
Abstract
Background:
Highly porous shells have been used with success to manage acetabular bone loss in complex (cTHA) and revision total hip arthroplasty (rTHA) for nearly 2 decades. Recently, a 3D-printed titanium shell with locking screw technology was developed. Our study sought to evaluate the survivorship of the novel variable-angle locking screw (VALS) acetabular component.
Methods:
This multicentre retrospective study analysed cTHA (n = 61) and rTHA (n = 145) using the VALS component. 206 patients were included in the final analysis, with a mean age of 65.1 (range 15–95) years, mean BMI of 30.9 ± 7.3 kg/m2, and 60.2% women. Mean follow-up was 1.1 (range 0.1–5.1) years. The Kaplan-Meier analysis was utilised to assess implant survivorship and reoperation.
Results:
Of the 206 included cases, 20 were reoperations, 9 of which involved acetabular revision. The 1-year and 2-year acetabular component revision-free survivorship was 95 and 94%, and all-cause reoperation was 90 and 86%, respectively. Importantly, there were only 2 cases of aseptic acetabular loosening identified.
Conclusions:
The novel VALS component demonstrated encouraging early survivorship with a low incidence of complications when utilised in complex acetabular reconstruction. Further studies are warranted to assess long-term survivorship.
Keywords
Introduction
As total hip arthroplasty (THA) becomes increasingly common among younger, more active patients, there is concern about an increasing burden of both complex and revision surgery. Often, surgeons are confronted with acetabular bone loss, osteoporosis, and obesity during complex (cTHA) and revision THA (rTHA).1 –3 Current projections indicate a 43–70% rise in rTHA by 2030, with a 70% increase from 2014 to 2030. 4 Thus, reliable contemporary acetabular components are warranted to address the multitude of challenges facing arthroplasty surgeons.
Historically, acetabular reconstruction in the setting of bone loss has posed challenges due to the difficulty in restoring both the structural integrity and the anatomic hip centre while achieving durable implant fixation. Early techniques were limited by inadequate understanding of defect classification, suboptimal implant designs, and the lack of biologically active materials to promote osseointegration. Severe segmental or cavitary defects often necessitated bulk allografts, which carried risks of resorption, collapse, and mechanical failure over time. Furthermore, balancing stability with restoration of bone stock – particularly in revision total hip arthroplasty – was complicated by variable defect morphology and compromised host bone, making long-term survivorship unpredictable.
Contemporary acetabular components have benefitted from manufacturing innovation and design improvements resulting in improved ingrowth surfaces, liner locking mechanisms, liner wear rates, and high stability bearing options, all helping to address common challenges faced in cTHA and rTHA. Despite these advancements, however, mechanical loosening remains a leading cause of rTHA in the United States, accounting for approximately 20% of all revisions. 5 Implant stability is critical for successful osseointegration, as micromotion as small as 150 microns can disrupt this process. 6 Recently, a porous titanium variable-angle locking screw (VALS) acetabular component has been commercialised. This design accommodates both locking and non-locking screws: variable-angle locking screws provide a fixed angle construct that may increase rigidity compared to conventional screws, potentially reducing micromotion, while non-locking screws allow compression at the bone-implant interface, which may promote bone ingrowth and improve long-term stability.7,8
This was a multicentre study involving 3 academic medical centres specialising in adult hip and knee reconstruction evaluating a novel porous titanium VALS acetabular construct. The aim of this study was to evaluate our early experience and report short-term outcomes. We hypothesised that the VALS acetabular construct would demonstrate stable fixation allowing for excellent osseointegration, and thus survivorship, during cTHA and rTHA.
Materials and methods
Study cohort
This retrospective chart review was approved through expedited review by the internal Institutional Review Board (E284). The cohort included patients who underwent cTHA or rTHA using a novel 3D-printed porous coated titanium VALS acetabular shell (REDAPT Fully Porous and Modular Shell Systems; Smith+Nephew, Memphis, TN, USA) at 3 large medical centres in the United States between November 2018 and April 2024. Revision THA was defined as any case in which the patient had a prior THA, while cTHA included patients without a prior THA who required THA in the setting of complex deformity, protrusio, prior fracture fixation, fusion takedowns, dysplasia, or previous septic arthritis (Table 1). All procedures were performed by 1 of 8 fellowship-trained arthroplasty surgeons using both direct anterior and posterior approaches based on surgeon preference. Indications for inclusion were cTHA or rTHA with confirmed implantation of the novel VALS acetabular component, as verified in both the implant log and operative report. Patients were required to have available radiographic and clinical follow-up.
Operative indications and surgical details (n = 206).
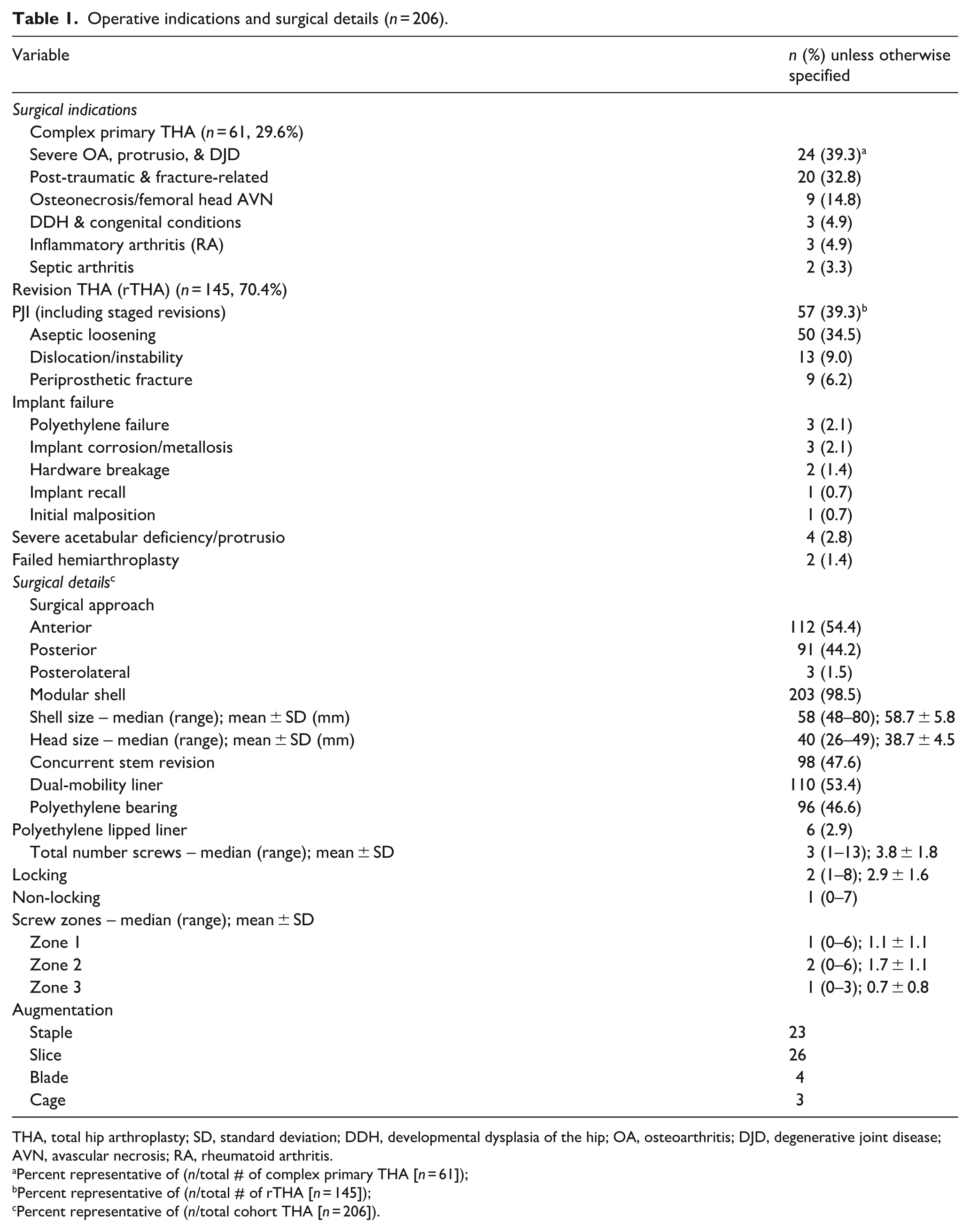
THA, total hip arthroplasty; SD, standard deviation; DDH, developmental dysplasia of the hip; OA, osteoarthritis; DJD, degenerative joint disease; AVN, avascular necrosis; RA, rheumatoid arthritis.
Percent representative of (n/total # of complex primary THA [n = 61]);
Percent representative of (n/total # of rTHA [n = 145]);
Percent representative of (n/total cohort THA [n = 206]).
The authors have extensive experience with standard non-locking revision shells, cup cage constructs and hybrid fixation techniques for complex acetabular reconstruction. The Smith+Nephew REDAPT acetabular shell was chosen as it presents a single implant solution from a single vendor that integrates porous titanium ingrowth surface for direct osseointegration and advanced fixation options including locking and non-locking screws. The length of the variable-angle locking screws ranges from 15 mm to 50 mm, with a diameter of 6.5 mm and a variable-angle lock up to 12° (included angle).
Augments were used at the discretion of the treating surgeon. The manufacturer identifies 3 different augment types in this system. The “staple” augment is “designed to allow the augment to span around a screw that is placed through the cup into the acetabulum.” It is shaped similar to a wedge-style augment with a large central cutout. The “slice” augment represents a relatively standard wedge-style augment. The “blade” augment is a 2-piece modular design augment that can be used for a “variety of pelvic anatomies.” All 3 augment types include variable-angle locking screw holes. The manufacturer recommends against drilling through these augments but rather fixing them to the acetabular cup with bone cement. The system allows either a “cup-first then augment” strategy or an “augment-first then cup” strategy.
Data collection
Relevant data, including patient demographics and hip-related characteristics, were retrospectively collected from electronic medical records (EMR). Patient demographics consisted of age, height (cm), weight (kg), body mass index (BMI), smoking status, Charlson Comorbidity Index (CCI), American Society of Anesthesiologists (ASA) classification, and indication for cTHA or rTHA. Indication for surgery, average time to follow-up calculated based on the last clinical or radiographic follow-up available in the EMR, need for subsequent revision or reoperation, indication for reoperation, and readmission within 90 days were also recorded. Revision was defined as a subsequent procedure requiring removal of the VALS acetabular shell. Surgical data collected included surgical approach, laterality, concurrent stem revision, bearing type (DM, polyethylene, lipped liners, cemented liner), shell size, femoral head size, total number and type of screws utilised (spherical and locking), zone of screw placement,1 –3,9 and use of augments and/or cages.
Radiographic analysis
Preoperative radiographic evaluation included the Paprosky grading system for acetabular bone loss, 10 as well as presence of pelvic discontinuity. Postoperative radiographs at the last recorded follow-up were evaluated for component position, signs of loosening, and/or radiolucent lines. 9 Radiographs were evaluated by 4 authors with any disagreement resolved by the senior author (BHN).
Data analyses
Primary outcomes were acetabular revision-free survivorship and all-cause reoperation. Secondary outcomes included surgical and medical complications, including infection, loosening, fracture, and readmission. Survivorship was analysed using the Kaplan-Meier curves. Patients without the event of interest at last clinical contact or lost to follow-up were censored at their most recent follow-up date, allowing them to contribute partial follow-up time while accounting for variable follow-up durations. 95% confidence intervals for survival estimates were calculated, and the number at risk was reported at predefined time points. Kaplan-Meier survival curves, descriptive statistics, including means, standard deviations, and ranges were generated in R version 4.4.2 (Vienna, Austria).
Results
The final analysis included 206 patients, comprising 61 complex primary THAs and 145 rTHAs, with a mean follow-up of 1.05 years (range 0.1–5.1 years). The mean age was 65.1 years (range 15–95 years), mean BMI was 30.9 ± 7.3 kg.m2, with 124 (60.2%) women (Table 2). 20 reoperations were identified within the cohort, 9 of which involved acetabular revision. The 1-year and 2-year acetabular component revision-free survivorship was 95% and 94%, respectively (Figure 1), with 76 and 33 patients at risk at those time points. All-cause reoperation-free survivorship at 1 and 2 years was 90% and 86%, respectively (Figure 2), with 73 and 31 patients at risk. There were 2 cases of aseptic acetabular loosening identified. Notably, a Kaplan-Meier survivorship sub-analysis of Paprosky 3A and 3B defects was performed and demonstrated 91% acetabular component survivorship at 2 years (Figure 3).
Baseline cohort demographics (n = 206).
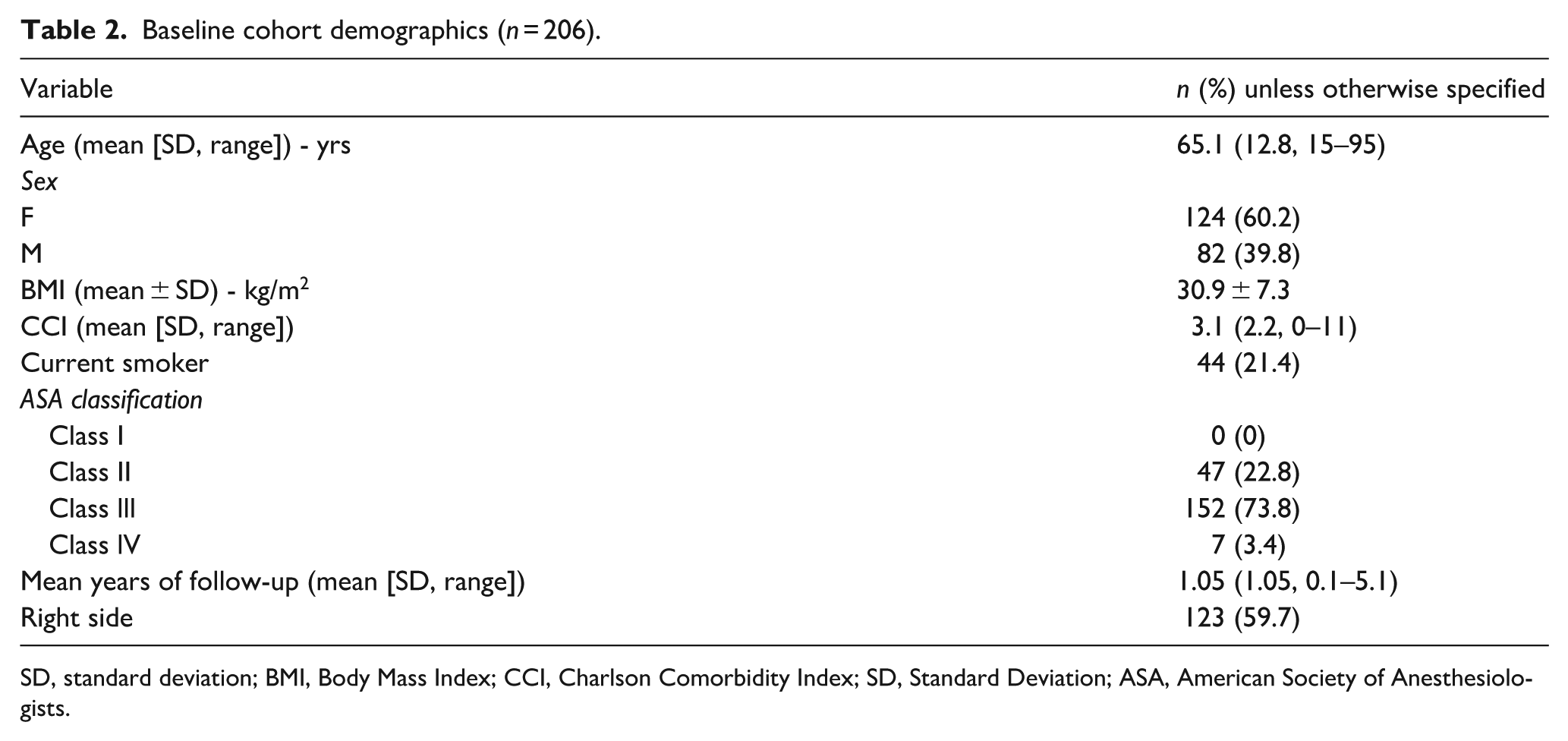
SD, standard deviation; BMI, Body Mass Index; CCI, Charlson Comorbidity Index; SD, Standard Deviation; ASA, American Society of Anesthesiologists.
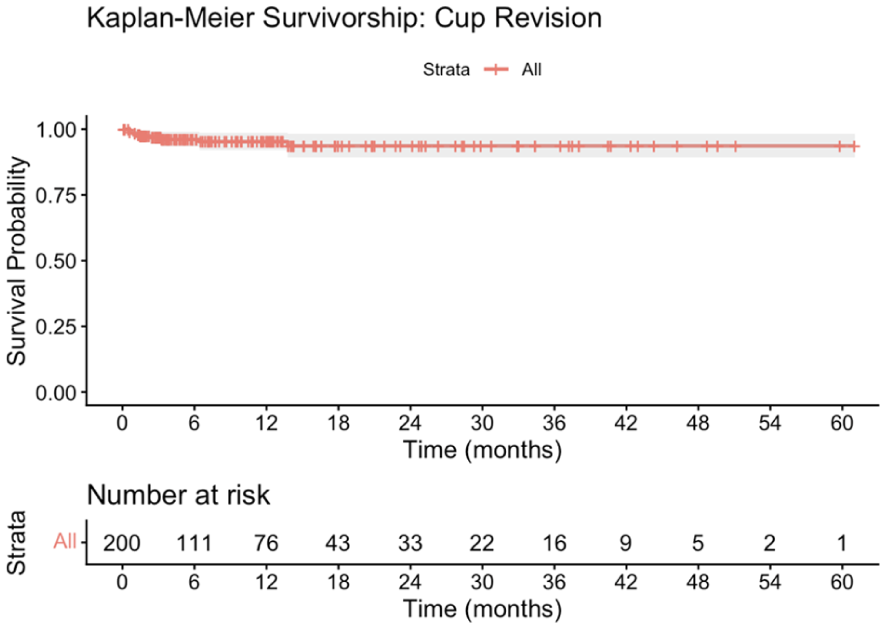
Kaplan-Meier survival curve: acetabular component revision.
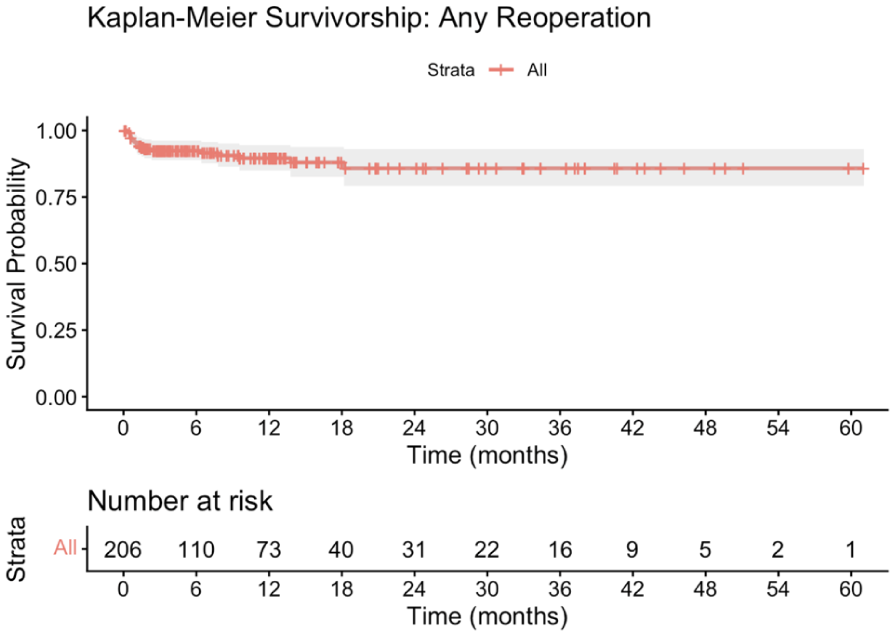
Kaplan-Meier survival curve: any reoperation.
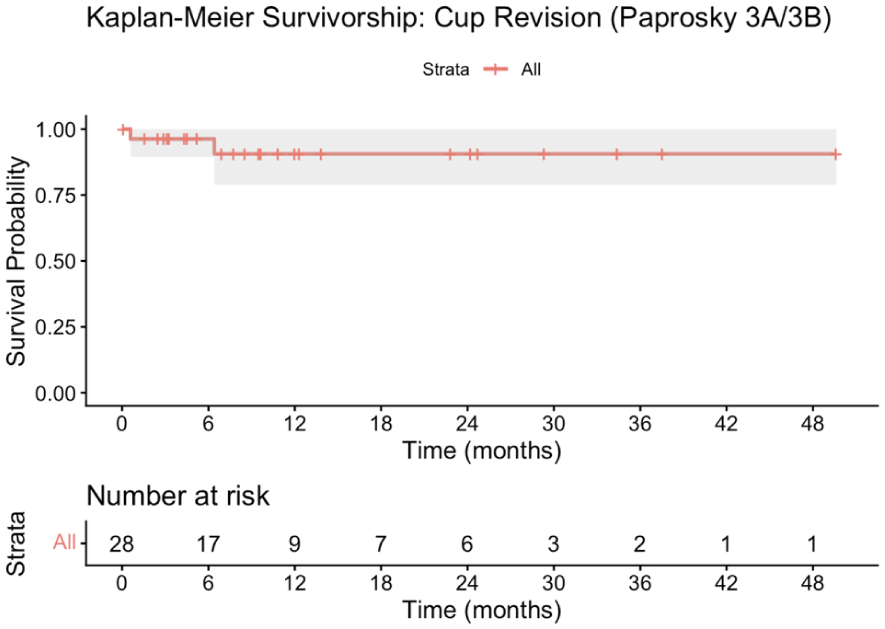
Kaplan-Meier survival curve: Paprosky 3A and 3B acetabular component revision.
Indications for the index THA and surgical details are reported in Table 1. Among cTHAs, the most common indications were severe osteoarthritis and protrusio (39.3%), post-traumatic and fracture-related (32.8%), osteonecrosis (14.8%), congenital conditions (4.9%), rheumatoid arthritis (4.9%), and previous septic arthritis (3.3%). Conversely, history of chronic periprosthetic joint infection (39.3%) and aseptic loosening (34.5%) were the leading indications for rTHA. Additional indications included dislocation/instability (9.0%), implant failure (6.9%), and periprosthetic fracture (6.2%). Acetabular defects are detailed in Table 3, including type 1 (n = 58), 2A (n = 22), 2B (n = 19), 2C (n = 17), 3A (n = 18), and 3B (n = 11) (Figure 4).
Paprosky Classification of revision cases (n = 145).
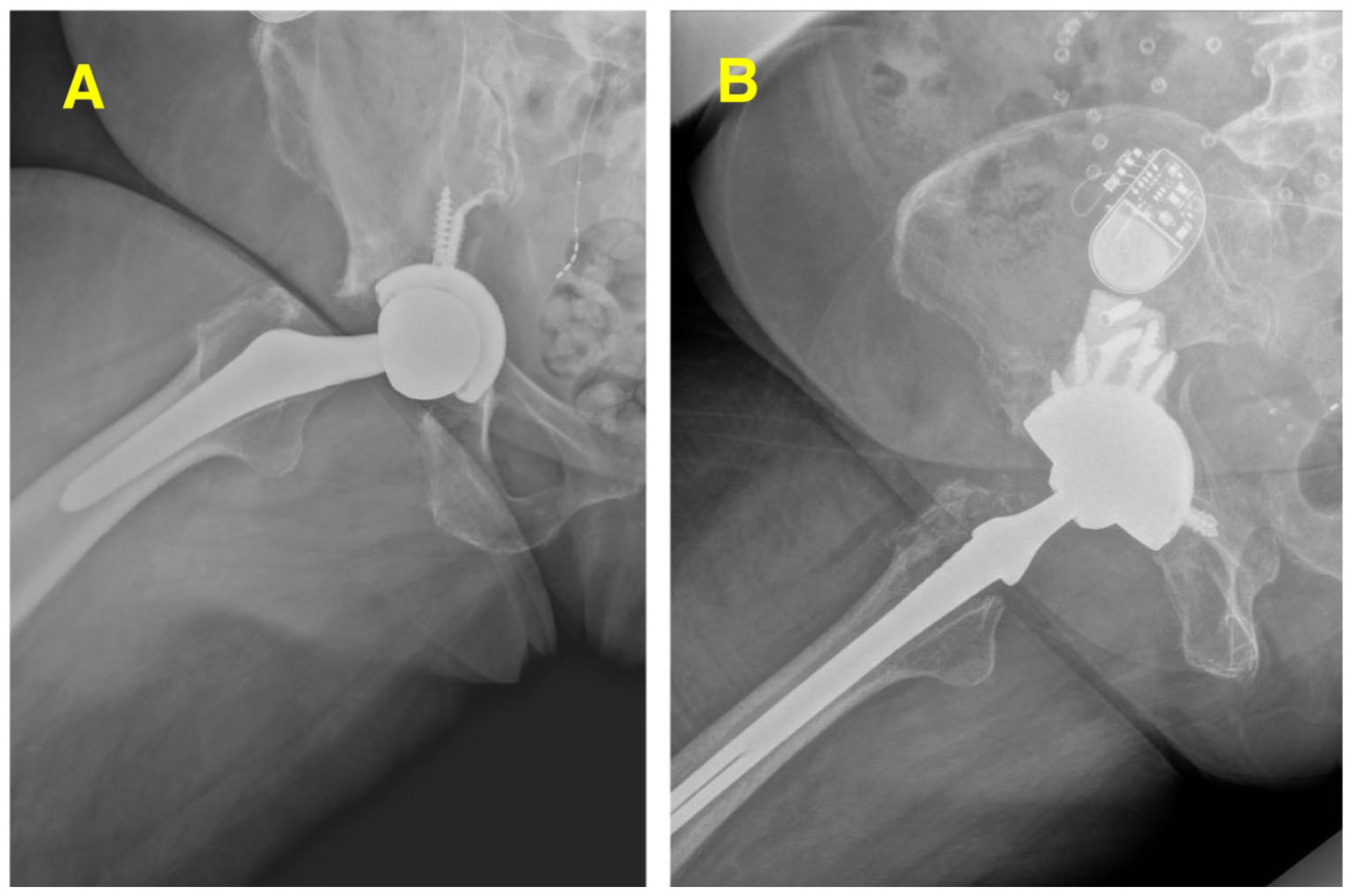
(a) Preoperative imaging of a Paprosky 3B defect. (b) Postoperative imaging of a Paprosky 3B defect managed with a novel variable-angle locking hole acetabular shell. Upon evaluating the socket, there was a mildly displaced posterior column fracture. Given fracture instability and a deficient posterior wall, the construct included a posterior superior buttress, jumbo cup, with attempted initial screw fixation to essentially act as a tri-flange without pubic fixation.
The anterior approach was used in 54.4% of cases, followed by the posterior approach in 44.2%. Modular shells were used in 98.5% of cases, with a mean shell size of 58.7 mm (range 48–80 mm). The distribution of acetabular component sizes is shown in Table 4. Concurrent stem revision was performed in 47.6% of patients, while 53.4% received a DM liner and 46.6% received a PE liner. The average number of screws used was 3.8 ± 1.8 (range 1–13), with an average of 2.9 ± 1.6 (range 1–8) locking and 1.5 ± 1.1 (range 0–7) non-locking screws. Screw placement varied across acetabular zones, with a mean of 1.1 ± 1.1 screws in Zone 1 (range 0–6), 1.7 ± 1.1 in Zone 2 (range 0–6), and 0.7 ± 0.8 in Zone 3 (range 0–3). There were 53 augments used with 3 anti-protrusio cages placed.
Distribution of acetabular component sizes.
Survivorship: acetabular component revision and all-cause reoperation
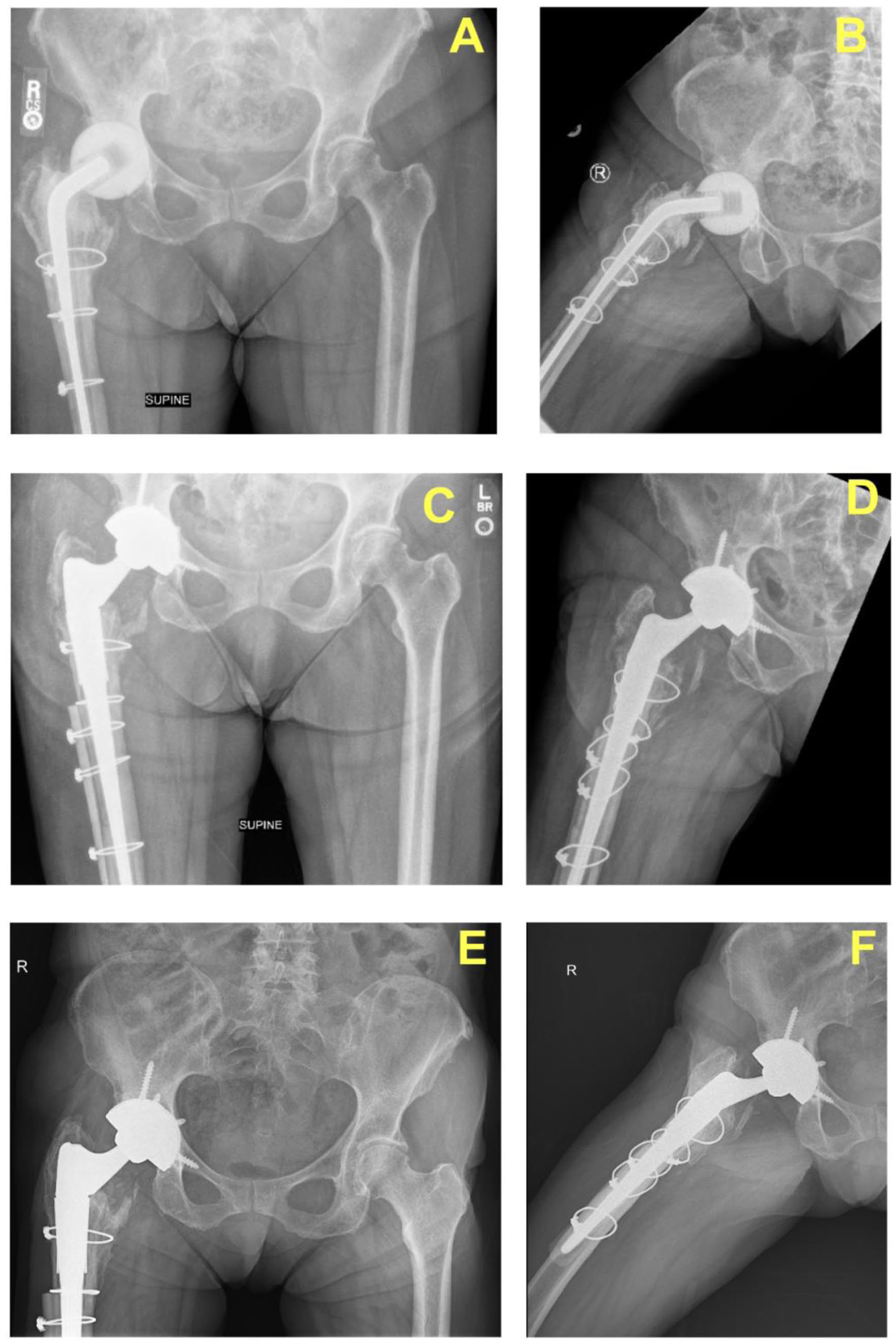
Of the 9 components explanted (4.9%) in 8 patients (Table 5), 3 components underwent resection arthroplasty for recurrent dislocations, and 3 underwent 2-stage revision for periprosthetic joint infection (PJI). 1 patient experienced aseptic loosening that resulted acutely after a fall; this was treated with successful rTHA. The fall was 40 days post-op with signs of continued component motion. Initial fixation included 3 screws, 2 in Zone 1 and 1 in Zone 2, all of which were locking (Figure 5). 1 patient underwent 2 acetabular revisions. In the index procedure, the VALS shell was fixed with multiple locking screws. The first revision occurred 18 days postoperatively for dislocation and component loosening, during which the existing construct was revised using a posterior approach with a dual DM liner, modular 58-mm cup, and porous metal augmentation (Figure 6(a) and (b)). The second revision was performed 195 days later due to a periprosthetic fracture, which necessitated a custom triflange component in the final reconstruction for enhanced stability and fixation (Figure 6(c) and (d)).
Acetabular components explanted and details.
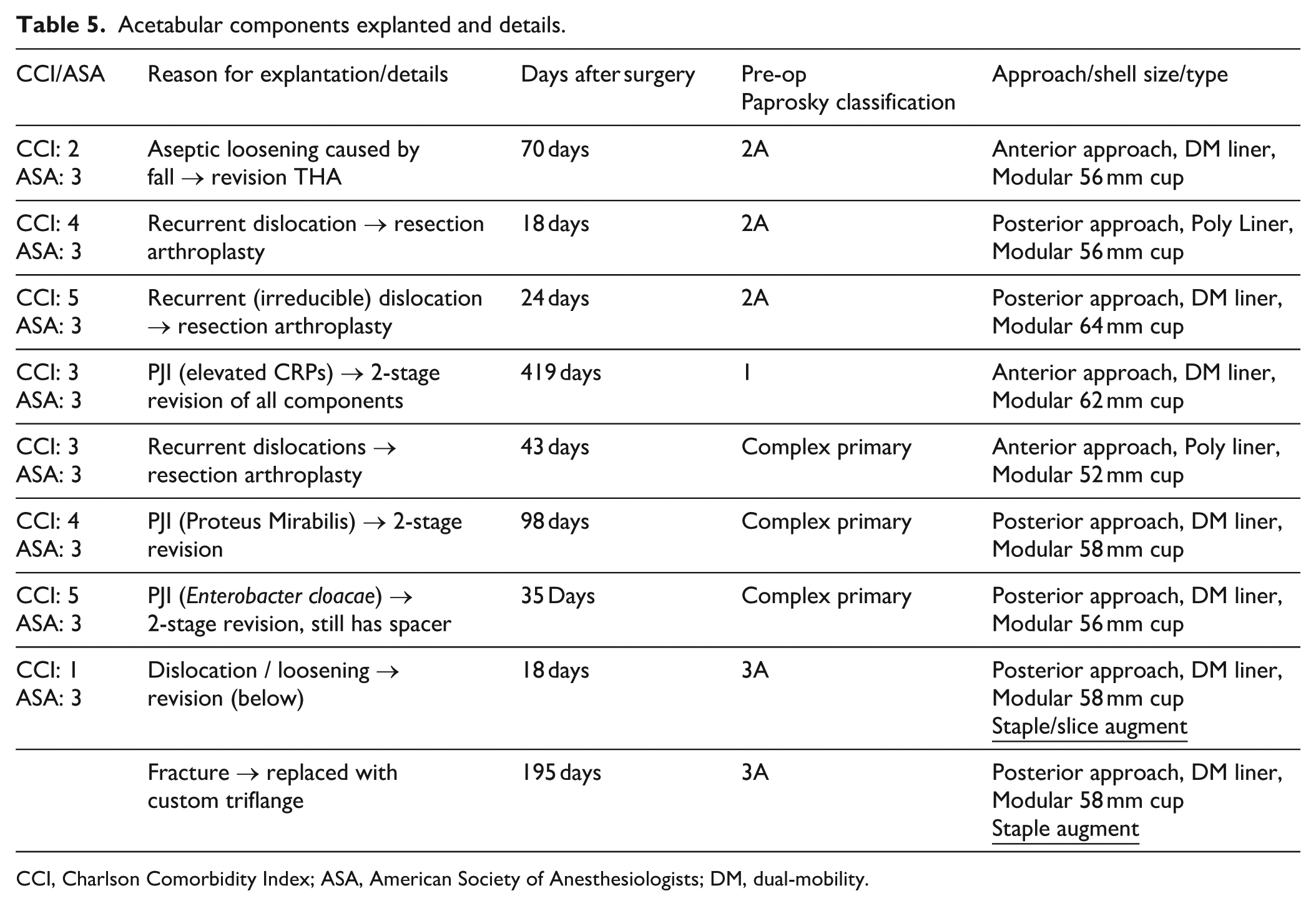
CCI, Charlson Comorbidity Index; ASA, American Society of Anesthesiologists; DM, dual-mobility.
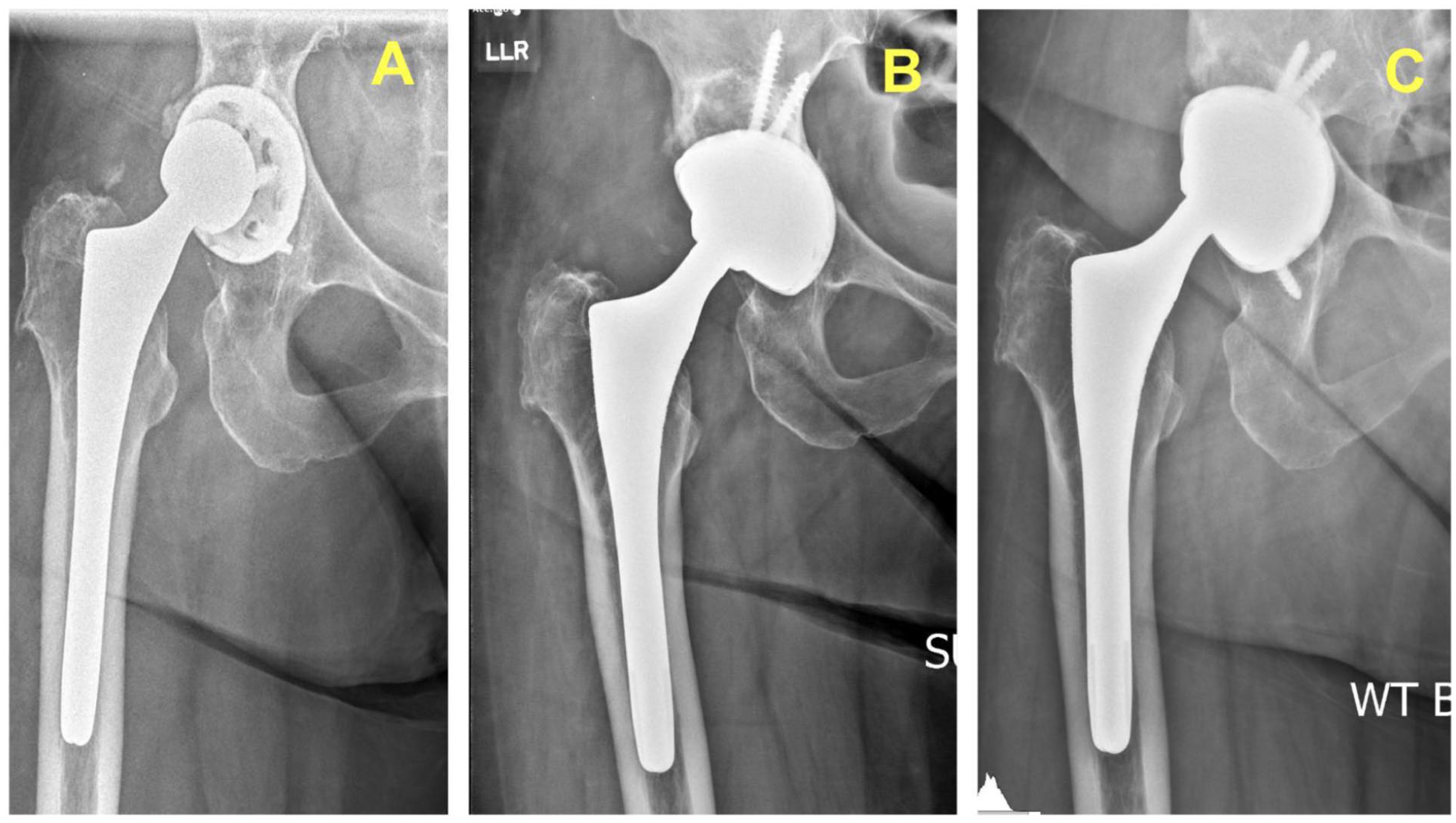
(a) Anteroposterior pelvic radiograph preoperative imaging prior to initial revision with variable-angle locking screws (VALS). (b) AP radiograph 2 weeks post VALS component implantation. (c) AP radiograph following fall from standing height.
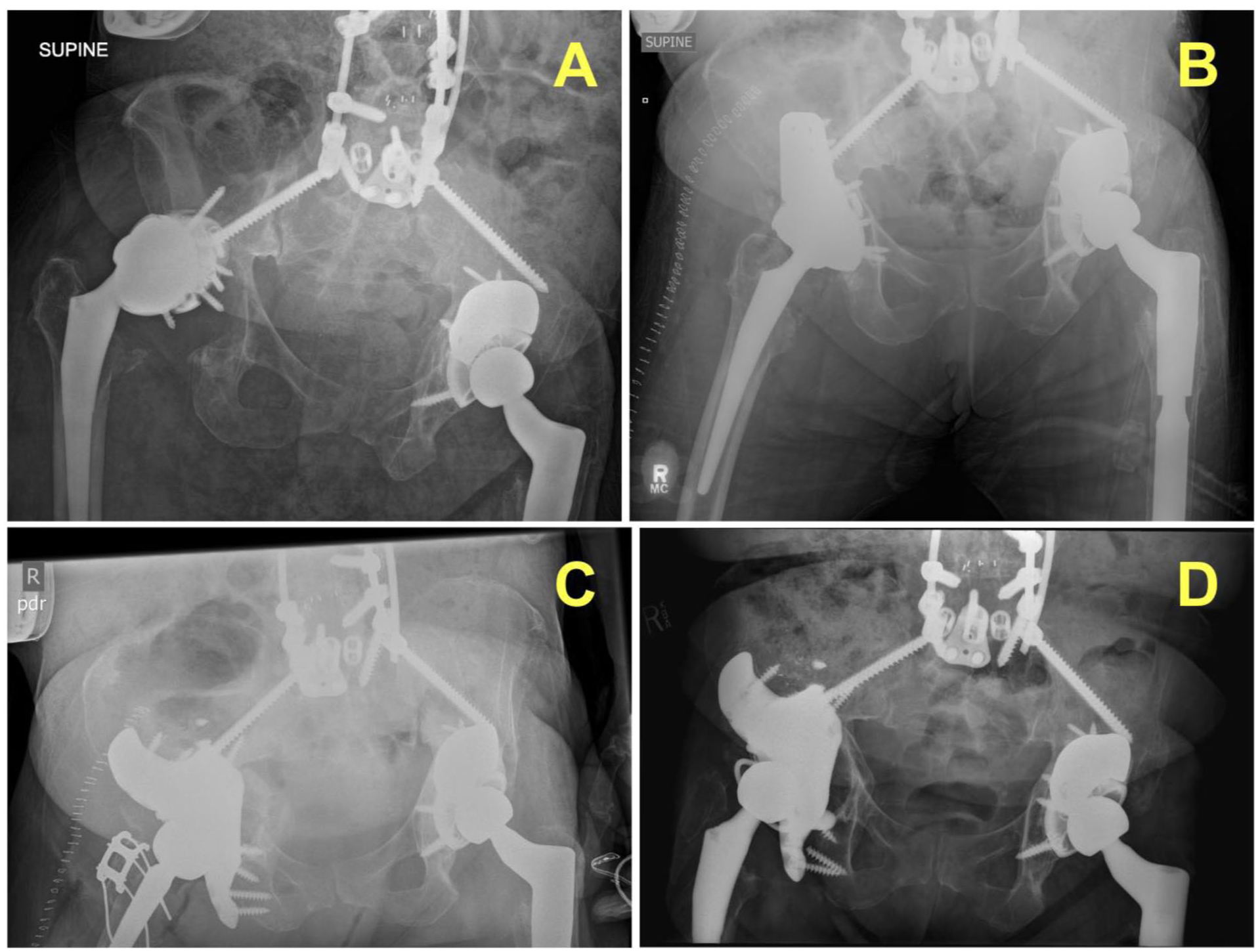
(a) Anteroposterior pelvic radiograph showing the postoperative construct following acetabular revision variable-angle locking screws (VALS). (b) AP radiograph showing right hip following revision for dislocation/loosening. (c) AP radiograph following periprosthetic fracture. (d) AP radiograph following revision for fracture.
Of the 20 total reoperations, 11 did not involve acetabular revision. These included irrigation and debridement (I&D) procedures (n = 5) for various causes: pseudotumour, superficial wound infection, seroma, and PJI. Additional reoperations were constrained liner/head revisions after dislocation (n = 3), head/liner exchange for wound dehiscence and suspected PJI (n = 2), and 1 I&D procedure with only head exchange for acute PJI (Table 6).
Non-operative/operative complications excluding acetabular component revisions (n = 29).
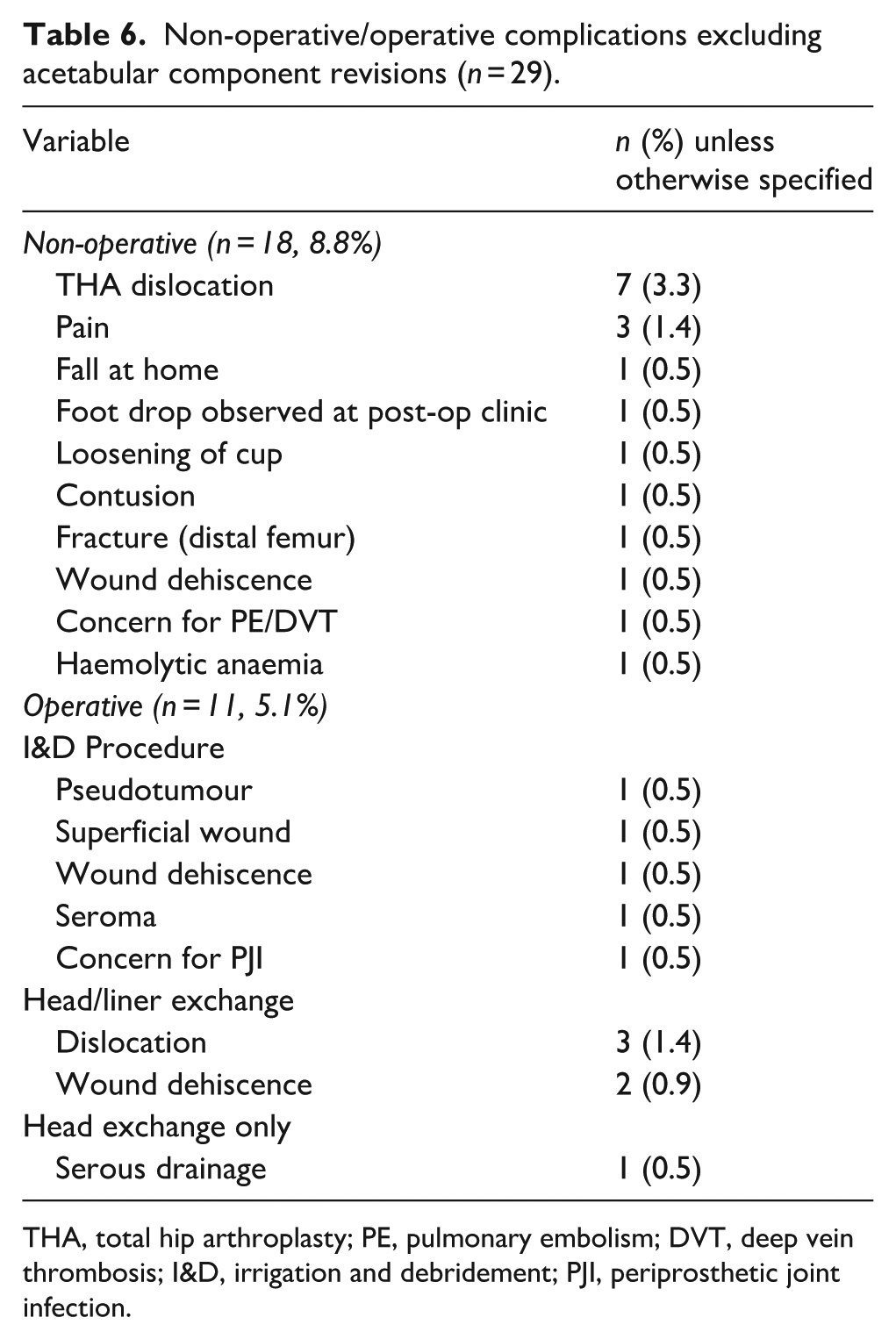
THA, total hip arthroplasty; PE, pulmonary embolism; DVT, deep vein thrombosis; I&D, irrigation and debridement; PJI, periprosthetic joint infection.
Discussion
Technological advancements in acetabular components continue to improve fixation and long-term outcomes in both cTHA and rTHA. Highly porous metals, such as titanium, have demonstrated excellent mid-term to long-term survivorship, even in the setting of substantial bone loss, by enhancing osseointegration and achieving stable fixation.11 –13 Despite these improvements, very few studies have evaluated modern acetabular components that include nascent acetabular component locking screw technology, which may provide additional stability in challenging reconstructions.11,12,14 –20
The present cohort included both complex primary THA (cTHA) and revision THA (rTHA), which differ in underlying pathology and surgical considerations. Revision cases often involve additional challenges such as removal of prior implants or hardware and management of prior infection. However, both groups frequently present with similar reconstructive challenges, particularly acetabular bone loss requiring stable fixation. Surgical indications were reported separately for cTHA and rTHA (Table 1). In our series, cTHA most commonly involved severe osteoarthritis with protrusio or post-traumatic/fracture-related deformity, whereas rTHA was most frequently performed for chronic periprosthetic joint infection and aseptic loosening. Despite the differences in indication and morphology, both situations may benefit from locking screw fixation, which can improve rigid fixation and reduce micromotion. Given the relatively small cohort sizes, these groups were analysed together to evaluate the overall performance of the VALS acetabular construct in complex acetabular reconstruction, and the implant demonstrated reliable fixation across both settings. This combined analysis introduces heterogeneity in patient pathology, surgical complexity, and baseline risk profiles, which may influence survivorship outcomes and limit direct interpretation of implant performance across these groups.
To date, our study is the largest cohort of revision and complex acetabular reconstruction using a porous titanium VALS acetabular component. The 2-year survivorship for acetabular component revision was 94%, which compares favorably to historical loosening rates in rTHA, and aligns with previously reported survivorship for porous titanium designs.11,12 Notably, even in cases with severe bone loss (Paprosky 3A and 3B defects), survivorship was 91% at 2 years, demonstrating the potential of this construct in the most complex reconstructions. However, revision-free survivorship may underestimate overall failure, as several complications were managed without acetabular component revision.
Previous studies on porous titanium acetabular components have explored the outcomes of this innovation; for example, Berlinberg et al. 11 reported an 88% survivorship free of acetabular shell revision at 2 years in a multicentre cohort of 68 revision cases using a porous titanium acetabular shell. Recently, Braun et al. 12 reported 99% survivorship free of acetabular shell revision, with a 9.7% reoperation rate in 103 cTHA and rTHAs. In a single institution study of 59 hip arthroplasty revisions, Shaarani et al. 21 achieved early fixation with a 3D-printed porous coated titanium VALS acetabular shell, with only 2 shell migrations, and 1 revision of the liner. Other studies using different porous titanium designs have also demonstrated favorable short-term outcomes. Using the Tritanium cup (Stryker, Mahwah, NJ), a highly porous titanium-coated multi-hole shell, Hosny et al. 20 observed a 98.4% aseptic survivorship at a mean follow-up of 87.6 months in 62 revision THAs. Geng et al. 22 reported a 99.1% survivorship at a minimum 2-year follow-up with a 3D-printed fully porous titanium trabecular shell, while Delanois et al. 23 observed a 97% aseptic survivorship at 5 years using highly porous titanium shells in revision THA.
Our complication profile aligns with prior reports of cTHA and rTHA using porous metal components. Despite the high-risk nature of our cohort, the observed acetabular revision for PJI (1.4%) and aseptic loosening (0.5%) rates were lower than those previously reported, while instability rates (1.9%) were similar.11,12,23,24
Collectively, these studies demonstrate that modern porous titanium acetabular components achieve excellent survivorship in both cTHA and rTHA. Our findings further support the durability of this technology, particularly when combined with VALS in Paprosky 2B and greater acetabular defects. Figure 7 shows a case of a Paprosky 2B acetabular defect treated with the VALS construct and 4 locking screws. The implant demonstrated stable fixation at 45 months despite a complex pre-implantation clinical course including periprosthetic fracture and infection.
Representative case of revision total hip arthroplasty using a variable-angle locking screw (VALS) acetabular component. The patient had a history of periprosthetic fracture requiring ORIF, followed by periprosthetic joint infection managed with 2-stage revision, resulting in substantial bone loss. At 45 months after VALS component implantation, radiographs demonstrate stable fixation without evidence of loosening.
We identified several surgical techniques that may optimise the use of this implant. First, the use of locking screws may help optimise initial stability and reduce micromotion, which could theoretically enhance osseointegration. 7 In our experience, the combination of a press fit, high friction porous surface, and rigid VALS construct provides stable fixation. While advances in implant design have improved survivorship of contemporary acetabular components, the addition of locking-screw technology may offer a further advantage in rTHA. 11 We achieved excellent survivorship despite using fewer screws on average (3.8 ± 1.8 per case; 2.9 ± 1.6 locking, 1.5 ± 1.1 non-locking) than reported by Braun et al. 12 (5.5 ± 1.74 total; 3.4 ± 2.4 locking, 2.0 ± 1.7 non-locking) and Berlinberg et al. 11 (median 4 screws). When used, a non-locking screw may provide further cup-bone compression, followed by the addition of at least 1 locking screw. However, many cases utilized locking-screw fixation only. The authors recommend an initial iliac screw without fully seating and locking, followed by locking ischial fixation, and finally locking the initial iliac screw. This sequence helps to avoid cup spinout when locking the screw, particularly in tenuous acetabular defects.
Limitations
This study has several limitations. This study represents our early experience with a novel acetabular reconstruction system in the setting of both complex primary and revision THA, with relatively short follow-up and a retrospective design that introduces potential selection bias. The heterogeneity of anatomy findings in both groups, the relatively short follow-up period, and the significant number of options present within the acetabular system itself make a comparative analysis between cTHA and rTHA both difficult and potentially misleading. Therefore, this analysis was not performed, which limits interpretation of implant performance across these cohorts. The retrospective design introduced inherent bias, particularly selection bias. However, no patients who received the novel 3D-printed cup and had any postoperative follow-up were excluded for any reason. 13 patients were excluded from analysis due to loss to follow-up or incomplete records, including 3 who died prior to first follow-up, 4 with no postoperative radiographic or clinical documentation, 3 without accessible electronic medical records, and 3 lacking a documented operative note. We also did not perform a comparative analysis of our patient demographics, complications, and other descriptive statistics. Additionally, all patients with postoperative imaging and evaluation were included regardless of follow-up duration. While Kaplan-Meier analysis allows inclusion of patients with varying follow-up through right-censoring, it assumes non-informative censoring. Also, radiographic assessment was performed internally by 4 authors with discrepancies resolved by the senior author. The internal nature of review may introduce observer bias in the reported radiographic results. Finally, surgical techniques, including approach, screw insertion type and sequence, and bone void filling varied by surgeon.
Conclusion
The use of a novel porous-coated titanium VALS acetabular component in complex and revision THA exhibited encouraging early survivorship with a low risk of revision, even in Paprosky 3 defects, at early follow-up. Stable fixation was achieved using a combination of locking and non-locking screws, supporting the versatility of this construct in cTHA and rTHA. Further research, including prospective trials and mid- to long-term follow-up, is needed to further understand the potential advantages of this construct compared to other traditional revision acetabular components.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.