
Abstract
Introduction:
Heterotopic ossification may develop after major hip surgeries, thus preventive strategies including radiation therapy and non steroid anti-inflammatory drugs are commonly employed. There are certain concerns regarding the effects of radiation therapy on implant loosening and carcinogenesis. Our study aims to evaluate whether radiation therapy results in implant loosening or radiation-induced tumours in the long term.
Patients and methods:
This was a prospective study including 97 high-risk patients for heterotopic ossification who underwent total hip arthroplasty. Patients were divided into 2 groups and received either a combination of radiation therapy and indomethacin (Group A), or indomethacin alone (Group B). Evaluated outcomes included implant loosening or development of radiation-induced tumours during the follow-up period.
Results:
The follow-up period of the study was 10 years. Group A consisted of 50 patients, while Group B consisted of 47 patients. 3 patients died during the follow-up. There were 2 cases of implant loosening, 1 from each of the 2 groups at 9 and 10 years after surgery respectively; thus, no statistically significant difference regarding implant loosening was found (p < 0.05). During the follow-up period no cases of radiation-induced tumours were identified.
Conclusion:
Our results are consistent with those of other studies supporting the safety of radiation therapy as a preventive strategy for heterotopic ossification following major surgeries in high risk patients. Further studies with even longer follow-up may be required to definitely exclude the possibility of adverse outcomes linked with radiation therapy.
Introduction
Heterotopic ossification (HO) is a frequent complication following major hip surgery 1 Its incidence after total hip arthroplasty (THA) is estimated to be up to 90%, although the incidence of clinically relevant HO is much lower (3–7%).2–8 Development of HO follows activation of osteogenic precursors which in turn stem from pluripotent mesenchymal cells. The signal that promotes differentiation of these pluripotent cells into osteoblasts is believed to involve several inflammatory mediators such as prostaglandins and overexpression of bone morphogenetic proteins.9,10
Preventive strategies for HO are required in high-risk patients. The 2 mainstay modalities for HO prophylaxis include radiation therapy and non-steroid anti-inflammatory drugs (NSAIDs).9–11 Radiation therapy suppresses osteoblastic activity. Its use as a preventive measure for HO was 1st described back in 1981 by Coventry and Scanlon. 12 Since then many modifications have been made regarding the radiation dose and fractionation of this dose.13–15 The rationale for NSAIDs as a preventive measure for HO lies in the fact that these agents work by inhibiting the production of prostaglandins, as well as by directly inhibiting differentiation of osteogenic precursors cells.16–18 A combined therapy including both radiation therapy and NSAID has been found to be more effective than NSAID use alone, so a prevention protocol including both measures may be the optimal method for HO prophylaxis. 1
There are certain risks associated with both of these 2 modalities. NSAIDs increase the bleeding risk in patients with peptic ulcer and may exacerbate asthma symptoms. They are also contraindicated in patients with renal insufficiency or hepatic dysfunction, so their use is limited to a certain proportion of patients. 10 On the other hand, radiation therapy is also linked with some adverse outcomes. The 1st concern is about the theoretical effect on carcinogenesis. Although there is no evidence from clinical studies supporting the idea that radiation therapy results in increased rates of cancer, opponents say that the lack of such documented cases may be due to the fact that radiation-induced tumours have a long latency period, so studies with a short follow-up may fail to identify development of such tumours.10,19 The other adverse event that is hypothesised to be associated with radiation therapy is implant loosening. Since radiation therapy suppresses osteoblastic activity, and bone ingrowth is needed for a rigid long-term fixation of the femoral and acetabular components into the native bone, there are reasonable concerns about the long-term stability of these implants.9,20 Moreover, the additional use of NSAIDs with radiation therapy in a combined protocol raises a further concern about the combined effects on implant stability, since both of these 2 modalities are potent inhibitors of new bone formation.
There is sparse evidence about the incidence of these theorised adverse effects of radiation therapy in the long-term. Our study aims to evaluate the hypothesis that radiation therapy increases the risk of carcinogenesis and implant loosening in patients after THA, even when radiation therapy is combined with NSAID, with a long follow-up.
Methods
Study design
This is a prospective study including high-risk patients for HO (hypertrophic osteoarthritis, previous history of HO formation) who underwent THA for primary osteoarthritis between October 2004 and January 2006 at the Department of Orthopaedics, University Hospital of Ioannina, Greece. All participants provided informed written consent, while IRB (Institutional Review Board) approval was also obtained. The study population was divided into 2 groups. Group A received a combination of radiation therapy and NSAID, while Group B received only NSAID for prevention of HO formation. Radiation therapy consisted of a single postoperative dose of 7 Gy within the 1st 3 days after surgery, while NSAID therapy included 75 mg of indomethacin once daily for the 1st 3 weeks postoperatively. Proton pump inhibitors were additionally administered in patients who received indomethacin for alleviation of adverse gastrointestinal effects. Exclusion criteria included patients with renal failure, severe hypertension, hepatic dysfunction or known allergy to NSAID.
Operation and radiation therapy protocol
All operations were performed by the same team. A posterolateral approach and a cementless press fit technique for both femoral and acetabular components were used in all surgeries. Postoperatively, patients received a daily dose of low molecular-weighted heparin (tinzaparin) for thromboprophylaxis for the following 5 weeks. The radiation therapy protocol included simulation prior to therapy at the Department of Radiation Therapy in our hospital. Based on the body size, an individual portal of 12–14 × 12–14 cm was selected to include all periarticular soft tissues. Irradiation was delivered with a linear accelerator (6 MV). 2 parallel-opposed fields (anteroposterior and posteroanterior) were applied. A single dose of 7.0 Gy was administered in the midplane.
Evaluation and statistical analysis
All patients were assessed radiologically and clinically for development of implant loosening up to 10 years postoperatively. At the same time patients were also interviewed for any presence of radiation-induced cancer since the administration of radiation therapy. Radiological confirmation of implant loosening was based on precisely defined findings including: component migration or periprosthetic zone of radiolucency around the bone-prosthesis interface > 2 mm. 21 In case of periprosthetic radiolucency > 2 mm, patients were considered positive for loosening when this sign of abnormality was associated with clinically relevant symptoms including femoral or hip pain. Otherwise, patients with this degree of radiolucency were followed at short intervals (every 6 months) for any signs of progressively enlarging radiolucency, which was also considered a positive finding indicating implant loosening. In cases with persistent femoral or hip pain and no abnormal radiological signs or equivocal signs of loosening, further imaging studies such as 3-phase bone scans were performed. Primary endpoints of the study were implant loosening as defined by the combination of positive imaging and clinical findings, and presence of any radiation-induced tumour, including blood malignancies like leukemia or pelvic tumours, like testicular cancer in men or cervical cancer in women.
For the statistical analysis, the chi square approximation test for categorical variables was used in order to compare the frequency of implant loosening or radiation-induced cancer between the 2 groups. Hazard ratios for implant loosening or radiation-induced cancer were also calculated. Group differences were tested using the chi-square approximation test for categorical variables and the Mann-Whitney U test for continuous variables. Level of statistical significance was set at p < 0.05.
Results
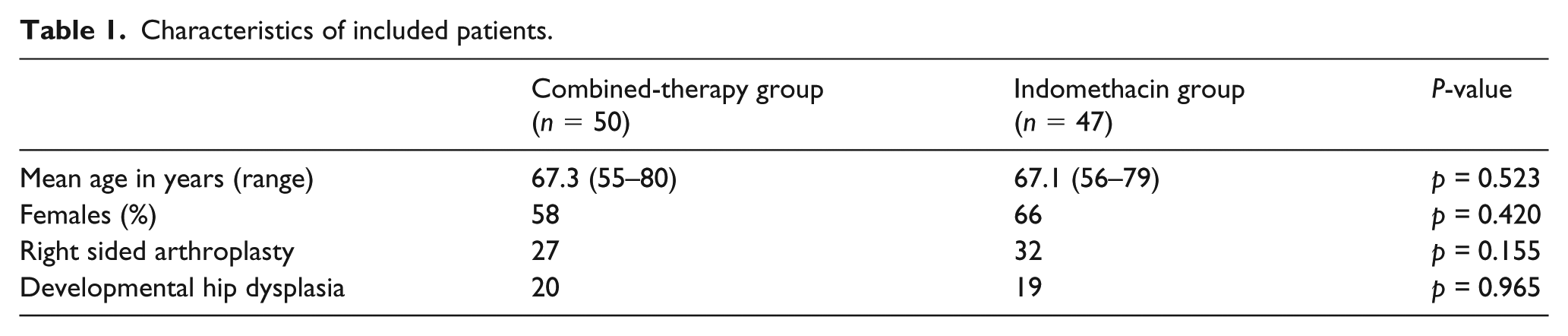
In total 97 patients were included in the study. 50 patients were allocated to Group A and received the combined therapy, while 47 patients were allocated to Group B and received indomethacin alone. 3 patients died during the follow-up period, 1 from Group A and 2 from Group B. The main demographics of the patients are presented in Table 1. Additional screw fixation for the acetabular component was needed in 19 patients from Group A and in 15 patients from Group B. Acute side effects during the radiation therapy included mild nausea; however, this did not require discontinuation of the radiotherapy session though. There were no statistically significant differences in patient characteristics between the 2 groups (p < 0.5).
Characteristics of included patients.
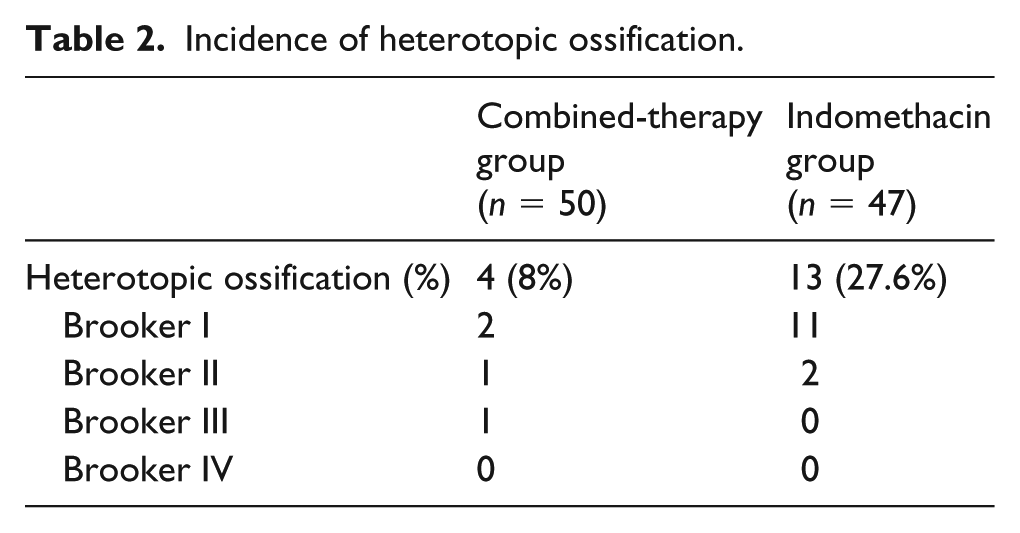
Heterotopic ossification was radiologically evident in 17 patients (in 4 patients from Group A and in 13 patients from Group B) during the 6 postoperative months (Table 2). The incidence of HO in patients who received combined therapy was statistically significant, lower than in those who received only indomethacin (p = 0.01). Clinically significant (Brooker grade III–IV) HO developed in 1 patient from Group A, while no patient from Group B had clinically significant HO.
Incidence of heterotopic ossification.
Regarding implant loosening, there were 2 cases of loose components that were confirmed by positive clinical and imaging signs, 1 from each group. Subsequently, there was no statistically significant difference between these 2 groups (p = 0.964). Alternatively, the associated risk for implant loosening with radiation therapy was not increased (hazard ratio [HR] = 0.940, 95% confidence interval [CI] = 0.0605–14.6031). In the patient from Group A, implant loosening was assumed from x-rays due to signs indicating possible cup migration (slight change in the abduction angle of the cup) along with polyethylene wear at 9 years postoperatively (Figure 1). This patient also reported worsening pain in the hip for the previous 11 months, aggravated by excessive walking and alleviated by rest. Further evaluation with a 99-technitium bone scan confirmed acetabular cup loosening. In the 2nd patient from Group B implant loosening was confirmed at 10 years postoperatively by a progressively enlarging radiolucent zone around the acetabular component over a 6-month period. Along with this finding, the patient reported worsening pain in the hip area for the same period. In both cases the femoral stems did not demonstrate any clinical or radiological signs of loosening. Both patients underwent revision arthroplasty for acetabular cup exchange only. Intraoperatively, acetabular components were found to be loose in both cases, while stability of the femoral stems was further confirmed. Neither of these 2 patients demonstrated any further signs of loosening after the revision procedure until the end of the follow-up period.
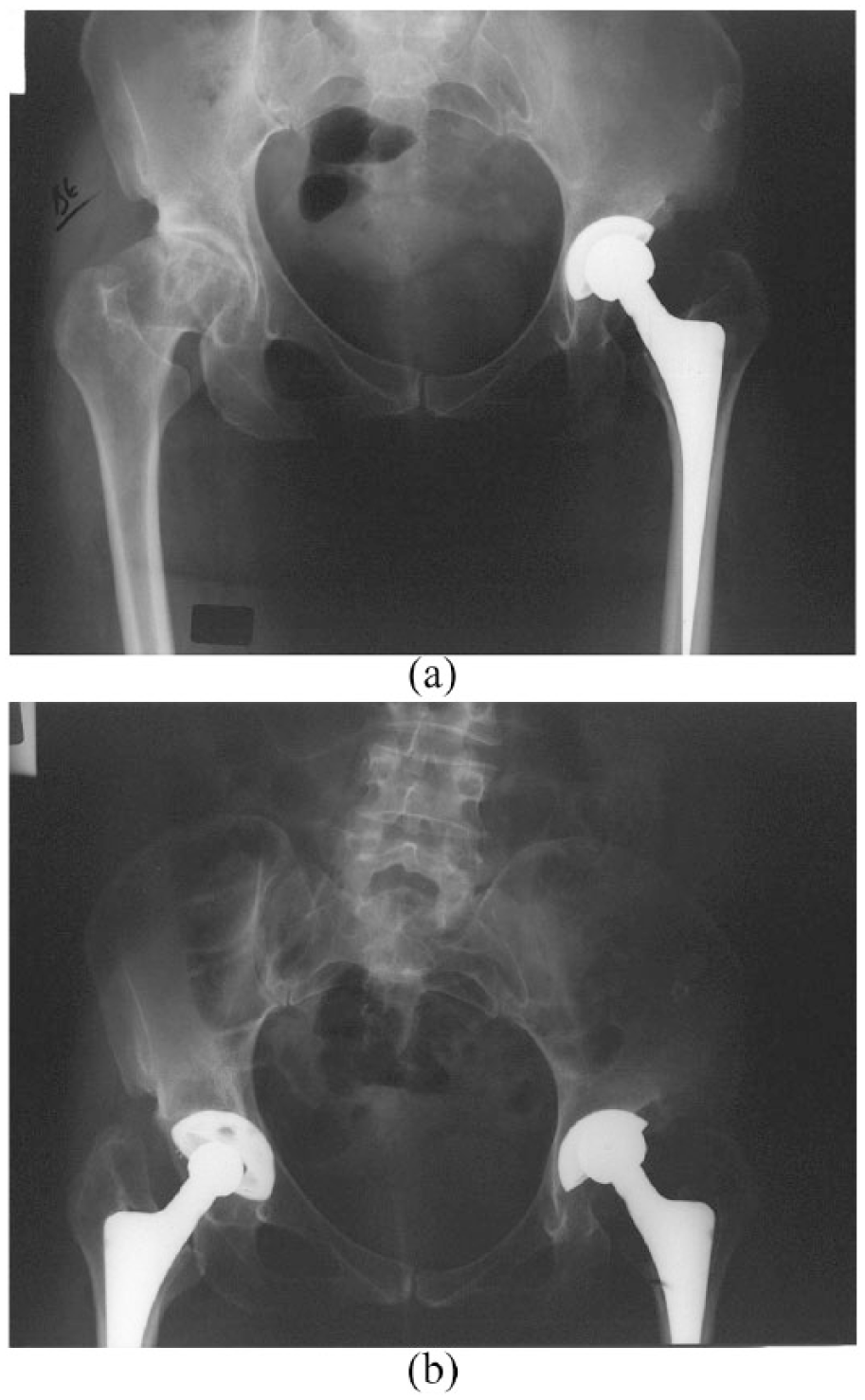
(a) An anteroposterior radiological view of the pelvis demonstrating a left THA. (b) A pelvic x-ray of the patient 9 years after the left THA showing possible migration of the acetabular cup as indicated by the slightly different abduction angle of the cup, and polyethylene wear.
Regarding carcinogenesis related to radiation therapy, there were no cases of associated tumours. In total, 3 patients from Group A developed lung, breast and brain cancer respectively. The patient with lung cancer died 15 months after diagnosis, and thus did not complete the follow-up evaluation. Malignant tumours were developed in 5 patients from Group B. These tumours included thyroid, lung, colon, brain and breast cancer respectively. Patients with lung and ovarian cancer died during the follow-up period. There was no statistically significant difference regarding radiation-dependent carcinogenesis between the 2 groups.
Discussion
While radiation therapy for HO prevention has been linked with carcinogenesis and implant loosening, no clinical data exist to support these concerns. The results of our study further support the safety of radiation therapy since it did not increase rate of implant loosening, while there was no incident of radiation induced carcinogenesis. Moreover, the combination of radiation therapy with indomethacin proved to be more efficient than indomethacin alone in HO prevention. Thus, our proposed protocol, including a single radiation dose of 7 Gy and additional use of indomethacin, seems to be a safe and successful strategy for HO prophylaxis.
The increased rate of component loosening has been extensively shown in cancer patients who received adjuvant radiotherapy for pelvic tumours and underwent total hip arthroplasty in the following period, although the dose of radiation that is used in radiotherapy for pelvic tumours is much higher than the 1 given for prevention of HO as in our study.22–25 Conversely, association between radiation therapy for HO prevention and implant loosening has not been clearly demonstrated in clinical studies and only experimental data exist to support this hypothesis. An animal study in rabbits found that the pull-out strength of rods inserted in the tibia was significantly decreased in those that received a 10 Gy dose of radiation therapy. 20
Potential impairment of new bone formation by NSAID is a controversial issue that has been evaluated by numerous studies, without any clear findings. 26 Although the role of NSAID as a potent inhibitor has been mainly studied after bone fractures, there are also studies regarding the implication of these agents in early aseptic loosening. 27 Since our common protocol for HO prevention includes a combination of radiation therapy and indomethacin, an increased rate of early implant loosening would probably be expected as the potential adverse effects of radiation therapy may be added up to those of NSAID. However, this was not evident in this study as the incidence of aseptic loosening was not increased.
Although radiation doses < 30 Gy do not seem to have any effects on carcinogenesis, there is sparse evidence regarding the effects of the radiation doses used for HO prevention in the long-term. 9 In our study there were no incidences of radiation-induced tumours, as defined tumours in pelvic area or blood malignancies, up to 10 years after radiation therapy.
Another concern is the effect of radiation on the testes and whether damage may be induced on spermatogenesis. Shielding of the testes is recommended during radiation therapy. Reversible oligospermia, with doses as low as 0.2 Gy, may occur, as shown in experimental studies. 19 It has been estimated that when a dose of 8 Gy is used for HO prevention, the received dose to the testes is 0.25 Gy when no shielding blocks are used, while with shielding the received dose is 0.11 Gy.28,29 It seems that radiation therapy with shielding is a safe strategy limiting the risk of testicular damage.
The main strength of our study is the long-term follow-up which allows us to extract relatively safe conclusions about the association of radiation therapy with carcinogenesis and implant loosening. On the other hand, there are certain limitations of our study that must be addressed. Although the follow-up of the study is up to 10 years, even this duration of follow-up may be insufficient to detect radiation-induced tumours as there is evidence that such tumours may present up to 15–25 years after radiation therapy.13,19 Another limitation is the relatively small number of patients included in our study which attempts to identify rare events such as radiation induced tumours and implant loosening. Last, the lack of young patients in our study did not enable us to evaluate the possibility of adverse effect of radiation therapy on spermatogenesis.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.