
Abstract
Background
Various ocular implants were suggested as a means of enhancing vision in patients with advanced age related macular degeneration. Recently, a new generation of implantable telescopes has been released. The purpose of this study is to report the surgical technique of implantation along with patient outcomes.
Methods
This work focuses on the surgical technique. Crucial surgical steps are carefully reported along with discussion on main drawbacks and limitations.
Results
This approach uses a preloaded delivery system with improved features and requires a smaller incision. First patient outcomes are also reported.
Conclusions
Surgical steps to implant this preloaded intraocular telescope are easier than previous versions, however this remains a complex procedure. Initial patient functional outcomes look promising.
Introduction
The primary cause of vision loss in the population over 50 years old in developed countries is age-related macular degeneration (AMD). 1 So far, there is no treatment for advanced AMD and patients are trained to use supportive measures for low vision including external magnifiers and telescopes. Surgical options in this cases are currently limited and include macular translocation surgery and, more recently, retinal pigment epithelial transplant. 2
In this context, different ocular implants were proposed to improve vision in advanced AMD patients: the Implantable Miniature Telescope (IMT) (Visioncare Ophthalmic Technologies, Inc.), 3 the Intraocular Lens for Visually Impaired People (IOL-VIP, Lenspecial) 4 and The iolAMD (London Eye Hospital Pharma). 5
More recently a new device the SING IMT (Small-Incision New Generation Implantable Miniature Telescope) was introduced. The SING IMT is a Galilean telescope implant with an ultra-precision wide-angle micro optics that creates a magnifying telephoto effect reducing the visual impact of scotoma using a 2.7x magnification. It is a preloaded delivery system with a foldable wing design made of glass and silicon. The optic diameter is 3.6 mm, the haptic diameter is 10.8 mm, the axial length is 4.4 mm and the visual field is 20°. To the best of our knowledge there is no published study with this new device, preliminary results will be published as soon as necessary data will be available. The purpose of this study is to describe the surgical technique of this new implant.
Surgical procedure
Pre-operative procedure
Topical nonsteroidal anti-inflammatory drug (NSAID) was prescribed for 3 weeks before surgery. Topical mydriatic agents were used for pupil dilation, and anesthesia was induced by peri-retrobulbar delivery of ropivacaine 7.5 mg/ml.
Incision, capsulorhexis and phacoemulsification
The incision, capsulorhexis, and phacoemulsification were performed. An 8 mm corneal ink mark with a Castroviejo caliper was made, and a fornix-based conjunctival peritomy was carried out from 8 to 2 o'clock (Figure 1). A 2.2 mm sclero-corneal incision was then made at 1 mm behind the limbus. The capsular rhexis was 6 mm in size, and a standard phacoemulsification was performed with the Stellaris Elite (Bausch & Lomb, Inc.) phacoemulsification system. Afterwards, the main incision was enlarged to 8 mm, and the anterior chamber and capsular bag were filled with cohesive ophthalmic viscosurgical device (OVD). The endothelium was covered with dispersive OVD to ensure protection (Figure 2).
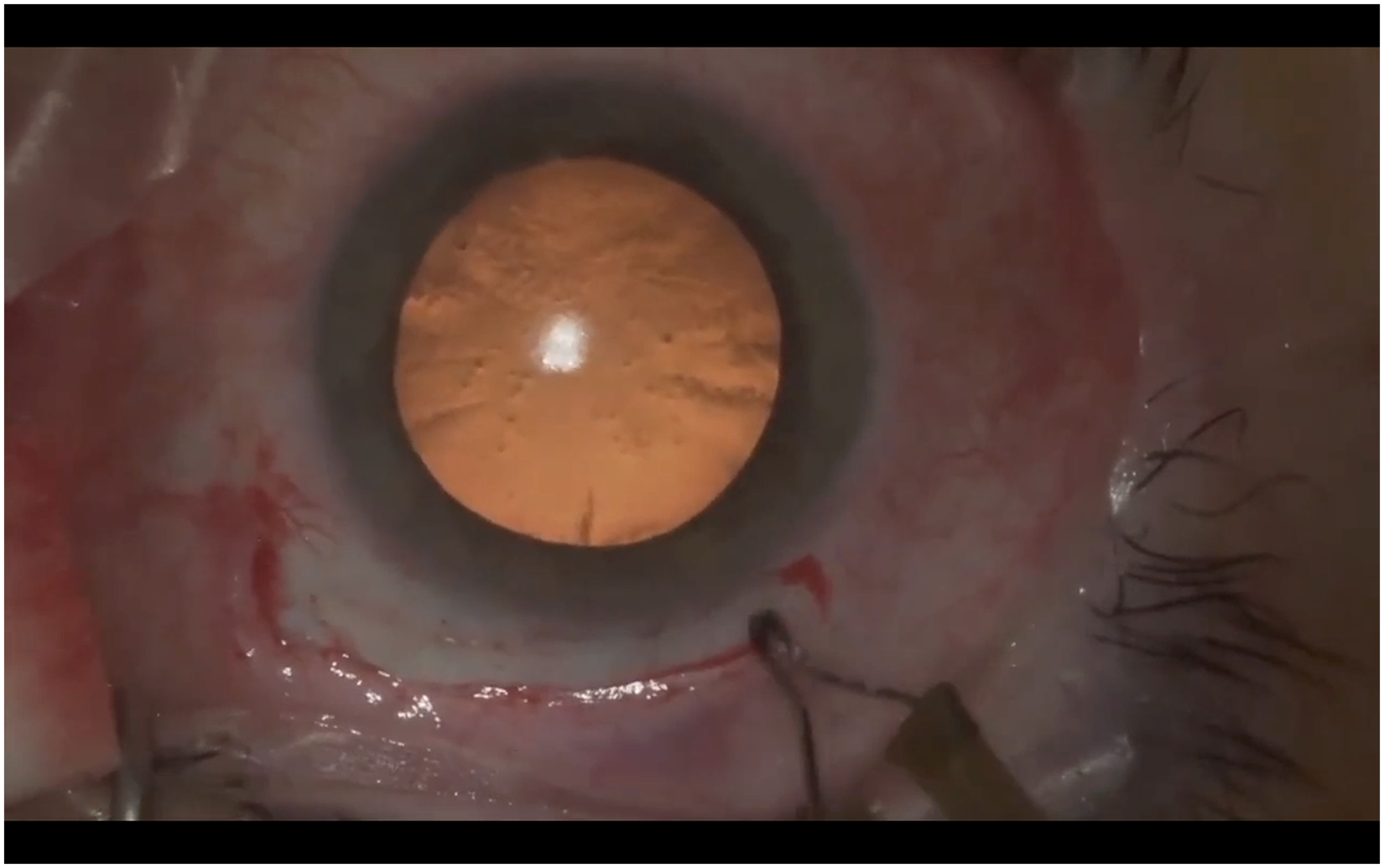
First surgical step: Conjunctival peritomy.
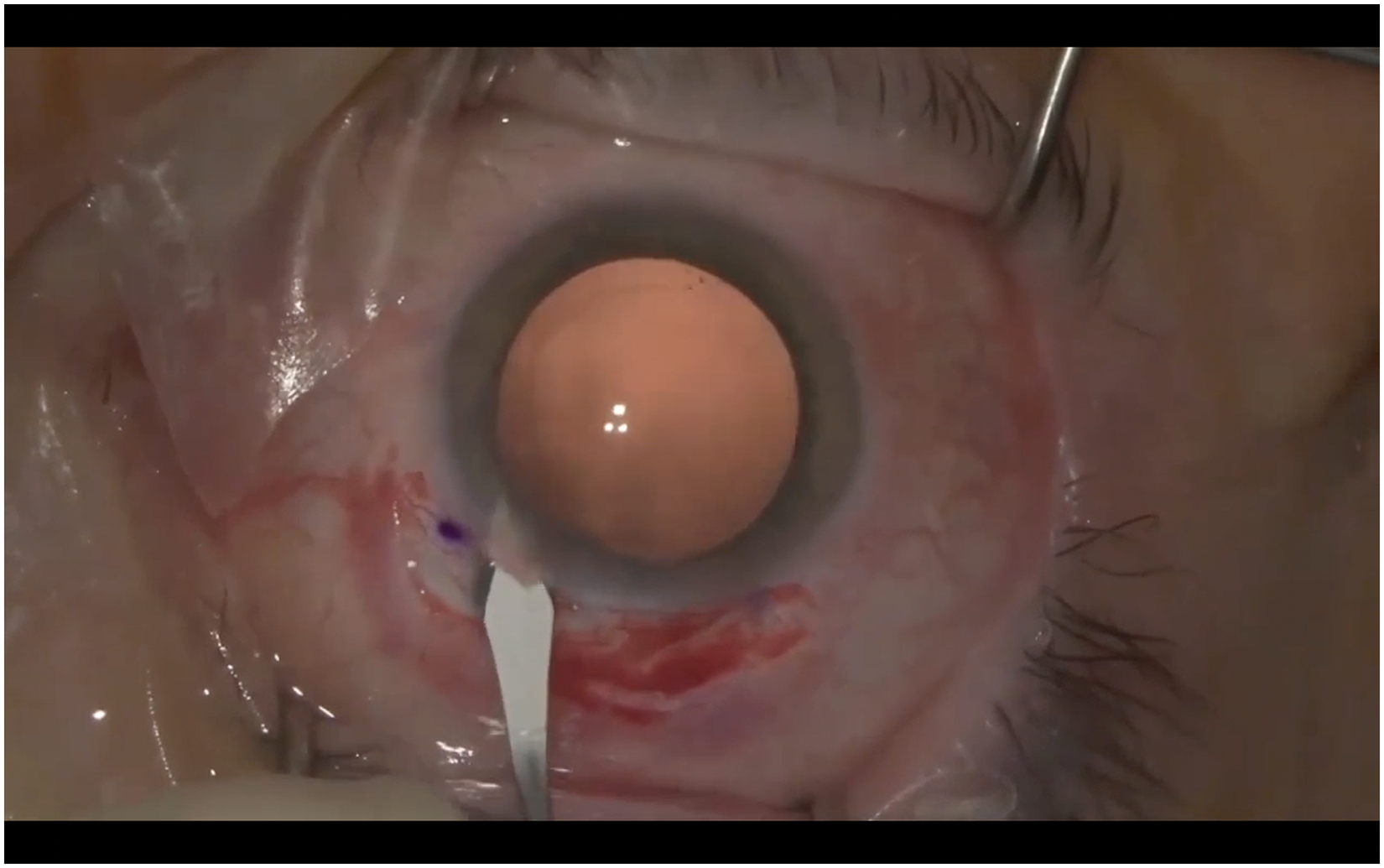
Enlarging the main incision up to 8 mm after marking with a ink colored Castroviejo caliper.
Preloaded system preparation
The preloaded system was prepared by connecting the OVD syringe to the cartridge, unlocking and loading the system, and pushing the plunger into the tip. The empty space at the edge of the tip was filled with OVD to prevent air bubble insertion into the anterior chamber, and the safety cap was removed.
Device implant
The device tip was slowly inserted into the limbal incision, bringing it to the rhexis plane bag while gently lifting the cornea to avoid its bending (Figure 3). Once the syringe wings were rotated to the preferred injection angle, the device tip was positioned at about a 50° angle to the surface of the rhexis of the capsular plane. The leading haptic of the device deployed first in the bag equator and was designed to leverage the other haptics. After implant delivery, the injector body was gently removed out of the eye by short rotating movements. Haptics were placed at 12, 4, and 8 o'clock. At the end of the positioning, the OVD was gently removed from the capsular bag with bimanual irrigation-aspiration, and wound closure was carried out with a continued 10-0 nylon suture (Figure 4). Intracameral cefuroxime was injected as prophylaxis for endophthalmitis. The conjunctiva was closed with two single Vycril 8-0 sutures.
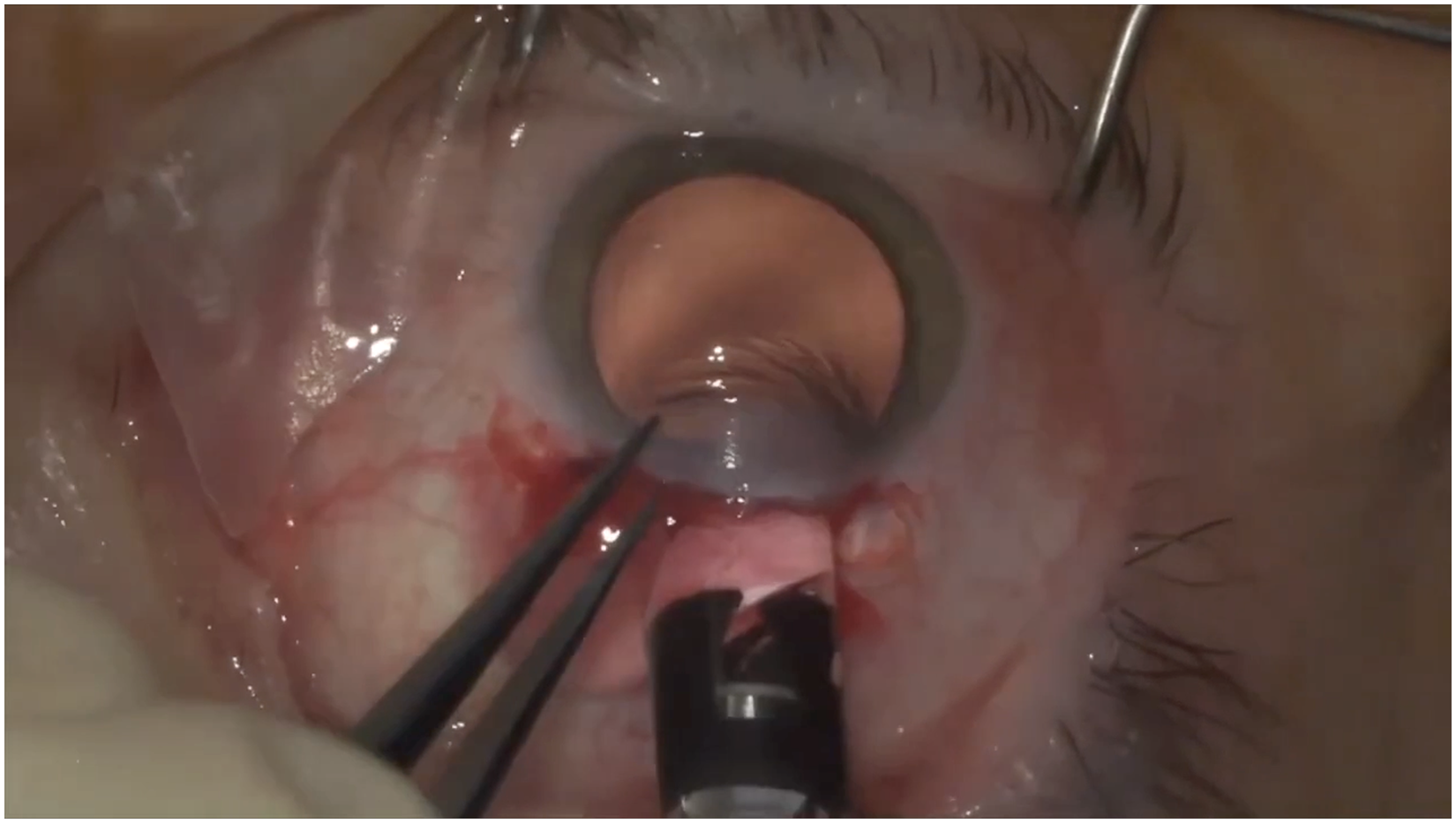
SING IMT delivery using the preloaded system.
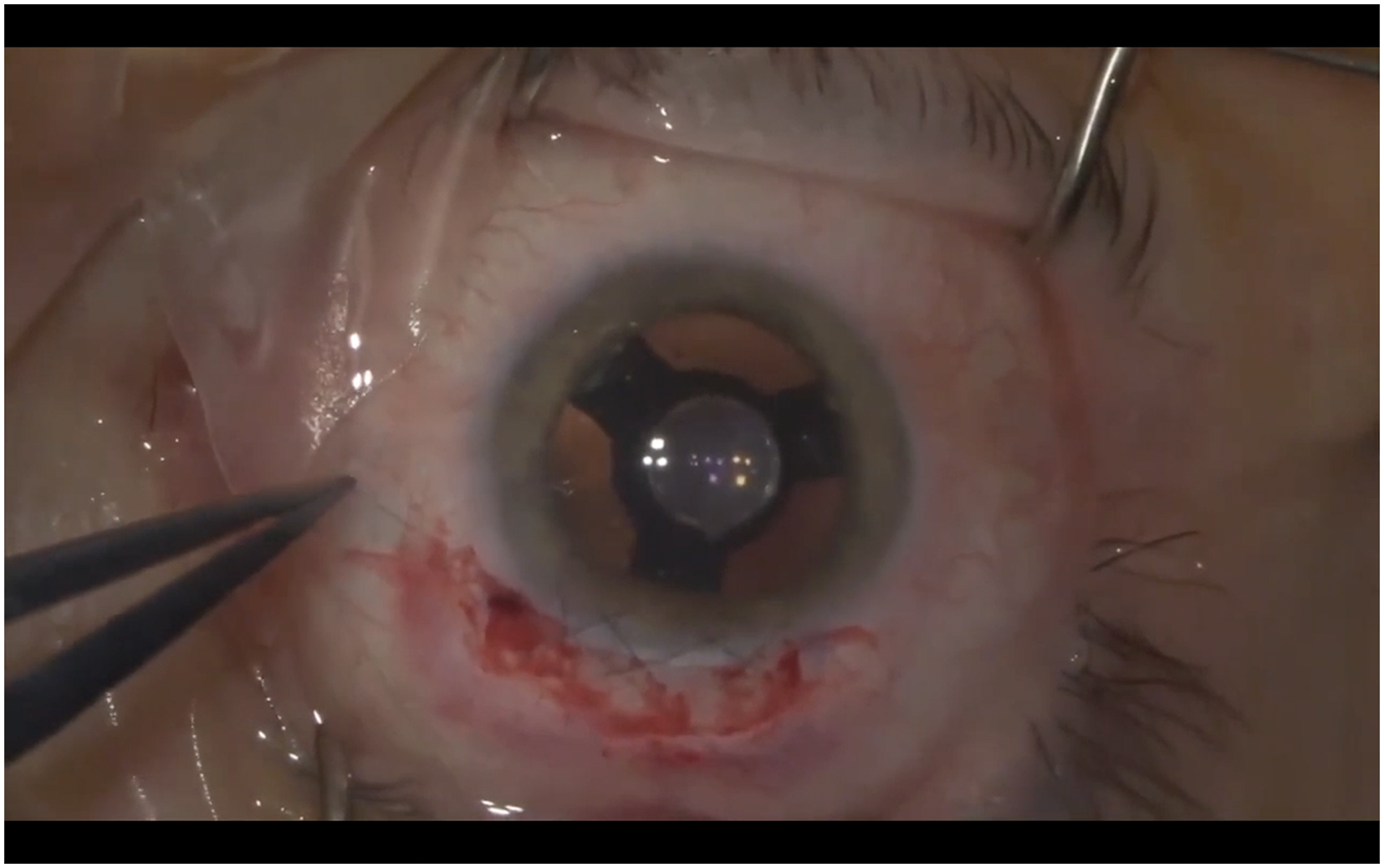
Final result, SING IMT centered and main access sutured with a 10-0 nylon continuous suture.
Post-operative period
Post-operative therapy included topical 1 mg/ml dexamethasone with 5 mg/ml and levofloxacin 5 mg/ml four times a day for seven days, followed by 2 mg/ml topical dexamethasone for fourteen days and then tapered down. Lastly, a peripheral YAG (yttrium aluminium garnet) iridotomy was performed two weeks after surgery, as small as possible, to avoid a second image while preventing a potential pupillary block.
Patient outcomes
In this case of a 70-year-old woman affected by bilateral dry age-related macular degeneration, the device was implanted after obtaining informed consent. The best corrected visual acuity (BCVA) was 1.0 logMAR (Logarithm of the Minimum Angle of Resolution). Four months after the implant in the right eye, the BCVA was 0.6 logMAR, intraocular pressure was 14 mmHg, and no relevant astigmatism was notable in subjective refraction and on corneal topography (Figure 5). The patient reported a dramatic improvement in the quality of life, restarting activities she stopped doing, including riding a bicycle and writing (Figure 6).
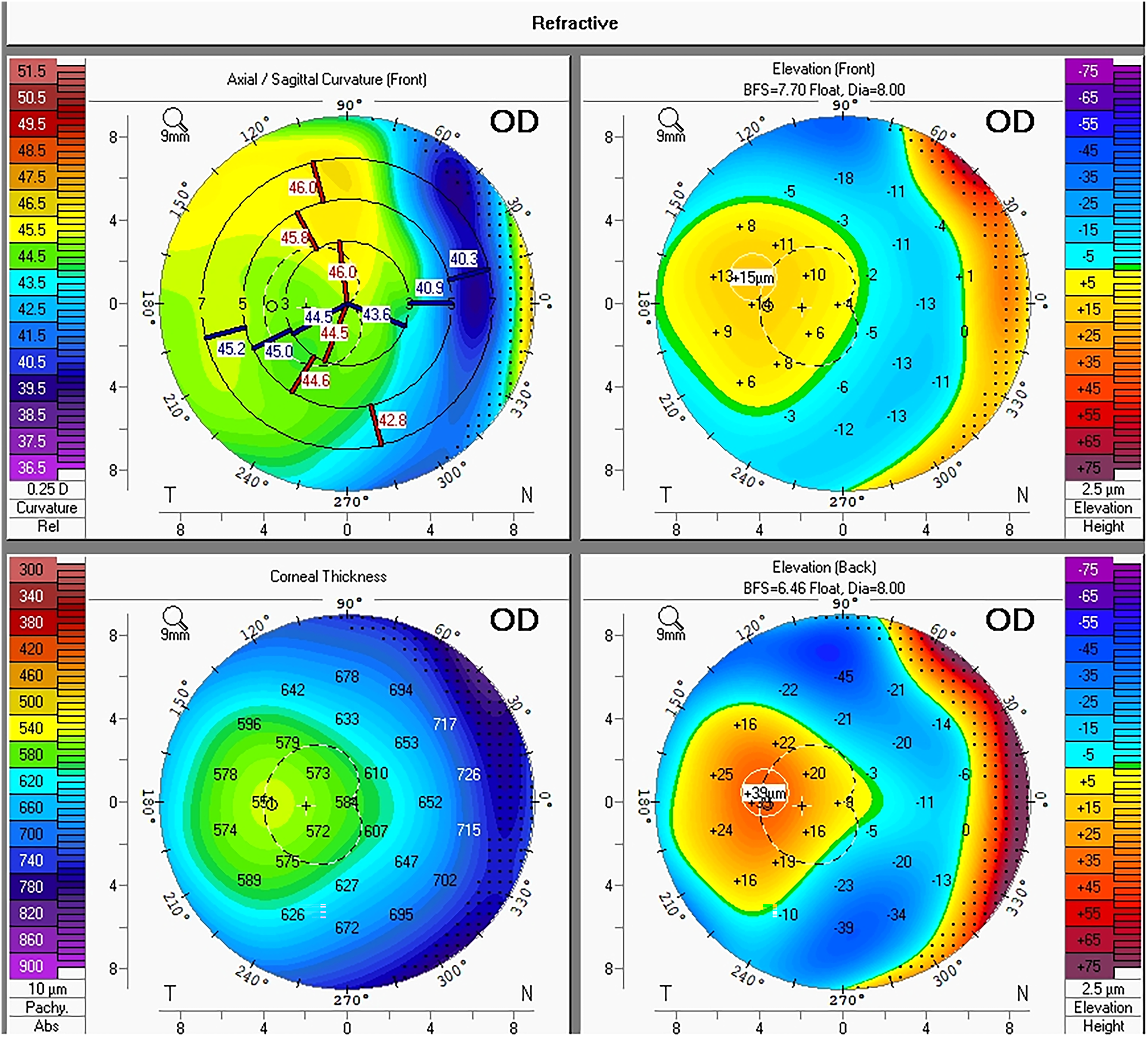
Corneal topography 4 months after the implant.
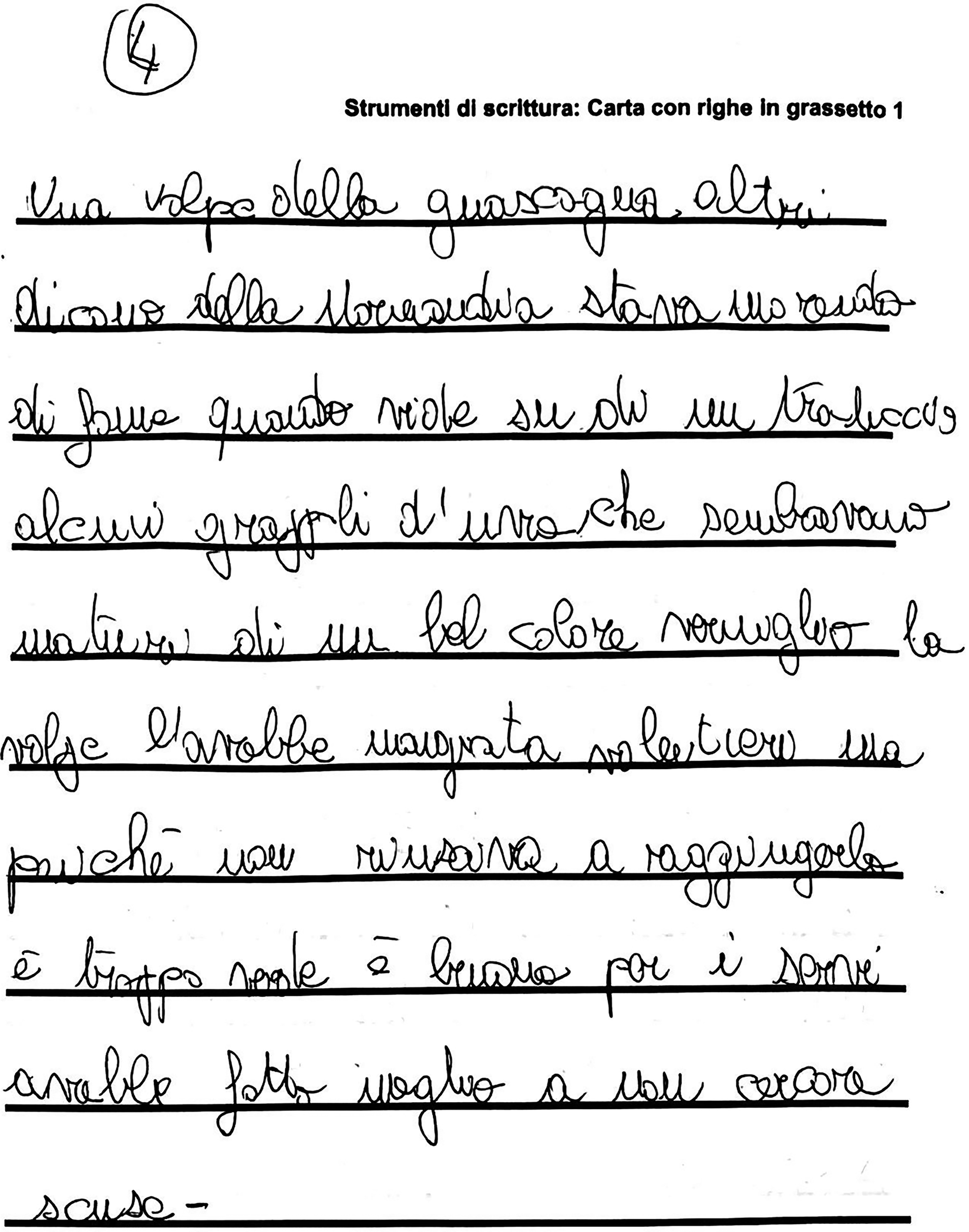
First page hand written by the patient after years.
Discussion
The new SING IMT shows promising characteristics, however careful study of the procedure is necessary to ensure the best outcomes. Short-term safety and efficacy results with the new SING IMT are encouraging, 6 as well as in vitro recent assessment. 7
First of all, the cornea incision should not be performed on clear cornea in order to avoid high surgical induced astigmatism (SIA) which has been reported more than 10 Diopters in the IMT. 8 In fact, continuous suture is more indicated in order to induces less SIA. 9 On the other hand, if performed too scleral the incision limits surgical movements rising difficulty of cataract surgery with potential iris prolapse.
Secondly, we highlight the importance of performing a centered 6 mm continuous curvilinear capsulorhexis. If too small loops may be placed in the ciliary sulcus tilting the SING IMT.If too wide the implant can undergo dislocation from the capsular bag. Moreover it is important to perform careful and effective cortex aspiration since capsulotomy can only be done with a pars plana vitrectomy.
Another crucial surgical step is the telescope cartridge orientation during the delivery, we point up the importance of inserting the cartridge bevel at 50° with the iris plane in order to ensure proper placement of the haptics in the capsular bag. It is possible that one or more haptic wings fall outside the bag; in this case a surgical hook can be used to return it in the bag using gently pressure to the base area of the haptic and folding it in the bag. Moreover, the cartridge tip is not clearly visible, if the localization is too posterior the pressure of the injection may lead to a posterior capsular rupture or bag luxation.
Endothelial damage is a main surgical concern in this procedure, our surgical technique is oriented to prevent any type of trauma to avoid endothelium damage, for this reason we decide to use two type of OVD, dispersive in anterior chamber (AC) and cohesive in the bag. However, the IMT was reported to have an endothelial cell loss up to 25% per year, 8 this new device is designed to reduce impact on the endothelium, however there are no published data so far. In this respect, it is important to avoid anterior chamber inflammation since chronic iritis may empathize cellular loss, anti-inflammatory therapy should be carefully observed by the patient. Indeed persisting iritis was the most common adverse event observed in a 5 year follow up of patients with IMT. 8
One of the drawbacks is that after the implant, the posterior pole will not be visualizable with traditional fundoscopy, however, a partial visualization can be achieved in mydriasis looking though the haptics. Optical coherence tomography (OCT) has lower quality but is capable of detecting retinal layers with acceptable quality.
Patient selection in this cases remains crucial, the patient will lose stereopsis and needs to be trained with dedicated session to learn how to properly use the implant.
Conclusion
We describe for the first time the surgical procedure of SING IMT implant. The new preloaded system along with a smaller incision and a re-designed telescope carry a significant improvement in terms of surgical complexity and iatrogenic damage.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.