
Abstract
Purpose:
To describe the clinical course of a case of bilateral Salzmann nodular degeneration (SND) treated with superficial keratectomy (SK) followed by intense pulsed light (IPL) for the treatment of coexisting meibomian gland dysfunction (MGD).
Case description:
A 54-year-old man who presented to us complaining of progressive blurred vision associated with foreign body sensation in both eyes because of SND and coexisting MGD. In view of symptoms and visual acuity (VA) deterioration, bilateral SK was performed. Two months after SK, IPL treatment to the face and meibomian gland expression (MGX) using the E-eye device (E-SWIN, Paris) on days 0, 15, and 45, were performed in both eyes with the aim to avoid recurrence and/or progression of MGD. One year after SK, the patient was asymptomatic and VA was 20/20 in both eyes; however because of worsening of non-invasive tear film break-up time measured on Sirius® Scheimpflug tomograph, IPL and MGX were promptly repeated and scheduled every 6 months.
Conclusion:
In our case, IPL was a safe and effective option to control MGD in a patient with SND requiring SK with no observed recurrence of SND 2 years after surgery.
Keywords
Introduction
Salzmann nodular degeneration (SND) is a slowly progressive condition resulting in raised corneal nodules causing ocular surface irritation, dryness, and possible decreased vision. SND was first described in 1925 as single or multiple bluish or whitish gray corneal opacities in one or both eyes. 1 Histopathologic correlates demonstrated sub-epithelial nodules anterior to Bowman’s layer, thinning of the corneal epithelium overlying the nodule, and variable duplication of the epithelial basement membrane with disruption of Bowman’s layer. 2 The etiology of SND is multifactorial and local inflammation induced by the corneal epithelium is believed to play an important role in the pathophysiology of the disease. 2
While SND has been mainly associated with meibomian gland dysfunction (MGD), several other ocular conditions including chronic blepharitis and keratitis can cause SND.
The common factor among all of the conditions associated with SND is poor epithelial protection, due to chronic irritation or mechanical disruption of the epithelial-stromal barrier during trauma or surgery. 2
The choice of treatment in SND is influenced by the presenting symptoms and the severity of disease. 3 Since SND does not usually affect the vision, conservative management is usually advised. Topical cyclosporine, topical corticosteroids and/or oral doxycycline may be indicated in cases of severe inflammation. 2
Raised nodules, involvement of central visual axis causing reduced vision, or failure of conservative management are common indications for surgical intervention. 2 Surgical options include superficial keratectomy (SK), excimer laser phototherapeutic keratectomy, and lamellar keratoplasty depending on the degree and irregularity of the corneal opacity. 2
Unfortunately recurrence of SND after surgery is not uncommon. Rate of recurrence is unpredictable and may range from none to 100%. 3 To avoid the recurrence it is paramount to reduce as much as possible the effects of the underlying associated conditions such as MGD.
Over the last years, intense pulsed light (IPL) treatment to the face has been shown to consistently improve MGD.4,5 In this report, we describe the clinical course of a case of SND treated with SK followed by IPL for the treatment of coexisting MGD.
Case report
A 54-year-old man with no significant past medical history presented to us complaining of progressive blurred vision associated with foreign body sensation in both eyes. He reported preservative-free lubricant eye drops use for many years and no known allergies. Manifest refraction was +6.75sph –6.25 cyl@55 in the right eye (RE) and +10.00sph –8.25cyl@100 in the left eye (LE) and his corrected distance visual acuity (CDVA) was 20/25 in both eyes (Table 1). On examination a single large whitish gray nodule in the superonasal quadrant of RE and about 4 to 5 small nodules in the superior quadrants of LE were found (Figure 1(a) and (b)). Red lid margin, terminal duct obstruction of the meibomian glands and qualitative/quantitative changes in meibum were suggestive of MGD. Type 2 Schirmer’s test revealed wetting of the paper strips measured 12 mm. A non-invasive tear film break-up time (NI-BUT) was collected using the advanced analysis of the tear film provided by the Sirius® Scheimpflug tomograph (CSO). The NI-BUT value, which represents the average time to break-up of the tear film, measured 9.1 s in RE (first rupture after 5.7 s) and 6.6 s in LE (first rupture after 2.8 s). Central corneal thickness (CCT), maximum corneal thickness (MCT), simulated keratometry (Sim-Ks) and root-mean square (RMS) of higher-order aberrations (HO) values are listed in Table 1. Intraocular pressure, lens transparency and fundus examination were unremarkable.
Tomographic data of the cornea at presentation and 2 years after surgery.
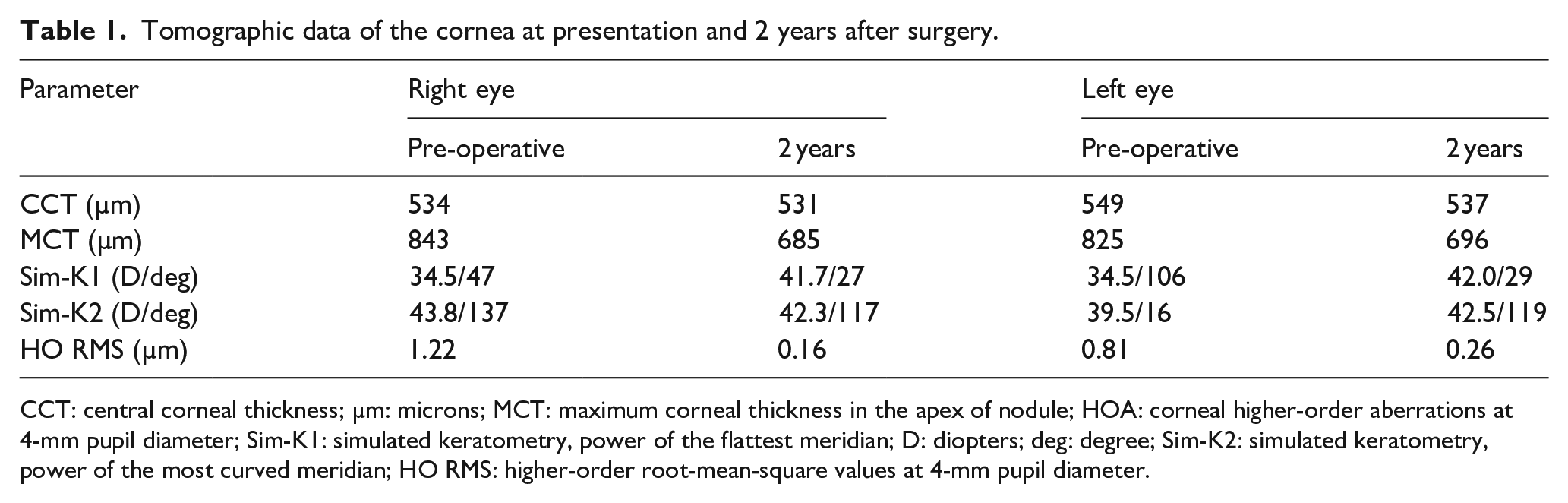
CCT: central corneal thickness; µm: microns; MCT: maximum corneal thickness in the apex of nodule; HOA: corneal higher-order aberrations at 4-mm pupil diameter; Sim-K1: simulated keratometry, power of the flattest meridian; D: diopters; deg: degree; Sim-K2: simulated keratometry, power of the most curved meridian; HO RMS: higher-order root-mean-square values at 4-mm pupil diameter.
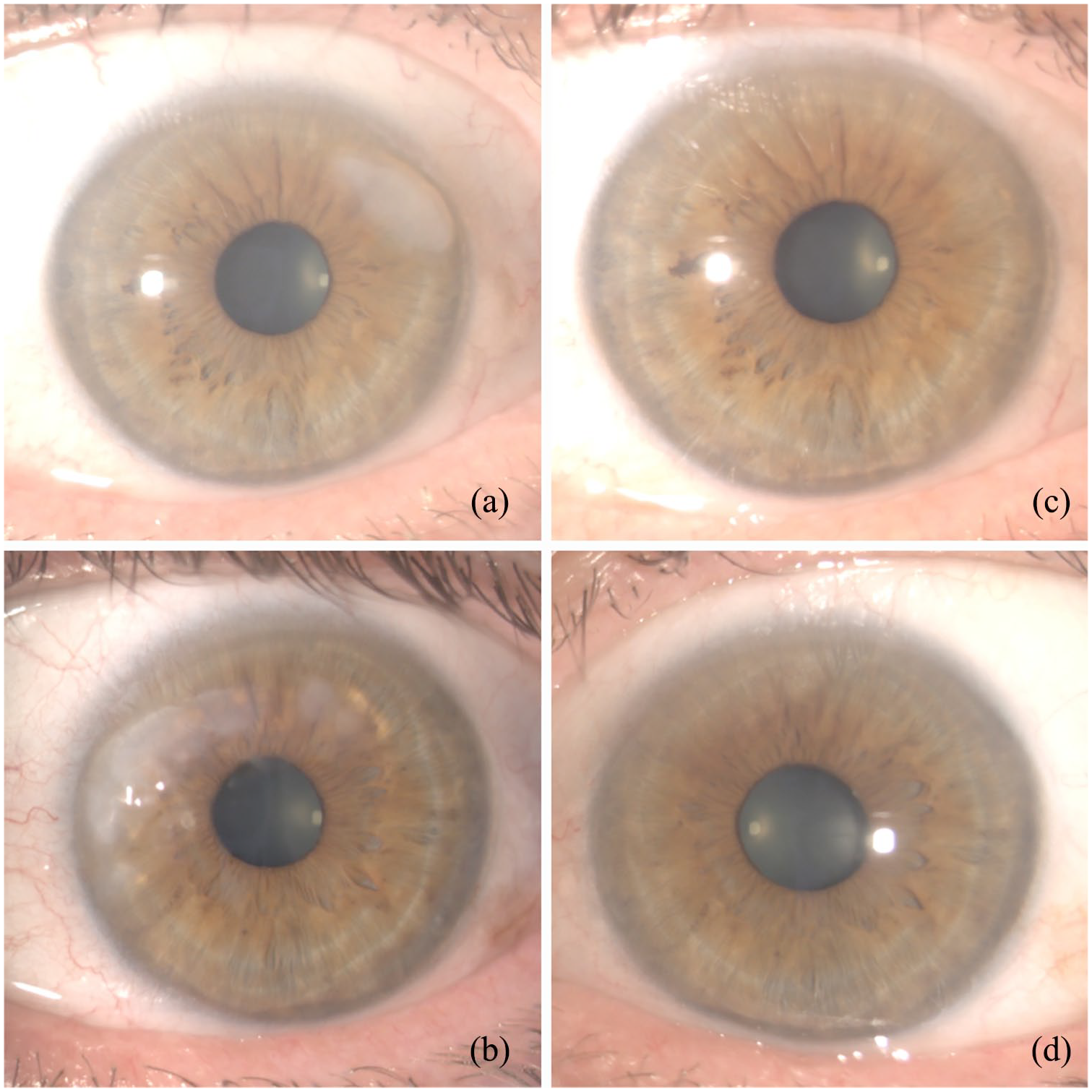
Slit-lamp examination at presentation showing Salzmann’s nodular degeneration in the right eye (a) and left eye (b). Slit-lamp examination two years after superficial keratectomy of the right eye (c) and left eye (d).
In view of the VA deterioration and presence of symptoms, SK with alcohol delamination was planned. Patient was explained that laser vision correction would have not been optimal given his high hyperopic refraction.
An uncomplicated procedure was performed in both eyes, as previously described. 6 Post-operative treat-ment included preservative-free levofloxacin and fluorometholone acetate eye drops.
One month after SK, patient reported subjective improvement and CDVA improved to 20/20 in both eyes. Manifest refraction was +1.75 –1.00 × 45 in the RE and +2.50 –1.00 × 120 in the LE. Slit-lamp biomicroscopy showed clear corneas with a moderate fluorescein staining consistent with superficial punctate keratitis but at lid margin persisted redness despite fluorometholone once a day. For these reasons and in attempt to avoid recurrence of SND and steroid-related long-term complications, fluorometholone was stopped, and an IPL treatment of the lower eyelids was planned for the management of MGD and its related ocular surface disease.
Two months after SK, a combination of IPL and meibomian gland expression (MGX) using the E-eye device (E-SWIN, Paris, France) were performed on days 0, 15, and 45, as previously described. 7
One year after SK, patient did not report any symptoms. CDVA was 20/20 in both eyes. Manifest refraction was +2.00 –1.25 × 60 in the RE and +2.50 –0.75 × 120 in the LE. Slit-lamp biomicroscopy showed clear corneas and no fluorescein staining. However, NI-BUT showed no improvement in time to rupture, values were 7.9 s in RE (first rupture after 7.9 s) and 6.9 s in LE (first rupture after 3.6 s). For this reason, a second single session of IPL and MGX was promptly repeated. The patient was then advised to continue preservative-free lubricant eye drops as long-term treatment and an IPL treatment was performed every 6 months thereafter.
Two years after SK, the patient was asymptomatic and CDVA was 20/20 in both eyes with unchanged manifest refraction. Slit-lamp biomicroscopy showed clear corneas and no fluorescein staining (Figure 1(c) and (d)). NI-BUT improved measuring 10.6 s in RE (first rupture after 5.5 s) and 11.6 s in LE (first rupture after 5.2 s). Central corneal thickness, maximum corneal thickness in the apex of nodule, simulated keratometry, and corneal higher-order aberrations at 4-mm pupil diameter values are listed in Table 1. The patient was advised to continue preservative-free lubricant eye drops as long-term therapy and IPL treatment was given every 6 months up to 2 years after surgery. No signs of postsurgical recurrences and/or progression of the disease were noted during follow-up.
Discussion
We present a case of a patient with high refractive error secondary to SND successfully treated with SK followed by IPL for coexisting MGD. Many options for the treatment of MGD-related dry eye are available, including topical corticosteroids, immunomodulatory agents (cyclosporine ophthalmic emulsion/solution), and the recently available lymphocyte function-associated antigen (LFA-1) antagonist lifitegrast ophthalmic solution.7,8 However long-term potential side effects and compliance of patients represent the main limitations of these treatments. Use of IPL was aimed at avoiding recurrence and/or progression of MGD and sparing of long-term topical and/or systemic anti-inflammatory drugs.
To the best of our knowledge, this is the first report on such approach. Indeed IPL has been shown to be a safe and effective procedure in terms of tear breakup time, corneal staining and eyelid margin measurements, meibum quality, meibomian gland expressability and ocular surface disease index in all stages of MGD, irrespective of patient’s compliance. 7 Several properties of IPL supports its use to address MGD. Specifically, hemoglobin absorbs the heat administered in IPL, thereby reducing telangiectatic blood vessels which represent an hallmark of MGD. 9 Theoretically, restoration of a more physiological environment on the skin may help reducing the cutaneous inflammation causing characteristic ocular surface changes. Additionally, IPL may eradicate Demodex microbe infestation, commonly associated with MGD, through coagulation, and, as such, may provide therapeutic suppression of the disease. 10 IPL treatment also upregulates anti-inflammatory cytokines, downregulates proinflammatory molecules, and suppresses matrix metalloproteinases, thereby inducing a more favorable cutaneous molecular milieu. 11 At present it is unclear how many sessions and the interval between the sessions of IPL treatments are needed to stabilize MGD. We contend that at least 3 sessions are needed as a loading dose but annual IPL treatment as booster dose may not be sufficient to control disease, especially for patients with MGD-correlated corneal degenerations. As a matter of fact, in our report one year after the procedures, the patient, in spite of the absence of symptoms, experienced a worsening of the NI-BUT. For this reason, a single session of IPL and MGX was promptly repeated and the patient was scheduled on IPL treatment every 6 months achieving good stabilization of the NI-BUT. The observation from our report that the absence of symptoms does not necessarily correlate with the control of the MGD-related dry eye, supports periodical testing with NI-BUT examination and a tear film osmolarity in the management of these patients. We also contend that the frequency of IPL treatments may be adjusted on the results of the aforementioned tests in order to avoid the worsening of the ocular surface.
In conclusion, we report promising results on the use of IPL treatment following SK for SND. In our case we did not observe recurrence of SND 2 years after surgery. However because of the slowly progressive nature of SND, recurrence may still be expected.
A randomized clinical trial comparing IPL with topical immunosuppressive treatment (i.e. steroid or cyclosporine) would be required to evaluate the best treatment strategy in these patients. Further study with longer follow-up including a large cohort of patients is warranted to confirm our preliminary report.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the participants of this case report and any accompanying images.