
Abstract
Purpose
To compare the efficacy of 15-s versus 30-s intraoperative applications of 0.02% mitomycin C (MMC) in preventing corneal haze after photorefractive keratectomy (PRK) for moderate myopia.
Methods
This prospective, paired-eye study enrolled 50 patients (100 eyes) with bilateral moderate myopia (−3.00 to −6.00 D). Each patient underwent bilateral wavefront-optimized PRK. One eye was randomized to receive
Results
The median age was 25.5 years (range, 18–53). Preoperative refractive errors were symmetrical between paired eyes (P > 0.05). Postoperative corneal haze was minimal and transient. Median haze scores were 0 at all timepoints beyond the 1-week visit. Haze severity decreased significantly over time in both groups (P < 0.01), with no statistically significant differences between the 15-s and 30-s groups at any follow-up visit (P ≥ 0.08). At 6 months, the median UDVA was 0.00 logMAR in both groups (P = 1.0).
Conclusions
A 15-s intraoperative application of 0.02% MMC
Introduction
Photorefractive keratectomy (PRK) is a well-established surface ablation procedure for correcting myopia. A principal challenge in its postoperative course is the potential development of subepithelial haze, a corneal opacity that results from aberrant wound healing. This process, triggered by epithelial and stromal ablation, involves keratocyte apoptosis, the proliferation of activated myofibroblasts, and the deposition of disorganized extracellular matrix, which scatters light and reduces visual quality.1,2
The prophylactic intraoperative application of mitomycin C (MMC) has significantly reduced the incidence of this complication. MMC, an alkylating antimetabolite, inhibits DNA synthesis, thereby suppressing the proliferation of fibroblasts and myofibroblasts.3,4 While its efficacy is well-established, the optimal application parameters remain a subject of ongoing refinement. Early protocols for high myopia corrections with broad-beam lasers employed exposure times of up to 2 min.
5
However, modern wavefront-optimized excimer lasers create smoother ablations with less stromal disruption, potentially reducing the
Recent studies have explored shorter MMC durations. Virasch et al. found a 12-s application to be as effective as longer times, 8 and Thornton et al. reported efficacy even with low concentrations. 9 Building on this evidence, we conducted a prospective, paired-eye study to directly compare the clinical efficacy of 15-s and 30-s applications of 0.02% MMC in preventing haze following modern wavefront-optimized PRK.
Methods
Study design and participants
This prospective, paired-eye study was conducted at a single tertiary care center following approval by the Institutional Review Board of Al-Azhar University,
Fifty patients (100 eyes) with bilateral moderate myopia (spherical equivalent, −3.00 to −6.00 diopters) were enrolled. Exclusion criteria included a history of prior ocular surgery, clinical or topographic evidence of corneal ectasia, any corneal dystrophy, active ocular surface disease, or systemic conditions known to impair wound healing (e.g., uncontrolled autoimmune disease). Patients with hyperopia, pure astigmatism, or those undergoing PRK enhancement were also excluded.
Surgical technique
All surgeries were performed by a single experienced surgeon (H.A.Z.). After administering topical anesthesia, the corneal epithelium was removed mechanically
This consistent laterality-based allocation (15 s to the right eye, 30 s to the left eye) was used to simplify the surgical procedure and postoperative analysis while maintaining the paired-eye controlled design. The cornea was then copiously irrigated with 20 mL of balanced salt solution, and a bandage contact lens was applied.
Postoperative regimen and follow-up
The postoperative medication regimen included topical moxifloxacin 0.5% until re-epithelialization was complete, and a tapering course of topical corticosteroids
Patients were examined at 1 week and 1, 3, and 6 months postoperatively. At each visit, a masked examiner
Statistical analysis
Statistical analysis was performed using SPSS version 26.0 (IBM Corp.). The Wilcoxon signed-rank test was used to compare paired data (haze scores and UDVA). The Friedman test evaluated changes in haze scores over time. A P value of < 0.05 was considered statistically significant.
Results
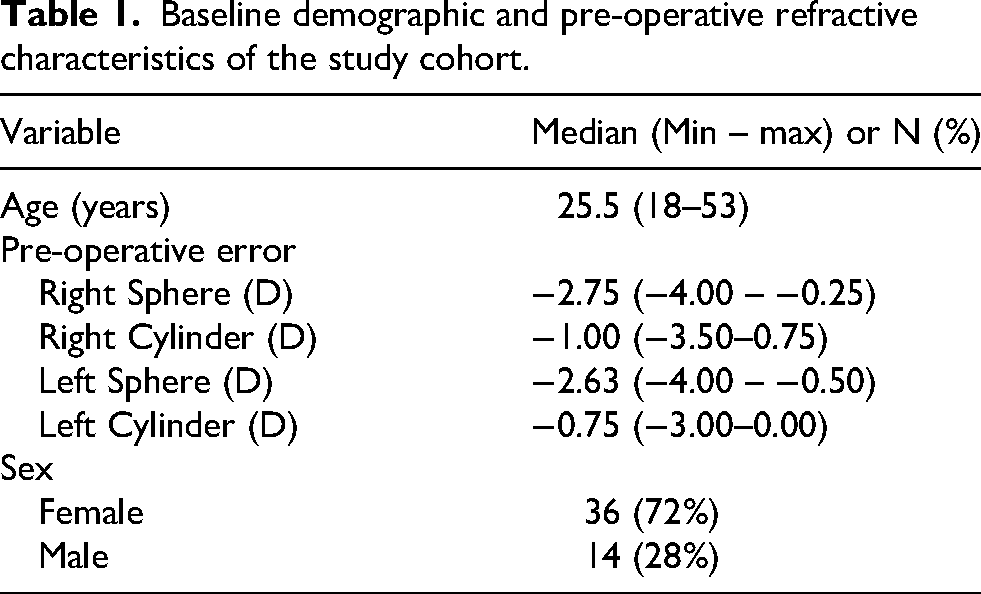
All 50 patients completed the 6-month follow-up. The cohort had a median age of 25.5 years (range, 18–53), and the majority of patients were female (72%, n = 36) Preoperative refractive errors were comparable between fellow eyes (Table 1).
Baseline demographic and pre-operative refractive characteristics of the study cohort.
Corneal haze was minimal and transient. At 1 week postoperatively, clinically significant haze (Fantes grade ≥1) was observed in 18% (9/50) of eyes in the 15-s group and 10% (5/50) in the 30-s group, with all cases ≤ grade 2. Median haze scores were 0 (range, 0–2) in the 15-s group and 0 (range, 0–1) in the 30-s group (P = 0.08). Haze severity decreased significantly over time in both groups (P < 0.01), with complete resolution (grade 0) in all eyes by the 3-month follow-up.
When analyzed as a binary endpoint (grade ≥1), the absolute risk difference at 1 week was 8% (95% CI: −6% to 22%), indicating no statistically or clinically significant difference between the two exposure durations. By 1 month, the incidence of clinically significant haze declined markedly, and no eyes demonstrated grade ≥1 haze from 3 months onward (Tables 2a, 2b, 3).
Comparison of pre-operative refractive errors, postoperative haze, and visual outcomes between 15-second MMC group and 30-second MMC group.
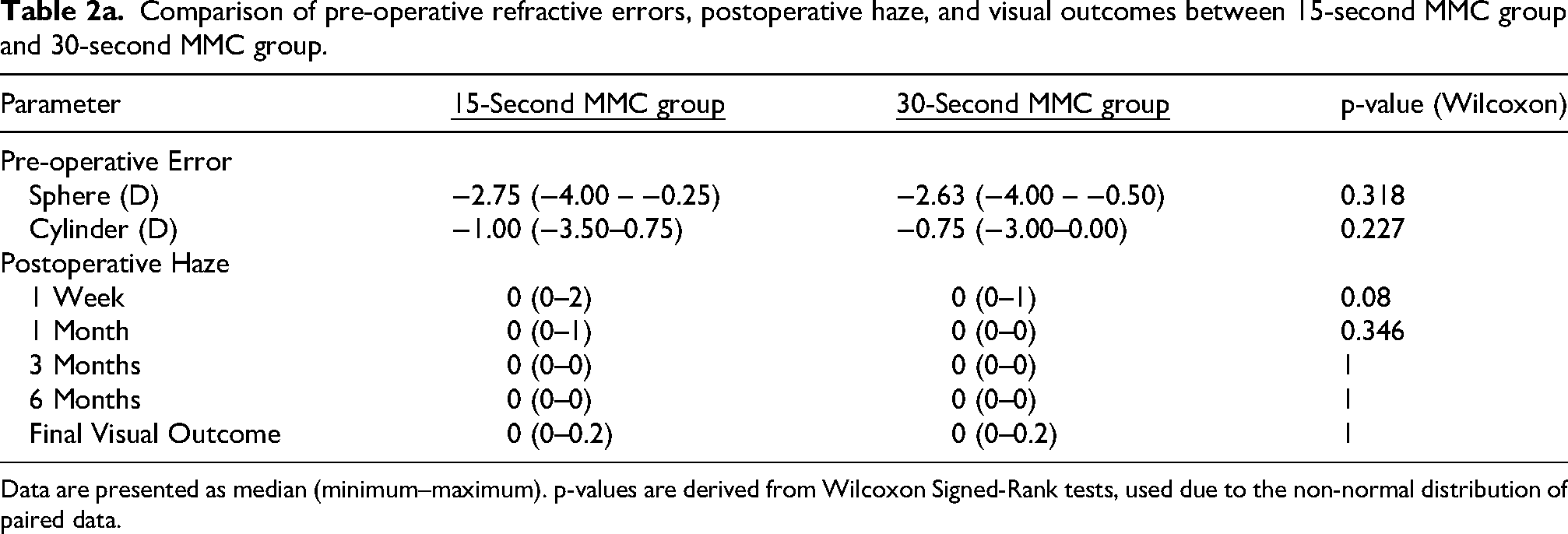
Data are presented as median (minimum–maximum). p-values are derived from Wilcoxon Signed-Rank tests, used due to the non-normal distribution of paired data.
Frequency distribution of corneal haze grades by eye and time.
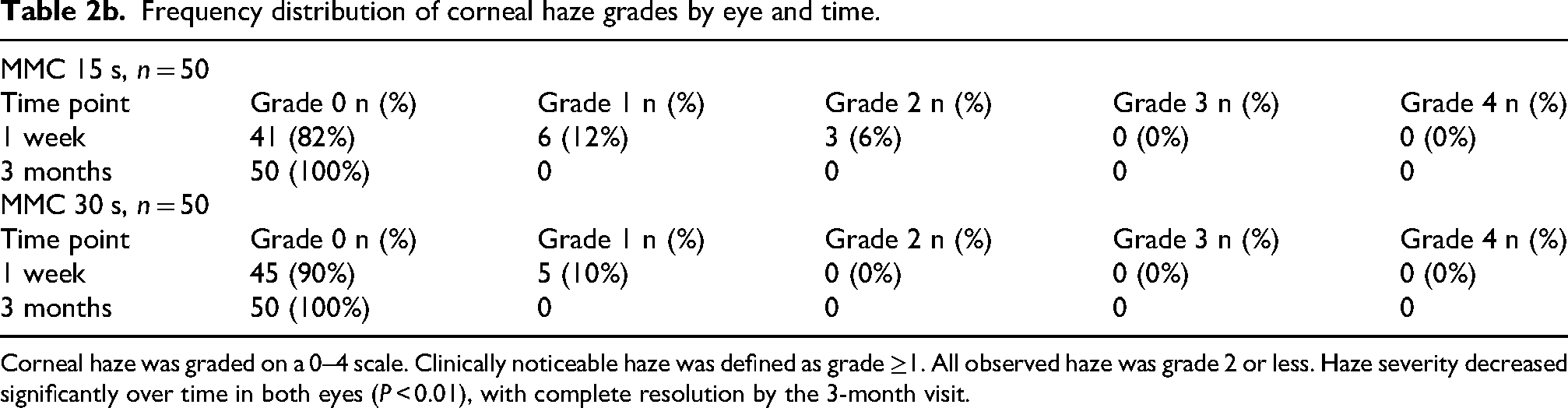
Corneal haze was graded on a 0–4 scale. Clinically noticeable haze was defined as grade ≥1. All observed haze was grade 2 or less. Haze severity decreased significantly over time in both eyes (P < 0.01), with complete resolution by the 3-month visit.
Temporal changes in postoperative corneal haze scores for 15-second MMC group and 30-second MMC group. Following Refractive Surgery.
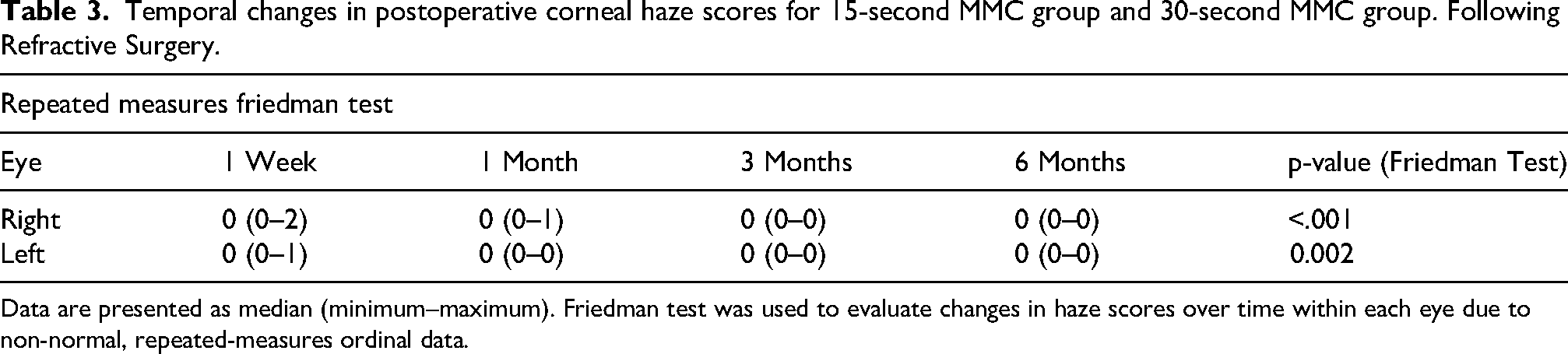
Data are presented as median (minimum–maximum). Friedman test was used to evaluate changes in haze scores over time within each eye due to non-normal, repeated-measures ordinal data.
Comparison of final visual outcomes between male and female patients following bilateral refractive surgery.
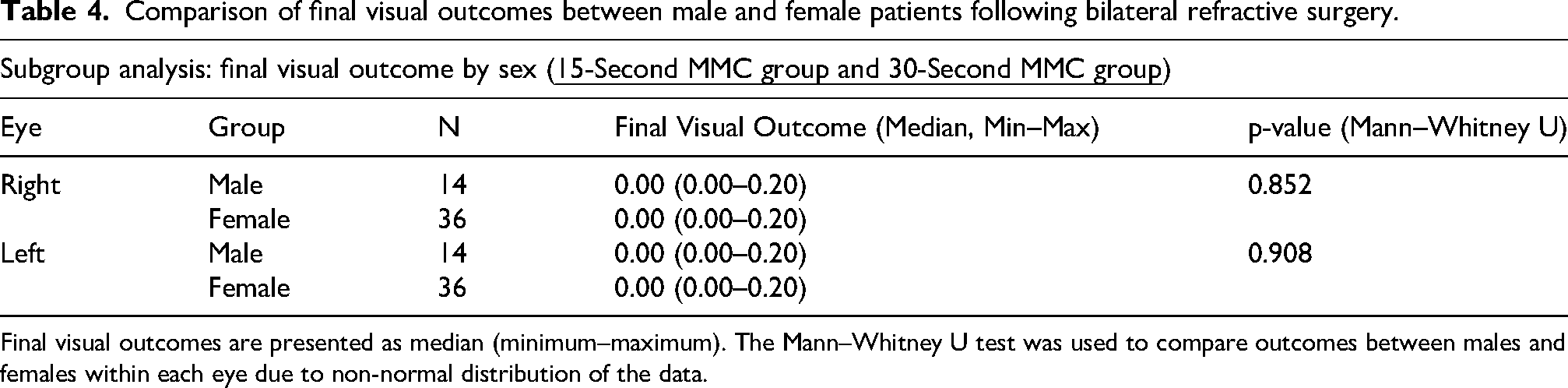
Final visual outcomes are presented as median (minimum–maximum). The Mann–Whitney U test was used to compare outcomes between males and females within each eye due to non-normal distribution of the data.
Refractive Outcomes and Safety: Postoperative refractive stability was excellent. The median postoperative spherical equivalent at 6 months was −0.12 D (interquartile range [IQR]: −0.38 to ±0.25) in the 15-s group and −0.09 D (IQR: −0.41 to ±0.19) in the 30-s group (P = 0.65). The median time to complete re-epithelialization was 4 days (range 3–5 days) in both groups, with no significant difference (P = 0.72). Epithelial healing averaged 3 days in both groups, with no delayed healing observed in either. No eye in either group developed a persistent epithelial defect, infection, visually significant regression (>0.50 D), or any other adverse event related to the MMC application.
Visual outcomes were excellent and comparable between groups. At 6 months, the median UDVA was 0.00 logMAR (20/20) in both groups (P = 1.0). (Table 4)Spearman's rank correlation demonstrated no significant associations between preoperative refractive error and final visual outcome. In the 15-s MMC group, neither sphere (ρ = −0.084, p = 0.562) nor cylinder (ρ = 0.188, p = 0.190) correlated with visual acuity. Comparable findings were observed in the 30-s group for sphere (ρ = −0.141, p = 0.328) and cylinder (ρ = −0.034, p = 0.817). (Table 5).
Correlation analysis between preoperative refractive errors and final visual outcomes following bilateral refractive surgery.
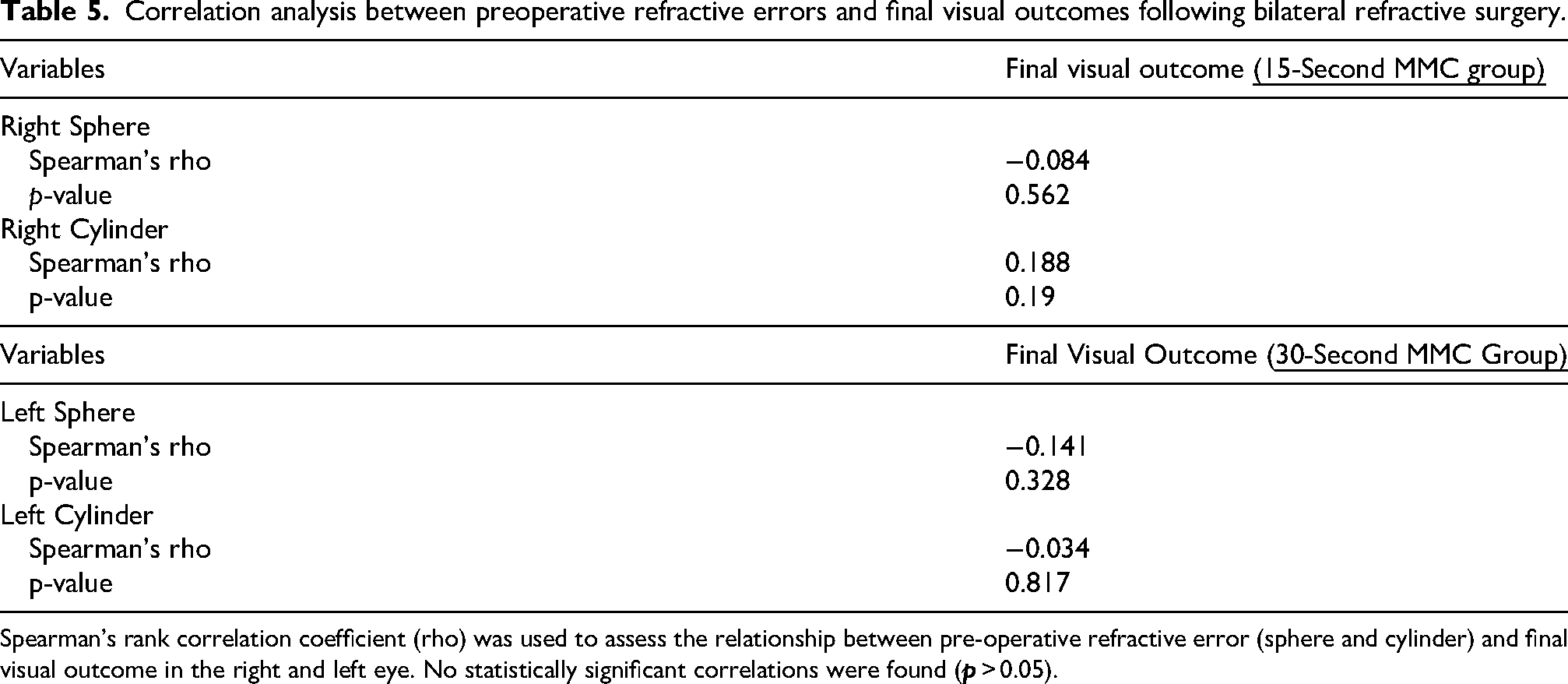
Spearman's rank correlation coefficient (rho) was used to assess the relationship between pre-operative refractive error (sphere and cylinder) and final visual outcome in the right and left eye. No statistically significant correlations were found (
Discussion
In this prospective, paired-eye study, no statistically significant differences in corneal haze scores or visual acuity were observed between a 15-s and a 30-s application of 0.02% MMC for preventing corneal haze and promoting excellent visual recovery after wavefront-optimized PRK for moderate myopia.The paired-eye design provided a robust internal control by minimizing inter-individual variability.
Corneal haze is a well-known complication of PRK, arising from a complex wound-healing response. The ablation of Bowman's layer and the anterior stroma triggers a cascade involving inflammation, keratocyte activation into myofibroblasts, and the deposition of disorganized collagen and extracellular matrix, leading to light scatter and opacity.1,11 Because this risk is positively correlated with the degree of myopic correction, we focused our study on a cohort with moderate myopia to control for this key variable. 12
The lack of correlation between preoperative refractive error and final visual acuity indicates that baseline sphere and cylinder do not influence visual outcomes following PRK with either MMC duration. These findings suggest both exposure times yield consistently effective rehabilitation across moderate myopic corrections, with no need to restrict patient selection based on pretreatment refractive status.Our findings support the growing consensus that shorter MMC exposure durations are adequate with modern laser technology. Early protocols, such as that of Carones et al., established the efficacy of a 2-min application for high myopia using conventional broad-beam systems. 5 Subsequent investigations have consistently supported shorter times. Virasch et al. reported that a 12-s application was as effective as longer durations, 8 and a recent systematic review concluded that shorter exposure times provide comparable haze prevention. 13 The equivalence we observed is likely multifactorial. Modern wavefront-optimized laser systems create smoother ablation profiles and induce less stromal disruption, thereby provoking a less aggressive wound-healing response. 6 Furthermore, MMC is a highly potent agent with rapid cellular uptake; its antiproliferative effect on keratocytes may achieve a critical threshold within the first 15 s of application. 4
In vitro and in vivo studies have documented dose- and time-dependent cytotoxic effects of MMC on keratocytes and corneal endothelial cells.14,15 Although our study did not measure endothelial cell density, adhering to the principle of using the lowest effective dose helps mitigate potential long-term risks, such as delayed stromal healing or endothelial compromise. By establishing non-inferiority for a 15-s exposure, our study provides an evidence-based rationale for enhancing procedural safety without sacrificing efficacy. Our results are consistent with Hofmeister et al., who found no difference in visual outcomes or endothelial cell density with different MMC application times, 16 and we observed no clinically significant delays in epithelial healing, a complication noted in some earlier studies. 17
The primary strengths of this study include its prospective design, paired-eye control, and masked outcome assessment. However, certain limitations must be acknowledged. The 6-month follow-up period, while sufficient to capture typical haze formation, may not detect very late-onset haze. Furthermore, our results are specific to patients with moderate myopia and may not be generalizable to those with high myopia or thinner corneas. A further limitation is the lack of endothelial cell count data. Future studies incorporating long-term endothelial cell counts and in vivo confocal microscopy to evaluate keratocyte density are warranted.
Conclusions
In patients with moderate myopia undergoing wavefront-optimized PRK, a 15-s intraoperative exposure to 0.02% MMC provides haze prevention and visual outcomes equivalent to a 30-s exposure.
Precis
In a prospective paired-eye study of 50 patients, a 15-s application of 0.05% mitomycin C was as effective as a 30-s application in preventing corneal haze and achieving excellent visual outcomes after photorefractive keratectomy for moderate myopia.
Footnotes
Acknowledgments
None
Ethical approval and informed consent
This study was approved by the Ethics Committee of the Faculty of Medicine, Al-Azhar University (Approval No. [insert number if applicable]).
Written informed consent was obtained from all participants prior to surgery in accordance with the Declaration of Helsinki.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.