
Abstract
Purpose
To analyze the surgical results of bilateral medial rectus recession (BMR) versus unilateral medial rectus recession and lateral rectus resection (RNR) in patients with non-alternating esotropia associated with similar visual acuity in both eyes.
Methods
Data of suitable patients operated between 2010 to 2023 were collected from their electronic records immediately before surgery and during follow-up until the last available visit. Surgical success was defined as deviation of 10 prism diopters (PD) or less.
Results
473 patients had strabismus surgery for esotropia correction during the study period and 26 (5.5%) of them met the study's inclusion criteria: 12 (46.2%) in the RNR group and 14 (53.8%) in the BMR group. Final angles of deviations after RNR (distance 2.1 ± 2.9PD and near 3.6 ± 3.7PD) were not different than after BMR (distance 1.4 ± 2.4PD and near 4.0 ± 4.5PD, p = 0.54 and p = 0.80 respectively). Additionally, a similar success rate was achieved after both types of surgeries (100% for RNR and 92.8% for BMR, p = 0.35).
Conclusion
Patients with non-alternating esotropia and equal vision in both eyes who express concerns about the necessity of strabismus surgery on their non-deviating eye can achieve comparable outcomes following RNR performed exclusively in the deviating eye.
Introduction
Esotropia can manifest as alternating or non-alternating based on patient's fixation behavior. The primary cause of fixation preference is typically better vision in the non-deviating eye. However, certain patients with monocular non-alternating esotropia exhibit a pronounced eye dominance despite having equal vision in both eyes.1–3 Certain patients may necessitate strabismus surgery to rectify their ocular misalignment. This surgical intervention can be executed through bilateral medial rectus recession (BMR) or unilateral medial rectus recession and lateral rectus resection (RNR).4,5 Bilateral surgery is generally considered less probable to cause incomitance, while unilateral surgery mitigates surgical risks associated with performing strabismus surgery in both eyes. In the case of non-alternating comitant esotropia, the necessity of surgical intervention for both eyes may induce additional anxiety in patients and their caregivers. This anxiety stems from the lack of comprehension regarding the rationale behind the need to operate the non-deviating eye. To our knowledge, a comparative analysis of bilateral versus unilateral surgical approaches in this scenario, when visual acuity is both eyes is similar, has not been previously conducted.
The aim of the current study is to analyze the surgical results of BMR vs RNR strabismus surgery in patients with non-alternating esotropia that is not associated with visual acuity disparity between eyes.
Methods
Ethics approval
The study was approved by the institutional review board and was conducted following the rules and regulations of the tenets of the Declaration of Helsinki.
Study design
The medical records of all patients who underwent strabismus surgery for esotropia at a single tertiary university affiliated hospital, between January 2010 and September 2023 were retrospectively reviewed.
Inclusion and exclusion criteria
Inclusion criteria: (1) Esotropia accompanied by monocular fixation preference, diagnosed according to the criteria established by Friedman et al., 2 when refixation with the preferred eye occurred within a second of removing the occluder from the non-deivated eye. (2) Best Corrected Visual Acuity (BCVA) within a difference of < 2 lines on the Snellen Chart between eyes; (3) BCVA of at least 20/30 in both eyes; and (4) Surgery was either BMR or unilateral RNR.
Exclusion criteria: (1) Prior strabismus, orbital or intraocular surgery; (2) An underlying neurologic or developmental pathologies associated with strabismus; (3) An ocular, orbital or craniofacial pathology; (4) Inability to cooperate with complete eye exams; and (5) Follow-up of less than 3 months.
Data collection
Patients who met the inclusion criteria were identified from the hospital's database and data were collected from their electronic records, including patient demographics, type of esotropia, age at the time of surgery, strabismus measurements in primary gaze at distance and near fixations using alternate prism cover test, BCVA and full cycloplegic refraction. Data were collected from the visit immediately before surgery and thereafter until the last available follow-up appointment. All strabismus evaluations preoperatively and during follow-up were performed by certified and experienced orthoptists. This was an unmasked retrospective study and final decision of surgical procedure conducted was reached after a comprehensive discussion between the surgeon, patients, and their caregivers, weighing the advantages and disadvantages of each surgical approach. All recessions were performed by a scleral fixation technique, and surgical dosing was at the discretion of the individual surgeon.
Following previous reports,6–9 a good surgical outcome was defined as ocular misalignment within 10 prism diopters (PD) of orthophoria at distance and near fixation during follow-up until the last available visit, without the need for additional strabismus surgery during follow-up. Surgical efficacy was calculated as preoperative deviation minus postoperative deviation at last follow-up for each patient.
Statistical analysis
Statistical analysis was performed using Microsoft Excel (Microsoft corporation, Redmond, WA, USA). Data are presented as mean ± standard deviation (SD) or by median and interquartile range (IQR). Means were compared using the student's t-test and the Chi-squared test was used for analyzing proportions. Statistical significance was defined at a p level <0.05.
Results
473 patients had strabismus surgery for esotropia correction during the study period and 26 (5.5%) of them met the study's inclusion criteria. Twelve (46.2%) were operated by RNR and the other 14 (53.8%) by BMR. Patient's belonging to both groups did not differ in gender, deviating eye laterality, BCVA, preoperative horizontal esodeviation at distance and near fixation, but differed in age (Table 1). Mean age of patients undergoing RNR was higher than that of patients operated by BMR. Another distinction between the groups was observed in their refractive errors. Patients undergoing RNR exhibited a slight myopia in both eyes, while those undergoing BMR demonstrated a mild hyperopia (Table 1).
Demographics and baseline characteristics of patients in the RNR and BMR groups.
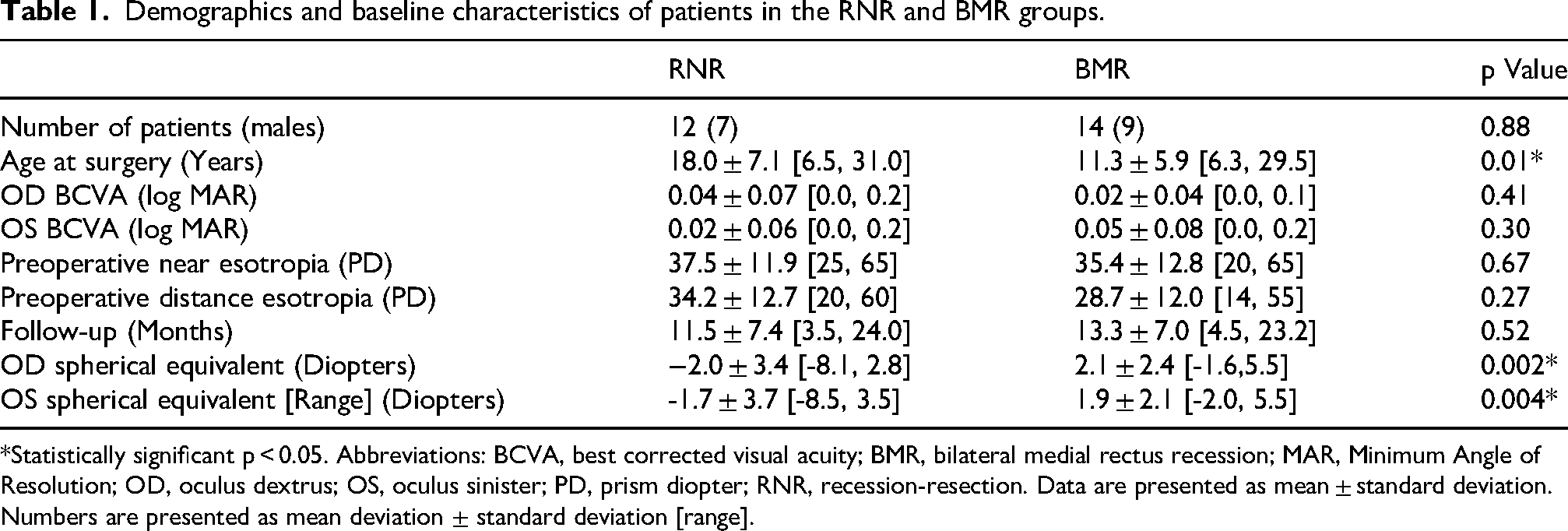
*Statistically significant p < 0.05. Abbreviations: BCVA, best corrected visual acuity; BMR, bilateral medial rectus recession; MAR, Minimum Angle of Resolution; OD, oculus dextrus; OS, oculus sinister; PD, prism diopter; RNR, recession-resection. Data are presented as mean ± standard deviation. Numbers are presented as mean deviation ± standard deviation [range].
Ocular misalignment decreased significantly following surgery performed by both surgical techniques. Final angles of deviations after RNR (distance 2.1 ± 2.9 PD and near 3.6 ± 3.7 PD) were not significantly different than after BMR (distance 1.4 ± 2.4 PD and near 4.0 ± 4.5 PD, p = 0.54 and p = 0.80 respectively). Additionally, actual surgical effect and a similar success rate were noted after both types of surgeries (100% for RNR and 92.8% for BMR, p = 0.35, Table 2). One patient in the BMR group exhibited residual esotropia exceeding 10 PD at near fixation. This patient was satisfied with their outcomes and did not want further surgical intervention. Notably, only one patient developed a minor angle consecutive exodeviation of 4 PD following the RNR procedure, without visual or cosmetic complaints. Visual acuity and stereopsis improvement were similar in both groups (Table 2).
Surgical and follow-up data of patients in the RNR and BMR groups.
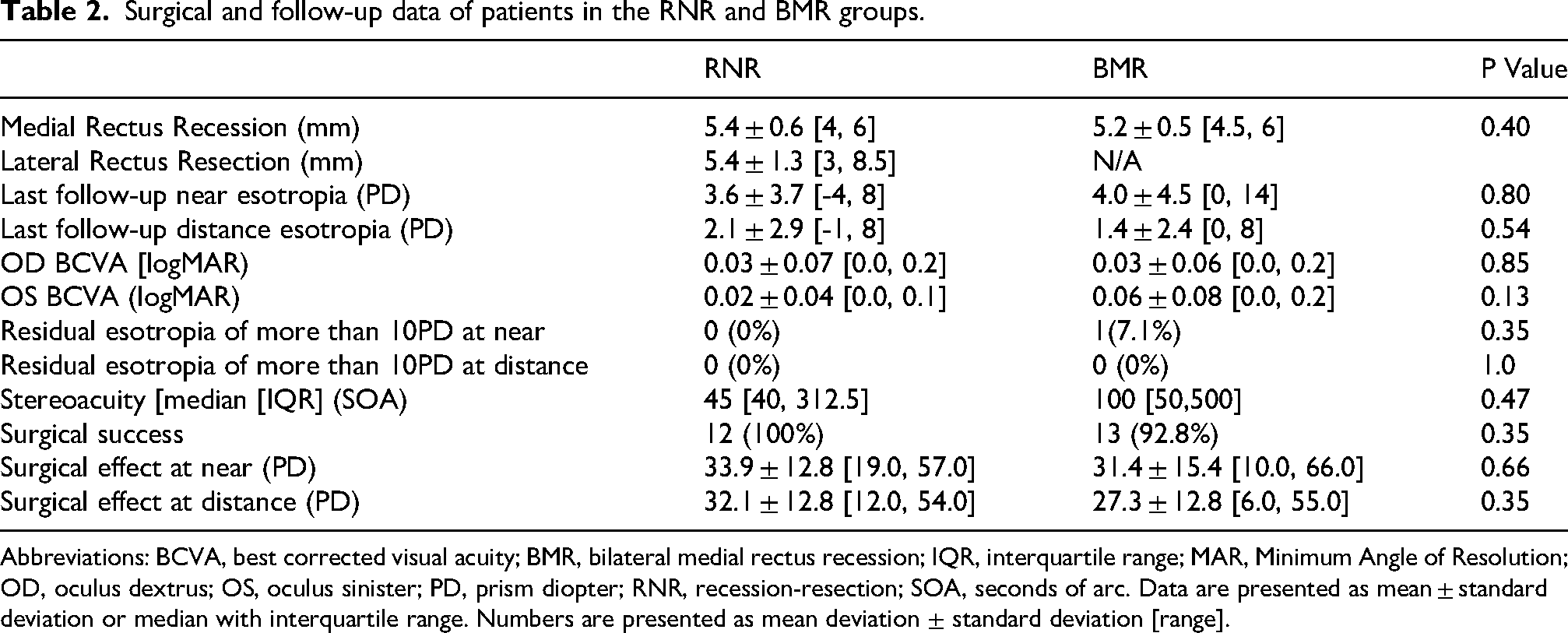
Abbreviations: BCVA, best corrected visual acuity; BMR, bilateral medial rectus recession; IQR, interquartile range; MAR, Minimum Angle of Resolution; OD, oculus dextrus; OS, oculus sinister; PD, prism diopter; RNR, recession-resection; SOA, seconds of arc. Data are presented as mean ± standard deviation or median with interquartile range. Numbers are presented as mean deviation ± standard deviation [range].
Discussion
In this study, we compared surgical outcomes of RNR and BMR in patients with non-alternating monocular esotropia that is not associated with different vision between eyes. The final surgical success rate was high for both surgical techniques, 100% after RNR and 93% after BMR, indicating that both strategies can be equally considered in these circumstances.
The comparison between unilateral and bilateral surgery is a subject of multiple studies in various strabismus types. While bilateral surgery is perceived as less likely to cause incomitance, unilateral surgery allows sparing of one eye, which is oftentimes preferable by both patients and caregivers. Interestingly, the debate whether either technique yields better outcomes has yet to be resolved, hence, in most cases, the decision is left to surgeon's discretion. Bartley et al. analyzed 129 children with esotropia who underwent RNR and 77 children who underwent BMR and found that unilateral surgery had a favorable outcome. 10 However, because patients undergoing RNR had a higher frequency of amblyopia and smaller esodeviations, the authors were hesitant to conclude that RNR is superior for esotropia correction. In contrast, our study exclusively included patients with monocular esotropia associated with equal vision in both eyes, and the preoperative deviation in both groups was comparable. More recently, Ismail et al. reported equal success for bilateral and unilateral strabismus surgery in non-amblyopic patients with alternating partially accommodative or non-accommodative esotropia. 11 Similarly, we found a very high and similar success rates for bilateral and unilateral surgeries in non-amblyopic patients with non-alternating esotropia. Polling et el. Reported good surgical outcome for either unilateral or bilateral strabismus surgery in non-amblyopic children with infantile esotropia; however, their study did not differentiate between alternating and non-alternating deviations. 12 Other studies found contradicting results. Arnoult et al. reported that patients undergoing RNR had a better outcome than those operated by BMR for correction of esotropia smaller than 50 PD, 13 whereas Kim et al. found the opposite, advocating bilateral surgery. 8 In our study, mean preoperative esotropia measured approximately 35 PD in both groups and surgical success was similar following both unilateral or bilateral surgeries.
This study presents several limitations that warrant discussion. Firstly, it is a retrospective study, which inherently presents challenges. Secondly, the sample size reported is relatively small. However, our methodology of restricting the study population to individuals with non-alternating esotropia without amblyopia and nearly equal visual acuity in both eyes is reflective of the prevalence of this condition within the family of esodeviations (6%). Another limitation is the significant age disparity between patients undergoing surgery using both techniques, with patients undergoing RNR being notably older. It is plausible that older patients having a higher level of concern regarding the operation of the non-deviating eye preferred to undergo unilateral surgery. Interestingly, other studies have also reported that patients undergoing unilateral surgery for esotropia correction were older than patients who underwent bilateral surgery.8,10 The observed age disparity may also account for the refractive error variations observed between groups, as it is well-established that with age, there is a gradual myopic shift in refraction. 14 Furthermore, we utilized the widely accepted definition of favorable surgical outcome following strabismus surgery, which is a deviation within 10 degrees of orthophoria. However, it is important to acknowledge that this definition has certain limitations. Some patients with smaller residual deviation may develop monofixation syndrome, leading to a loss of sensory fusion. Additionally, some patients may still experience a cosmetically noticeable ocular misalignment. Finally, our strabismus assessment did not always include measurements on side gaze. Although none of the patients complained of noticebale lateral incomitance or diplopia on side gaze, we cannot fully ascertain that there was no lateral incomitance postoperatively.
In summary, non-alternating esotropia, associated with similar visual acuity in both eyes, is a relatively uncommon form of strabismus. Our findings indicate that for patients with this type of esodeviation who have concerns about the need to operate on their non-deviating eye, equal surgical outcomes can be achieved by performing RNR exclusively in the deviating eye.
Footnotes
Ethical approval
The study was approved by the IRB committee of the medical center and was conducted in accordance with the Helsinki tenets. Approval number 0809-20-RMC.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Statements and declarations
All authors have read the final version of the manuscript and approved the submission to the journal.