
Abstract
Purpose
To describe a technique for Salzmann Nodule removal assisted by Microscope-Integrated Intraoperative Optical Coherence Tomography (iOCT).
Methods
The study describes a novel approach utilizing iOCT for enhanced visualization and accurate dissection of difficult-to-see nodules, while clarifying their relation to anterior stromal haze.
Results
This method leverages iOCT for effective nodule identification and removal, ensuring minimal disruption to surrounding tissue. It provides real-time feedback on dissection depth, facilitating precise excision without extensive keratectomy, and is particularly beneficial for surgeons with limited experience or in cases of reduced visibility.
Conclusions
Utilizing iOCT during superficial keratectomy for Salzmann Nodular Degeneration allows for precise detection and removal of degenerated nodules. iOCT- guided keratectomy allows the corneal surgeon to preserve surrounding healthy corneal tissue and improves surgical results in Salzmann Nodular Degeneration.
Introduction
Salzmann nodular degeneration (SND) is a progressive degenerative disorder characterized by nodular corneal opacities. Initially identified as a dystrophy in 1925, SND has been reclassified as a degenerative condition. It occurs in both primary and secondary forms and predominantly affects older women. 1
SND cases can be associated with infectious diseases such as measles, scarlet fever, and trachoma, along with inflammatory conditions such as various types of keratitis and meibomian gland dysfunction.1,2 Previous corneal surgery has also been identified as a risk factor.3,4 Non-inflammatory predisposing conditions, including the use of rigid contact lenses and epithelial basement membrane dystrophy, are comparatively rarer. 5
Typically, Salzmann's nodules appear paracentrally or peripherally on the cornea, but central involvement can be present, often leading to significant visual disturbances like distortion and glare due to high-order corneal aberrations. Furthermore, SND may coexist with and contribute to irregularities, foreign body sensation, and subtarsal conjunctival inflammation, all of which can degrade visual quality.
Medical treatment mainly consists of lubrication and eyelid hygiene, with a small proportion of patients requiring surgical intervention for severe symptoms or vision impairment. Preferred surgical techniques in the management of SND include alcohol delamination, 6 superficial keratectomy (SK), 7 phototherapeutic keratectomy (PTK), or a combination thereof.1,8 SK is generally the technique of choice in primary SND removal, especially in cases with a preserved Bowman layer. Nonetheless, distinguishing between small nodules for selective excision and diffuse corneal scarring during SK in SND poses a challenge. Insufficient identification can lead to either incomplete removal of affected tissue or overly aggressive resection, risking damage to the deeper corneal stroma.
In this context, we present an innovative surgical strategy for SND treatment that incorporates Microscope-Integrated Intraoperative Optical Coherence Tomography (iOCT) to improve nodule detection and selective excision, aiming to preserve surrounding corneal tissue. By integrating this advanced imaging technique into the surgical process, we seek to improve the safety, effectiveness, and accuracy of SND treatment.
Methods
The use of iOCT to aid the superficial keratectomy of affected areas in two cases of SND is described in this case report.
After the instillation of topical anesthetic drops and Povidone Iodine 5% drops, the surgical procedure begins with the placement of a sterile drape, followed by careful drying of the ocular surface using surgical spears to enhance visibility. Subsequently, an iOCT scan (EnFocus intraoperative OCT, Proveo 8, Leica Microsystems, Heerbrugg, CH) targets the anterior stromal layer of the cornea. This scan, offering a 360-degree view, enables a thorough analysis of the anterior corneal stroma, facilitating the accurate identification of nodular formations (Figure 1A) (Video 1).
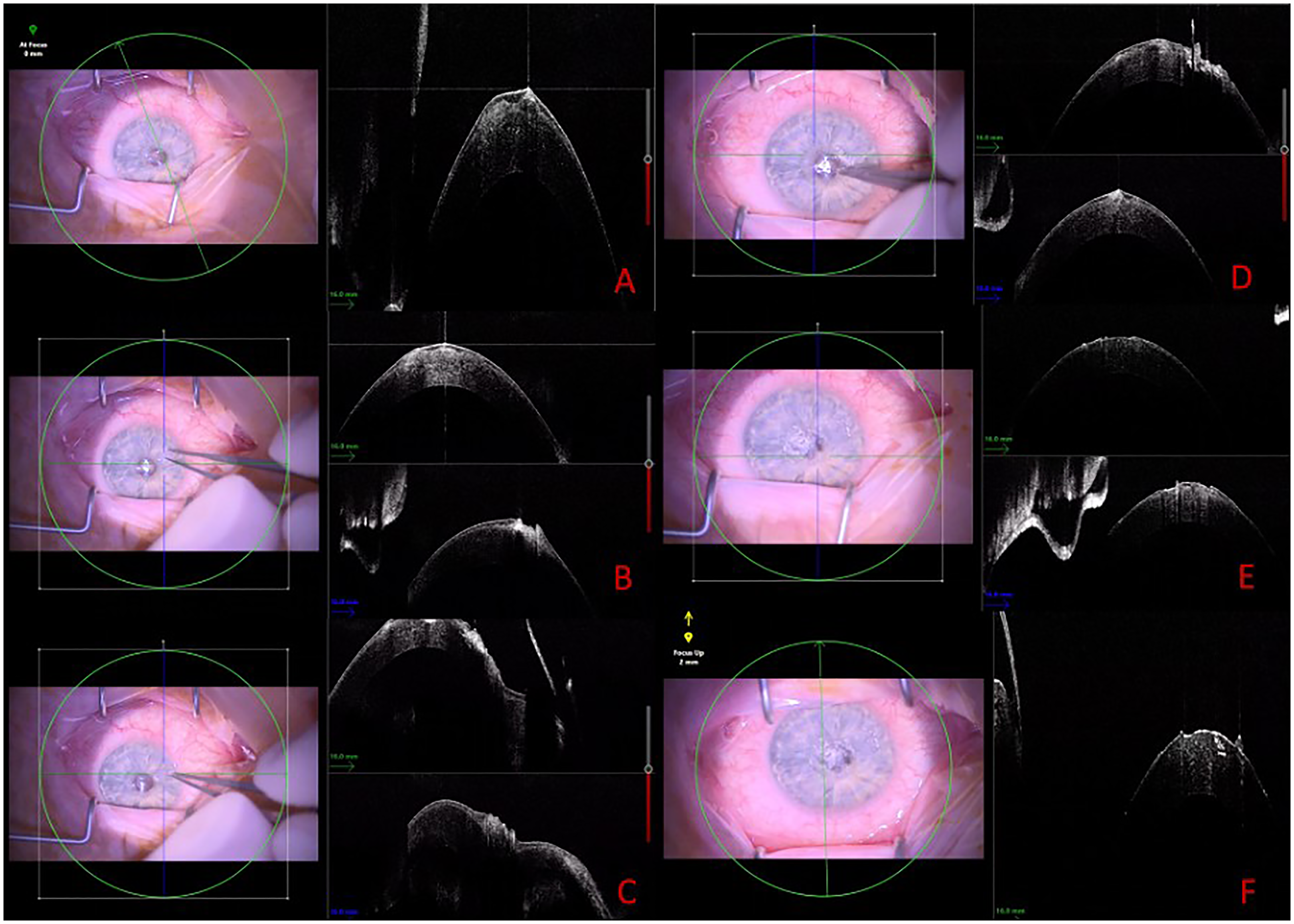
Intraoperative OCT (iOCT) serves as a guide in superficial keratectomy (SK) for Salzmann nodular degeneration (SND).
Surgical ophthalmic forceps, such as Hoskins forceps, are used for the precise excision of identified nodules. They provide a firm grip and allow for the elevation of the nodule's edge, enabling selective removal (Figure 1B-D).
In the presence of dystrophic tissue, the lesion is delicately detached from Bowman's layer using a blunt blade or a cellulose micro sponge, with the goal of removing it in a single layer. When it is difficult to peel the peripheral membrane from the limbus or achieve a smooth surface beneath the lesion, sharp dissection is utilized.
The iOCT is crucial in this process, offering exact mapping of the cleavage plane between the nodules and the surrounding healthy tissue.
Additionally, this technology assists in a comprehensive post-nodulectomy evaluation of the stromal bed (Figure 1 E-F), ensuring the complete excision of dystrophic tissue and reducing the likelihood of leaving behind nodular remnants.
After the nodules have been successfully removed, postoperative care includes the application of topical antibiotic eye drops to prevent infection and mydriatic eye drops to reduce intraocular inflammation. A bandage contact lens is placed over the cornea to mitigate discomfort and support epithelial healing.
Results
Performing superficial keratectomy with the assistance of iOCT enables precise identification and removal of nodules, thereby reducing disruption to surrounding tissue, while real-time feedback on dissection depth facilitates careful excision. After dissection, the stromal bed can be scanned again to check for residual degenerated tissue which might not be easily discernible under the surgical microscope. Residual SND material can be then selectively removed while sparing healthy corneal stroma without the need for extensive keratectomy.
Discussion
Surgical intervention in SND, such as SK, PTK, or their combination, is often necessary for cases with central involvement or peripheral nodules adversely affecting vision. SK is typically favored as the initial surgical treatment for SND owing to its efficacy in alleviating symptoms, its low recurrence rate with adjunct treatments, and its comparative simplicity and cost-efficiency versus PTK. 7 Yet, selecting the most appropriate surgical method must consider individual patient factors, including the specific etiology, any concurrent conditions, and previous interventions.
The advent of anterior segment optical coherence tomography (AS-OCT) has significantly enhanced diagnostic accuracy in SND, offering non-invasive visualization of nodules for detailed examination of tissue planes around the fibrotic nodules. This advancement has proven invaluable for surgical planning, enabling precise localization and characterization of SND nodules.9–12 In this paper, we describe how the intraoperative implementation of OCT technologies (iOCT) has the potential to further improve the surgical management of patients affected by SND, leveraging the unparalleled real-time visualization and resolution of corneal structures offered by iOCT. 13 In this report we highlighted how iOCT has allowed us to identify cleavage planes of SND nodules, facilitating their peeling and assuring a complete removal of the dystrophic tissue, thus guaranteeing a smooth residual stromal bed. Thorough and complete removal of SND nodules, as confirmed in our intraoperative imaging by iOCT, is in fact a key determinant in reducing the risk of possible recurrences and ocular surface discomfort. 1
The use of iOCT in corneal surgery has proven effective in numerous studies.14–16 Notably, the DISCOVER study, the most extensive iOCT study for segment surgeries to date, highlights the reliability of imaging and its impact on surgical decisions, showing how intraoperative imaging crucially informs and guides surgical adjustments across various conditions. 16 Augmented intraoperative visualization of donor and host tissues by means of iOCT is steadily gaining popularity in corneal lamellar surgery and is particularly helpful in conditions of poor visualization. 13 Similarly, Urkude et al. demonstrated that iOCT enhances SMILE surgery outcomes through real-time monitoring of the lenticule's location, effectively combined with the curvilinear lenticulorrhexis technique for optimal results. 14
SND frequently cannot be adequately addressed using the standard scrape-and-peel technique under a microscope, as is typical for many cases. Instead, trimming is often necessary to remove the affected tissue. More accurately known as Salzmann's subepithelial fibrosis, 17 this condition could benefit greatly from iOCT, which aids in the precise excision of fibrotic tissue while minimizing risk to surrounding corneal tissue.
The use of iOCT during surgical procedures for SND signifies a major advancement, offering a deeper understanding of corneal structure and facilitating the precise excision of nodules. The capability of iOCT to provide immediate, detailed visuals of the anterior corneal stroma significantly enhances surgical efficiency by reducing procedure duration without compromising the accuracy or safety.
Furthermore, iOCT not only offers a direct and accurate evaluation of surgical results but also improves the procedure's safety for both patients and surgeons. 13 By enabling real-time observation of corneal layers and nodular formations, it assists in accurately identifying the areas for nodulectomy, thereby reducing the risk of accidental harm to surrounding stromal tissue. This feature increases surgeon confidence, fostering a more secure and controlled operating environment.
To date, the diffusion of iOCT has been limited by the entry cost of the technology. This means that the entry cost for a state-of-the-art iOCT also includes, in more cases than not, the purchase of an integrated microscope.
Nevertheless, clinical studies have proven the utility of iOCT in modern eye surgery and it is reasonable to think that with the increased adoption of these devices and with future technological improvements, their cost can also be mitigated. 13
Given the rapid pace of technological progress and the changing dynamics of ophthalmic surgery, iOCT is expected to become instrumental in future corneal surgeries as well. Its contribution to enhancing surgical precision, efficiency, and safety deems it an invaluable asset in treating SND and potentially other corneal conditions. As this technology becomes more widespread and cost-effective, its routine clinical integration is anticipated to expand, ushering in a novel phase in corneal surgery.
Conclusions
The incorporation of iOCT into surgical procedures for SND marks a notable advancement, facilitating accurate nodular excision and improving surgical efficiency through the provision of immediate, detailed visualization of the corneal structure. Its application in surgeries for Salzmann Nodular Degeneration enhances precision and tissue preservation, ultimately leading to improved surgical outcomes, particularly in circumstances with limited visibility.
Supplemental Material
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Patient consent
The collection of data was performed with approval of the patient. Written consent to publish this case was obtained. This article does not contain any personal information that could lead to the identification of the patient.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.