
Abstract
Budd-Chiari syndrome due to the tip of an internal jugular tunneled dialysis catheter malposition in inferior vena cava or hepatic vein is a rare complication. We aimed to present our experience and compare it with the previous reports to highlight the clinical features and the optimal management. A 57-year-old female with history of ANCAp vasculitis, treated by hemodialysis in the last 2 years on a right internal jugular vein tunneled catheter was admitted for pain in the right upper quadrant. A subacute Budd-Chiari syndrome due to catheter malposition was diagnosed. The catheter was removed, and a new tunneled hemodialysis line was inserted in the right internal jugular vein with the tip at the junction of right atrium with superior vena cava. Anticoagulation with apixaban 2.5 mg twice daily was started after catheter replacement and the patient was discharged. At 1 month follow-up the patient had no symptoms, and the ultrasound revealed the absence of the thrombus in the inferior vena cava. Imagining monitoring for malposition after insertion or in a clinical context suggestive for Budd-Chiari syndrome is essential for early diagnosis and treatment. In our case, anticoagulation with apixaban and prompt catheter replacement resulted in Budd-Chiari syndrome resolution.
Keywords
Introduction
Tunneled central venous catheters (CVC) are used as initial vascular access in 60% to 80% of the incident hemodialysis patients and as permanent vascular access by a more than a third of the prevalent hemodialysis patients. 1 However, the use of CVC is associated with increased morbidity and mortality due to high infection rates, central venous stenosis, and thrombosis. 1
Hepatic vein obstruction, also known as Budd-Chiari syndrome (BCS), leads to increased hepatic sinusoidal pressure, which results in portal hypertension and decreased liver perfusion. 2
To the best of our knowledge there are only eight cases reported of BCS related to hemodialysis CVC (Table 1). Therefore, we aimed to present our experience and compare it with the previous reports in order to highlight the clinical features and the optimal management of this rare complication.
Overview of case reports on Budd-Chiari syndrome due to hemodialysis central venous catheters.
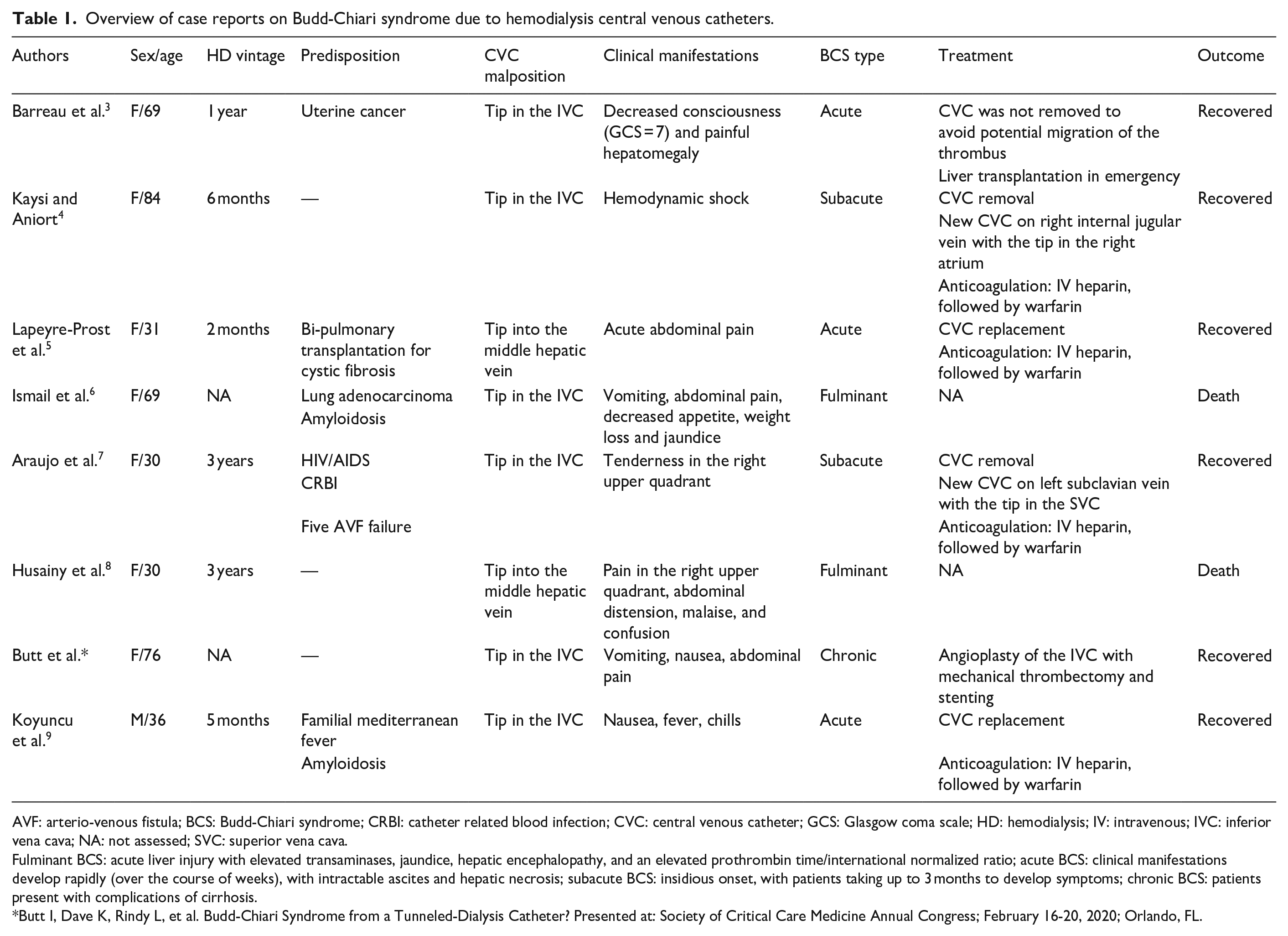
AVF: arterio-venous fistula; BCS: Budd-Chiari syndrome; CRBI: catheter related blood infection; CVC: central venous catheter; GCS: Glasgow coma scale; HD: hemodialysis; IV: intravenous; IVC: inferior vena cava; NA: not assessed; SVC: superior vena cava.
Fulminant BCS: acute liver injury with elevated transaminases, jaundice, hepatic encephalopathy, and an elevated prothrombin time/international normalized ratio; acute BCS: clinical manifestations develop rapidly (over the course of weeks), with intractable ascites and hepatic necrosis; subacute BCS: insidious onset, with patients taking up to 3 months to develop symptoms; chronic BCS: patients present with complications of cirrhosis.
Butt I, Dave K, Rindy L, et al. Budd-Chiari Syndrome from a Tunneled-Dialysis Catheter? Presented at: Society of Critical Care Medicine Annual Congress; February 16-20, 2020; Orlando, FL.
Case report
A 57-year-old female with history of ANCAp vasculitis, treated by hemodialysis in the last 2 years on a right internal jugular vein tunneled CVC (HemoStar™) was admitted for pain in the right upper quadrant.
Upon admission, her vital signs were normal: afebrile (temperature 36.3°C), normotensive (blood pressure 120/60 mmHg), heart rate 80 beats per minute, respiratory rate 18 breaths per minute and oxygen saturation 99% on room air. During physical examination, abdominal distension and tenderness in the right flank were noted, but with a negative Murphy sign.
Labs revealed mild to moderate elevation of liver enzymes (in IU/L): AST 102, ALT 144, ALP 160. Chest X-ray was normal, except for the CVC tip located in the inferior vena cava.
Ultrasound examination revealed a large thrombus in the inferior vena cava extending from the tip of the CVC to the hepatic veins (Figure 1(a)). Also, gray-scale imaging demonstrated lobulated borders of the liver with an enlarged caudate lobe and diminished visualization of the hepatic veins.
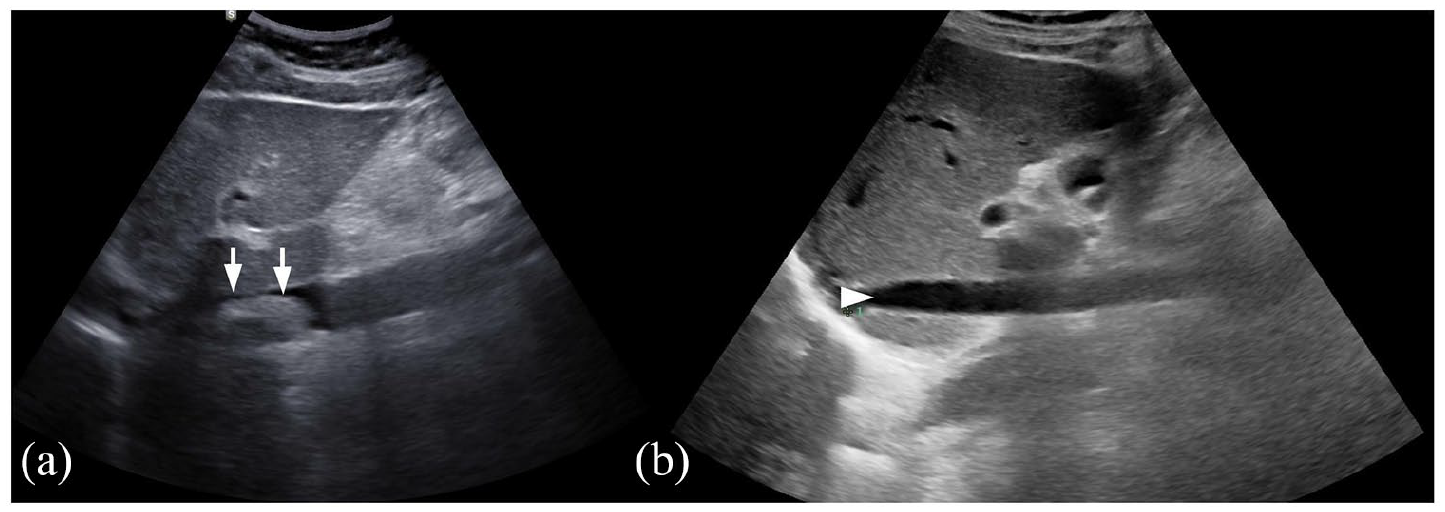
(a) Large thrombus in the inferior vena cava (white arrows) and (b) ultrasound after 1 month of treatment shows the absence of the thrombus in the inferior vena cava (white arrowhead).
The contrast enhanced CT scan showed a massive venous thrombus extending from the tip of the CVC into the inferior vena cava, occupying 80% of the lumen in the superior region of the inferior vena cava and reaching the hepatic veins, mostly in the right hepatic vein. Below the hepatic veins, the thrombus occupied 60% of the inferior vena cava lumen on 47 mm, without reaching the renal veins (Figure 2(a) and (b)).
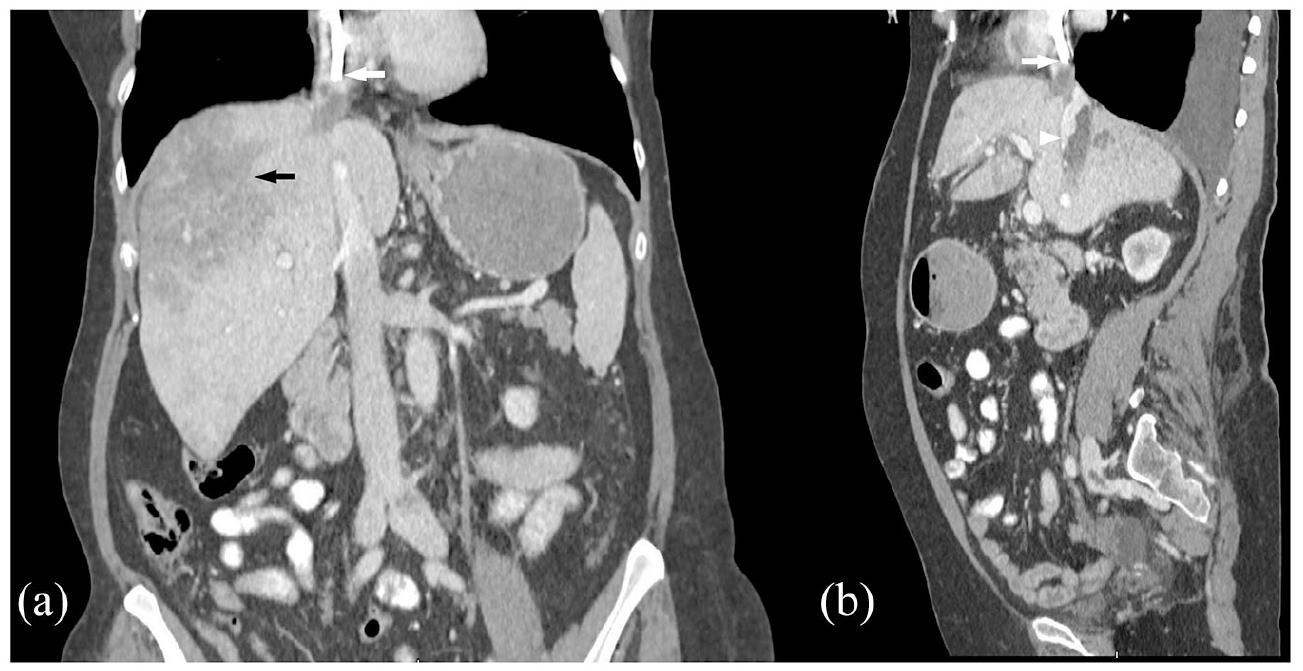
(a) Coronal section: venous thrombus at the tip of the central venous catheter extending in the inferior vena cava (white arrow). The liver has blunt edges and heterogeneous density, with predominance of hypodensity in segments IV and VIII (black arrow) and (b) sagittal section: venous thrombus at the tip of the central venous catheter (white arrow) extending in the inferior vena cava (white arrowhead).
The liver had blunt edges and heterogeneous density, with a predominance of hypodensity in segments IV and VIII (Figure 2(a)).
A subacute Budd-Chiari syndrome due to catheter malposition was diagnosed. The catheter was removed, and a new tunneled hemodialysis catheter was inserted in the right internal jugular vein with the tip at the junction of right atrium with superior vena cava.
Anticoagulation with apixaban 2.5 mg twice daily was started after catheter replacement and the patient was discharged.
At 1 month follow-up the patient had no symptoms, and the ultrasound revealed the absence of the thrombus in the inferior vena cava (Figure 1(b)).
Discussion
Primary Budd-Chiari syndrome is defined as hepatic venous outflow obstruction, usually due thrombosis. Epidemiological studies report that in non-Asian countries BCS is more common in women and usually presents in the third or fourth decade of life. 2 Interestingly, BCS related to CVC respects this epidemiological distribution, more than half of the patients were in the third decade and only one in a male (Table 1).
Patients with end stage kidney disease (ESKD) are at increased risk of venous thrombosis due to high levels of fibrinogen that directly contribute to a hypercoagulable state. 7 However, most of the reported cases of BCS related to CVC had a supplementary risk factor for thrombosis: malignancy, infections, autoimmune diseases (Table 1). In line, our patient was diagnosed with ANCA associated vasculitis (AAV), and thrombosis is a recognized and significant complication, particularly during active disease. 10 The pathogenesis of thrombotic events in AAV is not well understood. In ANCAc vasculitis, an anti-plasminogen antibody interacting with a restricted motif of plasminogen, resulting in decreased conversion of plasminogen to plasmin, which correlated with thrombotic events risk was reported. 10 However, Stassen et al. 10 reported a higher incidence of thrombotic events in also ANCAp patients. These suggest that endothelial damage, likely propagated by neutrophil-endothelial interactions in a proinflammatory milieu could also favor thrombosis in patients with AAV.9,10
CVC malposition was also present in all the previous cases of BCS related to CVC (Table 1); mostly the tip was in the inferior vena cava, but also in the middle hepatic vein in two cases. Malposition of the central line occurs due to in time migration or dislocation related to intrathoracic pressure changes during deep breathing, cough, and formation of fibrin sheath around the tip. 9 CVC migration can be reduced by positioning the tip at the junction of the right atrium and the superior vena cava, which is located approximately two vertebral body units below the carina on chest X-ray. 9 In our patient we promptly replaced the catheter with a shorter one placed in the same internal jugular vein but with the tip correctly positioned.
Our patient developed subacute Budd-Chiari syndrome. The clinical features had an insidious onset in 3 months and the symptoms were rather mild (vague discomfort in the mid epigastrium or right upper quadrant). Moreover, in contrast to the fulminant and acute BCS, in subacute forms ascites and hepatic necrosis may be minimal due to decompression of the sinusoids by portal and hepatic venous collaterals. 2
The diagnosis of BCS can be established in a noninvasive manner by hepatic Doppler ultrasonography findings: flat hepatic wave form, enlarged intrahepatic or subcapsular collaterals with continuous flow, large hepatic vein that appears void or has reversed or turbulent flow. Other, nonspecific ultrasonographic findings include hepatomegaly, ascites, intra-abdominal collaterals, caudate lobe hypertrophy, atrophy of other hepatic lobes, and compression of the inferior vena cava. 2
Contrast enhanced CT may reveal the same nonspecific anomalies observed with ultrasonography, and more specific signs, like delayed or absent filling of the three major hepatic veins, a patchy “flea-bitten” appearance of the liver due to increased centro-lobular contrast enhancement relative to periphery, rapid clearance of contrast from the caudate lobe and narrowing of opacification of the inferior vena cava. 2
The guidelines recommend that all patients be started on anticoagulation at the time of BCS diagnosis. 2 Nevertheless, the risk of anticoagulation should be evaluated in patients who present with bleeding complications or those with esophageal varices. Most patients with BCS related to CVC received anticoagulation, initially with intravenous heparin and then with vitamin K antagonist (Table 1). However, we report the first case of BCS efficiently treated with apixaban 2.5 mg twice daily. In this prescribed dose, apixaban resulted in drug exposure similar with that of the standard dose (5 mg twice daily) in patients with preserved renal function and might be a reasonable alternative to vitamin K antagonists in patients on hemodialysis. 11 Also, it is important to note that apixaban has been shown to be safer than vitamin K antagonist in patients on maintenance hemodialysis with respect to major bleeding events, both at the standard dose and the reduced dose. 12 Besides inhibiting free and clot-bound factor Xa, Apixaban hinders prothrombinase activity, which prevents thrombus growth.11,12
Treatment options for patients with acute or subacute Budd-Chiari syndrome who fail to improve with other treatments include the placement of a transjugular intrahepatic portosystemic shunt, surgical shunting, and liver transplantation. 2 There was only one case of liver transplantation for acute BCS related to CVC (Table 1).
The successful use of thrombolytic agents in Budd-Chiari syndrome is limited to small case series and individual reports. However, in most cases this approach has limited efficacy and exposes the patient to the risks of thrombolytic therapy, which include bleeding, stroke, and pulmonary embolism. 2 Moreover, we found no reports on thrombolysis in BCS related to CVC (Table 1).
If untreated, symptomatic BCS has a high mortality rate. Before specific therapy became available, 90% of patients died within 3 years. 2 However, the survival rates are significantly better with treatment: survival rates at 1, 2, and 5 years were 87%, 82%, and 74%, respectively. 2 From the total of eight cases of BCS related to CVC reported until now, only two were fatal; hepatic encephalopathy and liver failure were the causes of death (Table 1).
Conclusion
Budd-Chiari syndrome due to the tip of an internal jugular tunneled dialysis catheter malposition in inferior vena cava or hepatic vein is a rare complication. Imagining monitoring for malposition after insertion or in a clinical context suggestive for Budd-Chiari syndrome is essential for early diagnosis and treatment. In our case, anticoagulation with apixaban and prompt catheter replacement resulted in Budd-Chiari syndrome resolution.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study was carried out in accordance with the Declaration of Helsinki and approved by the Institutional Ethical Committee.
Informed consent
Written informed consent was obtained from the patient for publication.