
Abstract
Aim
To estimate the sensitivity and specificity of topographic and tomographic corneal parameters as determined by Sirius (CSO, Florence, Italy) in discriminating keratoconus (KC) and suspect keratoconus from normal cornea.
Method
In this retrospective case-series study, keratoconus screening indices were measured using Sirius tomographer. Receiver operating characteristics (ROC) curves were used to determine the test's overall predictive accuracy (area under the curve) and to identify optimal cut-off points to maximize sensitivity and specificity in differentiating keratoconus and suspect keratoconus from normal corneas.
Results
Receiver operating characteristics (ROC) curve analyses showed high predictive accuracy for Symmetry Index back (SIb), Keratoconus Vertex front (KVf), Symmetry Index front (SIf), Keratoconus Vertex back (KVb), Apex Keratometry (Curve-Apex) and Minimum corneal Thickness (ThkMin) to distinguish keratoconus from normal (area under the curve > 0.9, all). Symmetry Index back was identified as the best diagnostic parameter for detecting suspect keratoconus with AUC of 0.86. Highest specificity to detect keratoconus and suspect keratoconus was seen for SIb, 99.87% and 84.66%, respectively. These values were associated with optimal cut-off points of 0.46 D for keratoconus and 0.12 D for suspect keratoconus.
Conclusion
Sirius parameters evaluated in the study were effective to differentiate keratoconus from normal corneas. However, Symmetry Index back was the index with the highest ability to detect suspect keratoconus.
Keywords
Introduction
Keratoconus is a progressive corneal disease characterized by progressive stromal thinning of the central and para central portion of the cornea that results in myopia, irregular astigmatism and visual impairment.1,2 Several studies from the Middle East have found high prevalence rate of KC and suspect KC among refractive surgery candidates.3–5 Among different parameters proposed by Randelman et al. to predict the risk of post-LASIK ectasia, early KC was considered as the main risk of this disease. 6 Although the diagnosis of advanced stages of KC does not raise difficulties and is usually made through slit-lamp examination, keratometry, and retinoscopy, many screening tests are needed to detect the early stage of this disease. Initially, the term keratoconus suspect (KCS) was introduced to describe eyes that show subtle Placido-based videokeratography without clinical evidence of disease.7–9 Arbelaez et al. based their diagnostic criteria of KCS on videokeratoscopic and tomographic pattern of localized steepening in the posterior or anterior corneal surface or paracentral corneal thinning, provided there was no evidence of clinical keratoconus in either eye. 9 While Placido-based topography analyzes the central anterior corneal surface, Scheimpflug-based imaging provides data from anterior and posterior cornea and produces a full thickness map. More recently, a variety of corneal indices have been generated to increase the accuracy in detecting ectatic corneal diseases. However, the cut-off value for any parameter will vary depending upon the machine being used.
The aim of this study was to determine the diagnostic ability of Placido/Scheimpflug CSO Sirius tomographer in differentiating between keratoconus, suspect keratoconus, and normal corneas, as well as to ascertain the indices with the highest sensitivity and specificity.
Material and methods
This retrospective, case-control study was conducted at the cornea and refractive surgery department of ophthalmology, Tishreen University, Syria between February 2019 and December 2019. This study was approved by the research committee of Tishreen University in accordance with the ethical standards stated in 1964 Declaration of Helsinki, with informed consent obtained.
Inclusion criteria
The subjects included in this analysis were as follows: (a) known cases of keratoconus who came for follow-up, (b) subjects diagnosed as having keratoconus or suspect keratoconus during refractive surgery screening, (c) subjects with normal cornea recruited from the refractive surgery candidates. The data of one eye (right) was included if both eyes were KC or suspect KC. The patients were recruited consecutively and all the subjects meeting inclusion criteria were included in the study. The diagnosis of keratoconus was made if (a) there was irregular cornea, determined by distorted keratometry mires or distortion of the dilated retinoscopic reflex (or combination of these),10,11 in addition to, (b) at least two of the following tomographic/topographic findings: Abnormal posterior ectasia, abnormal thickness distribution, or symmetry index front (SIf) of > 1.17 D;12,13 or one of the following slit lamp findings: Vogt striae, 2-mm arc of Fleisher ring, or corneal scarring consistent with KC. 14 Suspect KC was defined if there was anterior and/or posterior corneal steepening, absence of clinical (keratometric, retinscopic, or biomicroscopic) signs of keratoconus in either eyes and best corrected visual acuity of 20/20 or better. 9
Exclusion criteria
Patients were excluded if they had previous corneal or ocular surgery (e.g. cataract, glaucoma, corneal cross-linking, excimer laser surgery, intra stromal corneal rings, phakic intraocular lens), any disease that could possibly interfere with the readings/results (e.g. dry eye disease, keratitis, glaucoma, uveitis Fuch's dystrophy, etc,.), corneal scarring not consistent with KC, autoimmune disease, lactation or pregnancy. Before evaluation, contact lens-wearing patients were asked to discontinue wearing their lenses for 3-weeks if utilizing rigid lenses, and for 1-week if utilizing soft lenses.
All subjects underwent a full ocular assessment, including:
Auto-refracto-keratometry (SEIKO CO, GR-3500KA, Japan), uncorrected distance visual acuity (UDVA), corrected distance visual acuity (CDVA), slit-lamp examination to detect the presence or absence of signs of KC (apical scar or thinning, Fleischer rings and Vogt's striae), Goldmann tonometry, and funduscopy. Dilated retinoscopic examination to detect the presence or absence of KC signs (scissoring reflex and Charleaux oil droplet) Placido/Sheimpflug-based corneal imaging.
Topographic, tomographic and pachymetric indices were obtained using Scheimpflug/Placido-based tomography system (Sirius, software version 1.2, Costruzione Strumenti Oftalmici, Florence, Italy). The Sirius is provided with a Scheimplfug rotating camera and 22-Placido rings. Data for the anterior corneal surface are obtained by both Placido disc and Scheimpflug camera, while data for posterior corneal surface and pachymetry are provided by Scheimpflug camera. The Sirius uses a network-based classification system to differentiate between keratoconus, suspect and normal. The sensitivity and specificity of the Sirius software is described elsewhere.
9
Studied parameters: Simulated Average Keratometry (Avg K), Apex Keratometry (Curve-Apex), Symmetry Index front (SIf), Keratoconus Vertex front (KVf), Symmetry Index back (SIb), Keratoconus Vertex back (KVb), Minimum corneal Thickness (ThkMin) and Central Corneal Thickness (CCT). Three Measurements were obtained with the eye aligned to the visual axis. Patients were asked to blink before each image was captured and only images with an acquisition of “OK” were taken.
The mean values of the evaluated indices in the KC, suspect KC, and normal eyes were compared using one way analysis of variance (ANCOVA). Receiver operating characteristic (ROC) curves were generated and areas under the curves (AUC) were calculated for the evaluated parameters. Optimal cut-off points, positive likelihood ratio and negative likelihood for these cut-off points were calculated.
For statistical analysis, MedCalc Statistical Software version 19.5.3 (MedCalc Software bv, Ostend, Belgium) and SPSS software (version, 17, SPSS Inc, Chicago, IL, USA) were used. P values less than 0.05 were considered statistically significant.
Results
A total of 914 eyes of 914 patients were evaluated in this analysis: (83) Eyes (keratoconus), (38) eyes (suspect KC), and (793) eyes (controls) with normal cornea. Mean patient age was (25 ± 6.07 years) overall, (23.61 ± 6.98 years) in the KC group, (25.95 ± 5.75 years) in the suspect KC group and (25.45 ± 5.96 years) in the normal. (Table 1) demonstrates the mean age and sex distributions of the study groups.
Characteristics of participants in the study.
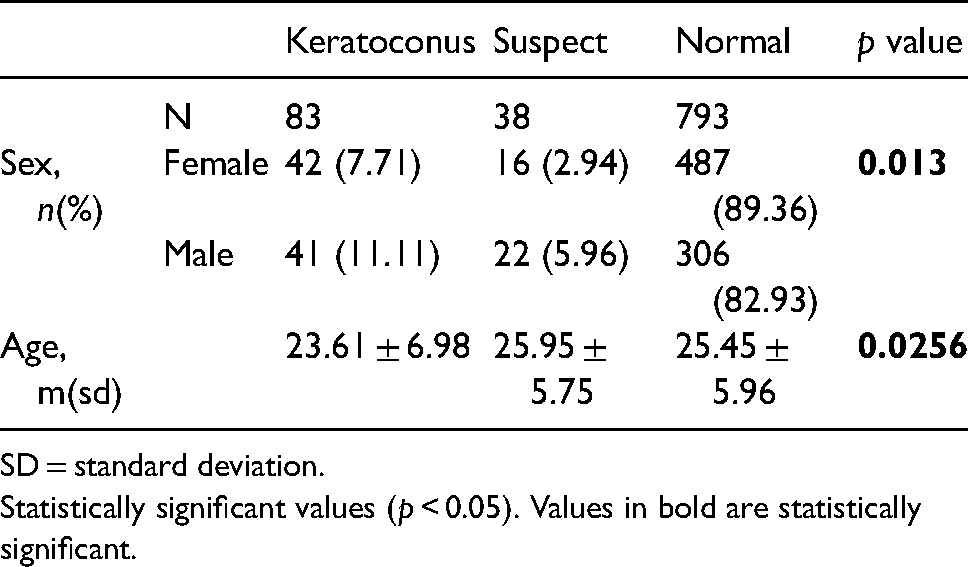
SD = standard deviation.
Statistically significant values (p < 0.05). Values in bold are statistically significant.
Mean values of the evaluated corneal indices for KC, suspect KC, and normal corneas are shown in (Table 2). There was a significant difference between all mean values of KC and normal eyes, and between KC and suspect KC eyes (p < 0.0001, for all). While simulated keratometries (K flat, K steep and K average) and maximum keratometry (curve-apex) of suspect KC showed no significant difference between suspect KC and normal eyes (p > 0.05, for all), the difference of the mean values of SIf, KVf, SIb, KVb, ThkMin and CCT was statistically significant (p < 0,001, for all).
Mean corneal data measurements in the study groups.
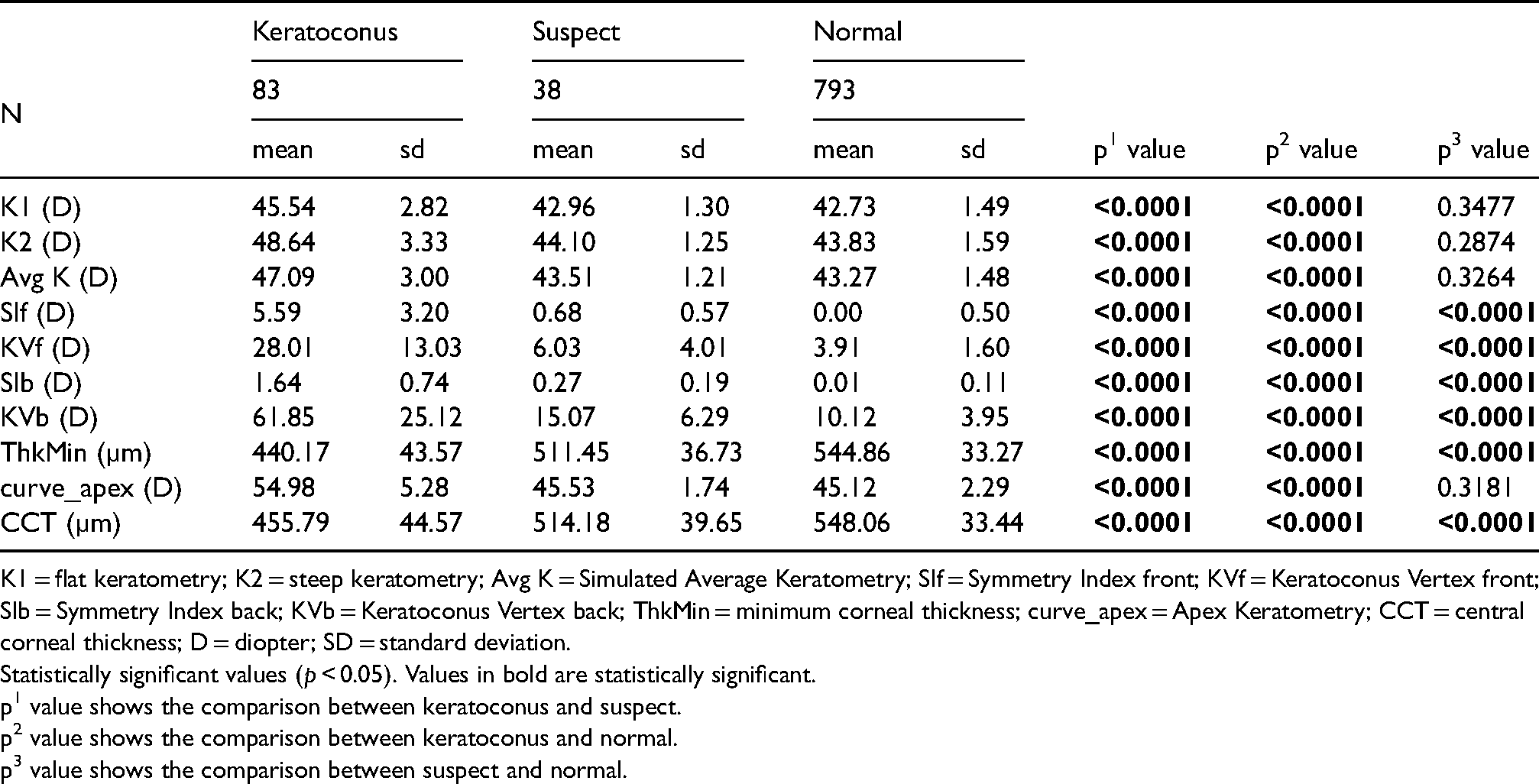
K1 = flat keratometry; K2 = steep keratometry; Avg K = Simulated Average Keratometry; SIf = Symmetry Index front; KVf = Keratoconus Vertex front; SIb = Symmetry Index back; KVb = Keratoconus Vertex back; ThkMin = minimum corneal thickness; curve_apex = Apex Keratometry; CCT = central corneal thickness; D = diopter; SD = standard deviation.
Statistically significant values (p < 0.05). Values in bold are statistically significant.
p1 value shows the comparison between keratoconus and suspect.
p2 value shows the comparison between keratoconus and normal.
p3 value shows the comparison between suspect and normal.
Tables 3 and 4 demonstrate the sensitivity, specificity, and positive and negative likelihood ratios (LRs) identified by cut-off points for evaluated parameters in differentiating between eyes with keratoconus and suspect keratoconus, respectively from normal. While all evaluated parameters showed high sensitivity of more than 90%, SIb was the index with the highest sensitivity and specificity (100% and 99.87%, respectively) to distinguish keratoconus from normal corneas. While ThkMin, CCT and SIb showed sensitivity of 92.11%, 90.91% and 81.58% respectively to distinguish suspect KC from normal eyes, the highest specificity (84.66%) was seen for SIb.
Sensitivity, specificity, positive and negative likelihood ratios and cutoff points for different corneal parameters to differentiate eyes with keratoconus from normal corneas.
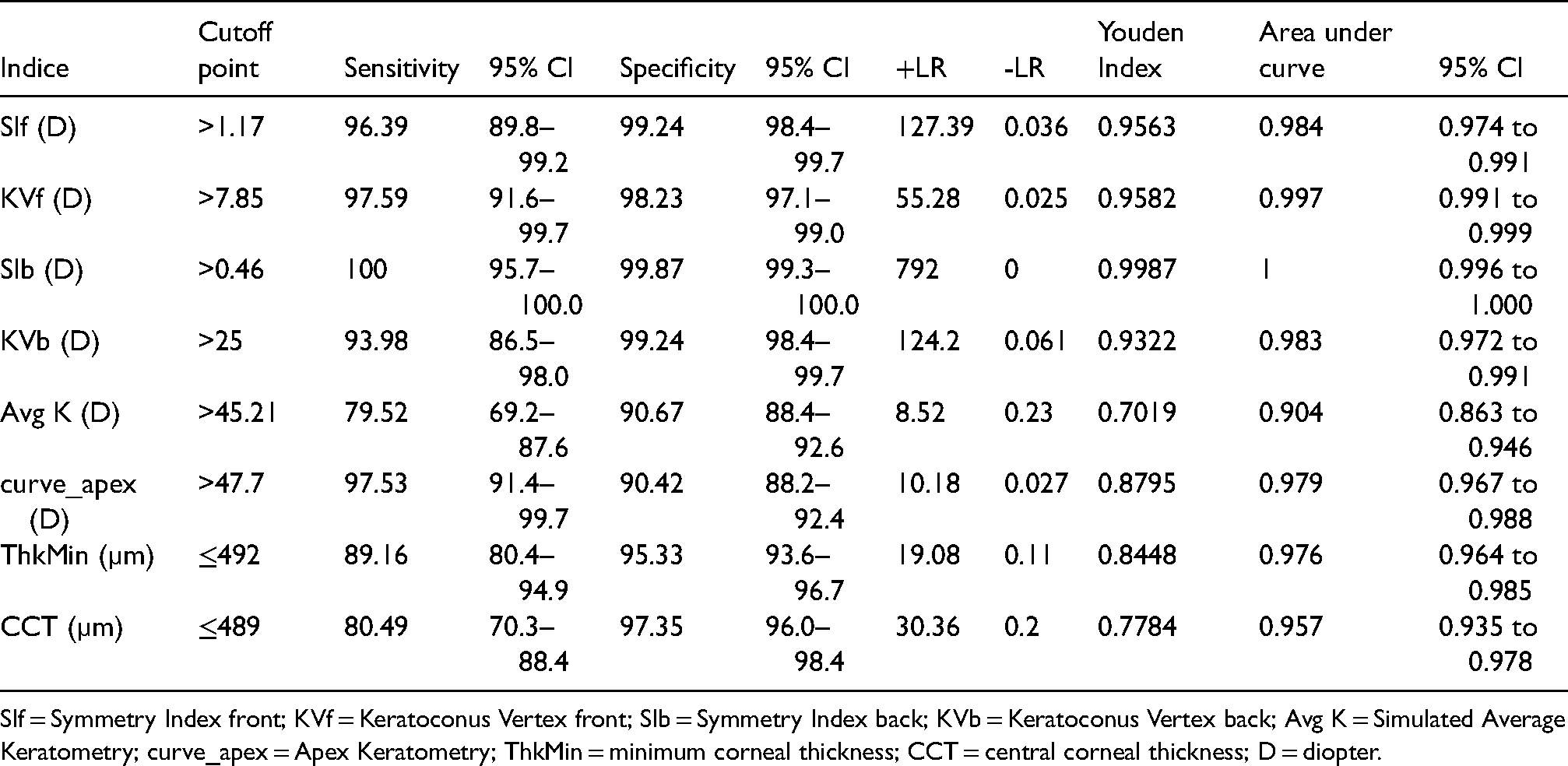
SIf = Symmetry Index front; KVf = Keratoconus Vertex front; SIb = Symmetry Index back; KVb = Keratoconus Vertex back; Avg K = Simulated Average Keratometry; curve_apex = Apex Keratometry; ThkMin = minimum corneal thickness; CCT = central corneal thickness; D = diopter.
Sensitivity, specificity, positive and negative likelihood ratios and cutoff points for different corneal parameters to differentiate eyes with suspect keratoconus from normal corneas.
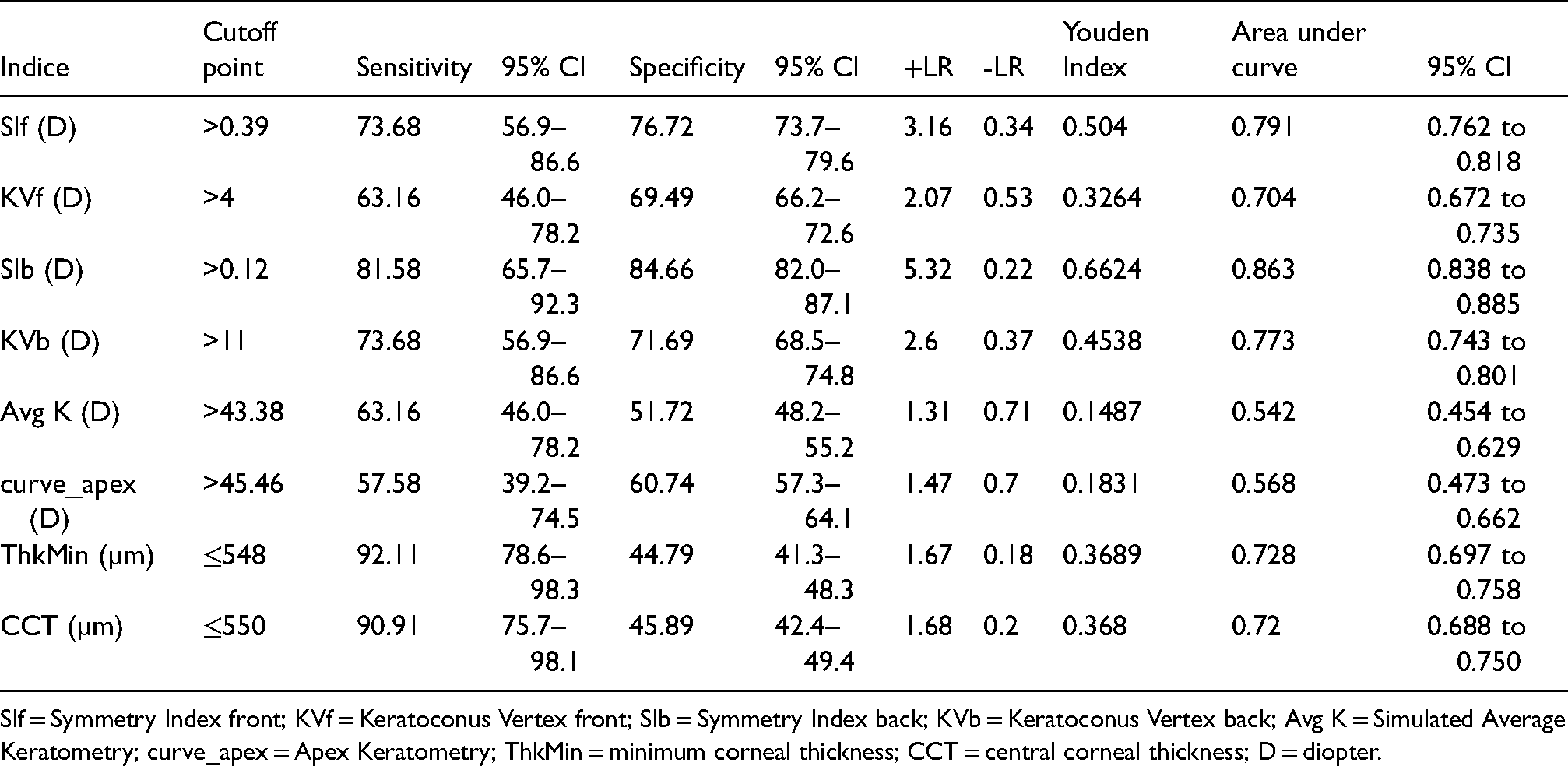
SIf = Symmetry Index front; KVf = Keratoconus Vertex front; SIb = Symmetry Index back; KVb = Keratoconus Vertex back; Avg K = Simulated Average Keratometry; curve_apex = Apex Keratometry; ThkMin = minimum corneal thickness; CCT = central corneal thickness; D = diopter.
Figures 1 and 2 compare the parameters that showed the best AUC to distinguish keratoconus and suspect keratoconus, respectively from normal eyes. While SIb, KVf, SIf, KVb, Curve-Apex and ThkMin were strong enough (AUC > 0.9, all) to distinguish keratoconus from normal eyes, the same was not true for suspect keratoconus (AUC < 0.9, all). However, SIb was the parameter with the best AUC to distinguish keratoconus and suspect keratoconus from normal, 1.0 (95% CI, 0.99–1.00) and 0.86 (95% CI, 0.83–0.88), respectively.
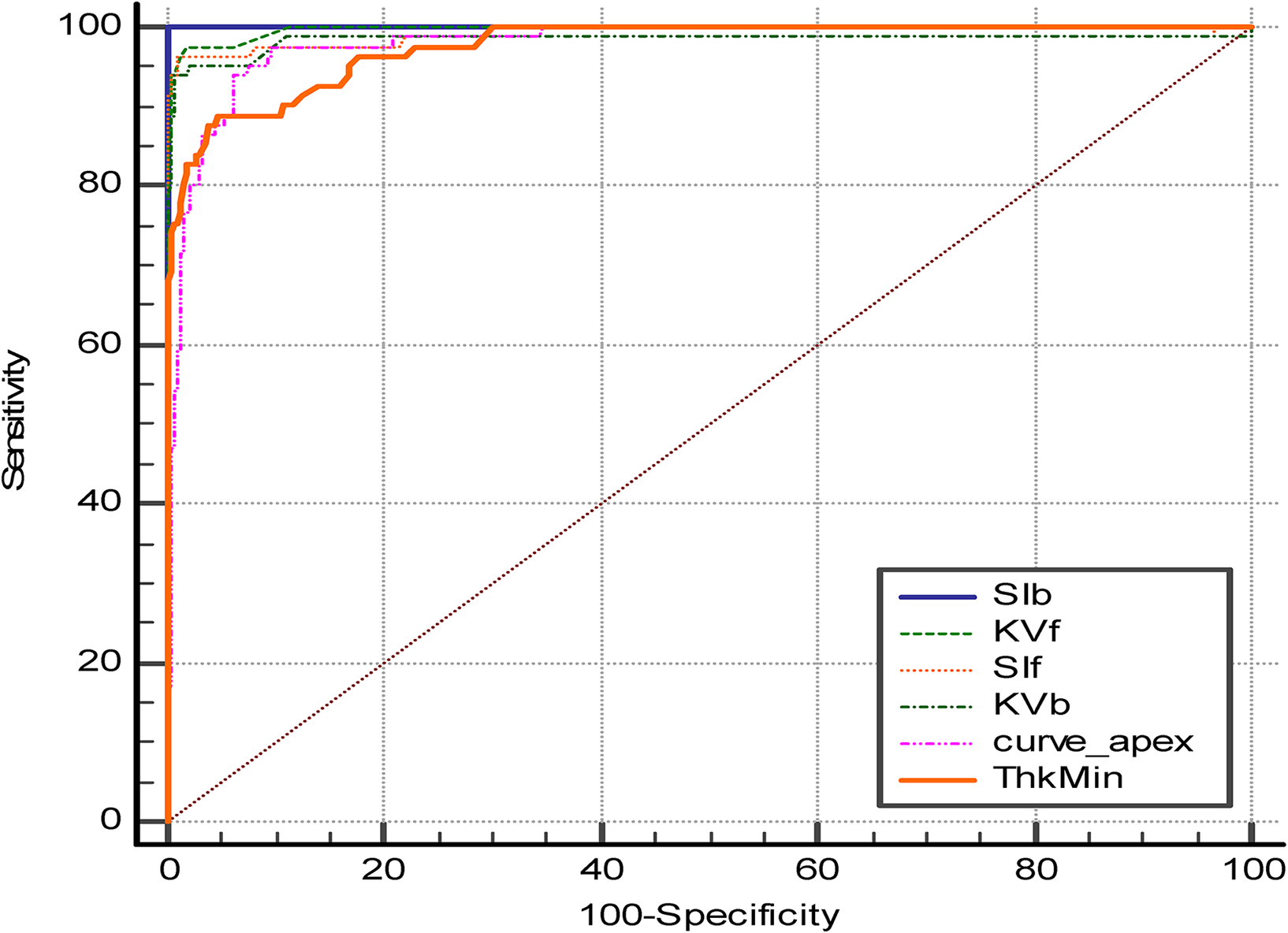
Comparison of the parameters that showed the best area under the receiver operating characteristic curves to differentiate keratoconus from normal eyes.
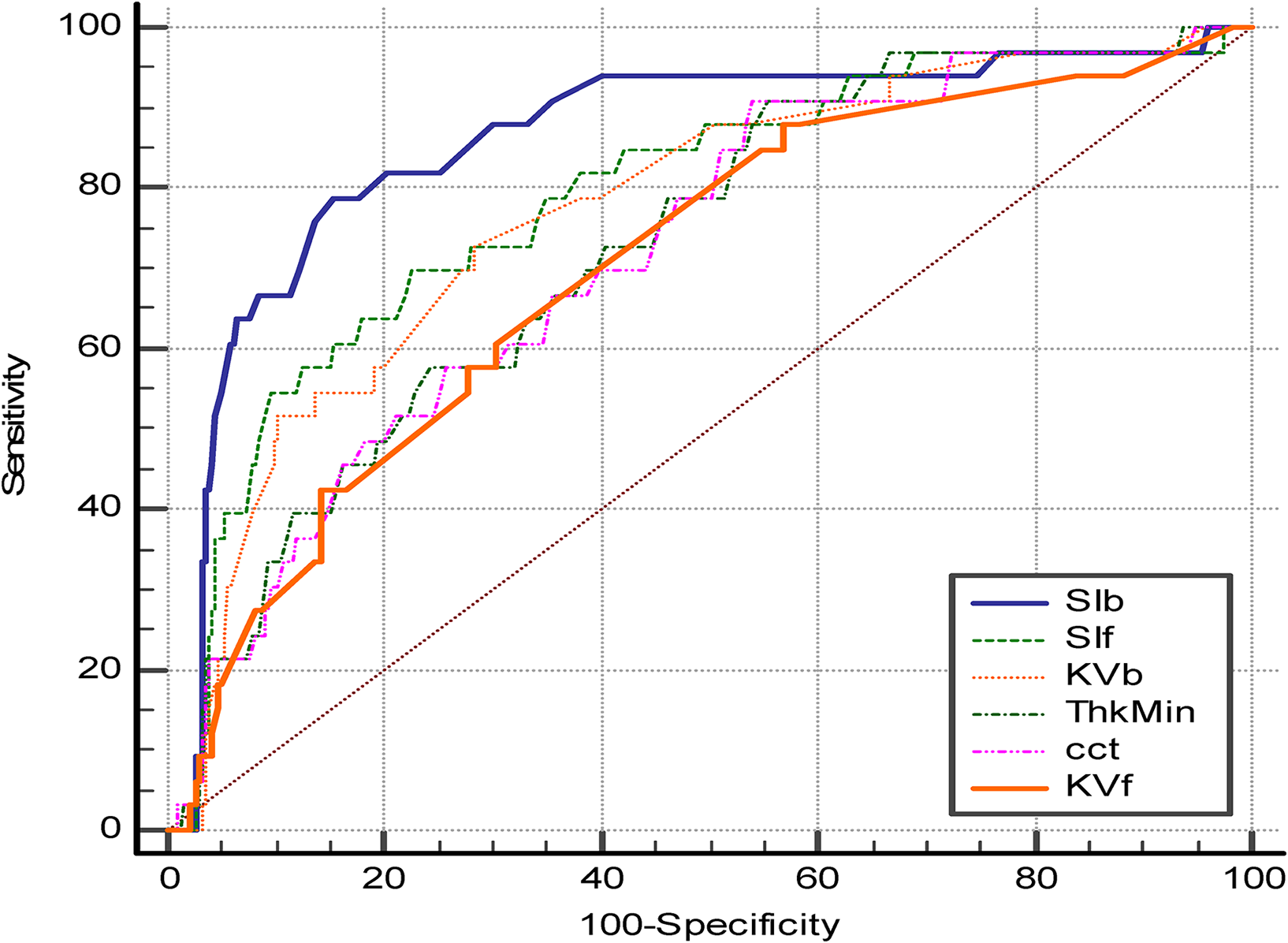
Comparison of the parameters that showed the best area under the receiver operating characteristic curves to differentiate suspect keratoconus from normal eyes.
Discussion
Corneal topography is important to diagnose a variety of corneal abnormalities such as keratoconus, forme fruste keratoconus and pellucid marginal degeneration. It is also a very essential tool for preoperative assessment in refractive surgery. All patients with a diagnosis of atopy, noninflammatory connective disease, Down syndrome or anisometropia coming for refractive surgery should be examined carefully for signs of keratoconus.15,16 Corneal tomography is also recommended in children with astigmatism and anisometropic amblyopia, as pediatric keratoconus could be misdiagnosed as meridional amblyopia. 17
A literature search showed a few previous studies evaluating keratoconus screening parameters of the Sirius topographer. Some parameters were evaluated in the study by Shetty et al. who compared the sensitivity and specificity of keratoconus screening indices of three different Scheimpflug devices, Pentacam, Galilie, and Sirius. 13 Based on the Sirius topographic and tomographic data, Arbelaez et al. introduced a support vector machine-based algorithm for the diagnosis of keratoconus. 9 Our study presents the characteristics of keratoconus indices measured with Sirius corneal tomographer in eyes with keratoconus, eyes with suspect keratoconus and controls, to evaluate their ability to distinguish between normal and ectatic corneas.
In consensus with previously reported studies,13,18,19 all parameters evaluated revealed statistically significant differences between the keratoconus and normal groups. The fact that age and gender distributions were significant among the groups may have caused the parameters affected by age and gender to be significant. We consider this issue as one of our study limitations, as age and gender matching could provide more objective data.
We further evaluated the area under the curves (AUC), which determines the ability of the parameter to classify the eyes with and without the disease. While all indices showed sufficient predictive accuracy, (AUC >0.9) to differentiate keratoconus from normal, Symmetry Index back (SIb) was the index with the highest ability to distinguish suspect keratoconus from normal. The SIb is defined as the difference of the mean posterior tangential curvature of two circular zones centred on the vertical axis in the inferior and superior hemispheres; positive values indicate a steeper inferior hemisphere, whereas negative values indicate a steeper superior hemisphere. The optimum cut-off point of SIb proposed by Shetty et al. to differentiate KC from normal was >0.32 D with sensitivity of 88.5% and specificity of 100%. 13 A cut-off point of > 0.42 D in our study showed sensitivity of 100% and specificity of 99.87%. We found that the best cut-off value to differentiate suspect KC from normal eyes was > 0.12 D with 81.58% sensitivity and 84.66% specificity. Although the cut-off value > 0.21 D proposed by Shetty et al. showed specificity of 100%, its sensitivity was 16.12%, suggesting very limited sensitivity. We assume the value of the cut-off point will vary if one is screening (e.g. refractive surgery) as sensitivity would be the main concern vs. treating (e.g. corneal cross-linking) where specificity has greater importance. Since we prefer to falsely account a cornea as ectatic than to miss suspect cases during the preoperative screening of refractive surgery, we find that our cut-off value is very effective and clinically applicable.
Besides the SIb index, we also evaluated indices obtained from the anterior corneal curvature. Consistent with Hashemi et al. who used similar indices obtained with Pentacam; Index of Vertical Asymmetry (IVA) and Index of Surface Variance (ISV), 18 we found that the predictive power of the Symmetry Index front (SIf) was higher than mean keratometry for distinguishing clinical and suspect keratoconus from normal. In line with our finding, Shetty et al. proposed a SIf cut-off point of 1.17 D to differentiate keratoconus from normal, which is the same of ours. However, the sensitivity was higher in our study; 96.39% versus 84.6% in Shetty et al. study. The cut-off point of SIf proposed by Shetty et al. to distinguish suspect KC from normal was 0.75 D with sensitivity of 29.7% and specificity of 79.1%. Our cut-off value of 0.39 D showed higher sensitivity (78.68%) and specificity (76.72%). This discrepancy could be explained by different age groups, sex and ethnicity in these two studies. According to the routine definition, mean keratometry value of more than 47 D is considered effective in detecting definite keratoconus; 19 our finding showed that a cut-off point of 45.2 D was more effective in detecting keratoconus. Consistent with our results, Hashemi et al. proposed a cut-off value of 44.9 D. Prakash et al. evaluated the difference in central (apex within central 2-mm) and non-central KC (apex outside central 2 mm), and they found that non-central KC had lesser effect on simulated keratometries. 20 They recommended using criteria of SimK steep >45.8 D to rule out keratoconus. Although these findings to some extent support our result, we do consider one of our study limitations to be that KC was not evaluated concerning cone location.
Our study showed that mean posterior corneal elevation was statistically higher in keratoconus (61.85 ± 25.12 µm) and suspect keratoconus (15.07 ± 6.29 µm) versus normal (10.12 ± 3.95 µm) (Table 2). In contrast, De Sanctis at el. reported higher mean posterior elevation values; 100 ± 49.2 µm for KC, 39 ± 15 µm for subclinical KC, and 19.8 ± 6.37 µm for normal. 21 Consistent with these findings, De Sanctis, et al. proposed cut-off values of 35 µm for KC and 29 µm for suspect KC. Our corresponding values were 25 µm for KC and 11 µm for suspect KC. We hypothesized these differences are attributed to the difference in diagnostic tools in each study, Sirius topography in the present study and Pentacam imaging in De Sanctis study. In De Sanctis’ study, measurements were taken as the maximum value above the best-fit sphere within the central 5 mm of the posterior cornea. Our values were obtained using Sirius, software version 1. 2 where posterior elevation data are taken as posterior elevation with respect to best-fit reference asphero-toric surface with asphericity equal to its average value in the 8 mm zone. This type of representation hides the contribution of astigmatism of the posterior corneal surface, where the ectasia appears earlier and stronger than in the anterior surface. 22 In this study, we found that both the cut-off points derived from anterior and posterior corneal elevations were associated with high sensitivity and specificity to differentiate KC from normal (Table 3). However, anterior elevation data was less powerful in discriminating suspect KC from normal eyes as compared to posterior elevation data (AUC; 0.77 versus 0.70). Several studies have indicated that the early ectatic changes can be seen on the posterior corneal surface.21–23 Reinstien et al. stated that epithelial remodelling might be significant enough in early KC to mask stromal surface changes from anterior surface topography. 24 These pathophysiologic findings may explain our results, which showed that parameters derived from posterior corneal surface were more powerful in detecting suspect KC as compared to those derived from anterior corneal surface.
In addition to corneal curvature and elevation indices, we evaluated thickness parameters. Ambrosio et al. hypothesized that relying on relative corneal thickness instead of thickness points is more important in detecting KC and FFKC. 25 In our study, although ThkMin and CCT revealed high ability to detect KC (AUC >0.9, both), their ability was less pronounced in detecting suspect KC (AUC <0.8, both). Thus, pachymetry indices should not be used alone in refractive surgery screening; they should be combined with other data for detecting cases with suspension.
According to the recent study by Tunç U et al. the parameters used in the diagnosis of KC in the Sirius corneal tomographer may differ more than expected at stage 3 and 4 of the disease. 26 We thus hypothesize that in our study, the reason behind the high sensitivity and specificity of the evaluated parameters in distinguishing KC may in fact be due to the overall advanced stage of the KC eyes included. This could be included as a limitation in our study, as corneal parameters were not compared across different stages of KC. Further prospective studies in different stages of keratoconus would result in more accurate reproducibility to detect keratoconus.
In the current study, special attention was paid to identifying suspect keratoconus. While SIf, KVf, KVb, ThKin and CCT indices revealed acceptable validity (AUC between 0.7 and 0.8), the Scheimplfug elevation-based Symmetry Index back (SIb) demonstrated the highest ability to discriminate suspect KC from normal eyes (AUC = 0.86). Ophthalmologists need to be aware that some corneal anomalies induced by corneal scars, dry eye or hard contact lens, may present videokeratoscopic inferior steepening identical to that seen during the early stage of keratoconus (false positive) (Figure 3). On the contrary, videokeratoscopy may show normal findings at the same time that Scheimpflug does detect abnormal posterior corneal changes (false negative) (Figure 4). Depending on Scheimpflug imaging, Wolf et al. reported four cases as forme fruste keratoconus FFKC, despite Placido-based data being normal. 23 These findings could explain the increased sensitivity and specificity of the indices obtained from the posterior corneal surface.
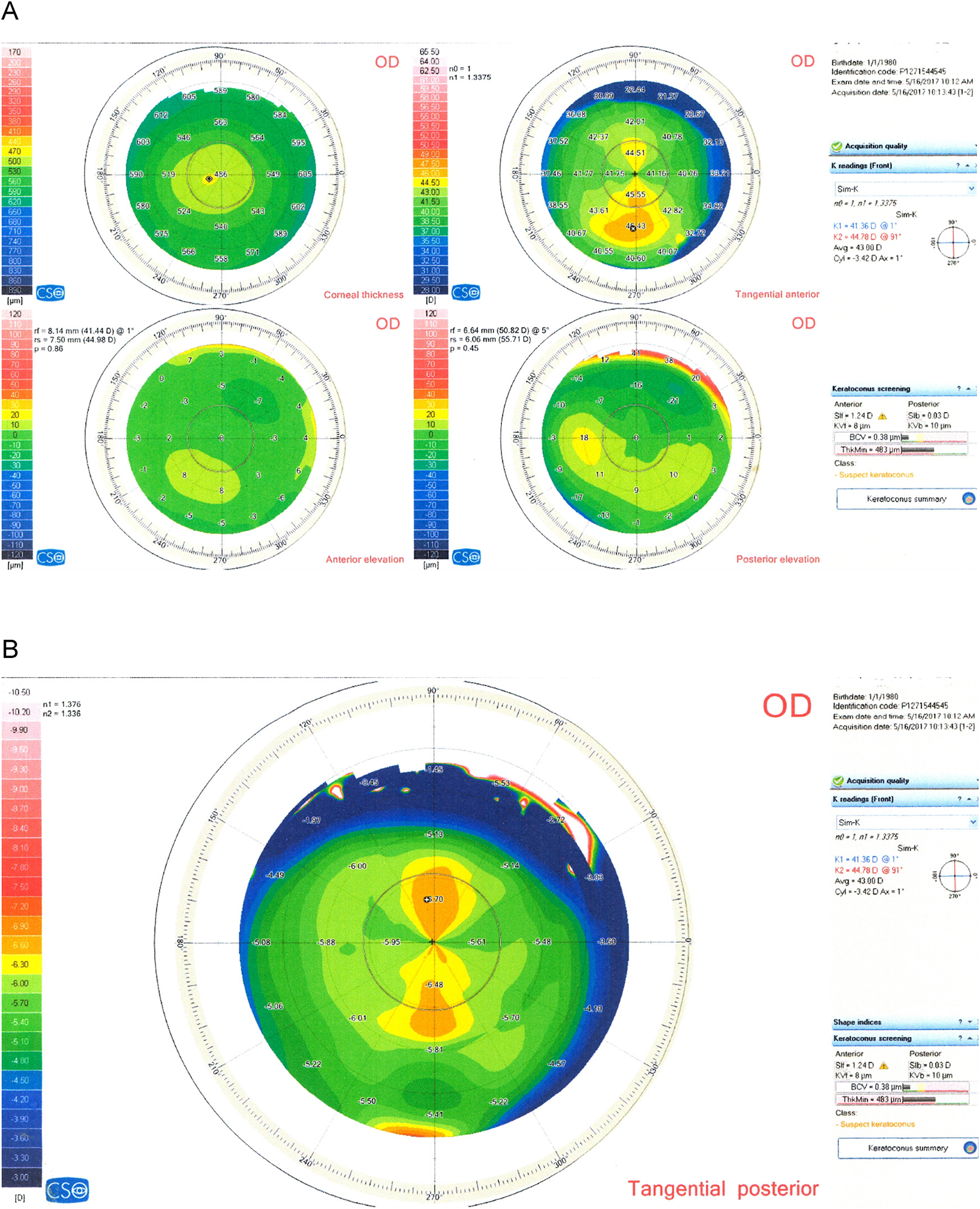
A: four-maps display on the Sirius showing inferior steepening with asymmetrical bow-tie on the tangential anterior map due to corneal scar (upper left). The Sirius software indicates Suspect Keratoconus class. B: Tangential posterior map of the same eye shows normal symmetrical bow-tie appearance; SIb = 0.03 D (False positive).
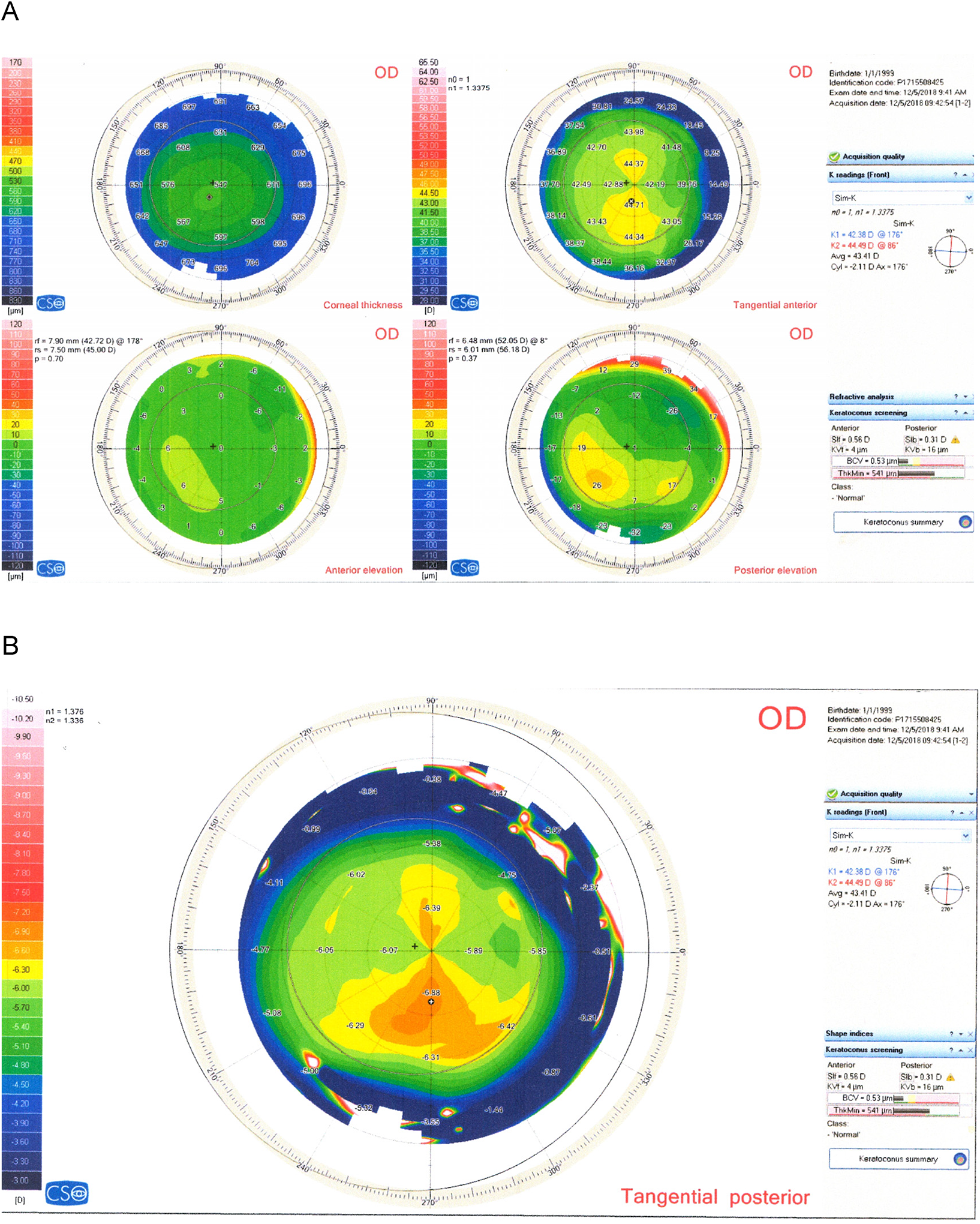
A: Four- maps display on the Sirius demonstrates normal symmetrical bow- tie curvature on the anterior tangential map, while Sirius software displays normal class. B: Tangential posterior asymmetrical bow-tie curvature with inferior steepening; SIb = 0.31 D. Based on SIb value (more than 0.12 D), this case should be considered as suspect and evaluated with great care before refractive surgery. Although Sirius software displays Normal class (False negative).
The multivariate indices that combine different topographic indices were found to have the best capability to diagnose suspect KC. Saad and Gatinell used Orbscan IIz and OPD-Scan (corneal Navigator; Nidek Co., Ltd) to introduce neural network criteria generated from corneal thickness and curvature measurements over the entire cornea centred on the thinnest point. 27 These indices reached high AUC in distinguishing KC and FFKC from normal, 0.99 and 0.98, respectively. When subclinical KC were differentiated from normal corneas, Shetty et al. found that the validity of Belin/Ambrosio display enhanced ectasia total deviation value (BAD-D) of Penatcam was similar to surface irregularity index (SRI) of Galilei but was significantly greater than 8 mm root mean squad per unit area value (RMS/A) of Sirius. In this study, symmetry index back (SIb) showed similar validity to BAD-D of Pentacam and SRI of Galilei in distinguishing suspect KC. The indices which were proposed in this study could enhance future machine-learned application for better detecting keratoconus and suspect keratoconus.
In conclusion, the cut-off points proposed in our study had sufficient enough sensitivity and specificity to discriminate keratoconus and suspect keratoconus from normal. However, Symmetry Index back (SIb) was the index with highest validity to detect suspect keratoconus eyes.
Footnotes
Author's contributions
AS was the major contributor, interpreted the data, and wrote the manuscript.
Availability of data and materials
The datasets used and analyzed during the current study are available from corresponding author (AS) upon reasonable request.
Consent of publication
Consent for publication, was obtained from all study subjects.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
This study was approved by the research ethics committee of Tishreen University in accordance with tents of the Declaration of Helsinki. Informed consent, in Arabic language, to participate in this study was obtained from all participants.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.