
Abstract
Purpose
To compare the modified Yamane (MY) technique with the modified double-flange (MDF) technique in the management of subluxated single-piece foldable intraocular lenses (IOLs).
Methods
This retrospective study was conducted on 29 eyes (group MY:17 eyes, group MDF:12 eyes). In both techniques, the subluxated IOLs were moved to the anterior chamber, and anterior vitrectomy was performed. In group MY, the IOL was extracted using an approach similar to the “twist-and-out” technique without enlarging the main incision.The surgery was performed by creating a scleral tunnel 2.5 mm posterior to the limbus using a 26-gauge injector.In group MDF,a 6.0 polypropylene suture was passed through the widest part of the haptic near the optical portion using a 27-gauge injector guide. Visual, refractive results and complications of the two groups were compared.
Results
Both groups exhibited significant improvement in corrected distance visual acuity.No differences were observed between the groups in terms of spherical refraction, spherical equivalent, surgical time, or intraocular pressure values (p > 0.05 for all). Cylindrical refraction was −1.21 ± 0.14 D in group MY and −1.76 ± 0.25 D in group MDF(p = 0.03).The pseudophacodonesis score was 0.45 ± 0.15 in group MY compared to 1.21 ± 0.55 in group MDF (p < 0.001).Central macular thickness was similar between the two groups preoperatively, while at 6 months postoperatively, it measured 251 ± 15 μm in group MY and 274 ± 18 μm in group MDF (p = 0.19 and p = 0.01).
Conclusion
To our knowledge, this study is the first to compare the MY and MDF techniques for subluxated IOLs. Both techniques showed similar efficacy and safety. However, group MY demonstrated better and more stable IOL centration.
Keywords
Introduction
Intraocular lens (IOL) dislocations are significant complications of cataract surgery that can occur in the early or late postoperative period, seriously affecting vision.1,2 Although the incidence of IOL decentration varies, a study with a 10-year follow-up reported that the rate of IOL dislocations requiring surgical intervention was 0.6% after cataract surgery.1,3 Considering that cataract surgery is the most commonly performed surgery worldwide and its frequency continues to increase, this incidence cannot be underestimated.
The primary cause of IOL subluxated is known to be inadequate support from the capsular bag-zonular complex. 4 Weakness in this complex can result from pseudoexfoliation, myopia, disruption of anterior and/or posterior capsular integrity during cataract surgery, a history of multiple ocular surgeries, trauma, or systemic diseases.4,5
Managing subluxated IOLs can significantly impact visual acuity and quality; therefore, it is an area of interest for all ophthalmologists.5,6 Consequently, various techniques have been developed and implemented by both anterior and posterior segment surgeons.7–9 The intrascleral fixation of haptics using a 30-gauge injector, as described by Yamane et al., has gained widespread acceptance and popularity. 7 Meanwhile, the technique introduced by Canabrava et al., which secures capsular tension rings or segments to the sclera using 6.0 or 5.0 polypropylene, and the double-flange technique applied by Samir et al. for single-piece foldable lenses in aphakic cases, have also been described in the literature.8,9 However, the lack of studies evaluating the efficacy and safety of the double-flange technique for single-piece subluxated IOLs further underscores the importance of this topic.
This study was designed based on the hypothesis that there may be differences in efficacy and safety between the modified Yamane (MY) technique and the modified double-flange (MDF) technique in managing subluxated single-piece foldable IOLs. It aimed to compare refractive outcomes, visual acuity, intraoperative and postoperative complications between the two techniques. The results will highlight the advantages and disadvantages of each technique.
Materials and methods
Ethical process
This retrospective study was conducted using data retrieved from patient records. Prior to commencing the study, necessary approval was obtained from the Ethics Committee of Yozgat Bozok University (approval number: 2025-GOKAEK-253_310). All procedures adhered to the principles of the Declaration of Helsinki.
Design and subject
The study included 29 eyes of 29 patients who presented to the Ophthalmology Clinic of Yozgat City Hospital between June 2022 and December 2024 due to subluxation of a single-piece foldable IOL and underwent surgical intervention. All patients had undergone cataract surgery in different centres and were referred to our clinic because of IOL subluxation. The choice of surgical technique was random. Patients treated with the MY technique were classified as group MY (n = 17), and those treated with the MDF technique were classified as group MDF (n = 12). Comprehensive ophthalmologic examinations were conducted preoperatively, on postoperative day 1, and at postoperative week 1, month 1, and month 6.
Clinical evaluation
These examinations included measurements of spherical, cylindrical, and spherical equivalent refractive values. Uncorrected and corrected distance visual acuity (UDVA and CDVA) were measured using the Snellen chart and converted to the logarithm of the minimum angle of resolution (logMAR) for statistical analysis. Intraocular pressure (IOP) was measured using an air-puff tonometer. Detailed evaluations of anterior segment structures were performed via biomicroscopy, and dilated fundus examinations were conducted after administering cycloplegic drops. Preoperative axial lengths and IOL power were calculated using the IOLMaster 500 (Jena, Germany). For group MY, the Sanders-Retzlaff-Kraff theoretical formula was used to calculate IOL power, targeting a refractive aim of −0.50 D for emmetropia. Intraoperative complications such as haptic damage and postoperative complications observed at six months, including IOL decentration, pseudophacodonesis, increased IOP, cystoid macular edema (CME), retinal detachment, hypotony, flange-related conjunctival erosion, vitreous hemorrhage, epiretinal membrane, and pseudophakic bullous keratopathy, were evaluated. Pseudophacodonesis was assessed by instructing the patient to look rapidly upwards, followed by holding the gaze for 5 s and then quickly shifting to a downward gaze (1). This evaluation was undertaken by two independent researchers. The score was accepted as 0 if there was no movement in the optical and haptic components of the IOL and they remained fixed in both directions. If there was even a minimal movement between the two views in the IOL, it was accepted as 1 score. The score was accepted as 2 if the components of the IOL were noticeable even in the primary position but felt more when looking up or down. The score was determined as 3 for IOL movement that was clearly noticeable in both primary position and up-down gaze. Retinal and optic disc pathologies were examined using optical coherence tomography (Cirrus OCT, Carl Zeiss Meditec). Central macular thickness (CMT) was measured based on the vertical section passing through the fovea. Exclusion criteria were irregular follow-up, preoperative retinal detachment, vitreous hemorrhage, epiretinal membrane requiring retinal surgery, preoperative corneal opacity, pregnancy, a history of ocular surgery other than cataract surgery, and age < 18 years. The cases included in the study consisted of cases with single-piece IOL subluxation.
Surgical procedures
All surgeries were performed by the same surgeon (M.I.) under retrobulbar anesthesia. The MY technique was executed as follows (Supplementary video 1 and Figure 1): Nasal and temporal corneal side ports were made, and dispersive viscoelastic material was applied to protect the corneal endothelium (Figure 1a). The subluxated IOL was moved into the anterior chamber with the aid of a spatula (Figure 1b). A 2.4-mm superior corneal main incision was created. One haptic of the subluxated single-piece foldable IOL was removed through the main incision (Figure 1c). The IOL was grasped from the optic portion, folded, and removed without enlarging the incision (Figure 1d). Triamcinolone was applied to the anterior chamber to confirm the absence of vitreous. Anterior vitrectomy and irrigation probes were introduced through the side ports, and vitreous cleanup was performed (Figure 1e). An additional inferior corneal side port was made, and an anterior chamber maintainer was inserted (Figure 1f). The corneolimbal junction was marked at the 3 and 9 o’clock positions. Additional markings were placed 2.5 mm posterior to the limbus on both quadrants. From these points, secondary markings were made 2 mm away in the vertical plane, corresponding to the haptic positions. A three-piece IOL (Sensar AR40e, AMO) was loaded into a cartridge and injector system. The 26-gauge needle used for the first haptic was prepared to mimic a “7-shape” by bending its medial ¾ portion, while the needle for the second haptic was bent into an “L-shape.” For the first haptic, the 26-gauge needle was inserted at the marked position to create a scleral tunnel and directed toward the vitreous cavity (Figure 1g). The three-piece IOL was inserted into the anterior chamber via the main incision (Figure 1h). The leading haptic was guided toward the tip of the injector, placed into its lumen, and checked using forceps. The haptic-injector complex was then exteriorized to the conjunctival surface along the same plane (Figure 1i). The exposed haptic was grasped, and its tip was melted using handheld cautery to create a flange (Figure 1j). The haptic remaining outside the anterior chamber was reintroduced into the anterior chamber with the aid of forceps (Figure 1k). For the second haptic, the prepared injector was inserted at the designated points, directed toward the vitreous cavity (Figure 1l). The second haptic, which had been positioned in the anterior chamber, was guided into the injector lumen through a side port using forceps (Figure 1m). The assembled haptic was exteriorized through the scleral tunnel to the conjunctival surface, where a flange was created at its tip using handheld cautery (Figure 1n). Both flanges were subsequently positioned within the scleral tunnels beneath the conjunctiva. After removing the anterior chamber maintainer, the anterior chamber was irrigated and aspirated for cleansing (Figure 1o). The corneal incisions were sealed using stromal hydration, and cefuroxime was administered into the anterior chamber to conclude the procedure (Figure 1p).
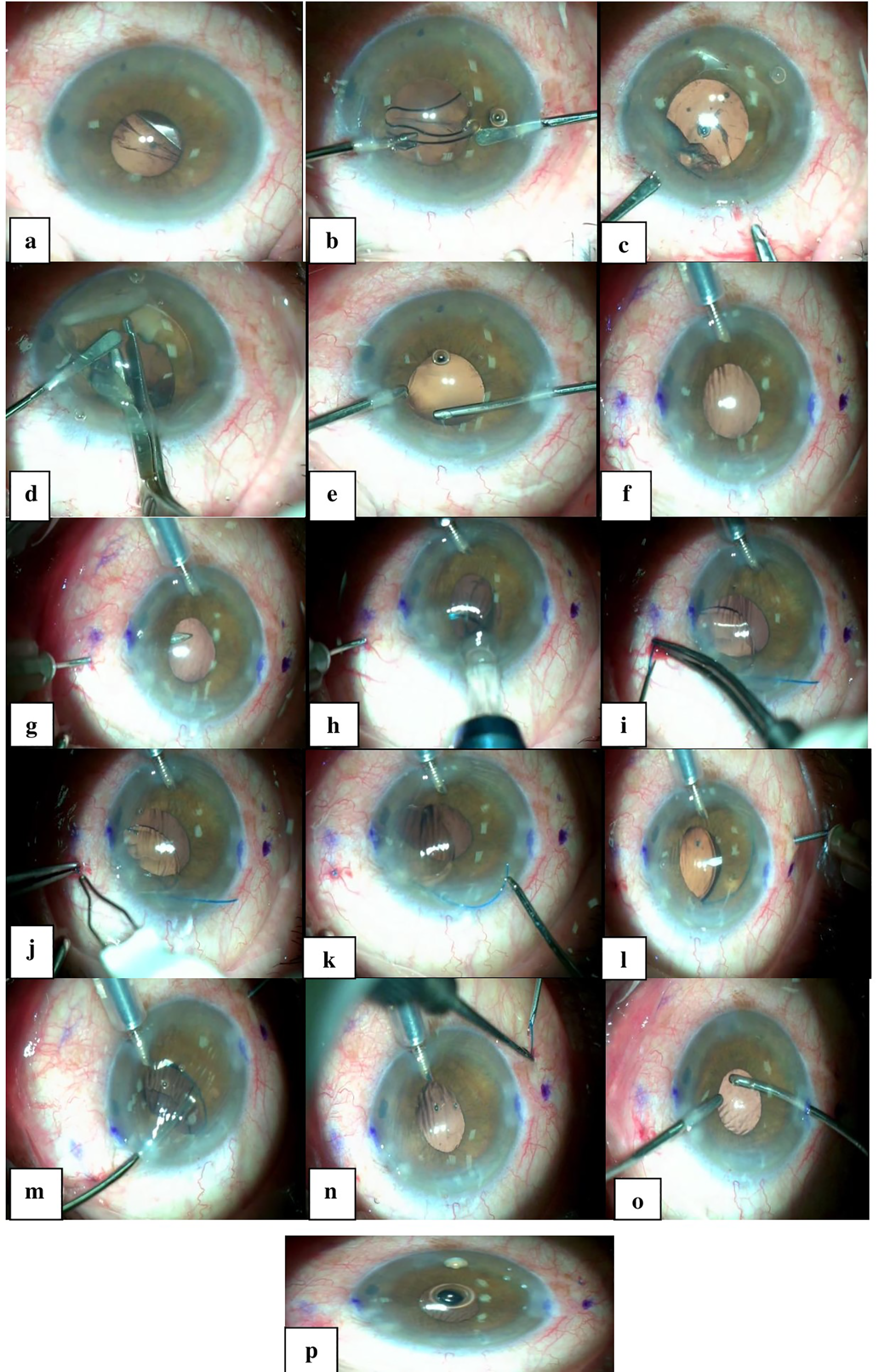
Extraction of a dislocated single-piece foldable intraocular lenses + all steps of modified Yamane surgery.
For the MDF technique, the following steps were performed (Figure 2 and Supplementary video 2) : Side ports were created at the nasal and temporal quadrants of the cornea. The corneal endothelium was protected with dispersive viscoelastic material (Figure 1a). A foldable subluxated IOL was moved into the anterior chamber (Figure 1b). Vitreous was examined under triamcinolone guidance, and anterior vitrectomy was performed through the side ports (Figure 1c, d and e). Following sufficient vitreous cleanup, a 2.4-mm main incision was created in the superior corneal quadrant. Through this incision, the first haptic was externalized, and the widest portion of the haptic (closest to the optic) was carefully guided through the tip of a 27-gauge injector (Figure 1f). A 6-0 polypropylene suture was threaded through the injector's tip and secured by melting one end with handheld cautery to form a flange (Figure 1g and h). This procedure was repeated for the second haptic (Figure 1i and j). Markings were placed at the inferior and superior quadrants to ensure a 180-degree alignment (Figure 1k). Using the 11 and 5 o’clock positions as reference points, a primary point was marked 2.5 mm in the vertical plane from the corneolimbal junction. A secondary point was marked 2 mm posterior to the first point in the horizontal plane to ensure an elongated scleral tunnel (Figure 1l). The haptic-polypropylene complex was introduced into the anterior chamber. Guided by a 26-gauge injector, the marked points were used to create scleral tunnels, and the vitreous cavity was accessed (Figure 1m). The 6-0 polypropylene sutures were inserted into the injector lumen and exteriorized through the scleral tunnels at their designated positions (Figure 1n). This process was repeated for the other quadrant (Figure 1o). Both ends of the polypropylene sutures were trimmed to a length of 1 mm and flanged using handheld cautery (Figure 1p and r). Viscoelastic material was removed through irrigation and aspiration via the side ports. The surgical wounds were sealed using stromal hydration, and cefuroxime was instilled into the anterior chamber to conclude the surgery (Figure 1s). Postoperatively, both groups received topical moxifloxacin four times daily for one week and topical corticosteroids four times daily for one month.
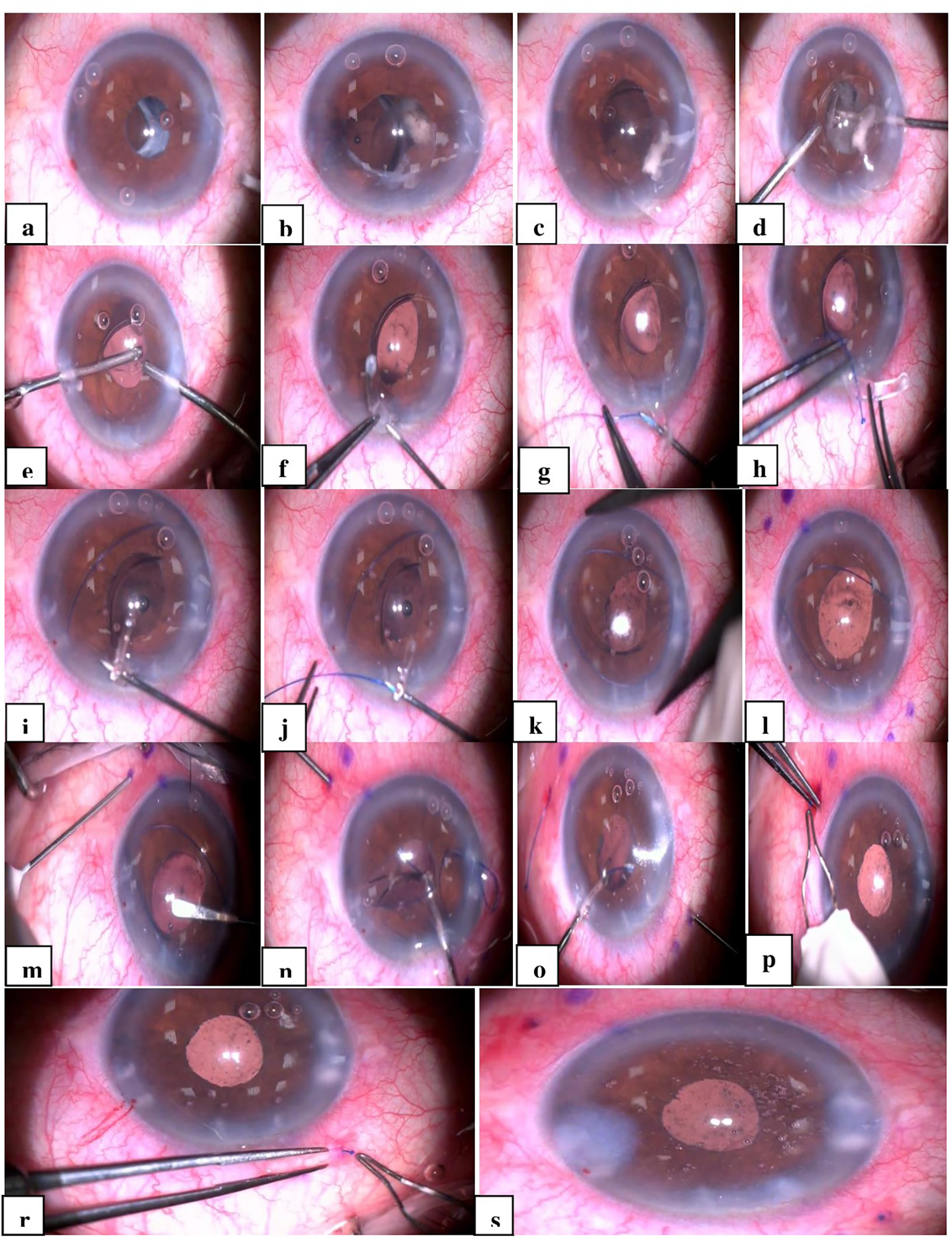
All steps of the modified double flange technique.
Statistical analysis
Data were analyzed using the Statistical Package for the Social Sciences (SPSS) version 22.0 (IBM, USA). Quantitative variables were expressed as mean ± standard deviation values. The normality of the data distribution was assessed using the Shapiro-Wilk test and histograms. The chi-square test, independent-samples t-test, and Mann-Whitney U test were used for intergroup comparisons. A p-value of <0.05 was considered statistically significant.
Results
This retrospective study was conducted on 29 eyes of 29 patients. The demographic data and preoperative parameters of the groups are presented in Table 1. No significant differences were found between the groups in terms of age, gender, laterality of the operated eye, preoperative axial length, visual acuity, intraocular pressure, or CMT (p > 0.05 for all). In the current study, pseudoexfoliation was observed in 13 (45%) of the 29 cases, and a history of blunt trauma was present in five (17%) cases. In addition, when IOL designs were analysed, all patients had monofocal IOLs.
Preoperative parameters and demographic data.
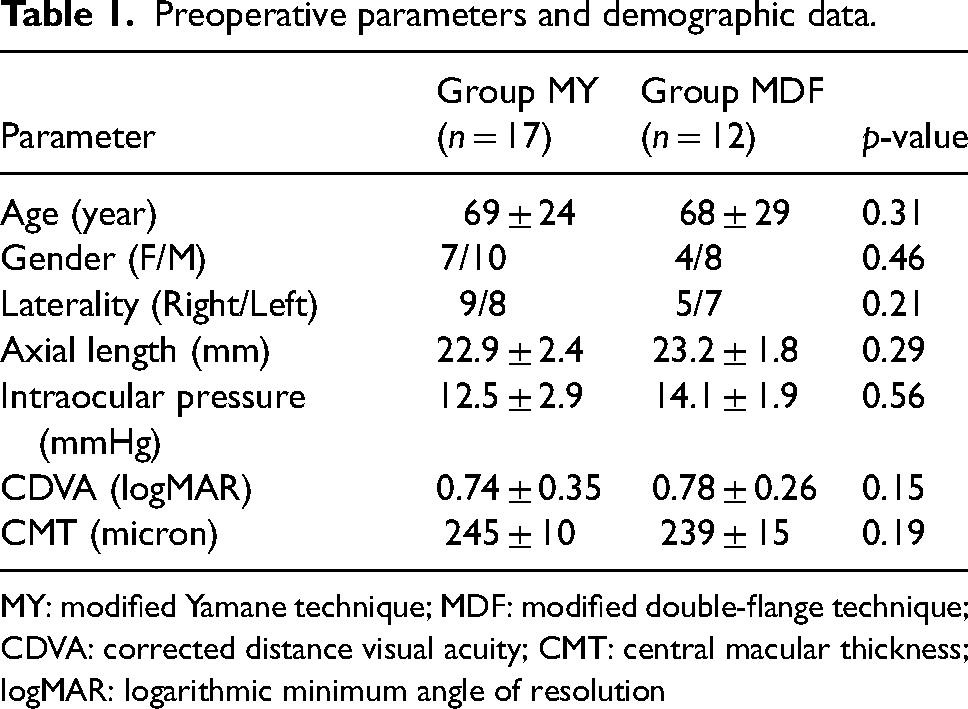
MY: modified Yamane technique; MDF: modified double-flange technique; CDVA: corrected distance visual acuity; CMT: central macular thickness; logMAR: logarithmic minimum angle of resolution
The refractive values, visual acuity, pseudophacodonesis scores, intraocular pressure measurements, surgical time, and CMT at the postoperative six-month visit are presented in Table 2. No differences were found between the groups regarding corrected distance visual acuity, spherical refraction, spherical equivalent, intraocular pressure, surgical time, or CMT at the six-month visit (p > 0.05 for all). No significant difference was found between the two groups in terms of corneal cylinder values (p > 0.05). However, the cylindrical refraction value was −1.21 ± 0.14 D in group MY and −1.76 ± 0.25 D in group MDF, indicating a statistically significant difference (p = 0.03). The pseudophacodonesis score was 0.45 ± 0.15 in group MY and 1.21 ± 0.55 in group MDF, significantly higher in group MDF (p < 0.001).
Comparison of postoperative six-month findings between the groups.
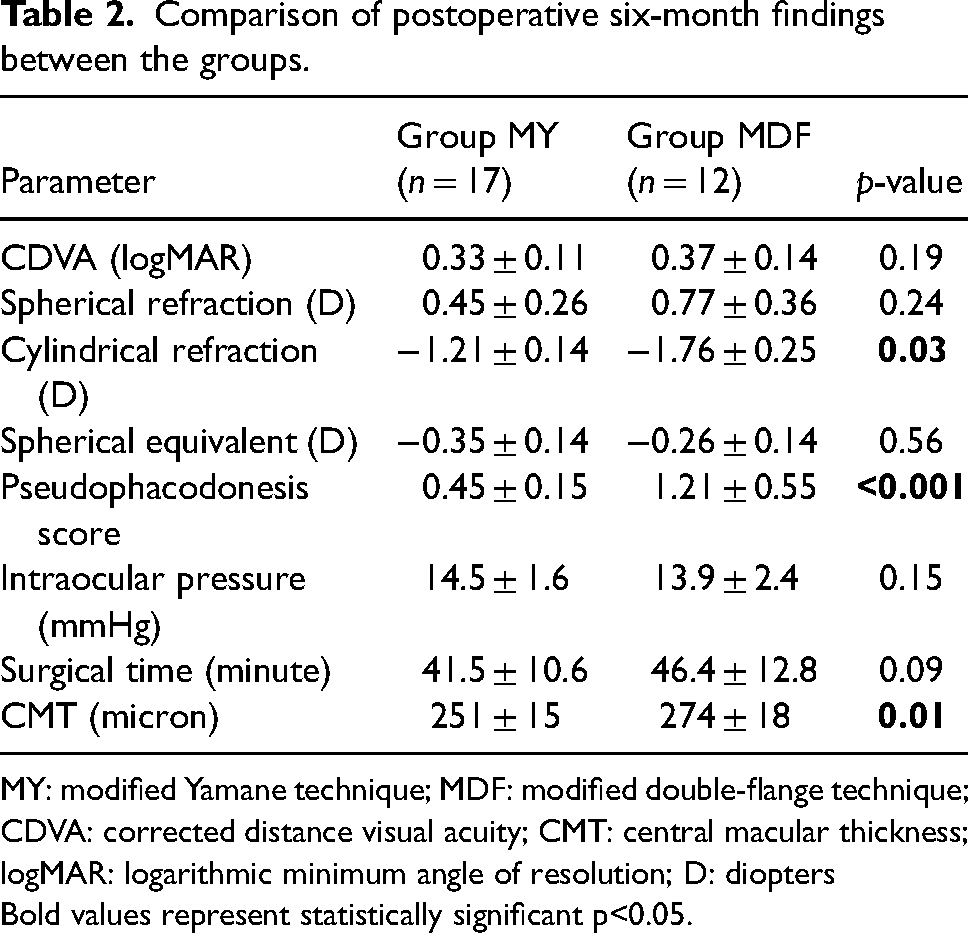
MY: modified Yamane technique; MDF: modified double-flange technique; CDVA: corrected distance visual acuity; CMT: central macular thickness; logMAR: logarithmic minimum angle of resolution; D: diopters
Bold values represent statistically significant p<0.05.
The distribution of intraoperative and postoperative complications is presented in Table 3. CME was observed in one patient (6%) in group MY and two patients (16%) in Group MDF. In group MY, one case (6%) of intraocular pressure increase and one case (6%) of pseudophakic bullous keratopathy were documented. In group MDF, one case (8%) of IOL decentration was identified. No cases of vitreous hemorrhage, complications related to haptic-propylene flanges, endophthalmitis, epiretinal membrane, or retinal detachment were observed in either group.
Evaluation of intraoperative and postoperative complications.
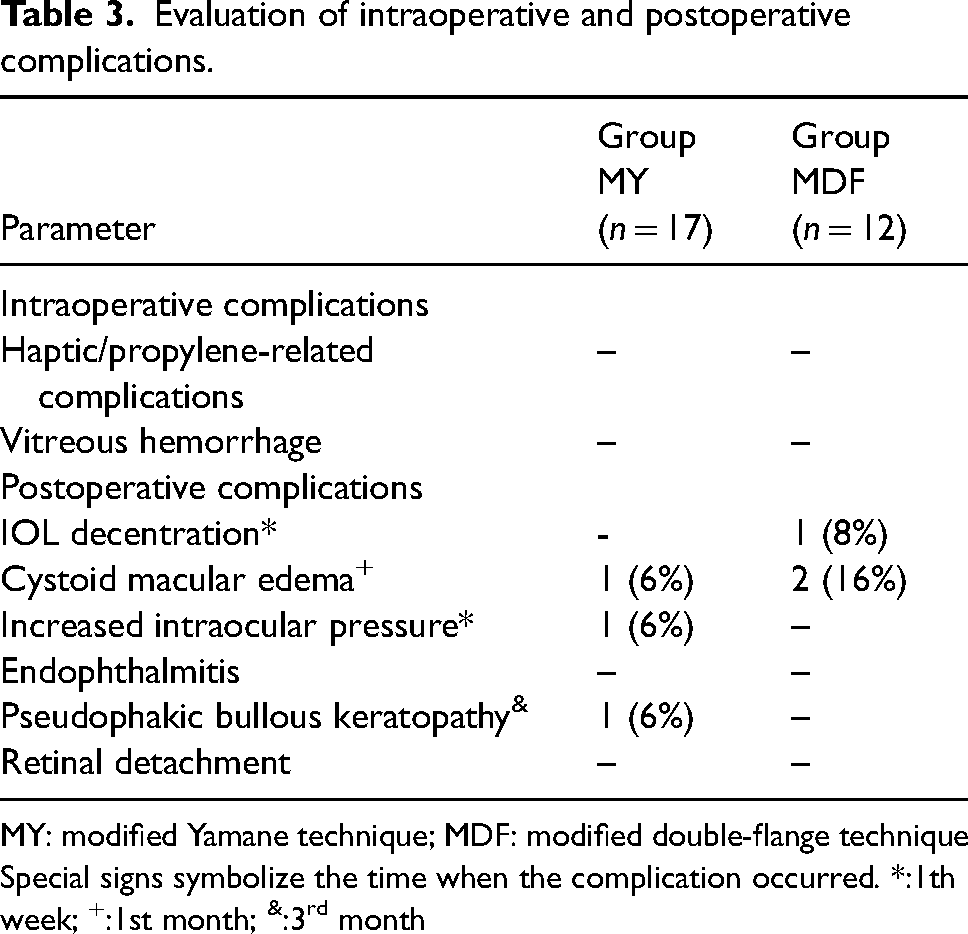
MY: modified Yamane technique; MDF: modified double-flange technique
Special signs symbolize the time when the complication occurred. *:1th week; +:1st month; &:3rd month
When examined in terms of efficacy; although no significant difference was observed in terms of visual acuity, spherical refraction and spherical equivalent values, it was observed that the group MY was more effective in terms of cylindrical refraction value. When evaluated in terms of safety; although different complications were observed in the two groups, there was no significant difference.
All cases of CME resolved with topical non-steroidal anti-inflammatory treatment, with resolution achieved by an average of six weeks (earliest at four weeks, latest at eight weeks). The case of increased IOP in group MY was managed with topical brimonidine. In the pseudophakic bullous keratopathy case in group MY, corneal decompensation was observed after the second postoperative month, and endothelial keratoplasty was recommended, but the patient declined further surgical intervention. The IOL decentration case in group MDF was resolved through reoperation, where the polypropylene ends were shortened symmetrically, and flanges were created using an electrocautery device and repositioned within the scleral tunnel.
Discussion
This study compared the refractive outcomes, visual acuity, and complication profiles of the MY technique and the MDF technique in cases of subluxated one-piece foldable IOLs. The findings demonstrated that: (1) while both groups exhibited significant improvements in CDVA and BCVA, group MY had significantly lower cylindrical refractive values compared to group MDF, despite no differences in spherical refractive errors or spherical equivalents between the groups; (2) the pseudophacodonesis score was significantly higher in group MDF; and (3) regarding complications, one case each of CME, pseudophakic bullous keratopathy, and increased IOP was observed in group MY, whereas group MDF experienced one case of IOL decentration and two cases of CME.
The Yamane technique has garnered considerable interest since its introduction and is widely utilized by many surgeons.7,10 While it can be applied in aphakic cases, it is also considered a safe approach for the management of one-piece IOL subluxations. 11 On the other hand, although the MDF technique was first described by Canabrava et al., no studies in the literature have demonstrated its applicability specifically in cases of subluxated one-piece foldable IOLs. 8 Nevertheless, its efficacy and safety in aphakic cases have been reported by various researchers.9,12 One notable finding of our study is that group MY demonstrated a postoperative six-month cylindrical refractive value of −1.21 ± 0.14 D compared to −1.76 ± 0.25 D in group MDF, as well as a significantly higher pseudophacodonesis score in the latter. Samir et al. reported significant improvements in postoperative visual acuity in 17 aphakic cases treated with the MDF technique but did not provide data on refractive outcomes. 9 In another study involving 27 aphakic cases, Boz et al. reported postoperative lenticular astigmatism of 1.61 ± 0.75 D and a pseudophacodonesis score of 1.56 ± 1.10. The authors also compared the MY and MDF techniques, concluding that the MY technique was superior in terms of cylindrical refraction and pseudophacodonesis. 12
With advancing technology, patients’ expectations following cataract surgery have steadily risen. Even in cases with complicated cataract histories requiring secondary surgical interventions, as in this study, achieving optimal postoperative refractive outcomes should be prioritized. Success in minimizing postoperative ocular astigmatism depends on multiple factors, such as corneal irregularity, IOL tilt, and decentration. Proper centration of the IOL is associated with symmetrical placement of the haptics. Although no studies have objectively evaluated IOL positioning in eyes treated with the MDF technique, Boz et al. have conducted subjective evaluations, as noted earlier. 12 Studies comparing the MY technique with suture-based scleral fixation have reported IOL tilt rates of 0–1% in MY groups compared to 0–10.4% in suture-based groups.13–16
Pseudophacodonesis, resulting from chronic mechanical effects, may lead to pigment dispersion from the iris. In cases where the posterior capsule is not intact, the likelihood of retina-vitreous involvement increases due to the elevated levels of various inflammatory cytokine groups in such discharges. 17 One of the most commonly expected complications associated with this involvement is CME. 18 In this context, the higher pseudophacodonesis score observed in group MDF in our study may explain the higher incidence of CME and greater CMT in this group.
Boz et al. also reported serious retinal complications requiring secondary surgery, including three cases of retinal detachment and two cases of vitreous hemorrhage, in their MY group. However, these complications were not observed in the MDF group. 12 Similarly, Samir et al. documented only one case of IOL decentration and no retinal complications in eyes treated with the MDF technique. 9 It is worth emphasizing that, unlike our study, these two studies involved aphakic cases.9,12
While the MY technique is popular, it presents intraoperative challenges. For instance, inserting the trailing haptic into the injector lumen is considered the most challenging step by many surgeons. 7 These challenges may lead to serious intraoperative complications, such as haptic breakage, haptic escape from the scleral tunnel, or IOL drop into the vitreous cavity. In contrast, the MDF technique involves fewer technically demanding steps than the MY technique, reducing the likelihood of such complications. However, the MY technique requires explantation of the subluxated IOL in cases involving one-piece foldable lenses. Despite various techniques being described for IOL explantation, 19 this procedure may lead to significant complications. Goemaere et al. evaluated the complications of IOL explantation in 492 patients and reported vitreous prolapse in 16%, elevated intraocular pressure in 6.5%, cystoid macular edema in 2%, and retinal detachment in 1.5% of cases. 20 In our study, pseudophakic bullous keratopathy was observed in one case in the IOL explantation group. This complication significantly affects vision and necessitates secondary surgery.
Unfortunately, we do not have quantitative information about endothelial count because we do not have a device to perform endothelial count in our clinic. However, we evaluate the layers of the cornea in detail in all preoperative biomicroscopic examinations. Our country is among the developing countries and unfortunately, we face different difficulties in terms of getting a new device for hospital management. Although we have emphasised the importance of detailed preoperative and postoperative evaluation in such special cases many times, unfortunately we have not made any progress in this regard. We have emphasised this important issue in the limitations of this study.
One of the strengths of this study is that it is the first to demonstrate the applicability of the MDF technique in subluxated one-piece IOL cases and the first to present comparative data with the MY technique. In addition, all surgeries were performed by a single surgeon. However, the study also has several limitations. First, the small sample size and retrospective design are notable constraints. Second, corneal endothelial cell counts, which could provide a more detailed evaluation of corneal impact, were not assessed. On the other hand, it can influence the visual results and the rate of complications, such as corneal decompensation. Third, pseudophacodonesis/IOL centration was not directly measured using anterior segment optical coherence tomography. Nevertheless, this limitation can be partially addressed by noting that subjective assessments of postoperative lenticular astigmatism and pseudophacodonesis provide indirect information about IOL centration. Lastly, it should be noted that preoperative and postoperative corneal astigmatism values were similar between the groups.
In conclusion, both the MDF and MY techniques led to significant improvements in visual acuity, with better and more stable IOL centration observed in group MY. Although the surgical times of the two techniques were similar, different complications were encountered. Further studies with larger cohorts and longer follow-up periods are needed to evaluate the anatomical and functional outcomes of these techniques.
Supplemental Material
Supplemental Material
Footnotes
Acknowledgments
None.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.