
Abstract
Background:
When performing anterior total hip arthroplasty (THA) for patients who require leg lengthening, surgeons often encounter difficulties during reduction due to soft tissue tightness. The purpose of this study was to introduce a new THA reduction technique for these patients.
Methods:
Between October 2018 and September 2019, 545 THAs were performed. In 15 hips (2.8%), reduction was not achieved with a traditional technique. The preoperative diagnosis was Crowe grade II in 4 hips, Crowe grade III in 4 hips, Crowe grade IV in 1 hip, and sequelae of Legg-Calvé-Perthes disease in 6 hips. All procedures were performed using a direct anterior approach. The new reduction technique was to use a lever hooked on the acetabular teardrop as a counter force against the preserved muscles. The lever was connected to the impactor with a wire and the counterforce was transmitted to the impactor.
Results:
Reduction was achieved in all cases without shortening osteotomy or muscle release. The mean lengthening of the operated limb was 30 mm (range 13–59 mm). Neither sciatic nor femoral nerve palsy were observed.
Conclusion:
We developed a new anterior THA reduction technique for patients who require leg lengthening. When the centre of the femoral head was reduced to the superior edge of the cup with the traditional technique, reduction was safely achieved with this technique.
Keywords
Introduction
The direct anterior approach (DAA) for total hip arthroplasty (THA) has been gaining popularity as a minimally invasive alternative. Several advantages of the DAA have been demonstrated by prospective randomised studies, including faster functional recovery, less perioperative pain, and low dislocation rate.1–4 However, as Barrett et al. 5 reported in a 5-year follow up study, the benefits of the DAA were limited only to the early postoperative period and there were no significant differences in survivorship, function, complications, or radiographic evaluation at longer follow-up. As the DAA can preserve muscles, surgeons often encounter difficulties during the procedure, especially in patients with sequelae of Legg-Calvé-Perthes (LCP) disease or in cases of severely dislocated hips. To achieve anterior THA reduction in patients with Crowe stage IV developmental dysplasia, the use of subtrochanteric shortening osteotomy or delayed reduction technique has been reported.6,7 However, these procedures have potential disadvantages, including longer operative time, non-union at the osteotomy site, shortened limb and longer hospital stay. The purpose of this study was to introduce a new anterior THA reduction technique.
Material and methods
Between October 2018 and September 2019, 545 THAs were performed by a single surgeon. The surgery was performed using the DAA on a standard surgical table in all cases. The anterior and superior capsules were resected, and the posterior capsule was released from the greater trochanter. If the anterior mobilisation of the proximal femur could not be sufficiently achieved to perform the femoral preparation, the short rotators were released. The acetabulum was reamed to the original configuration as closely as possible. In all cases the cups were placed in the original acetabular region, which was defined as the hip centre within 15% of the pelvic height from the tear drop line. Traditional reduction was performed by applying pressure inferiorly on the femoral head with an impactor, while keeping the knee and hip slightly flexed to loosen the rectus femoris and the hamstrings. To achieve the reduction, no muscles were released, including the iliopsoas, rectus femoris, hip adductors and tensor fascia lata muscle. In 15 hips, the centre of the femoral head was relocated to the level of the superior edge of the acetabular cup; however, reduction was not achieved. The new reduction technique was applied in these cases.
The study protocol was approved by the institutional review board and all patients provided informed consent.
Reduction technique
First, a lever was hooked onto the inferior edge of the acetabular teardrop and an impactor was placed on the femoral head. The lever used is a part of VERBRUGGE bone forceps. Second, a wire (1.2 mm in diameter) was looped around the lever and the impactor (Figure 1). Third, a reduction force was applied to the lever and the impactor simultaneously. An assistant pushed the impactor toward the centre of the acetabular cup while the surgeon pulled the lever caudally. The lever provided the counterforce to the cup and the force was transmitted to the femoral head through the wire to achieve reduction.
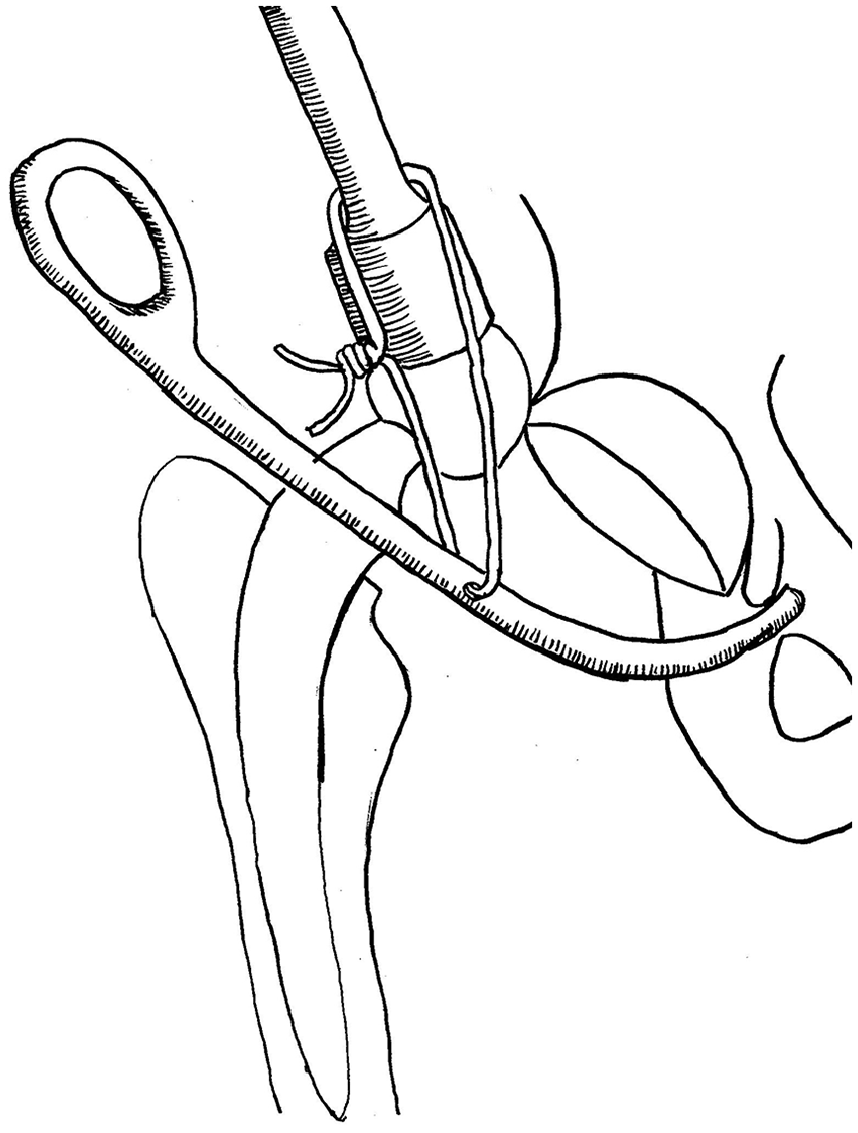
The tip of the lever was hooked on the inferior edge of the acetabular teardrop. A wire (1.2 mm in diameter) was looped around the lever and the impactor on the femoral head.
Cementless hemispherical acetabular components were applied in all hips, while femoral implants were selected based on the characteristics of each femur. The acetabular components used were the G7 (Zimmer-Biomet, Warsaw, IN, USA) and PINNACLE (DePuy, Warsaw, IN, USA). The femoral stems used were the CMK (Zimmer-Biomet, Warsaw, IN, USA) and CORAIL (DePuy, Warsaw, IN, USA).
Clinical and radiographic evaluations were performed before surgery and at the last follow-up. The clinical evaluation was performed based on the Japanese Orthopedic Association (JOA) hip score, which allocates 40 points for pain, 20 points for range of movement, 20 points for walking ability, and 20 points for activities of daily living, with a maximum total score of 100 points. The function of the sciatic and femoral nerves was examined by at least two doctors on the first postoperative day. The sensory disturbance of the anterolateral thigh area associated with the lateral femoral cutaneous nerve neuropraxia was not evaluated. Radiographic analysis was performed using serial anteroposterior pelvic views and limb lengthening was determined by comparing the change in the distance between the tip of the greater trochanter and a line drawn through both acetabular teardrops before and after surgery. The magnification of all radiographs was calibrated using the known diameter of the artificial femoral head. All measurements were made by 3 observers (KO, YN, YM), and the final results were the average value of these measurements.
Postoperative rehabilitation was initiated on the first day after surgery. Both active and passive motion exercises of the involved joint and full weight-bearing were allowed for all patients on the first postoperative day. If they were able to walk with a walking stick for over 300 m and go up and down stairs, they were discharged.
Results
There were 11 females and 4 males, with a mean age of 63 years (range 51–73 years). The mean height, weight, and body mass index (BMI) was 159 cm (range 145–170 cm), 60 kg (range 46–75 kg), and 24 kg/m2 (range 19.4–28.2 kg/m2), respectively. The preoperative diagnosis was Crowe II in 4 hips, Crowe III in 4 hips, Crowe IV in 1 hip, and sequelae of LCP disease in 6 hips.
The mean acetabular cup diameter was 49 mm (44 mm in 1 hip, 46 mm in 1 hip, 48 mm in 6 hips, 50 mm in 3 hips, 52 mm in 3 hips, and 54 mm in 1 hip). A CMK femoral stem was used in 13 hips and a CORAIL was used in 2 hips. The femoral head diameter was 32 mm in 14 hips and 28 mm in 1 hip.
Reduction was achieved in all cases without femoral shortening osteotomy or additional muscle release (Figures 2 and 3). The mean operated limb lengthening was 30 mm (range 13–59 mm), while the mean leg-length discrepancy improved from 23 mm (range 11–60 mm) preoperatively to 6 mm (range 0–11 mm) postoperatively. The mean operative time was 69 minutes (range 49–107 minutes), during which the mean operative blood loss was 361 g (range 120–750 g). The mean postoperative hospital stay was 4.7 days (4–8 days) and the JOA hip score improved from 43 points (range 33–59 points) to 85 points (range 72–97 points) at the last follow-up.
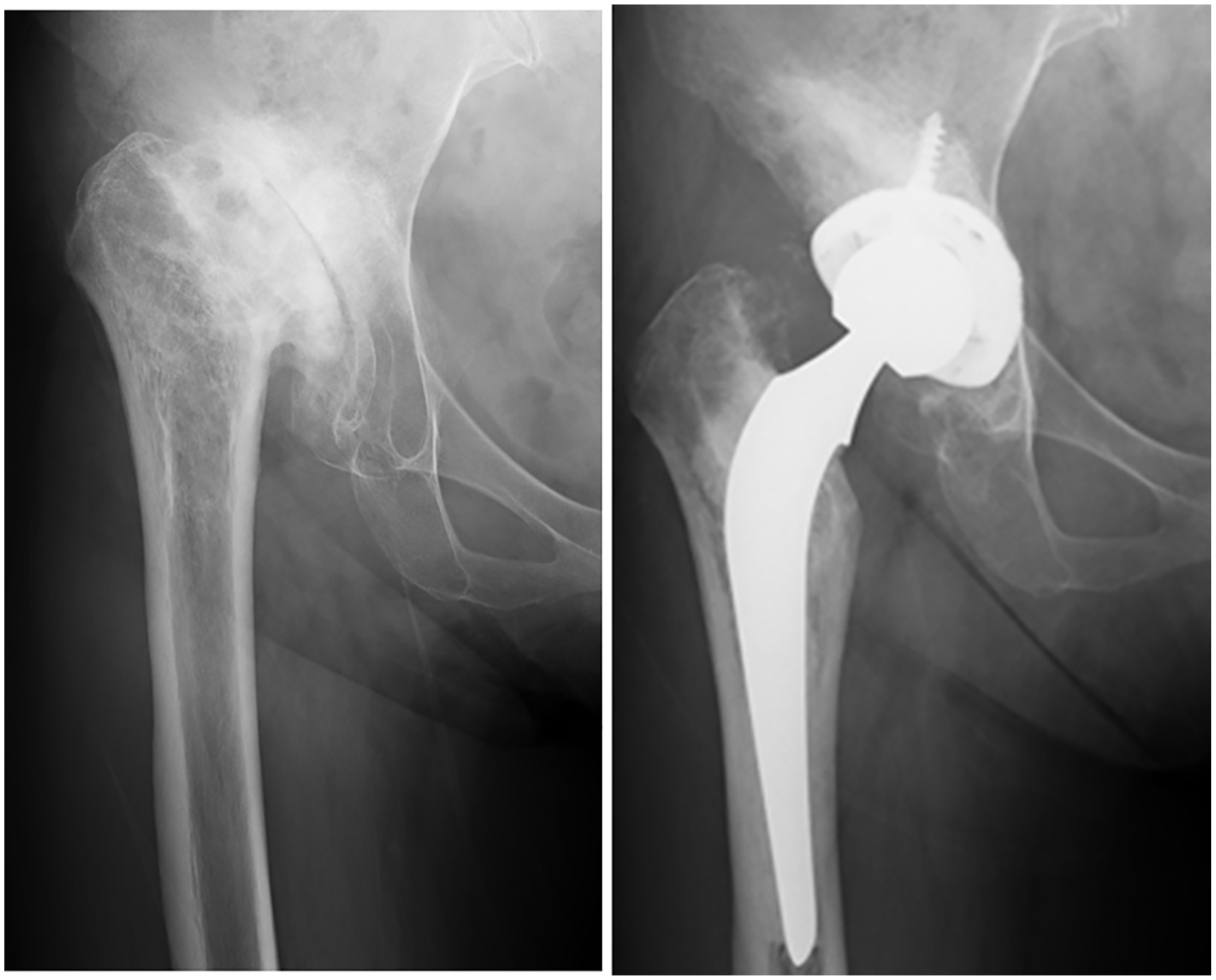
(A) A 61-year-old female with sequelae of Legg-Calvé-Perthes disease in her right hip. (B) The new reduction technique was applied and leg lengthening was 45 mm.
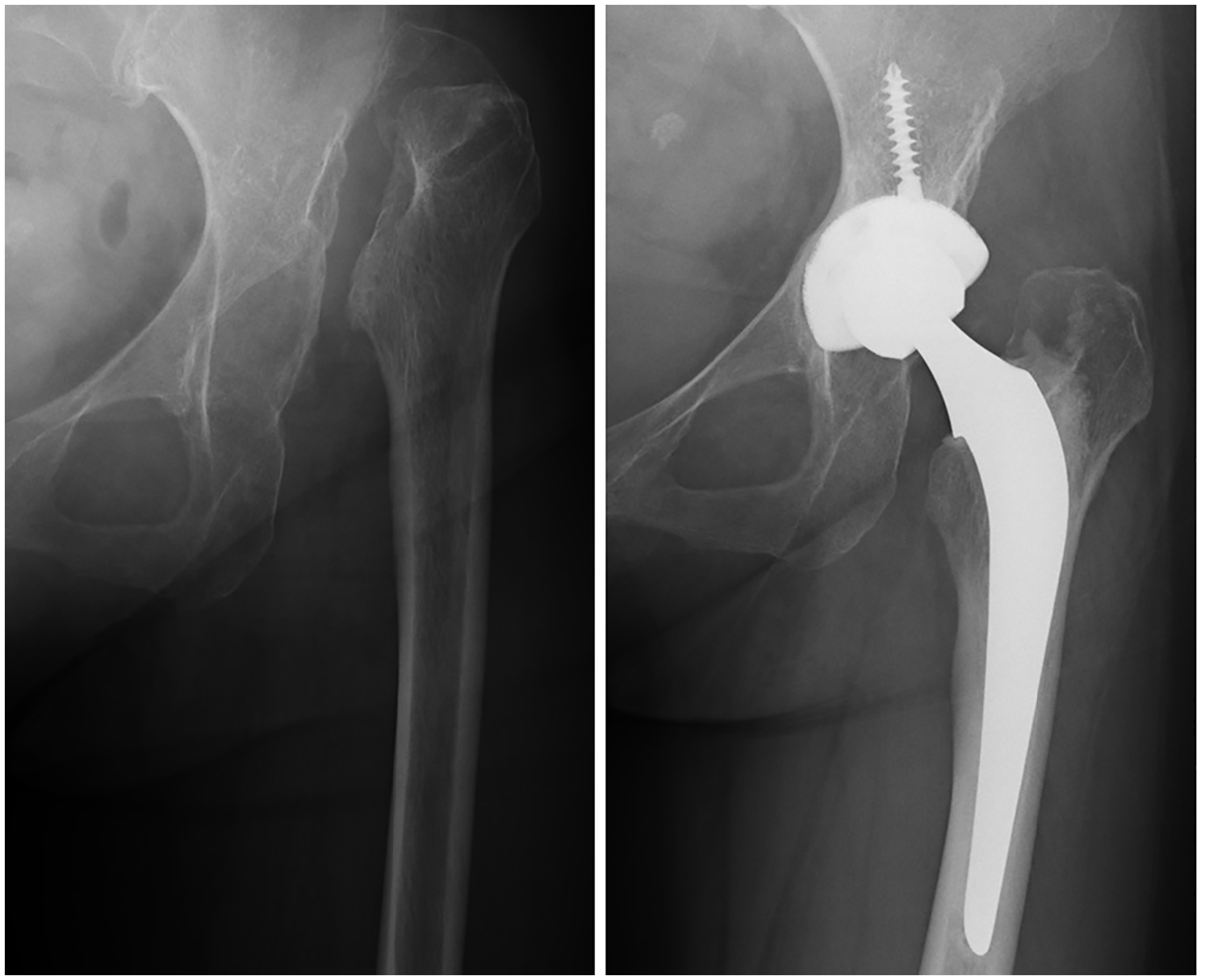
(A) A case of a 51-year-old female with Crowe grade IV in her left hip. (B) Reduction was achieved without shortening osteotomy.
There were no cases of sciatic or femoral nerve palsy or any other complications, including implant migration, dislocation, symptomatic pulmonary embolism, and infection. 3 patients displayed slight adduction and flexion contracture. However, they recovered with postoperative rehabilitation within 3 days after surgery.
Discussion
The essence of this reduction technique was to use a lever hooked on the acetabular teardrop to apply a counterforce, which was transmitted to an impactor through a wire. As a result, reduction was achieved without releasing any muscles or using shortening femoral osteotomy in all cases where reduction had not been achieved with the traditional technique. The use of this technique in this study was only applicable to the DAA. However, if the lever were hooked onto the acetabular tear drop, it could be used in other approaches.
The DAA uses the true inter-nervous plane and can be applied to THA for patients with highly dislocated dysplasia, allowing for muscle preservation without risk of denervation. 6 In the DAA, however, preserved muscles make it difficult to achieve reduction, especially in patients who require leg lengthening. When surgeons push the femoral head towards the centre of the cup with the impactor, the reduction force applied to the femoral head is transmitted to the pelvis when muscles are preserved. As a result, the acetabulum is pulled caudally by the reduction force. In this situation, regardless of the force applied to the femoral head, reduction is not achieved. In this study, reduction was not achieved in 15 hips (2.8%) with the traditional technique. Using the new reduction technique, a lever hooked onto the acetabular teardrop not only prevents the acetabulum from being pulled caudally but also enhances the reduction force to the femoral head with a wire looped around the impactor and lever.
Some authors have reported that excessive leg lengthening would be a risk factor for nerve palsy.8,9 However, Kerboull et al. 10 obtained a mean leg lengthening of 3.8 cm (range 2–7 cm) with only 1 case of peroneal nerve palsy which recovered completely within 1 week postoperatively in a long-term follow-up study of 118 THAs with Crowe grade IV dysplasia. Eggli et al. 11 reported that there was no significant correlation between the amount of leg lengthening and the occurrence of nerve palsy in 508 consecutive THAs in 370 patients with developmental dysplasia. They concluded that nerve palsy was most commonly caused by direct or indirect mechanical damage and not by leg lengthening on its own. In our study, no patients showed symptoms of motor nerve palsy. Moreover, the preserved muscles are thought to help the motor nerves not to be lengthened excessively.
There were not any perioperative complications in this study. However, there are some potential risks in patients who require a certain amount of leg lengthening. In these patients, the acetabulum is severely dysplastic and the bone around the tear drop is fragile. When the acetabulum is exposed with retractors, the femoral and sciatic nerves could be damaged. The lever hooked onto the tear drop could break the tear drop. The retractors should be inserted cautiously to avoid damaging the nerves. The cup should be fixed rigidly in order to support the lever, even if the tear drop was broken during the reduction.
We could not determine a limit for leg lengthening in this study. However, in all cases, the centre of the femoral head was reduced to the superior edge of the acetabular cup with the traditional technique and reduction was safely achieved with this technique. Therefore, unless the centre of the femoral head is reduced to the level of the superior edge of the acetabular cup with the traditional technique, it remains unclear whether the reduction will be safely achieved or not. Further studies with a larger number of cases are needed.
Conclusion
We developed a new THA reduction technique for patients who require leg lengthening. When the centre of the femoral head was reduced to the level of the superior edge of the acetabular cup with the traditional technique, this technique was safe and feasible.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.