
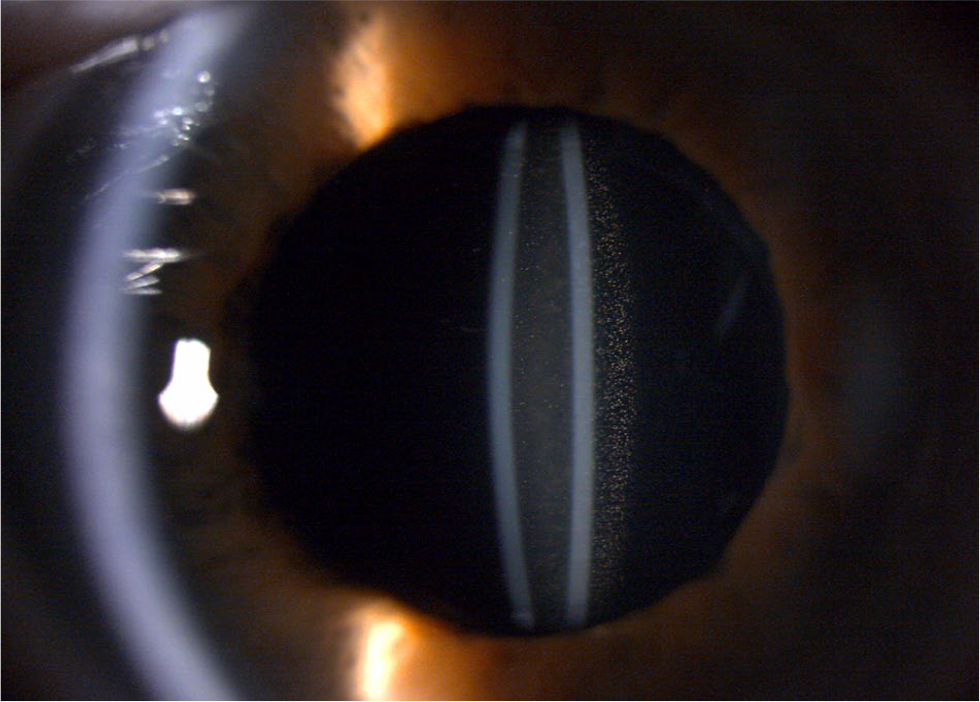
Sub-surface whitening or nanoglistenings seen as intense light scattering or whitening on anterior and posterior IOL surfaces. In addition, glistenings can be seen in the bulk of the IOL optic of an AcrySof SA60AT (Alcon Laboratories Inc., TX, USA).
Ong et al. 99 described a similar phenomenon to ‘whitening’, in AcrySof IOLs following explantations in five eyes and from human cadavers with non-implanted IOLs as controls. They found no inorganic/organic deposits on the IOL surfaces, but the hydration state of the IOLs significantly contributed to the intensity of surface light scattering and that clinically explanted and cadaver-eye explanted IOLs (but not control IOLs) exhibited minimal scatter when dry, intermediate scatter when wetted, and maximum scatter when hydrated. They documented on scanning electron microscopy sub-surface ‘nanoglistenings’, with diameters of less than 1 μm (between 140 and 185 nm) and within 120 μm of the IOL surface, as the source of the hydration-related surface light scattering.
Miyata et al. 100 investigated this IOL surface light scattering phenomenon and found it was greater in ‘AcrySof MA60BM’ and ‘AcrySof SA60AT’ IOLs (Alcon Laboratories) than that of ‘AR60’ and ‘ClariFlex’ IOLs (AMO, Santa Ana, CA, USA), although of note was that contrast sensitivity under photopic conditions was not statistically different among the four groups of IOLs at any spatial frequency. They reported that this scattering was due to uniform, membrane-like whitening of the IOL surface and was distinct from glistenings, concluding that glistenings and surface scattering differed in both location and appearance and probably in origin. 100 In a follow-up study, Miyata et al. 101 evaluated the surface light scatter using a Scheimpflug camera in a cross-sectional study of 466 eyes, implanted with either AcrySof 3-piece (MA30BA, MA60AC and MA60BM) or 1-piece (SA60BM) IOLs and showed that surface light scattering continued to increase up to 15 years postoperatively in all the AcrySof IOLs (Alcon Laboratories). 101 Unfortunately, they did not assess contrast sensitivity or assess for the presence of glistenings in the IOLs in this study, which could have influenced the results. Takahashi et al. 102 performed an optical simulation using ray-tracing software to evaluate visual effects of sub-surface nanoglistenings (SNG) in IOLs. They found that increased size and volume ratio of SNGs increased forward light scatter but that the modulation transfer function (MTF) was not affected. They also found that peak retinal irradiance reduced with increased SNG volume ratios. The limitation of this study was that the SNGs in this simulation were evenly distributed, which is not the case in real life. 102 The authors discussed an interesting observation, where visual function improved in patients with retinal diseases when IOLs with SNGs were replaced. Research has shown dissociation of Snellen acuity and contrast sensitivity, indicating that contrast sensitivity can be used as an early index of changes in the retina not demonstrated by measurements of VA. 103 The finding of no effect of SNGs on MTF by Takahashi et al. 101 is in line with findings by Werner et al., 104 who investigated light scatter and straylight in 17 AcrySof IOLs with SNGs removed from cadavers (11 SN60WF and 6 SA60AT; Alcon Laboratories). In addition to MTF, these authors examined Badal images obtained with the explanted IOLs through different size pupils and found no significant difference to controls (non-implanted IOLs). There was similar light transmission but increased light scatter in the explanted IOLs compared to control IOLs. However, the reported values were well below the value of straylight hindrance and the authors concluded that the light scatter caused by the SNGs would be unlikely to cause noticeable visual impairments. 104 Beheregaray et al. 105 also investigated the impact on visual function of SNGs in 42 eyes implanted with AcrySof IOLs (models SA60AT, SN60AT, MA60AC and MA60BM) and found that eyes with SNGs had increased forward light scatter but the CDVA was unaffected compared to 17 eyes implanted with hydrophobic acrylic iSert 251 or iSert 255 IOLs (Hoya Corp., Shinjuku, Tokyo, Japan) used as controls. The authors excluded subjects with ocular comorbidities. They documented that forward light scatter correlated with reductions in VA and contrast sensitivity, but the values were within the normal age range.
It appears therefore that in most eyes, SNGs while increasing light scatter do so at a level unlikely to be visually symptomatic. However, this is not always the case. In a recent case report, subjective visual impairment due to SNGs occurred in a single-piece AcrySof IOL SA60AT 5 years after IOL implantation with starbursts, flare/glare and cloudy vision. 106 Explantation was not performed, as the other eye was amblyopic. It will be of interest to note if acrylic IOLs manufactured after 2010 will show less propensity to the development of SNGs and if so-called ‘glistenings-free’ hydrophobic acrylic polymers IOL will not have this problem.
Coatings of silicone IOLs
Silicone oil
Late opacification of silicone IOLs due to interaction with silicone oil was reported by Apple et al. 107 in 1996 in three eyes. It generally is not seen by the implanting cataract surgeon but usually later if the patient undergoes vitreoretinal surgery necessitating the use of silicone oil. In two of the three reported eyes the IOLs were explanted, with the silicone oil coating manifest as a thick droplet-like glaze that was tenaciously adherent to the lens surface and could not apparently be dislodged by instruments or injection of viscoelastics. 107 In a further study, Apple et al. 108 performed an in-vitro experimental study to investigate silicone oil adhesion to various IOLs of different biomaterials, including fluorine-treated, heparin-surface-modified, PMMA, acrylic and silicone IOLs. The oil coverage of dry silicone IOLs was 100% and 82.5% in silicone IOLs that were immersed in normal saline. The least coverage was on the heparin-surface-modified lenses (mean score 9.4%). Yaman et al. 109 looked at the effects of heavy silicone oil and found it to be akin to normal silicone oil. The mean heavy silicone oil coverage was 7.05% ± 7.88% on PMMA IOLs, 100% on silicone IOLs, 12.17% ± 11.43% on hydrophobic acrylic IOLs, and 34.64% ± 13.28% on hydrophilic acrylic IOLs. Oner et al. 110 also evaluated the interaction between various IOLs, including: hydrophilic acrylic IOLs (Morcher, type 92s; Morcher GmbH, Germany); hydrophobic acrylic IOLs (AcrySof-SA60AT); PMMA IOLs (Intraocular Optical International-IOI-65130) and silicone optic IOLs (CeeOn Edge 911A). Silicone IOLs once again had the highest percentage (79.9%) coverage, whereas hydrophilic acrylic IOLs had the least (7.8%). They found no effect with varying concentration of the silicone oil. All these studies show that when performing small-incision cataract surgery in patients who may be at risk of requiring vitreoretinal surgery with silicone oil injection, for example, family history of retinal detachment, extreme myopia, congenital cataract and proliferative diabetic retinopathy, hydrophilic acrylic or hydrophobic acrylic lenses should be preferred over silicone lenses and that it is best to avoid, if possible, the use of silicone oil in eyes with pre-existing silicone IOLs.
Toxic anterior segment syndrome due to ophthalmic ointments and IOL materials
Werner et al. 111 reported eight cases of toxic anterior segment syndrome (TASS) related to an oily substance in the anterior chamber of patients following cataract surgery, with an oily coating of the IOL in some cases. All cases were performed by the same surgeon using clear corneal incisions, with implantation of the same type of 3-piece silicone IOL. Immediately postoperatively antibiotic/steroid ointment and pilocarpine gel was administered and the eyes firmly patched. On the first day, some patients presented with corneal oedema, raised intraocular pressure and an oily film-like material within the anterior chamber coating the endothelium, while others had an oily bubble floating in the aqueous, which later coated the IOL. Some of these eyes required additional surgical procedures such as keratoplasty, IOL explantation and trabeculectomy. Six explanted IOLs were analysed by microscopy in four cases by GC–MS, which confirmed the presence of an oily substance coating large areas of the anterior and posterior IOL optic surfaces with a mixed chain hydrocarbon compound seen on GC–MS, akin to that found in the ointment used postoperatively. Chew et al. 112 reported a case in which a patient required lens repositioning 11 and 13 months after initial apparently uncomplicated surgery and then at 18 months developed a greasy film over a 3-piece silicone IOL. The lens was explanted, with GC–MS identifying the presence of hydrocarbons, including docosane, tricosane and tetracosane (often found in ophthalmic ointments), on the IOL surface, which matched that found in one of the ointments used after IOL repositioning. Chen et al. 113 reported a similar case, where ‘Garamycin’ (gentamicin; Schering-Plough, USA) ophthalmic ointment, applied immediately postoperatively, was identified on the surface of an explanted IOL, removed at 3 years due to reduced vision and an oily-like lump on the anterior surface of the IOL.
It appears from these cases that ophthalmic ointments for topical use only can gain access to the anterior chamber and cause damage to other internal ocular structures, coating the surface of silicone IOLs. Such cases highlight the importance of good wound construction and postoperative wound integrity and the risks of tight eye patching following placement of topical ointment. Certainly, there have been several previous reports of ointment applied externally after reaching the anterior chamber, which has occurred both after cataract surgery and other anterior segment procedures,113–116 so care needs to be taken with its immediate postoperative usage with any penetrating ocular surgical wound.
Other types of IOL surface degradation: inter-lenticular opacification
While not a cause of opacification of the IOL itself, inter-lenticular opacification can result in significant visual loss necessitating IOL explantation. Gayton et al. 117 in 2000 presented two pairs of piggyback AcrySof hydrophobic acrylic IOLs, placed in the capsular bag, which were explanted because of opacification between the lens optics. There appeared to be a membrane-like, white material between the lenses, which on histopathological examination identified retained/proliferative lens epithelial cells mixed with lens cortical material. 117 Werner et al. 118 further examined the nature of the inter-lenticular material and documented that Elschnig pearls, which could be surgically aspirated, were observed in the peripheral interface between the lenses but the central interface between the lenses was occupied by an amorphous material, which could not be removed and was acellular on histological examination. In a follow-up paper, Werner et al. 119 reported on the histopathologic and ultrastructural features of three cases of inter-lenticular opacification and found the material opacifying the inter-lenticular space was composed mostly of retained/regenerative cortical material. They concluded that the pathogenesis was akin to that of PCO and that very careful removal of lens epithelial cells and cortical material is necessary in cases where piggyback implantation is being considered. 119 Such findings were confirmed by Eleftheriadis et al. 120 who published two pairs of in-the-capsular-bag piggyback AcrySof IOL implantation with bilateral intra-lenticular opacification in one patient. They documented a central contact zone between the two IOLs, surrounded by a homogeneous paracentral opacity, which in turn was surrounded by Elschnig pearls.
Werner et al. 121 in an in-vivo rabbit study, compared dual-optic silicone IOLs to piggyback in-the-bag IOL implantation with silicone and with hydrophobic acrylic IOLs. They confirmed that intra-lenticular opacification was significantly associated with pairs of hydrophobic acrylic lenses implanted in the bag and not silicone IOLs. Finally, Jackson and Koch 122 documented a case where in an eye with piggyback implantation, while the posterior IOL was placed completely within the capsule, one of the haptics of the anterior IOL was inadvertently placed in the ciliary sulcus and the other in the capsule. They noted that inter-lenticular opacification was localized to the area adjacent to the anterior lens haptic placed within the capsule but absent from the area near the anterior lens haptic in the ciliary sulcus. The concluded that sulcus placement of the anterior IOL may help to prevent inter-lenticular opacification.
While rare, it appears that intra-lenticular opacification is related to paired in-the-capsular-bag hydrophobic acrylic IOLs.117–122 It has been proposed that if such acrylic lenses are being inserted in the fashion, then meticulous removal of the lens epithelial cells and cortical material is mandatory. However, silicone lenses seem less susceptible to this complication and insertion of the anterior IOL into the ciliary sulcus (with an appropriate sulcus lens to avoid iris trauma and pigment dispersion) and not the capsule, together with correct placement of the posterior IOL into the capsular bag with complete coverage of the optic edge by the capsulorhexis, should negate this problem.
Conclusion
Over the past decades several differing degenerations, opacifications and discolourations of IOLs implanted after cataract surgery have been described. Reported anomalies have included photochemical degenerations, water vacuolation, internal and surface calcific deposits, surface coatings and discoloration. Investigations of the pathophysiology of these changes depend on the type of IOL material used and/or manufacturing processes and IOL storage conditions employed and can also be influenced by surgical technique, coexisting ocular pathologies and topical and systemic medications. The clinical significance of these degradations is variable, with some resulting in significant visual disturbance and the need for IOL explantation and others in only minimal optical impairments. Failure to recognize the precise nature of the problem may lead to unnecessary laser capsulotomy procedures. The correct identification and thorough investigation to determine the underlying cause is mandatory both for optimal patient management and the prevention of such problems. Indeed, there is a paucity of published research investigating the effects of material degradations of IOL, especially with time, on their optical properties, which needs to be addressed.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: D.P.S. O. and C.H. have held non-commercial research grants from Alcon Laboratories Inc., Fort Worth, TX, USA and from Rayner Ltd., Worthing, England, UK.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.