
Abstract
Aim:
The evaluation of the incidence of symptomatic upper limb venous thrombosis (ULVT) associated with midline catheters in patients admitted to the hospital.
Methods:
The frequency of symptomatic ULVT diagnosed in a group of patients with midline catheters confirmed by sonographic examination in hospitalised patients at Faculty Hospital over the period of 1 year.
Results:
Four hundred thirty-nine midline catheters were inserted in 430 patients (250 women and 180 men) during year 2015. Nine patients had two midline catheters. The average age of the patient was 68 years (range: 19–96 years). The median time of midline catheter introduction into a vein was 10 days (range: 1–112 days). Symptomatic thrombosis was diagnosed in 20 patients (4.5%), 3.3/1000 catheter days. It was associated with gender (male) and midline insertion in the cephalic vein.
Conclusion:
The risk of upper limb symptomatic thrombosis associated with midline catheters during a stay in the hospital should be taken into consideration when indicating optimal venous access.
Introduction
Midline catheters are indicated if peripheral venous access is expected to stay in place longer than 5 days or when visible or palpable superficial veins are not available. Peripheral venous access is indicated for infusing non-vesicant or irritant drugs, drugs with pH between 5 and 9 and drugs or solution with osmolarity of 800–900 mOsm. 1 Midline catheters may be used for months, if used in an appropriate way (mainly with regard to the type of infusates).2,3 However, during their stay in veins, complications like catheter dislocation, occlusion, infection and upper limb venous thrombosis (ULVT) may appear. 3
Ultrasound guidance is very useful in the selection of the appropriate vein, as well as for reliable insertion catheter insertion. Midline catheters may be inserted under sonographic navigation in the middle part of a deep vein. 3
Thrombosis is a multifactorial event, and its occurrence depends on congenital dispositions, the character of the underlying disease, the applied treatment and so on. In the case of catheter insertion, thrombosis is related to the ratio between the size of catheter and vein, to the number of attempts to enter the vein before successful insertion, to the type of securement used for catheter stabilisation and to the type of infusates administered through the catheter. 1
The risk of the ULVT in the literature is evaluated mainly in association with peripherally introduced central catheters (PICCs).3–5 According to previous reports, ULVT prevalence in midline catheters is lower in comparison with PICCs.6–8 but there is only a limited number of prospective studies providing this comparative information. 9 Therefore, the aim of the present study was to evaluate the incidence of symptomatic ULVT in hospitalised patients with the insertion of midline catheters prospectively.
Patients and methods
All the adult patients (18 years and older) admitted to the hospital and sent for the insertion of midline catheters to the Vascular Access Team of Faculty Hospital Prague Motol, Czech Republic in the year 2015 participated in the study. The patients were referred by the physicians of both surgical and medical departments according to the hospital guidelines.
Insufficient peripheral access or the necessity of a venous line for more than 5 days was considered to be an indication for midline catheter insertion. Midline was selected provided no irritant or vesicant drugs had to be introduced into the central line and if the pH of all the drugs and infusates given to the patients was between 5 and 9 and their osmolarity did not exceed 800 mOsm. 1 The catheters were removed when they were not needed any more or in case of complications. If the application of medication or infusates was indicated into the central line, a midline catheter was substituted for the central line (central venous catheter or PICC) in order to avoid its inappropriate use. Before the catheter insertion, the most appropriate vein in the middle part of the right or left arm was detected using sonographic examination. Usually, the vein with the largest diameter was selected. A 4 French (4F) 20-cm-long midline catheter was introduced (Medcomp, Harleysville, PA, USA). The procedure was contraindicated if no vein with a diameter of at least 4 mm was present. The midline 20 cm catheter insertion was performed in the mid-upper arm without any change in catheter length. The catheter was not placed into a paretic or plegic arm or if any pathological changes interfered with catheter insertion (e.g. fracture, lymph node enlargement due to cancer metastasis).
After disinfection of the puncture site and local anaesthesia, catheters were introduced under on-line sonographic navigation using the modified Seldinger method. At the end of procedure, a midline catheter was stabilised using fixation with Stat Lock (Bard Access System, Salt Lake City, UT, USA), properly flushed with saline using a 20 mL syringe. If the site of catheter entry was free from bleeding and the patient did not have a history of allergy, a combined chlorhexidine gel and film dressing for the insertion site was the first choice. Dressing changes were completed every 7–10 days. However, if bleeding or allergy was evident, a combination dressing was used consisting of 0.2% polyhexamethylene biquanide and film dressing. In this case, the dressing was changed after 24 h and substituted for a transparent dressing. The team also acknowledged that the issue of appropriate patient care following midline catheter insertion is important to ensure patient safety. Nursing staff in wards was regularly instructed on how to care for these catheters. The vein where midline catheter was inserted, its diameter, number of punctures used for catheter introduction, age, gender of patients, the duration of midline catheter placement in vein and presence of ULVT were recorded.
Symptoms of thrombosis due to midline catheter insertion were upper limb pain on the side of catheter insertion, arm swelling and its tenderness. In case of any symptoms suspicious of thrombosis, sonographic examination was indicated in order to confirm the correct diagnosis.
Sonographic examination
Two-dimensional (2D) scanning with compression testing, colour Doppler flow and pulsatility and variation with physiological manoeuvres were used in order to detect the existence of thrombosis. The diagnostic criteria were as follows: (1) loss of compression of imaged vein walls when pressure is applied on the skin during real-time imaging; (2) visualisation of echogenic material in vein; (3) blood flow defect in colour Doppler imaging; (4) loss of reduction of Doppler velocity spectrum changes and (5) reduction of disappearance of pulsatility and variation with physiologic manoeuvres (e.g. rapid inspiration). The examination was done by one experienced physician using a machine with a 8 MHz linear probe.
We evaluated the association of symptomatic thrombosis with the selected vein where midline insertion occurred, its size, number of punctures used for vein entry, age of patients, gender and number of days from catheter insertion until a diagnosis of thrombosis was achieved.
Statistical evaluation
Descriptive statistics for characterising the study population and midline-related thrombosis were used. The significance of the selected parameters of ULVT in association with midline catheters was analysed by Cox proportional hazard model. Age, gender, the selected vein, size of the vein, number of punctures during insertion and number of days since insertion until ULVT diagnosis were evaluated as independent predictors of ULVT.
Results
Four hundred forty-eight patients were indicated for midline catheter insertion in the year 2015. Eighteen patients (4%) were contraindicated, because no suitable vein was detected in both arms. Four hundred thirty-nine midline catheters were inserted in 430 patients (250 women and 180 men). Nine patients had two midline catheters. The median age of the patients was 68 years (range: 19–96 years). Total number of catheter days was 5963. The median time of midline catheter introduction into a vein was 10 days (range: 1–112 days). Sixty-nine patients died during admission (16%).
The catheter was introduced into the brachial vein in 219 (50%), into the basilic vein in 186 (42%) and into the cephalic vein in 34 (8%) insertions. One puncture to enter the vein was needed in 325 (74%), two punctures in 69 (16%) and three or more punctures in 45 (10%) cases. Three hundred seven (70%) midline catheters were used for more than 5 days. The size of the vein was at least 4 mm and 4F midline catheters were used in all the patients. The average size of the selected vein was 5.0 ± 0.5 mm.
ULVT developed in 20 patients (4.5%). The association of symptomatic thrombosis with age, gender, number of punctures, the selected vein and its diameter is summarised in Table 1. ULVT was present in 13 out of 325 patients (4%) if only one puncture was needed for catheter insertion. If the patient received two or more insertion attempts, the incidence increased to 6.4% (7 out of 107 patients) and in case of three or more attempts to 9% (4 out of 45 patients).
Comparison of midline catheters associated with and without symptomatic upper venous thrombosis.
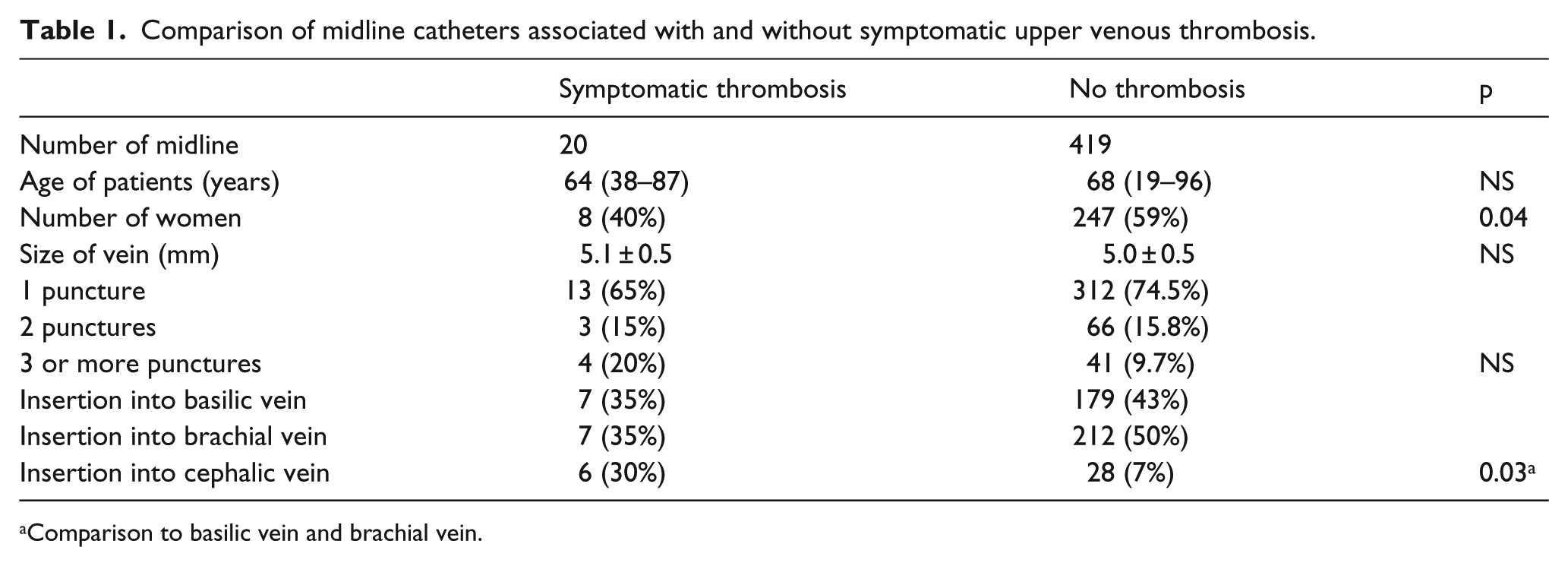
Comparison to basilic vein and brachial vein.
ULVT was diagnosed the first week after insertion in 10 patients, the second week in 4 patients and after 2 weeks in 6 patients. Number of days of midline introduction was not associated with the presence of ULVT. Out of 20 patients with ULVT, 12 patients presented with upper limb pain only (2.7%), another 2 had upper limb pain with leaking (0.5%) and 6 had arm swelling and tenderness (1.3%).
Discussion
According to previous reports, the prevalence of ULVT associated with midline catheter insertion is lower than with PICC and is below 2%.2,6,8 This conclusion is supported by retrospective studies or by the relatively small group of examined subjects. In the recent retrospective study, the incidence of ULVT associated with midline catheter insertion was 1%, but another 1.5% of patients reported upper limb pain and another 1% leaking. 9 However, it is not clear if ULVT was confirmed or ruled out by sonographic examination. It is important to note that 12 out of 20 patients with ULVT in our observation complained of upper limb pain only; another two patients complained of upper limb pain with leaking. Arm swelling and tenderness was detected only in six patients.
The prevalence of thrombosis depends on the precision of the catheter insertion and the disposition of the patient. The presence of the symptomatic ULVT in our patients was not associated with the diameter of the vein, where the catheter was inserted as far as the midline insertion was contraindicated and when the vein diameter was below 4 mm. The number of punctures needed during the insertion of the midline catheter has not been significantly associated with ULVT, although a tendency for its higher rate with two and even three or more punctures was evident. The rate of symptomatic ULVT was increased with the selection of the cephalic vein. It was already reported in PICCs and may be attributed to the angle of its connection to the subclavian vein. 10 The rate of ULVT was also higher in men. This finding was reported previously in PICC complications, but its explanation is not clear. 11
The prevalence of thrombosis is influenced by the patient’s morbidity. The high mortality rate in our group demonstrates that midline catheters were applied to the very seriously ill patients. These patients may have a higher risk of different types of complications, including the development of thrombosis. Unfortunately, we have not defined the risk of comorbidity parameters related to ULVT before starting our project, because we expected the very low incidence of ULVT.
We have tried to follow the recommended guidelines for the application of peripheral lines; however, we cannot rule out the application of some drugs inappropriate for peripheral use in wards despite informing the medical and nursing staff.
The distal end of the midline catheter should be located in the axillary vein according to the definition of the Infusion Nursing Society. When a 20-cm-long catheter is inserted in the mid-upper arm, the terminal position of the catheter may reach the subclavian vein. The previous reports described the significantly higher risk of thrombotic complications in central venous catheters if the distal part of the catheter was placed in the subclavian or innominate vein.12–14 However, there is no evidence in the literature for an increased risk of ULVT when tip of the midline catheter is in subclavian vein, if only peripherally compatible solutions are infused.
Conclusion
The insertion of midline catheters in our group was associated with a 4.5% incidence of symptomatic ULVT. The comparison of this figure with the incidence of ULVT associated with PICCs.3–6 in recent studies raised the question whether midline catheter has really the lower risk of ULVT. The same size of the inserted midline catheter and PICC in the arm vein should have the same impact on flow reduction, and the position of the distal part of catheter in the axillary or subclavian vein most likely does not protect the patient from thrombosis formation more than its position in the cavoatrial junction.
The negative consequences of ULVT may be limited using a shorter midline catheter (8 cm, mini-midline). According to a recent report, this type of midline catheter may be easily inserted and has also very low risk of complications from infections. 15
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
This study was supported by Ministry of Health, Czech Republic – conceptual development of research organisation, University Hospital Motol, Prague, Czech Republic 00064203.