
Abstract
Objective:
To evaluate, in the setting of persistent diabetic macular edema, the impact that continuous fluocinolone acetonide delivery has on treatment burden, visual acuity, central retinal thickness, and intraocular pressure.
Materials and methods:
A single-center, retrospective, cohort study of patients with persistent diabetic macular edema, previously treated with anti–vascular endothelial growth factor injections, dexamethasone implants, or focal laser, who were subsequently treated with fluocinolone acetonide was conducted. All retinal visits were analyzed prior to fluocinolone acetonide, until the most recent follow-up visit. Primary outcomes were pre– and post–fluocinolone acetonide changes in the best-corrected visual acuity and number of treatments required for diabetic macular edema. Secondary outcomes included changes in the central retinal thickness and intraocular pressure.
Results:
A total of 19 eyes with persistent diabetic macular edema were included and followed for a mean (SD) of 399.3 (222.9) days. Post–fluocinolone acetonide, the mean best-corrected visual acuity improved by 0.4 ETDRS letters for all eyes (p = 0.895) and the central retinal thickness decreased by 34.2 µm (p = 0.077). After fluocinolone acetonide, the number of treatments decreased from an average of one treatment every 2.7 months to one every 6 months (p = 0.009). Furthermore, post–fluocinolone acetonide, 10/19 eyes (52.6%) did not require additional treatment due to a dry macula, and those who did experienced a non-statistically significant reduction of treatments, from one every 2.6 months pre–fluocinolone acetonide, to one every 2.8 months post–fluocinolone acetonide (p = 0.622).
Conclusions:
In the setting of persistent diabetic macular edema, fluocinolone acetonide significantly reduces the therapeutic burden, while maintaining best-corrected visual acuity and improving the central retinal thickness. In patient-centered discussions, judiciously employing fluocinolone acetonide should be performed to mitigate this therapeutic burden for patients.
Keywords
Introduction
Diabetic macular edema (DME) is the most common cause of visual impairment in patients with diabetes mellitus affecting approximately 75,000 new patients in the United States each year. 1 Moderate visual loss will occur within 3 years in up to 33% of eyes with untreated DME,2–5 significantly affecting quality of life. 6 Currently, available treatments for DME include focal laser photocoagulation, anti–vascular endothelial growth factor (anti-VEGF) injections such as aflibercept 2 mg (Eylea), bevacizumab 1.25 mg (Avastin—used off-label), and ranibizumab 0.3 mg (in the United States; Lucentis) and 0.5 mg (In Canada, Europe, and elsewhere; Lucentis), and intravitreal steroids such as the slow-release dexamethasone 0.7-mg implant (Ozurdex).7–9 While these therapies have proven to be effective in treating DME, frequent injections are needed and up to half of patients still have persistent edema. 10 Anti-VEGF is currently the gold standard of care for treating DME, and the Diabetic Retinopathy Clinical Research Network (DRCR.net) Protocol T showed that after 2 years, 76%, 66%, and 71% of DME patients had a 3-line improvement in best-corrected visual acuity (BCVA) when treated with aflibercept, bevacizumab, and ranibizumab, respectively. Although with this, the treatment groups needed 15, 16, and 15 injections over the 2 years and most eyes (84%) still had persistent DME and required at least one injection during the second year.11–13 Current management of DME with a regimen of frequent intravitreal injections may be disruptive to a patient’s quality of life, for example, in a patient-centered study of 131 individuals with either DME (n = 86) or retinal vein occlusion (RVO, n = 45), the most prevailing desired improvement to the treatment regimen was to have fewer injections to achieve the same visual results. 14 Patients with DME who have additional diabetic-related comorbidities may also require frequent clinic visits with other medical providers (cardiovascular, nephrology, endocrinology, podiatry, and primary care physician), further disrupting the ability to lead a normal life. 15 Furthermore, physical adverse events to injections are more probable as the number of injections received increases in patients with unresponsive DME. 16
Thus, there is an increasing need to reduce the treatment burden of frequent injections for patients with DME, their caregivers, and for the physicians. 17 One can consider the use of longer-acting medications to achieve this goal if the treatment burden is deemed too high for certain patients. The 0.19-mg fluocinolone acetonide (FAc) intravitreal implant (Iluvien) is a Food and Drug Administration (FDA)-approved option which continuously releases 0.2-µg/day of FAc for up to 36 months. This sustained-release approach over this time period, thereby avoids the need for frequent, repeated injections, and the wide swings in intraocular drug concentrations that results from other discontinuous DME therapies such as anti-VEGF injections and dexamethasone treatments. FAc has also been shown to decrease the fluctuation of the central retinal thickness (CRT) between visits and may promote long-term photoreceptor viability. 18 FDA approval was granted to the low-dose (0.2 μg/day) FAc implant in the Fluocinolone Acetonide in Diabetic Macular Edema (FAME) study, where it met the study’s primary endpoint, in which 33% of patients gained 15 letters or more from their baseline BCVA at 3 years as opposed to 21% in the placebo group. 19 Since FAME, various studies have consistently shown that the usage of FAc leads to significant improvement in visual acuity and reduces the CRT.18–28 Although steroid-induced intraocular pressure (IOP) elevation was a concern in FAME, this risk can be mitigated if FAc is used clinically as per the FDA label, which mandates that the implant is only used in patients who have been previously treated with a course of corticosteroids without experiencing a clinically significant rise in their IOP. 28 In Europe and elsewhere, the label differs from the US FDA label.
Furthermore, an economic advantage of incorporating FAc for the management of refractory DME was demonstrated in a study performed in the United Kingdom which revealed that the costs saved when utilizing FAc was £2606.17 per patient over 3 years, compared to other discontinuous therapies.25,29 Finally, the U.S. Retrospective Chart Review in Patients Receiving Iluvien clinical study (USER study) presented data on 160 eyes treated with FAc, where 63% of the eyes required no additional DME treatment, significantly contributing both to improving patient outcomes and quality of life, and reducing the economic impact of frequent treatments. 30
Longer-term therapy is needed to reduce the therapeutic burden without compromising BCVA or CRT in patients with DME. We present a retrospective analysis of outcomes at our institution and compare the frequency of DME treatments before and after switching to FAc. We hypothesize that for persistent DME, improvements in VA and CRT are maintained, demonstrating non-inferiority when switching from discontinuous anti-VEGF and dexamethasone treatments to continuous FAc therapy with the added benefit of reducing the frequency of treatment. In addition, to the knowledge of the authors, this is the first study examining the impact FAc has on extending treatment intervals in patients who still require additional therapy, post-FAc.
Materials and methods
Study design
This is a single-center, retrospective cohort study of all patients with DME who received the 0.2 µg/day FAc intravitreal implant (Iluvien) at a tertiary care academic institution. The University of Chicago Biological Sciences Division Institutional Review Board reviewed and approved this study.
Study population
Electronic medical records were examined for all patients in the study, and each of the clinical encounter between 36 months prior to FAc injection, up until the most recent follow-up (until May, 2018) were analyzed. A query of all patients treated with FAc at our institution was performed. Patients over the age of 18, with a history of DME treated with either focal laser, anti-VEGF, or steroids, followed by treatment with the FAc implant, with at least one post-FAc encounter were included. Criteria for selection for FAc included patients with persistent DME, who have had an insufficient treatment response in the setting of prior treatments. Furthermore, FAc must have been used per FDA label (all patients must have been previously treated with a course of corticosteroids without a clinically significant rise in intraocular pressure). Finally, patient-centered discussions regarding further therapeutic options were presented. Exclusion criteria included patients under the age of 18 and those with macular ischemia (n = 1), patients with glaucoma, or any suspected ocular/periocular infection. In total, 19 eyes met these inclusion criteria.
All patients with DME were treated in a treat-and-extend algorithm prior to, and following, administration of the FAc implant. 31 Post-FAc, patients with a suboptimal response with persistent edema on optical coherence tomography (OCT) required a multifactorial approach with combinational therapy to also address edema mediated by high levels of VEGF. If necessitated, the choice of therapy was at the discretion of one sole treating retina specialist (S.M.H.) and made on a case-by-case basis.
Data analysis
Data gathered included (1) patient demographics, (2) BCVA in Early Treatment Diabetic Retinopathy Study (ETDRS) letters, (3) IOP, (4) CRT on Cirrus OCT (Carl Zeiss Meditec, Dublin, CA), and (5) any treatments received during each visit. Treatments for DME included either an anti-VEGF injection, intravitreal dexamethasone implant, or focal laser.
Patient clinic visits were described as a “baseline” visit (designated as the date of FAc administration) and every 3 months before and after baseline using ±45-day visit windows. Clinical encounters were reviewed from 36 months prior to receiving FAc up until the most recent follow-up time period. The primary endpoint was the change in BCVA and the treatment burden, calculated as the time period each patient was followed pre- and post-FAc divided by the number of treatments received for DME during these periods. Other secondary outcomes assessed were the pre- and post-FAc changes in CRT and IOP.
Statistical analysis
Microsoft Excel was used to organize clinical data. Statistical analyses were performed using a paired t-test, with a type 1 error rate of p < 0.05 were accepted as statistically significant using SAS software (version 9.3; SAS Institute Inc., Cary, NC, USA). Snellen VA was converted into the ETDRS letter scores as described by Gregori et al. to facilitate statistical calculation. 32
Results
Nineteen eyes from 15 patients who received the 0.2 µg/day FAc intravitreal implant were included in the study. Four patients received bilateral FAc treatment. The mean (SD) time of follow-up after FAc injection was 399.3 (222.9) days (Table 1).
Baseline characteristics.
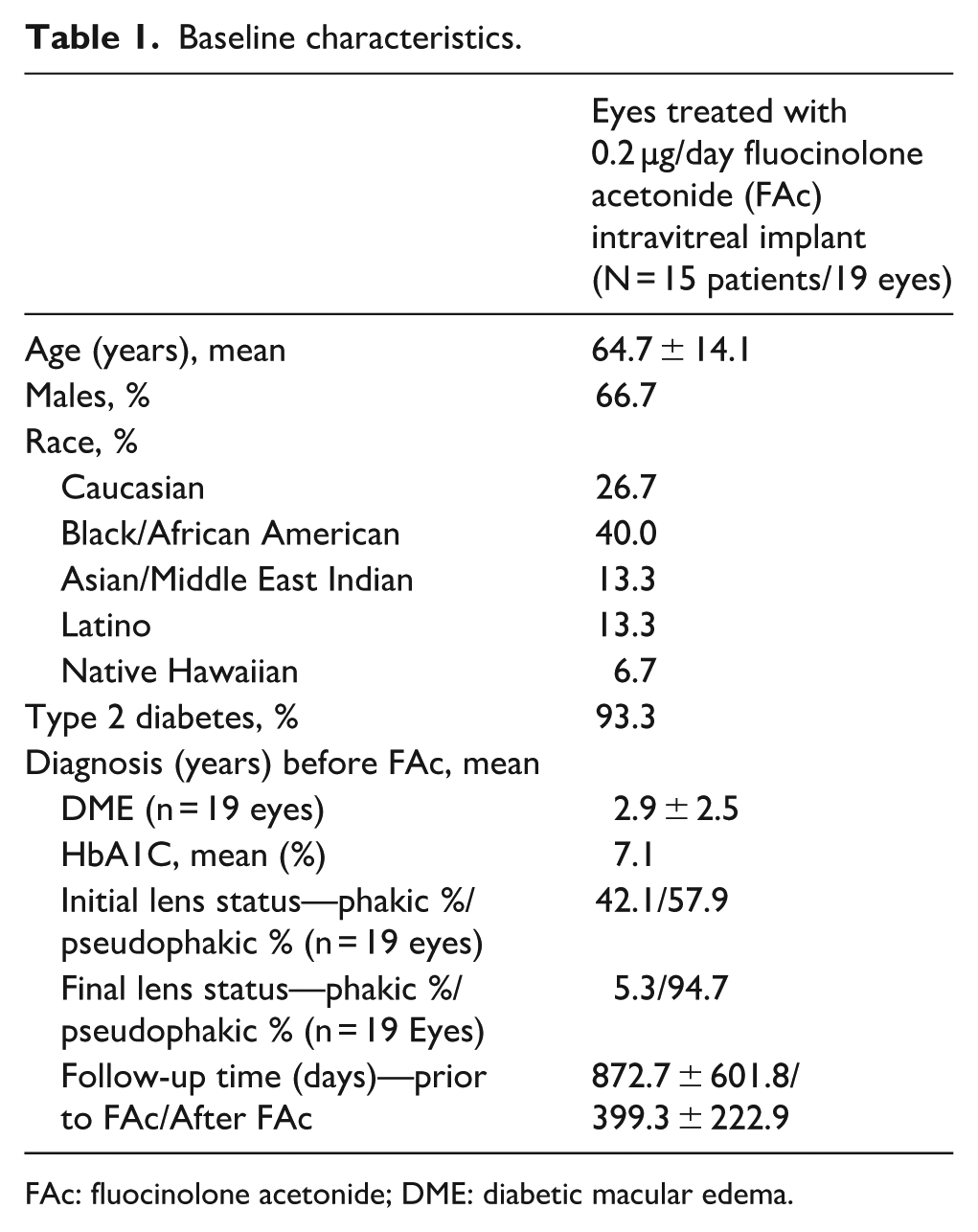
FAc: fluocinolone acetonide; DME: diabetic macular edema.
BCVA was maintained at the latest follow-up visit while on continuous FAc therapy; improving from an average of 64.0 (14.76) ETDRS letters at the time of FAc administration to 64.4 (19.59) ETDRS letters (p = 0.895) (Figure 1).
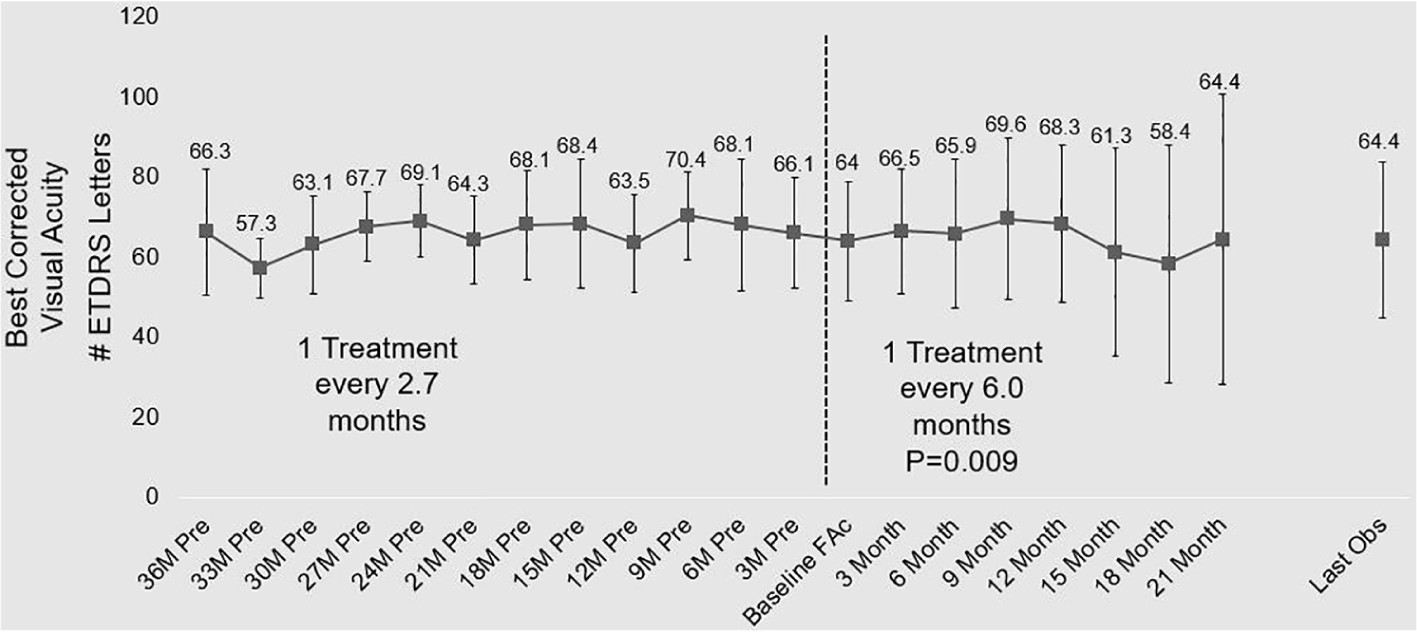
Visual acuity outcomes—all eyes.
Upon receiving FAc, 10/19 eyes did not require further treatment over the mean follow-up time period of 399.3 days. Prior to FAc, all eyes received an average of one treatment every 2.7 ± 5.9 months, whereas after FAc, the treatment burden reduced to an average of one treatment every 6 ± 5.3 months (p = 0.009). The number of retina visits, pre- (5 ± 2.13 visits) and post- (4.32 ± 1.40) (p = 0.203) FAc remained similar. For the nine eyes which still required additional treatments post-FAc, there was a non-statistically significant reduction in the treatment burden from an average of one treatment every 2.6 ± 7.5 months pre-FAc, to one treatment every 2.8 ± 5.7 months post-FAc (p = 0.622).
A non-statistically significant reduction in the mean CRT occurred from 328 ± 58.16 µm prior to FAc to 293.8 ± 59.63 µm at the latest follow-up visit after FAc treatment (p = 0.077) (Figure 2). Furthermore, 12 months prior to FAc treatment, 37.5% (n = 8) of eyes had a CRT of less than 300 µm, and at time of FAc injection, 42.1% 9 (n = 19) of eyes had a CRT less than 300 µm. At 12 months post-FAc, 55.6% (n = 9) of eyes had a CRT less than 300 µm (Figure 3).
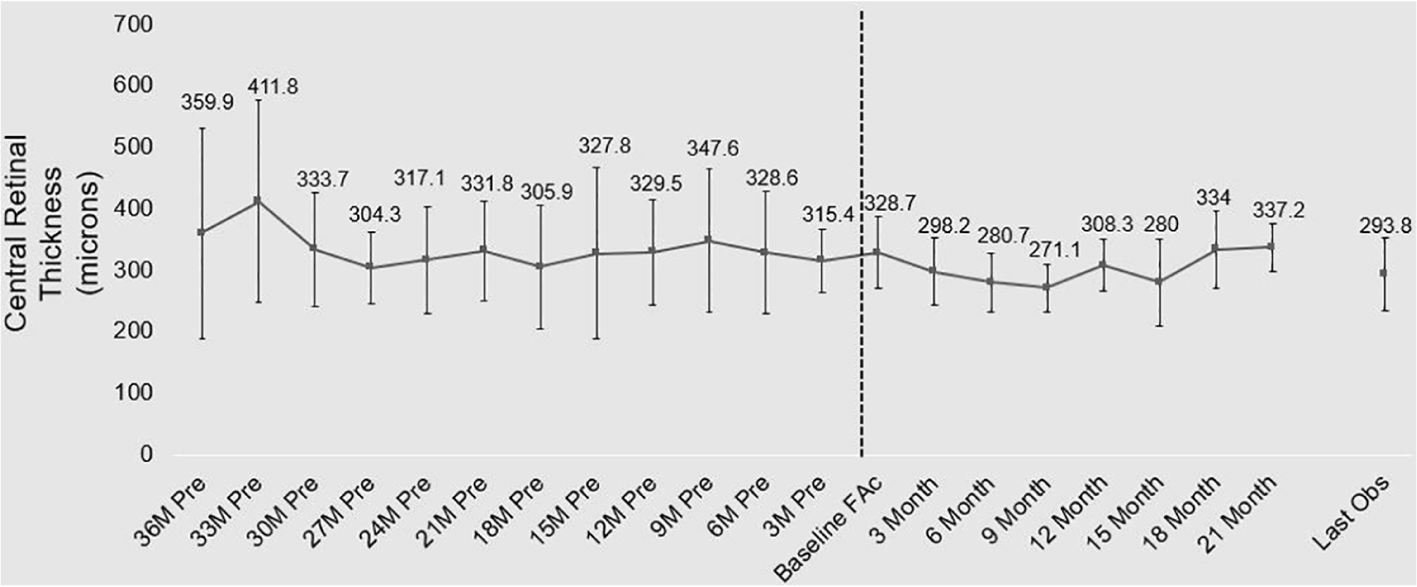
Central retinal thickness—all eyes.
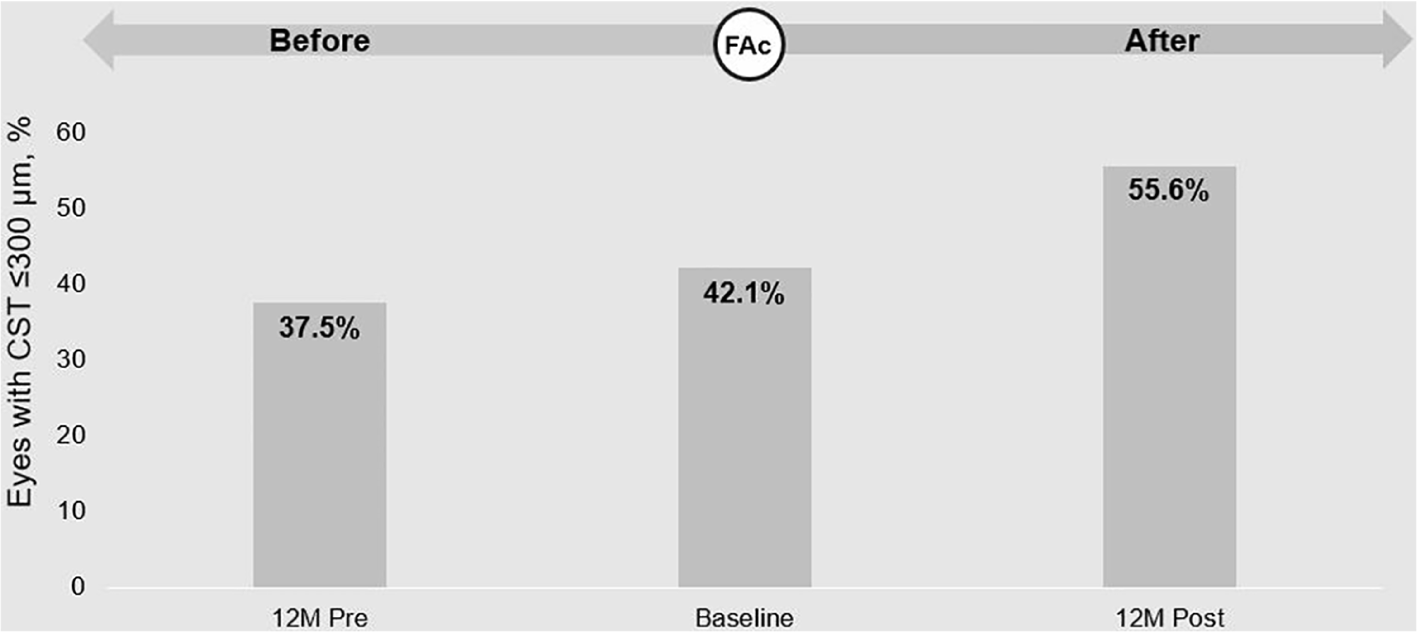
Percentage of eyes with CRT of less than 300 µm.
A non-significant IOP rise was noted from a mean of 15.9 ± 4.29 to 18.6 ± 5.22 mmHg following FAc for all eyes (p = 0.104). Ten of 19 eyes (52.6%) had a decrease or no change in IOP from baseline at latest follow-up. Conversely, 9 of 19 eyes (47.4%) had an increase in IOP, but only two eyes had an IOP increase of more than 7 mmHg. Six of 19 eyes (31.6%) needed IOP-lowering drops following FAc, with one eye (5.3%) needing additional procedures including laser trabeculoplasty and cyclophotocoagulation. No eye in this study required incisional surgery to manage IOP changes (Table 2).
Visual acuity, central retinal thickness and IOP changes before and after FAc.
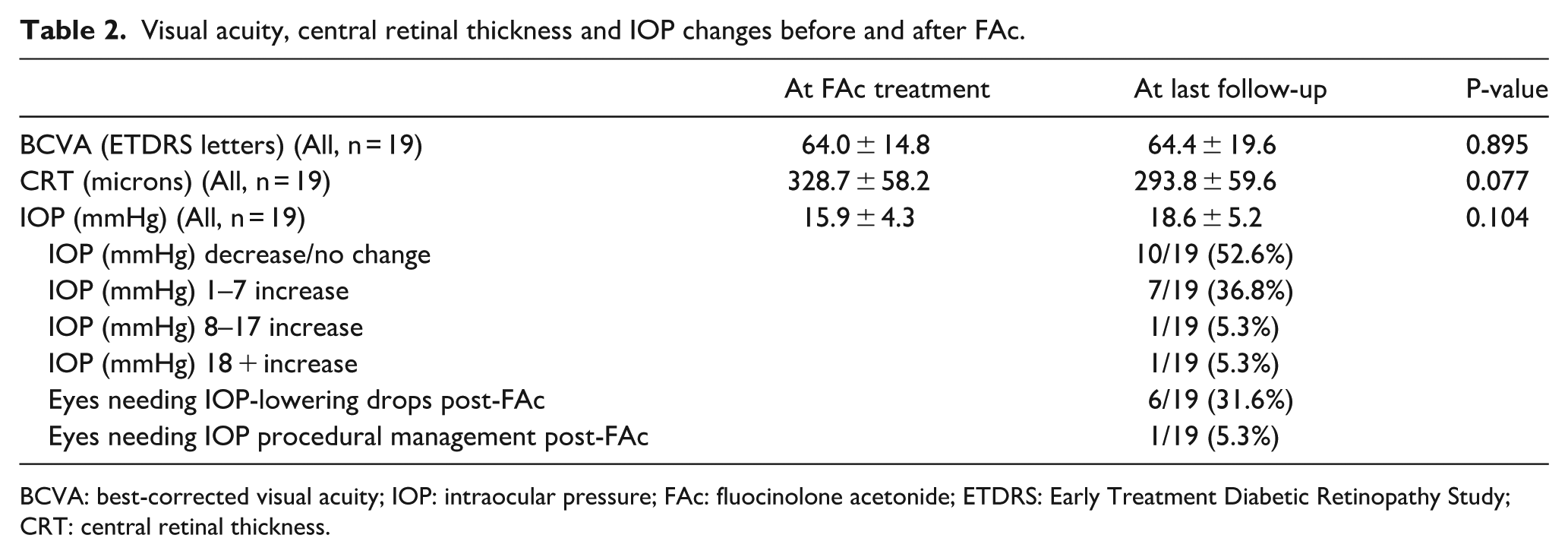
BCVA: best-corrected visual acuity; IOP: intraocular pressure; FAc: fluocinolone acetonide; ETDRS: Early Treatment Diabetic Retinopathy Study; CRT: central retinal thickness.
Before FAc, 17/19 of the eyes received anti-VEGF therapy, with aflibercept being the most commonly used in 15/19 eyes, 44 times. Eighteen of 19 eyes received dexamethasone implants before FAc totaling 37 treatments (the 19th eye received topical steroids with no IOP rise prior to receiving FAc injection). Furthermore, 10/19 eyes received focal/grid laser, for a total of 26 treatments. Following FAc, 10/19 eyes (52.6%) did not need further DME treatments at latest follow-up. Of the 9/19 eyes that required further treatment, all eyes received aflibercept for a total of 52 injections, dexamethasone was used once, and focal/grid laser was performed once as well (Table 3).
Treatments for diabetic macular edema for all eyes.
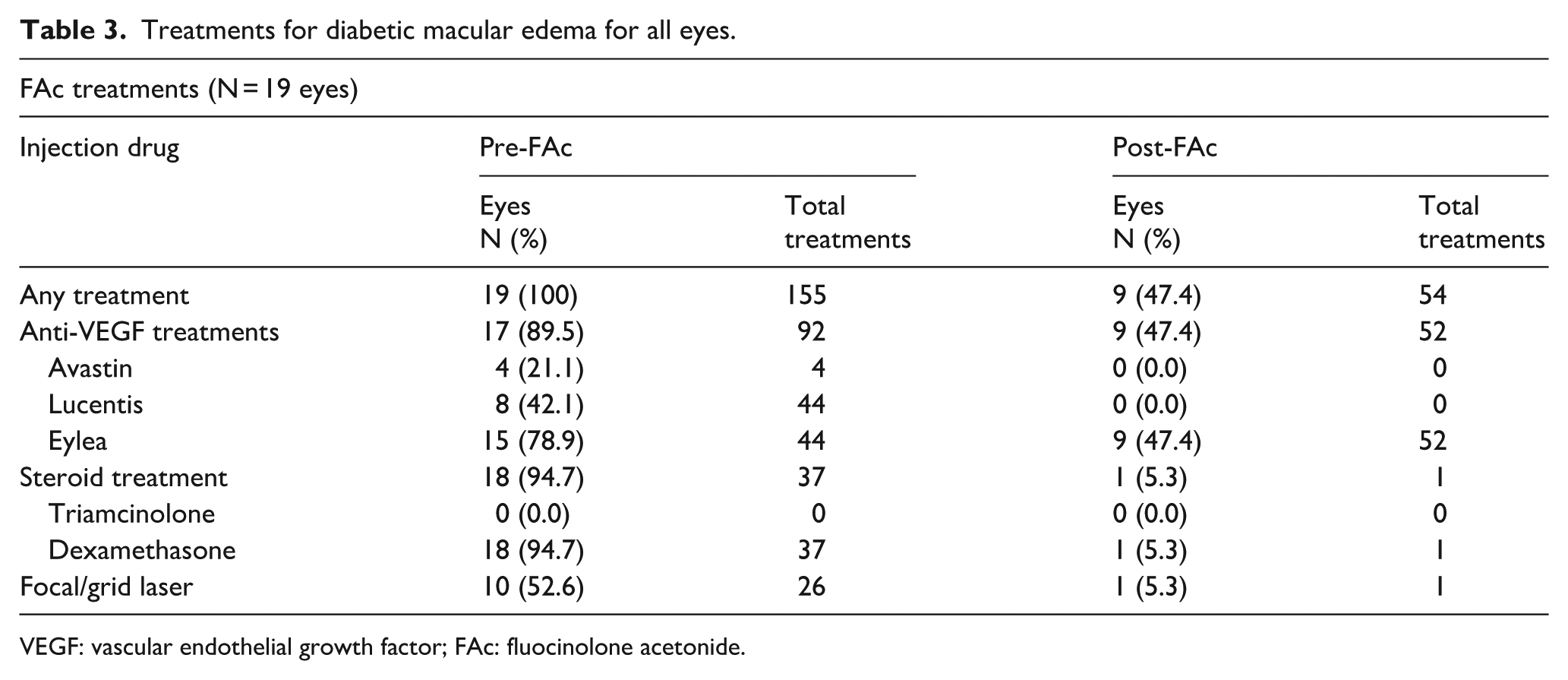
VEGF: vascular endothelial growth factor; FAc: fluocinolone acetonide.
Discussion
For many individuals afflicted with DME, the current treatment paradigm involves receiving frequent treatments in the form of intravitreal anti-VEGF and/or steroid injections and lasers in an attempt to treat and prevent visual loss. These procedures are not without risks, but for patients and treating physicians, the high treatment burden is problematic when managing persistent DME. For patients who are insufficiently responsive, the 0.2 µg/day FAc intravitreal implant is a promising addition to the armamentarium of managing DME. In the FAME study, in patients with persistent DME, up to 33% of patients receiving a low-dose 0.2 µg/day FAc intravitreal implant were able to gain ⩾15 ETDRS letters at 36 months following FAc, 19 and numerous studies demonstrated the longevity of this therapeutic option, where stabilization, and even improvement of patient’s BCVA and CRT have been shown.18–28,33 Our study examines all of this, but in addition, we explore the real-world implication of incorporating FAc on injection frequency, and furthermore assess the result for patients who continue to require treatments post-FAc.
In our study, 19 eyes of 15 patients were included with a follow-up duration of 399.3 days. Ten out of 19 eyes (52.6%) did not require further treatment following the FAc implant at latest follow-up, a slightly lower finding than the 63% reported in the USER study, 30 and the 64.3% reported in another similar study. 27 Furthermore, the percentage of FAME study patients that received 1, 2, or ⩾3 post-FAc treatments by month 36 in the low-dose treatment group was 76.1%, 18.7%, and 5.3%, respectively. 19 Although our results differ significantly from FAME, it represents a real-world example of how this therapy is utilized, where patients already received a gambit of therapies for DME and continued to suffer from persistent edema, where as in FAME, an inclusion criterion required that patients were treatment-naïve.
In the treatment of DME, extended duration treatment strategies are attractive in their ability to reduce the treatment burden for patients. 34 A striking finding in this series was a statistically significant reduction in treatment frequency where one treatment was needed on average every 2.7 months prior to FAc injection, whereas one treatment was needed only every 6 months post-FAc injection. In a multi-centered study performed in the United Kingdom of 345 eyes with DME, FAc treatment decreased the need of anti-VEGF, and/or laser treatments in 176 (51.3%) eyes in the 12 months post-FAc, whereas in the 12 months preceding FAc, 296 (85.7%) of eyes required treatment. 28 However, this study did not describe the impact FAc had on extending the time interval between treatments. In our study, not only did we depict a significant reduction in the overall treatment burden after FAc for all eyes, we examined the eyes (9/19) which still continued to require treatment post-FAc, and demonstrate a non-significant reduction in the therapeutic need from one treatment every 2.6 months to every 2.8 months. To our knowledge, this has not been demonstrated in previous literature.
In addition to the reduced burden on patients and physicians after FAc treatment, a reduction in health care costs has been described as well.25,29,35 For example, Holden et al. showed that following FAc administration, the lower need of anti-VEGF therapies led to the fewer outpatient appointments with an overall reduction in the health care resource costs associated with treating DME by a mean of £1452. 35 Our study furthermore adds to the growing body of literature supporting the savings incurred with FAc therapy. Our findings show that when switching DME therapy from frequent discontinuous treatments to continuous basal treatment with FAc, BCVA, and CRT are improved and/or maintained while the need for further treatments significantly decreases and can often be extended by several months. As mentioned, data from Sivaprasad and Oyetunde 14 reveal that patients who receive frequent intravitreal injection’s preference is to have a treatment regimen where fewer injections are needed to achieve the same visual results. Extrapolating our results highlights the utility of FAc in a patient-centered discussion regarding therapeutic options to decrease their treatment burden. For patients who have continued to have persistent edema, despite multiple anti-VEGF injections, experts have recommended switching to FAc after a course of 0.7 mg dexamethasone, in order to prevent the possibility of retina damage due to the cyclic nature of DME resolution and recurrence. 10
It should be noted that all patients with DME in our study were treated using a treat-and-extend protocol before and after FAc administration. 31 Furthermore, the number of visits did not significantly change or decrease following FAc treatment, and patients were followed just as closely prior to and after FAc treatment. While the pre-FAc treatments occurring an average of every 2.7 months may appear as undertreatment when compared to other clinical trials, this was a retrospective analysis and a “real-world” observation, where patients often miss scheduled appointments, thus highlighting the true nature a retina practice might have.
Elevated IOP following FAc is a well-known potential side effect19,21,22,24,29,34 and in the USER study, an elevation of ⩾10 mmHg was seen in 34% of patients. 30 In our cohort, 9/19 eyes (47.4%) had an overall IOP elevation with only two eyes having greater than a 7 mmHg increase. These two eyes were of the same patient where the right eye increased from 10 to 31 mmHg and the left eye increased from 11 to 26 mmHg following FAc injections. Neither eye had a steroid response beforehand following intravitreal dexamethasone, and both eyes had good IOP control with the use of IOP-lowering drops. Six eyes (31.6% of total eyes) had IOP control via topical medications, and only one eye needed a non-incisional procedure to control IOP. This eye had an acute IOP increase of 20–40 mmHg following FAc injection, and the IOP normalized after laser trabeculoplasty followed by cyclophotocoagulation. No eyes needed incisional glaucoma surgery.
Eyes with DME previously treated with anti-VEGF were included in this study, as opposed to the FAME study where eyes previously treated with anti-VEGF were excluded. Furthermore, in FAME, baseline BCVA was 52.9–54.7 ETDRS letters overall, with a retinal thickness of 461 µm in the low-dose group. Conversely, patients in our study had a better baseline BCVA of 64.0 ETDRS letters and lower baseline CRT (328.7 µm). Furthermore, in the FAME study, for the low-dose group, BCVA improved by 4.4 ETDRS letters at 2 years, while the retinal thickness reduced by 168 µm. This trend was comparable to our study, where over a mean follow-up period of 399 days, we saw an improved BCVA of 0.4 ETDRS letters and reduction of the CRT by 35 µm. Importantly, patients in our study differed by having better baseline BCVA and CRT, this may be indicative that continuous FAc therapy plays a role in the management of persistent DME across a wide spectrum of disease severity and can be important at various time period in a patient’s treatment history.
A limitation of this study is its retrospective nature without randomization. Furthermore, there were a relatively small number of eyes evaluated in the study, although currently, FAc is rarely used in clinical practices. In addition, we presented OCT findings in terms of CRT and did not analyze further in terms of intra-retinal fluid, cystic changes, or RPE/photoreceptor layer integrity all of which can affect visual outcomes as well. Nevertheless, this is a unique real-world evaluation of FAc treatment for DME in that all DME treatments (anti-VEGF, steroids, and focal laser) were compared pre- and post-FAc.
Conclusion
In patients with persistent DME who underwent various discontinuous treatments for DME, adding continuous therapy with FAc eliminated the need for additional DME treatments for 10/19 (52.6%) eyes, while maintaining improvements in BCVA and reduction in the CRT. Furthermore, there was a significant reduction in the number of treatments required per month when compared to the pre-FAc time period, and patients who still required additional therapy also experienced a reduction in the treatment frequency. Judiciously employing FAc in the treatment of persistent DME can improve the treatment burden inflicted on patients, caregivers, and treating physicians, and should be employed in patient-centered discussions of therapeutic options to mitigate this therapeutic burden.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: S.M.H. is a consultant or on the speaker’s bureau for Alcon, Allergan, Novartis, OD-OS, Clearside Biomedical, EyePoint Pharmaceuticals, Alimera Sciences, Spark, and Regeneron. O.E.A. and S.A.S. report no financial disclosures.
Ethical approval
The University of Chicago Institutional Review Board approved this study: IRB18-0165.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.