
Abstract
Patients with end-stage kidney disease are at increased risk of death from coronavirus disease 2019 (COVID-19). In addition, severe COVID-19 has been associated with an increased risk of arterial and venous thromboses. In this report, we describe the case of a hemodialysis patient who developed an otherwise-unexplained thrombosis of an arteriovenous fistula during a symptomatic COVID-19 infection. Despite prompt treatment with three technically successful thrombectomies along with systemic intravenous heparin and two rounds of catheter-directed thrombolysis with tissue plasminogen activator, the fistula rapidly re-thrombosed each time and he required tunneled dialysis catheter placement. He subsequently required admission for hypoxemia from COVID-19 pneumonia and ultimately developed a catheter-related blood stream infection that likely contributed to his death. As the fistula had been previously well functioning and no angiographic explanation for the thrombosis was found, we speculate in this case the recurrent thromboses were related to the hypercoagulable state characteristic of severe COVID-19. Interventionalists performing hemodialysis access procedures should be aware of the prothrombotic state associated with COVID-19 and should consider it when deliberating how to best plan and approach access interventions in patients with symptomatic COVID-19.
Keywords
Introduction
Patients with end-stage kidney disease (ESKD) are at increased risk of morbidity and mortality from coronavirus disease 2019 (COVID-19), with short-term death rates reported at approximately 30% across multiple cohorts worldwide.1–3 In addition, COVID-19 is associated with a hypercoagulable state and increased risk of thrombosis,4,5 but whether COVID-19 in ESKD patients contributes to an increased risk of thrombosis of hemodialysis access is unknown. Herein we describe a case report of a hemodialysis patient who developed an otherwise unexplained thrombosis of his arteriovenous fistula (AVF) that proved refractory to thrombectomy early in the course of a severe COVID-19 infection.
Case description
A 45-year-old man with ESKD from IgA nephropathy on hemodialysis, hypertension, tobacco use, and severe renal osteodystrophy with left femoral neck fracture 3 months prior presented to outpatient hemodialysis with fever and cough and was diagnosed with COVID-19 with a PCR of a nasal swab. Four days later, the patient experienced thrombosis of his right wrist radiocephalic AVF. The AVF had been created in 2008, and he had initially experienced recurrent thrombosis of the AVF requiring surgical revision in 2013, followed by stenting of a recurrent juxta-anastomotic inflow stenosis with a bare metal stent in 2014. Following the revision and stenting, the patient did not experience any further episodes of thrombosis but did require angioplasty of in-stent restenosis twice in 2016 and 2018. The AVF had been functioning well since his last procedure in 2018. His chronic outpatient medications included aspirin 81 mg daily but no other antiplatelet or antithrombotic agents.
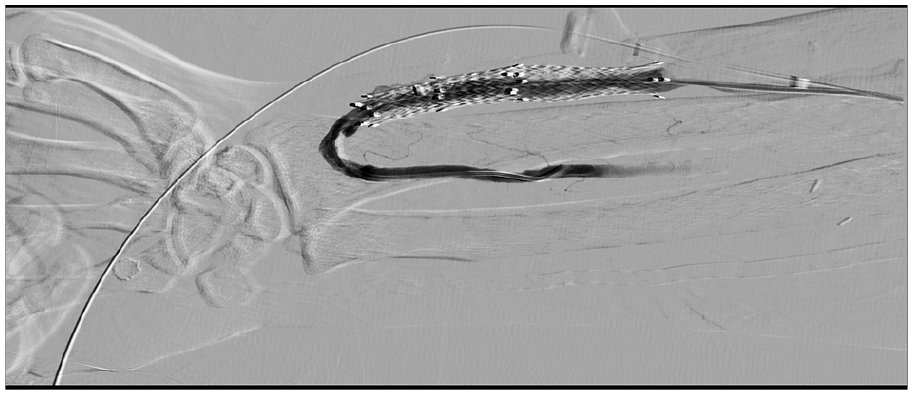
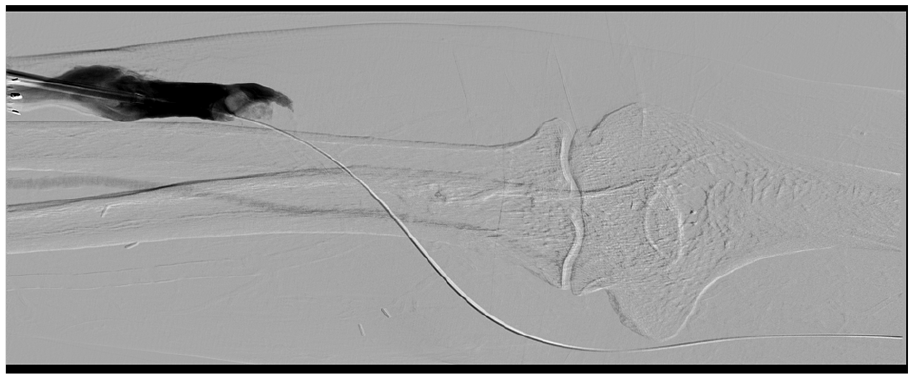
Upon diagnosis of the current thrombosis, the patient was immediately taken for attempt at percutaneous AVF thrombectomy. The AVF was accessed in the venous facing direction with a seven-French introducer sheath placed just beyond the outflow of the juxta-anastomotic stent. A Kumpe access catheter (Cook Medical LLC, Bloomington, IN) was advanced over a guidewire to the central circulation and confirmed patency of the central vasculature. A pullback venogram was then performed via the Kumpe catheter, confirming presence of thrombus beginning in the basilic vein outflow at the antecubital fossa. The upper arm basilic vein was noted to be patent. Following this, 2 mg of tissue plasminogen activator (tPA) were injected into the thrombus at this location to lyse the thrombus, after which an 8-mm Dorado angioplasty balloon (Bard Peripheral Vascular Inc., Tempe, AZ) was advanced to the location of the outflow thrombus and inflated to macerate the thrombus. Interestingly, there was no waist seen on the balloon prior to full effacement, and angioplasty was repeated within the AVF to the location of the venous-facing sheath, again without any significant waist seen indicating a lack of mechanical AVF outflow stenosis to account for thrombus formation. Following thrombus maceration, a second six-French introducer sheath was then placed facing the radial artery. A guidewire was easily advanced across the arterial anastomosis, after which an over-the-wire Fogarty catheter (Edwards Lifesciences Corp., Irvine, CA) was advanced, with balloon inflation and thrombectomy sweep performed with a small amount of hard fibrin plug aspirated through the arterial-facing sheath. A thrill could immediately be palpated in the AVF following thrombectomy sweep, and an arteriogram was then performed via the Fogarty catheter in the radial artery demonstrating restoration of flow via the AVF (Figure 1). Residual thrombus was noted just beyond the inflow stent and this was swept to the arterial-facing sheath with the Fogarty balloon and aspiration, followed by repeated angioplasty in the AVF toward the central circulation to evaluate for any residual stenosis, none of which was encountered. The patient had a strong thrill for approximately 30 s following these maneuvers, after which no thrill could be palpated. A repeat angiogram revealed rapid re-thrombosis of the AVF outflow beginning just beyond the inflow stent without flow seen into the upper arm basilic vein (Figure 2). Immediately, an additional 2 mg of tPA were injected through the venous-facing sheath to lyse the new thrombus, and the patient received a 5000-unit bolus of heparin through a peripheral IV. The Fogarty catheter was then advanced via the venous-facing sheath, inflated, and pushed easily without resistance toward the central circulation to clear out residual thrombosis, after which patency was briefly restored, with a small non-obstructing thrombus seen in the upper arm basilic vein central to the antecubital fossa. Repeat sweeping was then performed, following which the patient maintained a strong thrill for approximately 1 min, after which no further thrill could be palpated. The thrombectomy procedure was then repeated for a third time, once again with strong thrill following the procedure and minimal AVF stenosis encountered. Patency was confirmed again on post-procedure angiogram and greatly diminished upstream thrombus was noted (Figure 3). The AVF was monitored for approximately 5 min following the final thrombectomy, after which a strong thrill remained present. The introducer sheaths were then removed, and hemostasis achieved with Vicryl suture placement. Approximately 5 min after sheath removal, his AVF again thrombosed. Given the rapid re-thrombosis following all three thrombectomy attempts despite aggressive anticoagulation and a lack of a typical mechanical outflow stenosis to account for the thrombosis, it was felt that his fistula was most likely failing due to COVID-19-induced hypercoagulability. As further attempts at thrombectomy were felt unlikely to be successful, the AVF was abandoned. As both internal jugular veins were found to be chronically thrombosed, ultimately a right femoral tunneled hemodialysis catheter was placed, with plan for new AVF creation or surgical AVF revision after recovery from COVID-19. Of note, no laboratory studies (coagulation studies or otherwise) were obtained in the setting of his AVF thrombosis or the attempted thrombectomy.
Arteriogram demonstrating restoration of flow after first intervention, including lysis with tissue plasminogen activator, angioplasty, and thrombectomy sweep.
Re-thrombosis of arteriovenous fistula outflow after first thrombectomy.

Angiogram demonstrating restoration of patency and diminished upstream thrombus after the third thrombectomy.
Seven days later, the patient was admitted for 2 days with hypoxemia, multifocal pneumonia, and hyperkalemia requiring urgent dialysis. Admission labs included a normal platelet count of 206,000/μL, normal prothrombin time of 12.1 s, and elevated C-reactive protein of 4.6 mg/dL. Six days after discharge, he was readmitted with ongoing hypoxemia requiring up to 6 L/min of oxygen by nasal cannula and pain and tenderness at his femoral hemodialysis catheter site. Admission chest x-ray showed persistent “multifocal pneumonia, likely viral, or atypical,” and CT scan of the abdomen/pelvis revealed “edema and soft tissue stranding along the course of the right femoral tunneled dialysis catheter [with] no drainable fluid collection or soft tissue gas.” Labs upon readmission included mildly depressed platelet count of 138,000/μL, normal prothrombin time of 12.5 s, and C-reactive protein elevated further to 32 mg/dL (activated partial thromboplastin time, D-dimer, and fibrinogen were not obtained). COVID-19 PCR of a nasopharyngeal swab, repeated on admission, was again positive. Vancomycin and piperacillin/tazobactam were administered, and he was admitted to the medical service after surgery consultation concluded that he had cellulitis rather than necrotizing infection. About 6 h after presentation, he had a cardiac arrest due to ventricular tachycardia which proved refractory to approximately 30 min of cardiopulmonary resuscitation. The admitting hospitalist speculated that pulmonary embolism may have been a possible trigger for his arrest, but neither chest CT nor autopsy were performed. Blood cultures ultimately grew methicillin-resistant Staphylococcus aureus.
Conclusions
As in all medical fields, the COVID-19 pandemic has had a tremendous impact on the provision of care to patients with ESKD. However, while disruptions have been significant, dialysis access procedures have continued to be carried out in significant numbers during the pandemic. 6 Indeed, as illustrated by this case, the maintenance of vascular access is vital to the care and wellbeing of ESKD patients on hemodialysis, as the use of hemodialysis catheters is associated with an increased risk of morbidity and mortality compared to AVF or arteriovenous graft use. 7 In March 2020, the American Society of Diagnostic and Interventional Nephrology (ASDIN) and the Vascular Access Society of the Americas (VASA) issued a joint statement urging policymakers and hospital administrators to treat dialysis access procedures as high-priority (“Tier 3”) interventions that must continue to be provided during the pandemic to maintain the health and survival of ESKD patients. 8 And while the ASDIN, VASA, the Society for Vascular Surgery, 9 and the American College of Surgeons 10 all agree that interventions for thrombosed or non-functional dialysis access should not be postponed during the pandemic, the care of patients who develop AVF thrombosis during a symptomatic case of COVID-19 is less clear.
In particular, the well-established association between COVID-19 and increased risk of venous and arterial thromboses 4 raises questions about the optimal timing of hemodialysis access interventions in patients with symptomatic COVID-19. The prothrombotic state characteristic of severe COVID-19 appears to be mediated by a brisk inflammatory response and immune activation along with endothelial injury and dysfunction, together resulting in increased risk of both macrovascular and microvascular thromboses. 5 While hemodialysis access thromboses have been reported in other ESKD patients diagnosed with COVID-19,2,3 whether COVID-19 in ESKD patients independently contributes to an increased risk of thrombosis of hemodialysis access is unknown. In this case, the timing of thrombosis of previously well-functioning AVF during symptomatic COVID-19 infection, the lack of mechanical explanation for the thrombosis appreciated on angiography, and the recurrent thromboses so soon after three technically successful thrombectomies together suggest the patient’s access may have clotted in part due to a COVID-19-associated prothrombotic state. Notably, the prothrombotic coagulopathy of COVID-19 often develops early in the course of COVID-19 and, in severe cases, these hemostatic changes tend to evolve in parallel with increasing disease severity and precede subsequent multiorgan failure. 5 In this case, though we do not have enough data to determine whether a prothrombotic state directly contributed to his cardiac arrest, the recurrent fistula thromboses and the need for a hemodialysis catheter clearly ultimately contributed to his death.
In conclusion, whether COVID-19 independently confers an increased risk of hemodialysis access thrombosis in patients with ESKD warrants further systematic study. However, this case suggests that interventionalists performing hemodialysis access procedures should be aware of the prothrombotic state associated with COVID-19 and should consider it when deliberating how to best approach such interventions in patients with active COVID-19. While an initial attempt at thrombectomy ESKD in patients with symptomatic COVID-19 is likely reasonable in most cases of AVF thrombosis which are diagnosed promptly, having a lower threshold to place a hemodialysis catheter after an initial failed thrombectomy attempt may be reasonable, especially if the angiography reveals no mechanical explanation for the AVF thrombosis and/or the AVF re-thromboses rapidly.
Footnotes
Author contributions
JGO and JPT conceptualized the case report. JGO performed the procedure described, wrote the description of the procedure, and obtained the images. JPT and SAC wrote the rest of the case report, including the introduction, conclusions, and abstract. All authors reviewed and edited the manuscript and approved the final version.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Consent
Multiple attempts were made to contact the patient’s only known next of kin (nephew) but were repeatedly unsuccessful.